
Abstract
Anxiety in older adults can negatively impact driving behaviors due to the associated symptoms and medications used to treat them. We aimed to investigate the effect of anxiety and anxiolytics on driving behaviors in older adults using data from participants enrolled in the multi-site AAA Longitudinal Research on Aging Drivers Study. A total of 2,832 participants met the eligibility criteria. Using generalized linear models, compared to participants without anxiety or anxiolytic use, those with anxiety alone (−540 miles/year, 95% CI = −1,002 to −78) and those with both anxiety and anxiolytic use (−1,777 miles/year, 95% CI = −2,910 to −644) drove fewer miles. Additionally, participants with anxiety (1.19, 95% CI = 1.08–1.32) and those with both anxiety and anxiolytic use (1.32, 95% CI = 1.02–1.67) experienced a higher rate of hard braking events. Older adults with anxiety conditions and taking anxiolytics should use caution when driving.
• Older drivers using anxiolytic medications exhibited reduced driving distances compared to those not taking anxiolytics. • Older drivers using anxiolytic medications demonstrated a higher frequency of hard braking incidents, potentially indicating more erratic driving behavior and increased safety risks. • Significant differences in annual miles driven were observed across various subgroups, with females driving significantly fewer miles than males.
• The findings highlight the need for clinical precautions regarding driving for older adults using anxiolytic medications, including enhanced warnings on medication package inserts and labels. • Patient consultations should emphasize safe driving practices, which may help reduce hard braking events and prevent car crashes, particularly among older adult drivers. • Policymakers and healthcare providers can use this study as an educational tool to inform prescribing, dispensing, and regulatory decisions, raising awareness of the potential driving-related side effects of anxiolytic medications in older adults.What this paper adds
Application of study findings
Introduction
Every year, there are 1.35 million deaths worldwide due to motor-vehicle crashes (World Health Organization, 2018). In the United States, about one in five motor-vehicle crash deaths involved adults older than 65 years (National Safety Council Deaths and death rates by type of crash and victim age, United States, 2023). Older adults often face unique challenges related to driving and road safety such as age-related factors coexisting with chronic medical and mental health conditions (Aksan et al., 2015; Anstey et al., 2018; Carr, 2000). The reported prevalence of any anxiety disorders among older adults is 15.3% but lower compared to younger adults with any anxiety disorders (range of 30–35%) (Kessler et al., 2005). Anxiety disorders is one of the most prevalent mental health disorders in older adults, compared to mood disorder and substance use disorder (Reynolds et al., 2015). Clinically significant anxiety in older adults, however, has been associated with cognitive impairments, including deficits in short-term memory and general cognitive function (Petkus et al., 2017; Wolitzky-Taylor et al., 2010). Symptoms of anxiety include uncontrollable worrying, distress, and restlessness; older adults with anxiety have shown to display higher levels of muscle tension, fatigue, and sleep disturbances compared to asymptomatic older adults (Wolitzky-Taylor et al., 2010). Older adults with anxiety have also been reported to display more sleep disturbances compared to younger patients (Altunoz et al., 2018). Among older adults, the impact of anxiety disorders and their potential exacerbation during driving tasks are important for identifying risk factors associated with impaired driving performance. Previous research suggests a significant association between anxiety and impaired driving among older adults, indicating a potential exacerbation of anxiety symptoms triggered by driving tasks (Palumbo et al., 2019; Pitta et al., 2021). This finding emphasizes the importance of addressing anxiety disorders and implementing strategies to manage anxiety symptoms in older drivers, thus promoting road safety and overall well-being in this vulnerable population.
Several classes of psychotropic medications are used to treat anxiety disorders such as antidepressants, benzodiazepines, anticonvulsants, antipsychotics, and antihistamines (Bandelow et al., 2012). According to the US Department of Transportation and National Highway Traffic Safety Administration (Carr et al., 2023), more than 90 classes of medications have been associated with motor crashes in older adults. Medications that cause sedation, dizziness, and blurred vision, such as antidepressants, benzodiazepines, sedatives and hypnotics, and antihistamines, were the most offending agents (Hetland & Carr, 2014; Ivers & White, 2016). Numerous studies, conducted both internationally and in the United States, have observed that older adults (65–89 years) are prescribed sedative-hypnotic medications at a significantly higher rate compared to younger adults (18–69) and for longer duration than recommended (Neutel et al., 2012; Olfson et al., 2015; Sandelin et al., 2013). For instance, approximately 31% of older adults (65–80 years) in the US were reported to use benzodiazepines long term (Olfson et al., 2015) and 40% of older adults in Germany with generalized anxiety disorder (GAD) were prescribed relatively high doses of benzodiazepines, despite their classification as potentially inappropriate medications per the Beers Criteria (Samuel, 2023). The Beers Criteria for Potentially Inappropriate Medication (PIM) Use in Older Adults is published by the American Geriatrics Society to reduce exposure for PIM use in older adults and provide guidance to clinicians regarding the risks of these medications. Medications included in the Beers Criteria are generally contraindicated in older adults due to their sedating effects, risk of falls, and increased risk of cognitive impairment over time (de Gage et al., 2012; Pariente et al., 2008). According to the 2023 updated Beers Criteria, the anxiolytics included in this study are considered to have strong recommendations and high-quality evidence indicating that the risks of harm, adverse events, and other risks “clearly outweigh the benefits” in older adults (Samuel, 2023). In addition, national trends from 2003 to 2012 depict a notable rise in the prescription rates of benzodiazepines and other anxiolytics/sedative-hypnotics among older adults regardless of a mental health diagnosis, particularly during visits to primary care providers rather than psychiatrists (Maust et al., 2017). Given these concerning trends in medication prescribing practices among older adults and their associated risks, the current study aims to address a gap in knowledge by examining the impact of anxiety disorders, both with and without anxiolytic medication use, on driving behaviors in older adult drivers.
Methods
Study Population and Data Collection
The AAA Longitudinal Research on Aging Drivers (LongROAD) study is a multi-site, longitudinal, prospective cohort study to examine the driving behaviors and medication usage of older adults. In the LongROAD study, 2990 older adults aged 65–79 in the United States from July 2015 to March 2017 were enrolled in five different sites across the country (Ann Arbor MI, Baltimore MD, Cooperstown NY, Denver CO, and San Diego CA) in four geographic regions (Northeast, Midwest, South, and West) (Li et al., 2017). The methods have been described elsewhere (Li et al., 2017). Participant were excluded if they had diagnoses considered to contribute to unsafe driving, such as dementia, Parkinson, blindness, memory loss, late-stage cancers, or end-stage diseases. Participants with missing medication or driving data were excluded. The study was approved by institutional review boards at all sites (IRB# 141800).
Study participants underwent standardized assessments, including physical, cognitive, and physiological tests at baseline and then annually for up to 5 years. Comprehensive medication information was collected through a brown bag medication review conducted at the beginning of each year of enrollment and documented in a centralized database. The medications names were recorded and coded using the American Society of Health-System Pharmacists Pharmacologic-Therapeutics Classification System (AHFS) (American Society of Health-System Pharmacists, n.d.; Hill et al., 2020). Telemetric technology was used to collect driving behavior. The device, “DataLogger” (Danlaw, Inc, Novi, MI), tracked speeding events, number of trips, trip duration and time of day, turns, and rapid deceleration. We conducted an analysis based on data collected throughout the first year of the study, defined as each participant’s first 12 months.
Outcome Definitions
Medications Used for the Management of Anxiety.
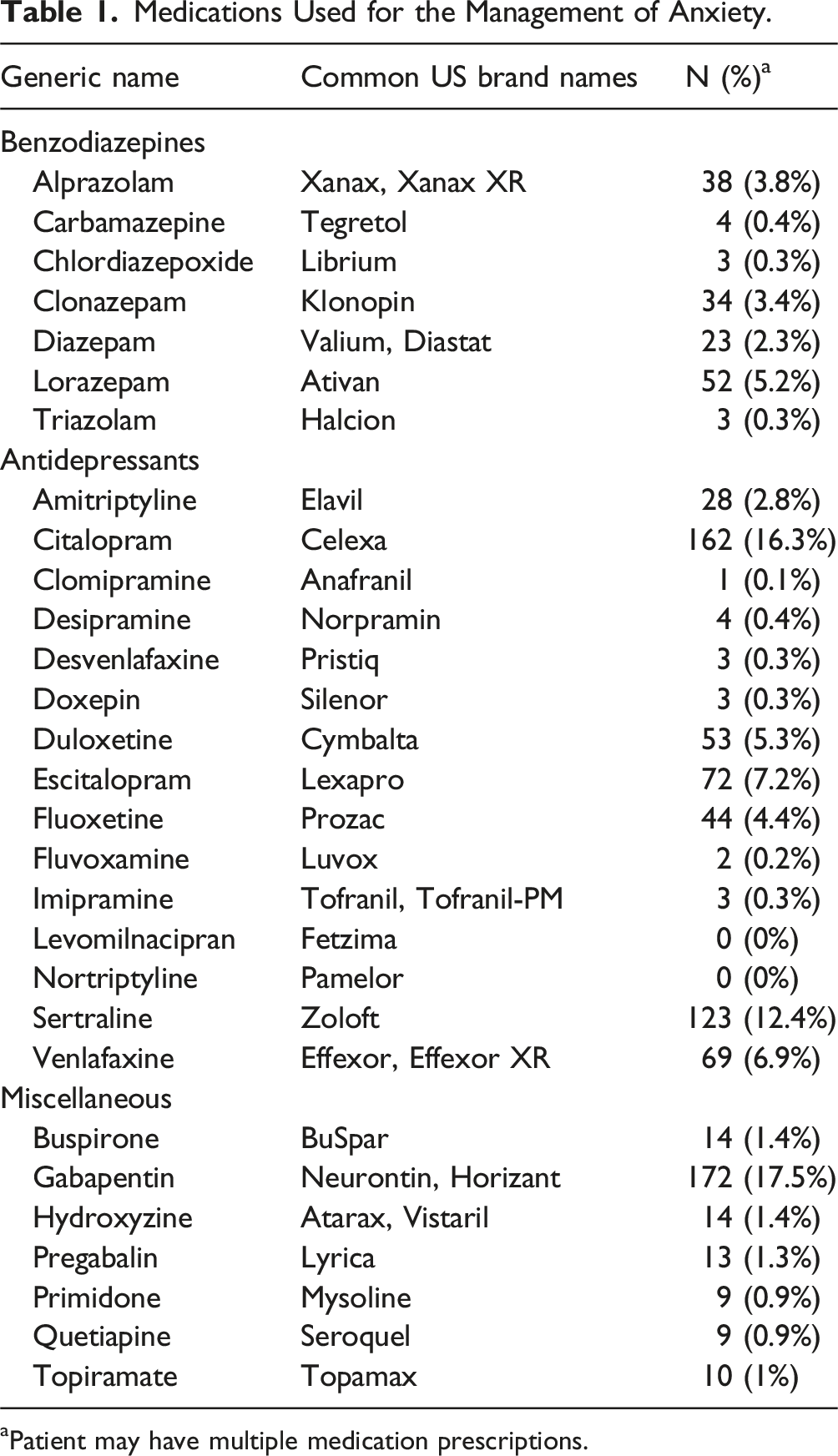
aPatient may have multiple medication prescriptions.
Based on their self-reported anxiety status and use of anxiolytic medications, participants were divided into four categories. The four groups were as follows: self-reported anxiety and current use of anxiolytics (A+M+), self-reported anxiety and no current use of anxiolytics (A+M-), no self-reported anxiety and current use of anxiolytics (A-M+), and no self-reported anxiety and no current use of anxiolytics (A-M-), which served as the reference group.
To assess the impact of self-reported anxiety and the use of anxiolytics on driving performance, the following driving outcomes were examined at baseline: instances of speeding, hard braking events, nighttime driving, and total mileage driven. Speeding events were defined as driving at a speed of 80 mph or greater for at least eight consecutive seconds, while a hard braking event was identified as a deceleration of ≥0.4 or more. Nighttime driving was categorized as a trip where 80% or more of the journey occurred during the nighttime, with a solar angle of greater than 96° (Hill et al., 2020).
Descriptive and Statistical Analysis
Participants were categorized into three age groups: 65–69, 70–74, and 75–79 years. Additionally, they were grouped based on gender, race, marital status, and education level, which included high school or less, some college (no degree), associates or bachelor’s, and advanced degrees. Further demographic information was collected, including the employment status of participants, engagement in exercise, volunteer work, and income.
Data were summarized using median (inter-quartile range [IQR]) or counts (%). Continuous variables were analyzed by two independent samples t test or the Wilcoxon rank-sum test, as appropriate. Categorical variables were analyzed using the chi-square test or Fisher’s exact test, as appropriate. Count variables were analyzed using Quasi-Poisson distribution to account for the over-dispersion of the data. The total counts of speeding, hard braking, and nighttime trips were analyzed per 1,000 miles to account for variability in annual mileage driven across participants.
To investigate the effect of anxiety and anxiolytics on miles driven per year and hard braking events, we performed multivariable regression analyses using generalized linear models, adjusting for the potential confounding effects of age, gender, race, marital status, volunteering, working, education, and income. Miles driven per year were assumed to follow a Gaussian distribution, while hard braking counts were assumed to follow a Quasi-Poisson distribution. All hypotheses were analyzed as two-sided, and the statistical significance level was set at 5%. We completed the statistical analysis using R version 4.3.3 and RStudio 2024.04.1.
Results
Participant Demographics.
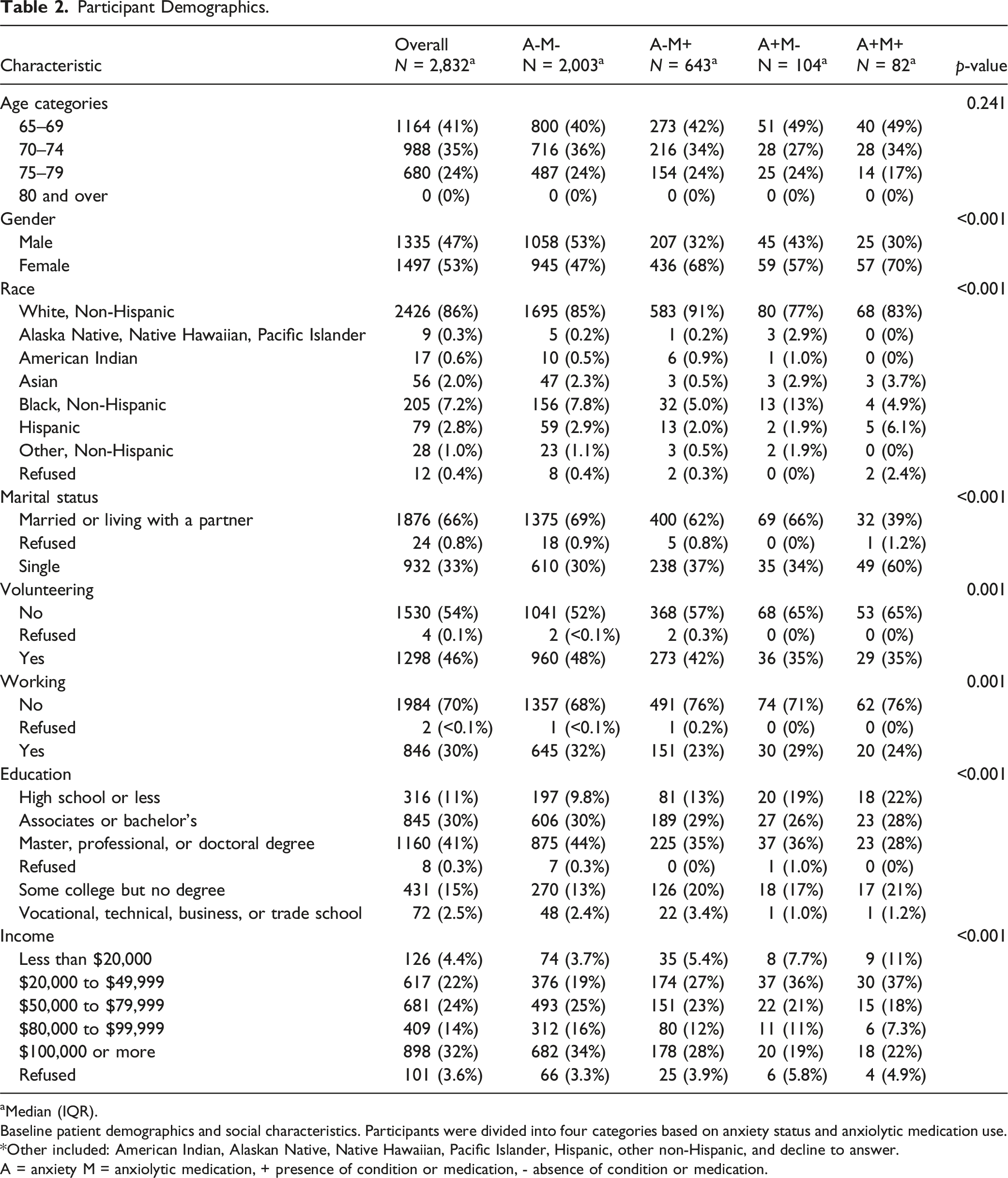
aMedian (IQR).
Baseline patient demographics and social characteristics. Participants were divided into four categories based on anxiety status and anxiolytic medication use. *Other included: American Indian, Alaskan Native, Native Hawaiian, Pacific Islander, Hispanic, other non-Hispanic, and decline to answer.
A = anxiety M = anxiolytic medication, + presence of condition or medication, - absence of condition or medication.
Unadjusted Driving Outcomes in Participants With and Without Self-Reported Anxiety and Anxiolytic Medication Use.
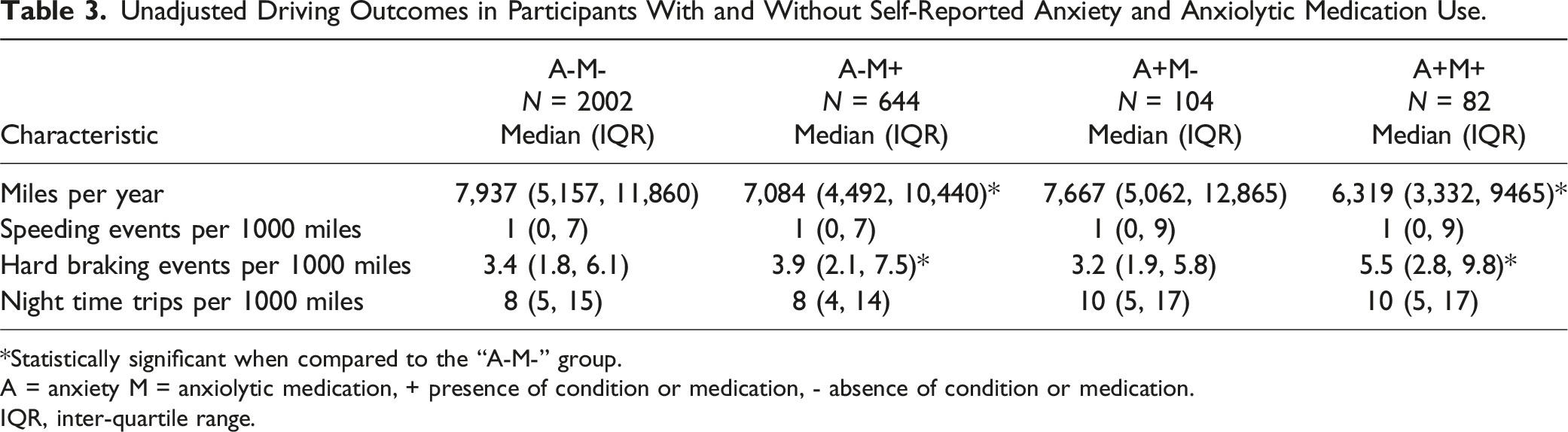
*Statistically significant when compared to the “A-M-” group.
A = anxiety M = anxiolytic medication, + presence of condition or medication, - absence of condition or medication.
IQR, inter-quartile range.
Adjusted Miles Driven per Year.
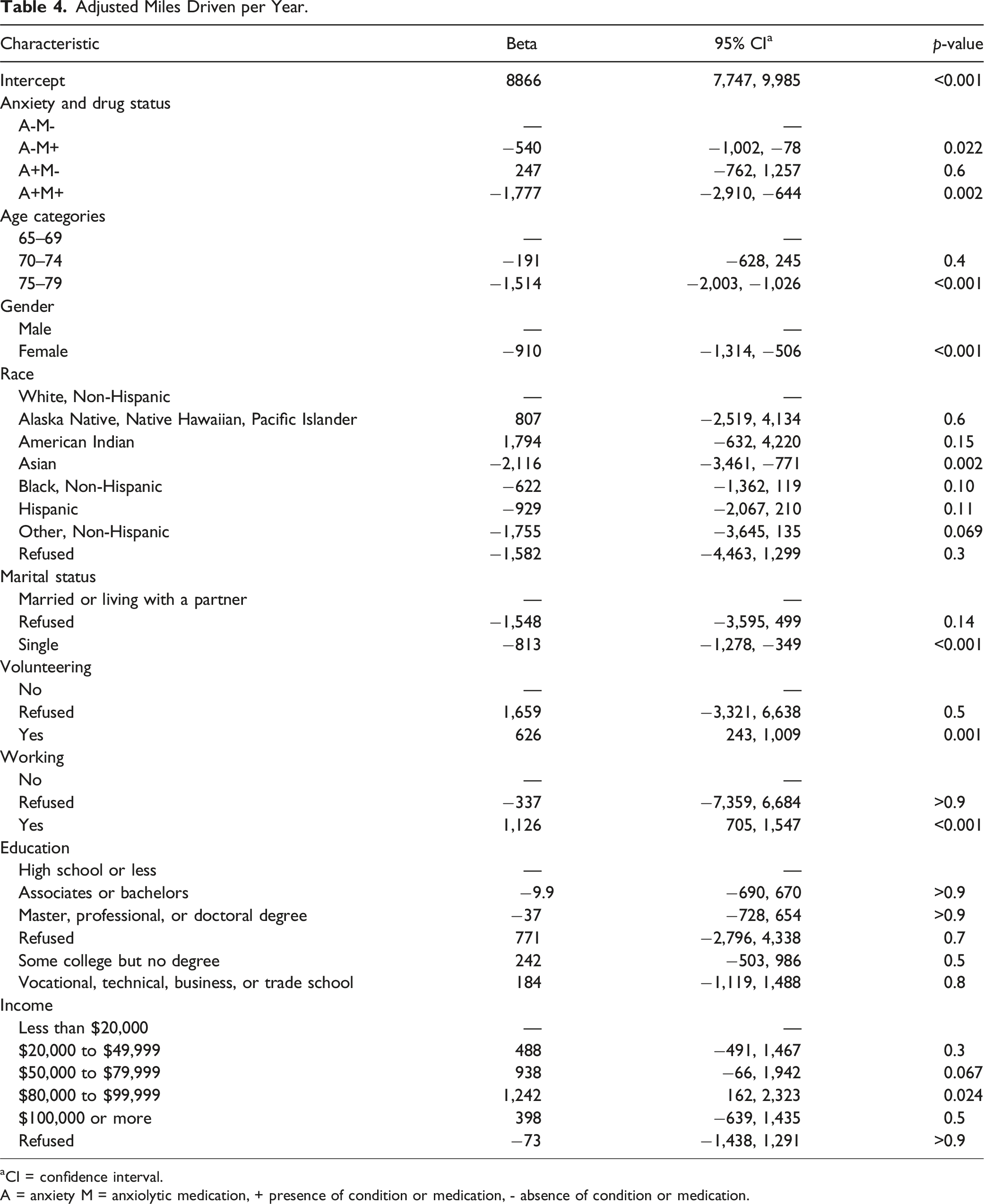
aCI = confidence interval.
A = anxiety M = anxiolytic medication, + presence of condition or medication, - absence of condition or medication.
Adjusted Hard Braking Events per 1000 Miles Driven.
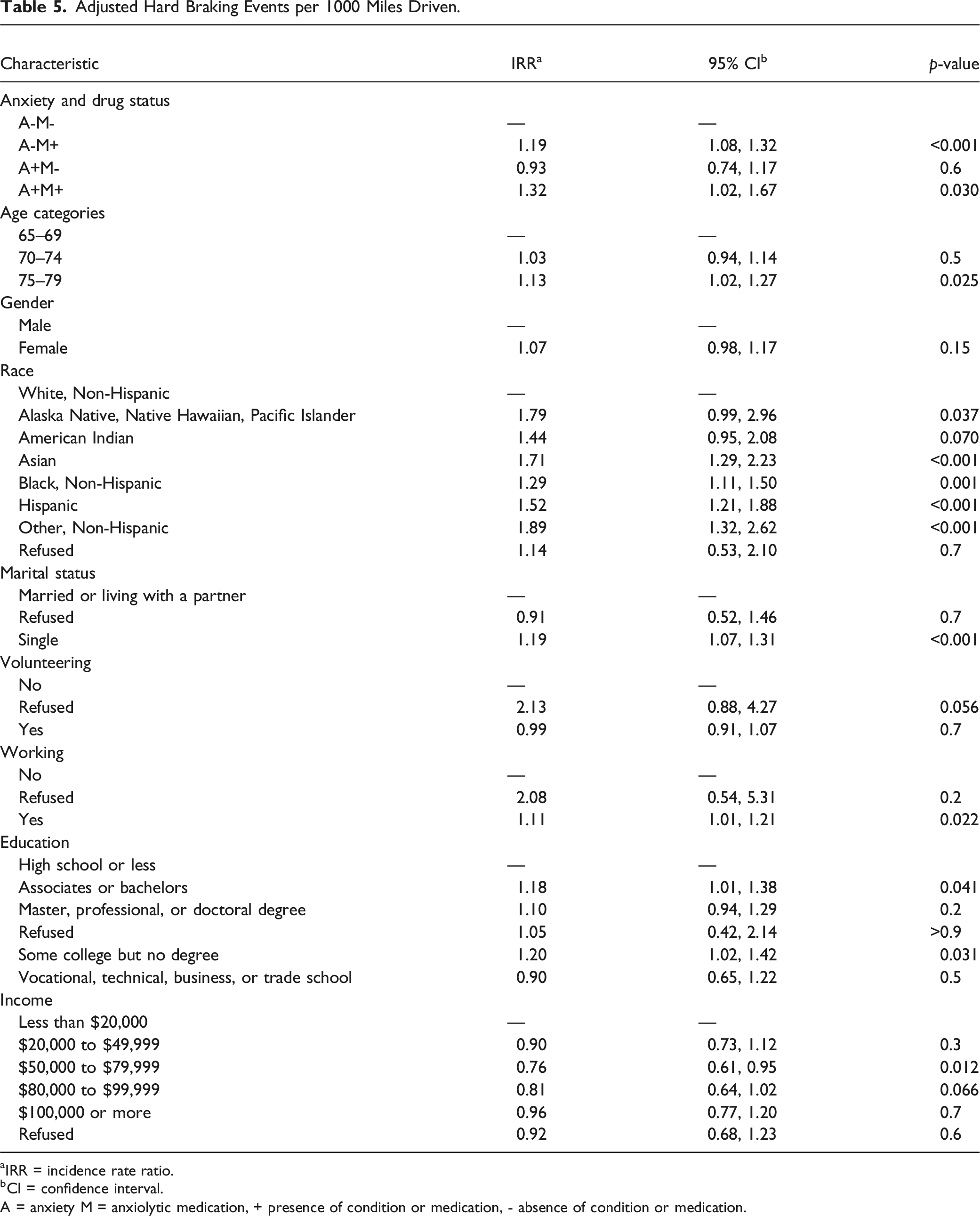
aIRR = incidence rate ratio.
bCI = confidence interval.
A = anxiety M = anxiolytic medication, + presence of condition or medication, - absence of condition or medication.
Discussion
Anxiety disorders (Brenes et al., 2005; Norton et al., 2012) and anxiolytics (Dassanayake et al., 2011; Verster & Vokerts, 2004) can significantly impact driving behavior and performance due to physiological and pharmacological effects, respectively, in older adults. Certain anxiety conditions such as panic and generalized anxiety disorder can affect driving by impeding concentration or by causing physiological symptoms such as hyperventilation and tachycardia. Either psychological or physiological symptoms can distract the driver from the tasks at hand (Mehta et al., 2007; American Psychiatric Association [APA], 2022). Anxiolytics, such as benzodiazepines (Dassanayake et al., 2011), antidepressants (Dassanayake et al., 2011), and antihistamines (Verster & Vokerts, 2004) can impair driving due to their pharmacological properties that can result in sedation, dizziness, and fatigue. As the driving population ages, it is important to identify potential disease- and medication-related factors that impact driving. In this study, older drivers who had anxiety and used anxiolytic medications had a higher frequency of hard braking incidents compared to those without anxiety or anxiolytic use.
In older adults, the prevalence of any anxiety disorders is estimated to range from 9 to 17% (Canuto et al., 2018; Kirmizioglu et al., 2009; Miloyan & Pachana, 2015; Norton et al., 2012; Welzel et al., 2019) with GAD among one of the most prevalent at 4–7%. In this current study of older adults, the prevalence of participants with anxiety symptoms was 6.5%; due to lack of diagnostic data, it is unknown whether the study participants had GAD or other anxiety disorders. In this study, female participants had a higher prevalence of anxiety and anxiolytics use compared to males. This is consistent with previous studies demonstrating consistently higher rates of anxiety in elderly females compared to males, with a statistically significant trend with age (Byers et al., 2010; Centers for Disease Control and Prevention, 2020). Women are also more likely to seek treatment for mental health conditions compared to men (Terlizzi & Schiller, 2022), and older adults have shown to be more likely to have help-seeking attitudes and positive beliefs about treatment when compared to younger adults (Mackenzie et al., 2008). There have also been reports that sub-threshold anxiety symptoms are prevalent in late life with associated decline in function, daily activities, and quality of life (Kang et al., 2016; Mehta et al., 2007; Norton et al., 2012; Porensky et al., 2009).
The use of antidepressant medications, often used to treat anxiety disorders, have been shown to increase with age, especially among women aged 60 years and over (24.3%) (Centers for Disease Control and Prevention, 2020). In another study, one third of older adults aged 65–80 years received a benzodiazepine prescription for longer than 4 months in one year (Olfson et al., 2015). In a European study, individuals aged 60 years and above constituted more than half of the total population consuming antidepressants, anxiolytics, hypnotics, and sedative medications (Kirmizioglu et al., 2009). These figures are consistent with the current study in which 25.6% of participants reported taking anxiolytics.
In the adjusted driving outcomes analysis, participants taking anxiety medication drove fewer miles per year, regardless of anxiety status compared to those without anxiety medications. In a study by Isom et al., antidepressant use was also associated with fewer miles driven per year (Isom et al., 2024). In one study of healthy older adults, selective serotonin reuptake inhibitors (SSRIs), serotonin norepinephrine reuptake inhibitors, and sedative or hypnotics were associated with a 2.7–2.8 increased risk of marginally or failing a road test compared to the control group over a 10-year period (Carr et al., 2023). In the current study, we also found that sex and race/ethnicity to be significant confounders for the relationship between anxiety and anxiolytics use and miles driven year and hard braking events, respectively.
Anxiety while driving has also been observed in older adults, which may impact their driving behavior. In one study of anxiety associated with driving in older adults, 10–27% of older adults reported mild to extreme levels of anxiety while driving (Taylor et al., 2018). Women were more likely to have mild to moderate anxiety while driving and those who were older than 70 years were more likely to have moderate to extreme anxiety (Taylor et al., 2018). They were also less likely to drive and drive for shorter distances. Anxiety associated with driving has been shown to have lower quality of life (Taylor et al., 2018, 2022). Due to driving anxiety, older adults may self-regulate their driving behaviors such as avoiding driving at night and reducing the frequency of driving or distance (Baldock et al., 2006).
In the current study, those taking anxiolytics had higher rates of hard braking regardless of anxiety symptoms. Hard braking among drivers has been associated with higher likelihood of crashes (Gitelman et al., 2018). In fact, older adults who were taking more than two medications were also found to have higher risk of hard braking events in a dose-related fashion (i.e., more medications, higher risk) (Jian et al., 2024). In another LongROAD study of participants with depression and antidepressant medications, older adults taking antidepressant medications had higher rates of hard braking events (Isom et al., 2024).
Prior studies reported an association between psychoactive drug use and increased crash risk in older adults (Cameron & Rapoport, 2016; Conen et al., 2011; Laddha et al., 2011; Peterson, 2009; Ray et al., 1992; Verster et al., 2005; Verster & Mets, 2009). Anxiolytics, in particular, are associated with central nervous system side effects including slowed movements and reflexes, slurred speech, and decreased balance, all of which could compromise driving abilities (Laddha et al., 2011; Verster et al., 2005; Verster & Mets, 2009). Compromised driving behaviors, specifically increased risk of hard braking, was found in this study among those taking anxiolytic medications. A retrospective cohort study of Medicaid enrollees 65–84 years of age showed an increased risk of injurious crash involvement in those receiving benzodiazepines and cyclic antidepressants (Ray et al., 1992). One study of older adults found that antidepressant drugs such as imipramine increased standard deviation of lateral position (SDLP) and impaired highway driving in the elderly (Cameron & Rapoport, 2016). In another study, drivers who used benzodiazepines, GABAergic compounds, and tricyclic antidepressants had higher SDLP and exhibited more weaving of the vehicle (Verster et al., 2005). In contrast, SSRIs, buspirone, venlafaxine, and serotonin antagonists showed no significant impairment on driving (Verster et al., 2005). With the increased usage of gabapentin as an off-label medication for anxiety, a study found an association between gabapentin and impaired driving as participants exhibited horizontal gaze nystagmus and poor performance on standardized field sobriety tests (Peterson, 2009). Similar to gabapentin, hydroxyzine also caused driving impairment as measured by SDLP in healthy participants when compared to bilastine (Conen et al., 2011). Compared to younger adults, psychoactive medications have a greater impact on older adults leading to higher impairment, greater SDLP suggesting erratic steering behavior, and lower performance (Verster & Mets, 2009). While we could not discern the impact of individual medications on driving behaviors in this study, there is concern regarding the use of anxiolytic medications as a class in older adults that could affect driving performance.
Due to the impact of these medications on driving, it is important for clinicians to educate patients about these risks, especially at the initiation of treatment. Patients should understand the laws surrounding driving while under the influence of not just from alcohol but also medications such as benzodiazepines. There is a need for heightened awareness of these risks among older adults and family members/caregivers. Potential interventions may include having flyers available at hospitals and clinic waiting rooms, pharmacies, and grocery stores. Public health campaigns such as the “Safe Driving” campaign in 2017 may help to promote safe driving and provide tips and resources for older adults (American Geriatrics Society, 2017). These strategies may help to spur conversations and promote awareness around medications while driving.
Strengths and Limitations
There are several limitations to the study. First, anxiety was defined by using the PROMIS Emotional Distress—Anxiety—Short Form scores which may not reflect an actual diagnosis of an anxiety disorder. We also could not distinguish between different anxiety disorders, which present very differently and have diverse symptomatology and treatments. We also could not distinguish the severity of anxiety symptoms at the time of the driving behaviors nor confirm whether the patients were actively taking the anxiolytic medication at any given time since medication history was taken only at baseline and annually. We also could not discern the differences between antidepressants, benzodiazepines, and other medication classes and their impact on driving behaviors since we grouped anxiolytics into one category. In a previous study of those with depression, antidepressants were identified to influence miles driven per day and associated with fewer trips at night. Assessing the interaction between medication class and other variables of interest, such as sex, race/ethnicity, and education, on driving behaviors remains a subject for future studies. It should be noted that the collection of PROMIS scores and medication information was completed at the beginning of the baseline year, and the analysis is based on the assumption that anxiety status and anxiolytics usage remained constant throughout the entire year. This assumption could have influenced our estimates of anxiety and anxiolytics impact on driving behaviors. Lastly, participants’ telemetric driving data was collected from their main car; driving in other cars was not captured, though participants consented to driving their instrumented vehicle at least 80% of the time. Despite the limitations, this study has strengths that are worth highlighting. First, medication assessments were completed in person as a “brown bag” review, allowing the capture of all prescription medications regardless of the dispensing pharmacy or prescribing provider. Second, using a DataLogger enabled accurate and continuous recording of a comprehensive set of objective driving behavior metrics while eliminating the reliance on self-reported information, thus reducing the risk of recall bias. Lastly, the LongROAD study recruited a large sample size of older adult drivers across different geographical locations, ages, and ethnicities, facilitating a comprehensive assessment of driving behaviors.
Future Directions
Future research includes evaluating the long-term effect of anxiolytic use, as well as the specific types of anxiety disorders that may impact driving behaviors. Participants with confirmed anxiety diagnoses would also be important to distinguish from those with transient anxiety symptoms to determine whether there are differences in driving behaviors. The individual risk of different classes of anxiolytics on driving behavior in older adults also needs to be explored. Beyond the research needs, public policies and campaigns to educate older adults on the impact of medications on driving behavior are also necessary. The impact of medication on driving performance presents a significant public health concern requiring focused efforts to enhance road safety.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the AAA Foundation for Traffic Safety (Longitudinal Research on Aging Drivers).
Ethical Statement
Data Availability Statement
Data is not publicly available but collaborative studies can be arranged with the investigators.