
Abstract
Care partners of hospitalized persons with dementia often experience significant burden at discharge. This study examined whether dementia care partner health literacy mediates the relationship between education and burden at hospital discharge. Data from 277 care partners in the Family-centered Function-focused Care (Fam-FFC) trial were analyzed using mediation analysis to assess indirect effects of education on burden (Short-Form Zarit Burden Interview [ZBI-12]) through health literacy (Rapid Estimate of Adult Literacy in Medicine-Short Form [REALM-SF]). Analyses were conducted using SPSS and AMOS. For medium education (B = −0.012; 95% CI = −0.019, −0.003), the indirect effect accounted for 18.5% of the total effect, while for high education (B = −0.018; 95% CI = −0.026, −0.006), it accounted for 21.4%, indicating partial mediation. Findings underscore the role of health literacy in reducing care partner burden and highlight the need to address education and literacy disparities to provide effective support at hospital discharge.
• Explores the mechanisms linking care partner education, health literacy, and burden, identifying health literacy as a mediating factor. • Demonstrates that higher education levels are associated with better health literacy, which in turn reduces care partner burden during hospital discharge. • Highlights the unique role of health literacy in care partner outcomes during the underexplored transition of hospital discharge.
• Hospitals should integrate health literacy assessments into discharge planning to identify care partners at greater risk of burden and provide tailored, accessible support. • Practical strategies include simplifying discharge instructions using plain language and visual aids, offering structured training programs to enhance caregiving skills, and implementing caregiver-centered communication tools to better prepare care partners for their roles. • Addressing health disparities in care partner education and literacy within healthcare systems can promote equity and improve outcomes for both care partners and patients.What this paper adds
Applications of study findings
Introduction
Persons living with dementia are hospitalized at nearly twice the rate of those without the condition and account for approximately one-fourth of hospital admissions among older adults (Alzheimer’s Association, 2024; Phelan et al., 2012). Frequent hospitalizations disrupt established caregiving routines and introduce new sources of stress for care partners (typically unpaid family members, such as adult children or spouses), including worries about the patient’s condition, uncertainty about managing care after discharge, and concerns over heightened care needs (Abbott et al., 2022; Boltz et al., 2015). This stress often extends into the post-discharge period, as care partners assume increased responsibilities during the hospital transition (Boltz et al., 2015, 2023; Dramé et al., 2012; Gual et al., 2018; Mathews et al., 2014; White et al., 2024). These responsibilities include managing increased caregiving tasks, understanding complex medical instructions, and supporting the heightened dependency of the patient, all of which can contribute to elevated care partner burden at hospital discharge (Boltz et al., 2023; Kuzmik et al., 2022, 2024).
Lower levels of education are closely associated with poorer health outcomes (Pellicer-Espinosa & Díaz-Orueta, 2022; Zajacova & Lawrence, 2018). For dementia care partners, limited education can make navigating healthcare systems and accessing resources more difficult (Gaugler et al., 2023), further complicating their caregiving responsibilities. Lower education levels have been linked to increased burden among care partners across various settings (García-Martín et al., 2023; Putri et al., 2022; Teahan et al., 2021). However, the mechanisms underlying this relationship, in the context of critical transitions such as hospital discharge, remain poorly understood.
Health literacy, which is strongly associated with education (Jansen et al., 2018; Lorini et al., 2023), is particularly relevant during hospital discharge. Health literacy levels play an important role in care partners’ ability to understand discharge instructions, which often include medication changes, scheduling and attending follow-up healthcare services, and adapting to changes in the care routine. Defined as the ability to locate, comprehend, and utilize information and services to make informed health decisions and take appropriate actions for themselves or others (U.S. Department of Health and Human Services, 2021), health literacy plays a vital role in dementia caregiving. Care partners with limited health literacy often face challenges in acquiring and applying the information necessary for effective caregiving (Gaugler et al., 2023; Putri et al., 2022). Low health literacy can lead to gaps in knowledge about dementia care, leaving care partners unprepared to navigate the complexities of their role (Gaugler et al., 2023). Additionally, low health literacy can hinder effective communication with healthcare professionals and reduce access to care partner support services (Jansen et al., 2018), intensifying care partner burden. While prior research has linked lower health literacy to greater care partner burden (Häikiö et al., 2020; Wang et al., 2020; Yuen et al., 2018), little is known about its role as a mediator between education and burden during hospital discharge.
Understanding the mechanisms through which care partner education and health literacy influence burden is essential for developing effective interventions to support dementia care partners during the post-hospital transition. Previous research has established that lower care partner education and limited health literacy are independently associated with greater burden across diverse geographic contexts (García-Martín et al., 2023; Häikiö et al., 2020; Putri et al., 2022; Teahan et al., 2021), yet the extent to which health literacy mediates the relationship between education and burden at hospital discharge remains unclear. It is important to address this gap because hospital discharge presents a period of heightened vulnerability, requiring care partners to process complex medical instructions, coordinate follow-up care, and adjust to increased caregiving demands, which may be especially challenging for those with lower health literacy. By identifying health literacy as a potential mechanism linking education and burden, our findings could help inform more targeted discharge planning strategies, enhance care partner education programs, and ultimately reduce disparities in caregiving burden. This study aimed to examine the mediating role of dementia care partner health literacy on the relationship between education level and burden at hospital discharge. We hypothesized that higher health literacy would mediate the relationship between higher education levels and lower burden.
Methods
Study Design, Sample, and Setting
This secondary analysis utilizes discharge data from the Family-centered Function-focused Care (Fam-FFC) trial, registered with ClinicalTrials.gov as NCT03046121. The Fam-FCC study integrates families and nurses in a collaborative care model designed to promote cognitive and physical recovery in community-dwelling patients with Alzheimer’s disease and related dementias (ADRD) during hospitalization and the 60-day period following discharge. The model also aims to improve family care partners’ preparedness and experiences. The effectiveness of this intervention for care partners has been previously published (Boltz et al., 2023). The study protocol, which received ethical approval from the university Institutional Review Board in Pennsylvania, United States, was published in detail (Boltz et al., 2018). Written informed consent was obtained from all participants prior to data collection.
A total of 277 care partners were included in this study, recruited from six medical units in three hospitals throughout Pennsylvania. The participants represented all care partners from the parent study who completed the health literacy assessment, forming a census of that subgroup. Inclusion criteria required care partners to (1) be at least 18 years old, (2) be fluent in English or Spanish, and (3) be designated by the patient or a legally authorized representative as the primary care partner with ongoing caregiving responsibilities. Care partner exclusion criteria included those who did not recall at least two words from a three-word memory assessment.
Care receiver inclusion criteria required individuals to (1) be 65 years or older, (2) speak English or Spanish, (3) reside in the community before hospitalization, (4) have a family care partner willing to participate, and (5) meet dementia screening criteria. Dementia status was determined by a Montreal Cognitive Assessment (MoCA) score of ≤ 25 (Nasreddine et al., 2005) and an AD8 Dementia Screening Interview score of ≥ 2 (Galvin et al., 2006). Additionally, cognitive and functional impairment was assessed using a Clinical Dementia Rating Scale (CDR) score between 0.5 and 2.0 (Morris, 1997) and a Functional Activities Questionnaire (FAQ) score of ≥ 9 (Pfeffer et al., 1982). A prior clinical diagnosis of dementia was not required; rather, study eligibility was determined through a rigorous screening protocol using validated cognitive and functional assessment measures (Boltz et al., 2018). Care receiver exclusion criteria included (1) admission from a nursing home, (2) enrollment in hospice care, and (3) a significant neurological condition unrelated to dementia affecting cognition or a major psychiatric disorder.
Procedures
Following consent and confirmation of eligibility, experienced research evaluators, blinded to the intervention assignment, collected data from family care partners within 72 hours of the patient’s hospital discharge. All data were gathered at the care partner’s home through structured interviews, which lasted approximately 20 minutes. The responses were recorded on paper forms and later entered into a secure database (REDCap) (Harris et al., 2009). Care partners provided descriptive characteristics, including education, and completed self-reported measures of health literacy and burden.
Measures
Care partner characteristics included age, sex, race, ethnicity, marital status, and relationship with the patient. Additional factors included employment status, average weekly hours worked outside the home, and whether they cohabited with the patient.
The independent variable, education level, was categorized into three groups: less than high school (low), high school, some college, or trade school (medium), and college degree or above (high).
The outcome variable, care partner burden, was measured using the Short-Form Zarit Burden Interview (ZBI-12), a 12-item tool that evaluates the impact of caregiving on both personal well-being and role responsibilities (Ballesteros et al., 2012). Each item was rated on a scale from 0 (never) to 4 (almost always), with total scores ranging from 0 to 48, where higher scores indicated a greater perception of burden. The internal consistency and concurrent validity of the tool have been demonstrated in prior research (Lin et al., 2017).
The mediator variable, care partner health literacy, was assessed using the Rapid Estimate of Adult Literacy in Medicine-Short Form (REALM-SF), in which participants read aloud and pronounced seven medical terms of increasing in difficulty (Arozullah et al., 2007). Participants received one point for each correctly pronounced word, with total scores ranging from 0 to 7. Higher scores indicated greater health literacy. A score of 0 corresponded to a literacy level below third grade, a score of 1–3 indicated a fourth–sixth grade reading level, a score of 4–6 reflected a seventh–eighth grade reading level, and a perfect score of 7 indicated a ninth grade reading level. Health literacy was analyzed as a continuous variable in this study. The REALM-SF is a validated tool, showing a strong correlation (r = 0.83) with a previously validated word recognition test that measures reading ability (Arozullah et al., 2007).
Data Analysis
Care partner characteristics were summarized using descriptive statistics, with continuous variables reporting means and standard deviations and categorical variables using percentages. Bivariate linear regression analyses were conducted to assess the relationships between care partner education, health literacy, and burden.
The mediation analysis examined whether care partner health literacy mediated the relationship between education level (independent variable) and burden (dependent variable), using a bootstrapping method with 5000 samples. Path coefficients for a, b, c, and c’ were estimated in the mediation model with unstandardized values, as represented in Figure 1. These paths included (1) the a-path, the effect of education on health literacy; (2) the b-path, the effect of health literacy on burden; (3) the c-path, the total effect of care partner education on burden without accounting for health literacy; and (4) the c’-path, the direct effect of care partner education on burden while controlling for health literacy. The indirect effect (a × b) was calculated, and mediation was considered significant if the 95% bias-corrected confidence interval did not include zero. Covariates in the mediation model were the intervention group assignment (control or intervention) and care partner factors: age and sex (Pillemer et al., 2018; Putri et al., 2022; Steinsheim et al., 2023). Analyses were conducted using SPSS and AMOS versions 27 (IBM Corp, Armonk, NY), with statistical significance defined as p ≤ .05. Hypothesized mediation model: Effect of care partner education on burden through health literacy. Note: The a-path represents the effect of the independent variable, care partner education, on the mediator, health literacy. The b-path represents the effect of the mediator, health literacy, on the dependent variable, burden. The c-path indicates the total effect of care partner education on burden without health literacy, while the c’-path reflects the direct effect when health literacy is controlled for in the model.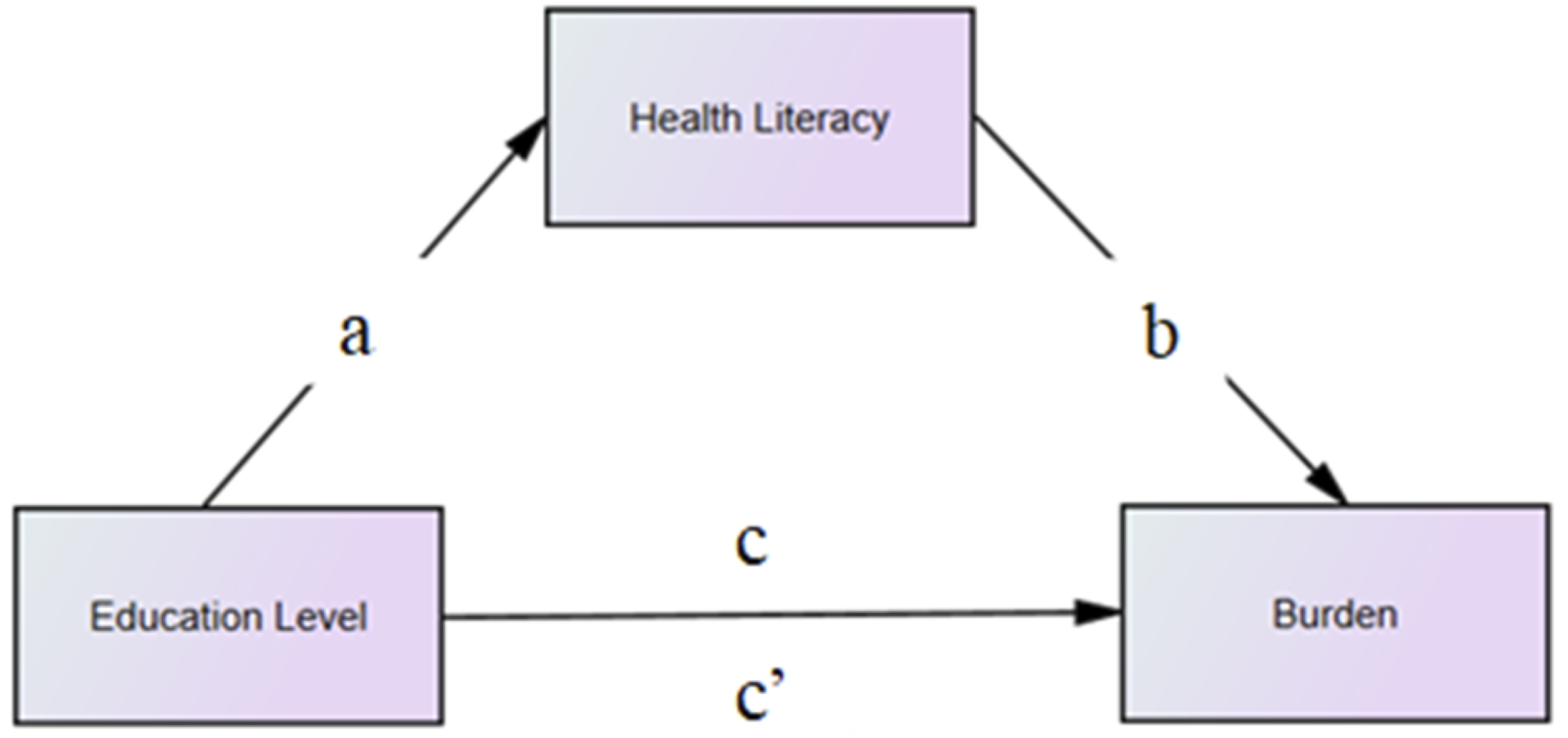
Results
Characteristics of the Study Sample (N = 277).
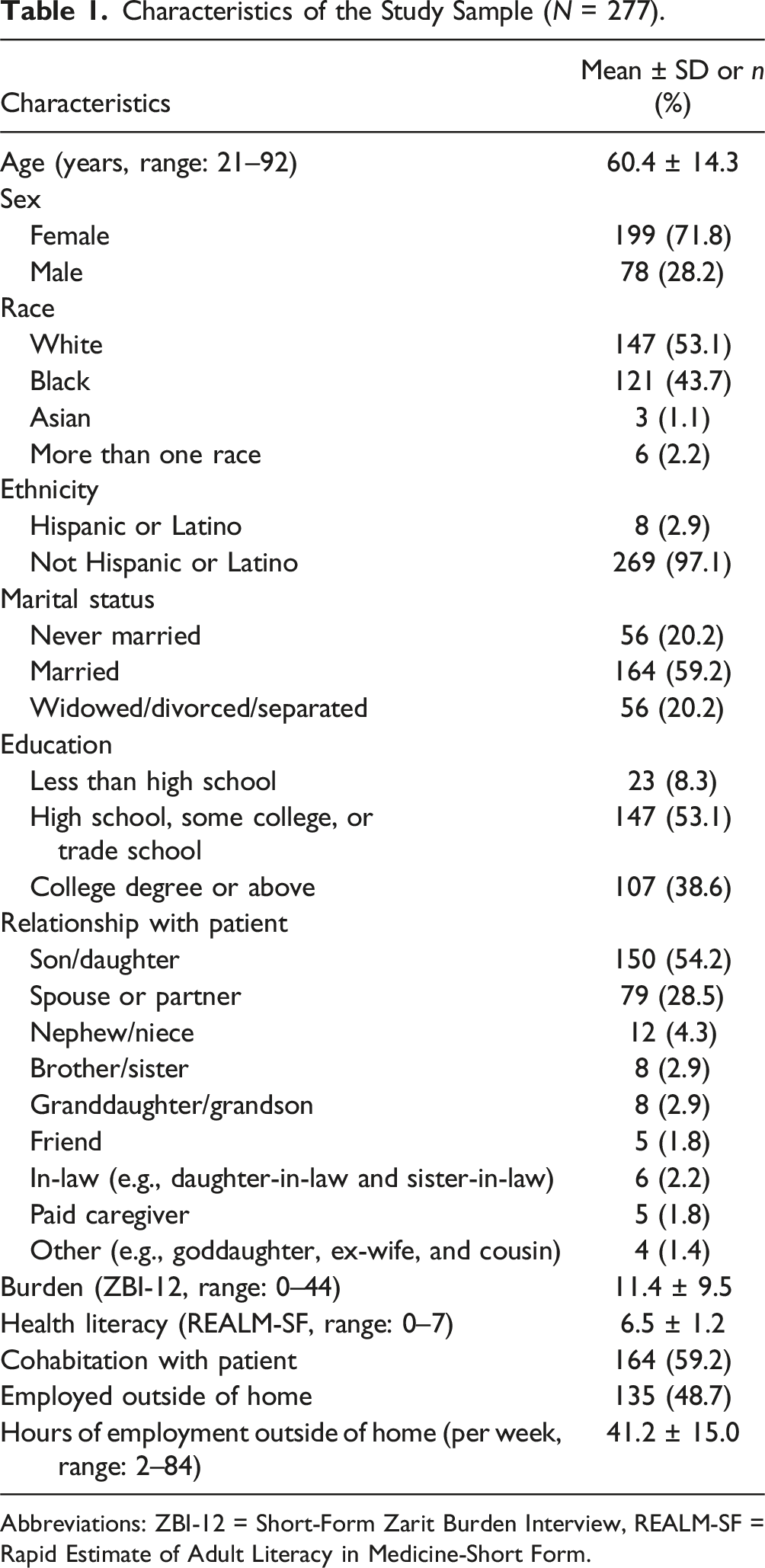
Abbreviations: ZBI-12 = Short-Form Zarit Burden Interview, REALM-SF = Rapid Estimate of Adult Literacy in Medicine-Short Form.
Care Partner Health Literacy Across Education Levels.
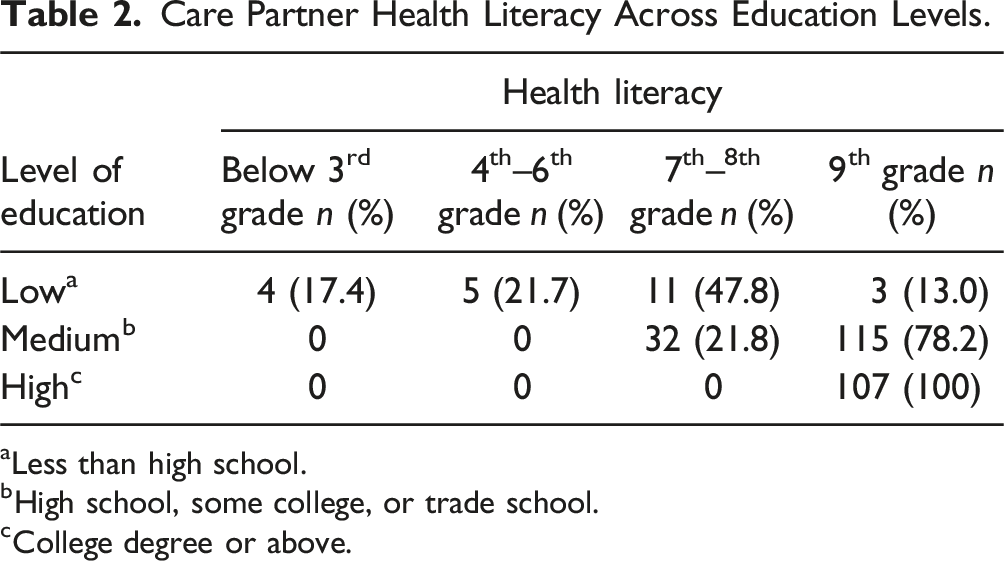
aLess than high school.
bHigh school, some college, or trade school.
cCollege degree or above.
Bivariate Linear Regression Results for Care Partner Education, Health Literacy, and Burden.
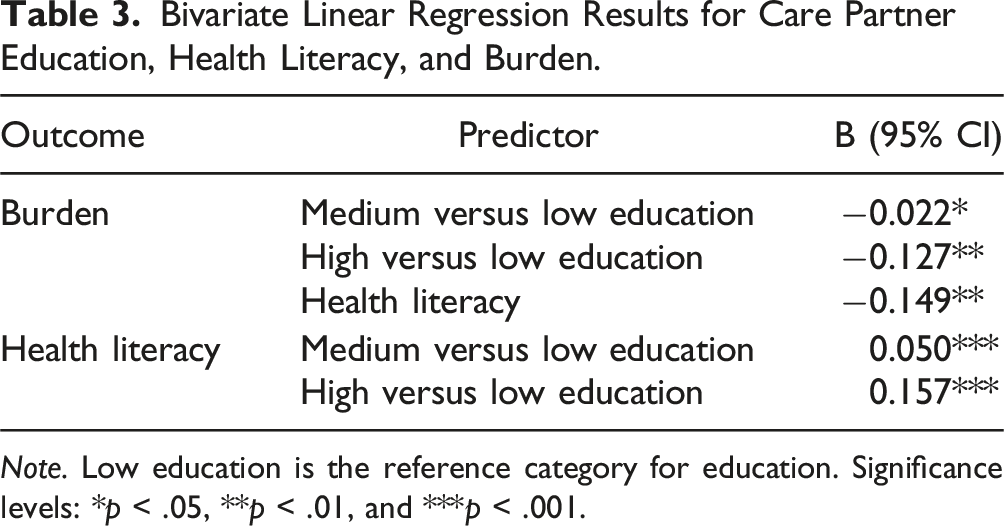
Note. Low education is the reference category for education. Significance levels: *p < .05, **p < .01, and ***p < .001.
Mediation Model Analysis for Care Partner Education, Health Literacy, and Burden (N = 277).
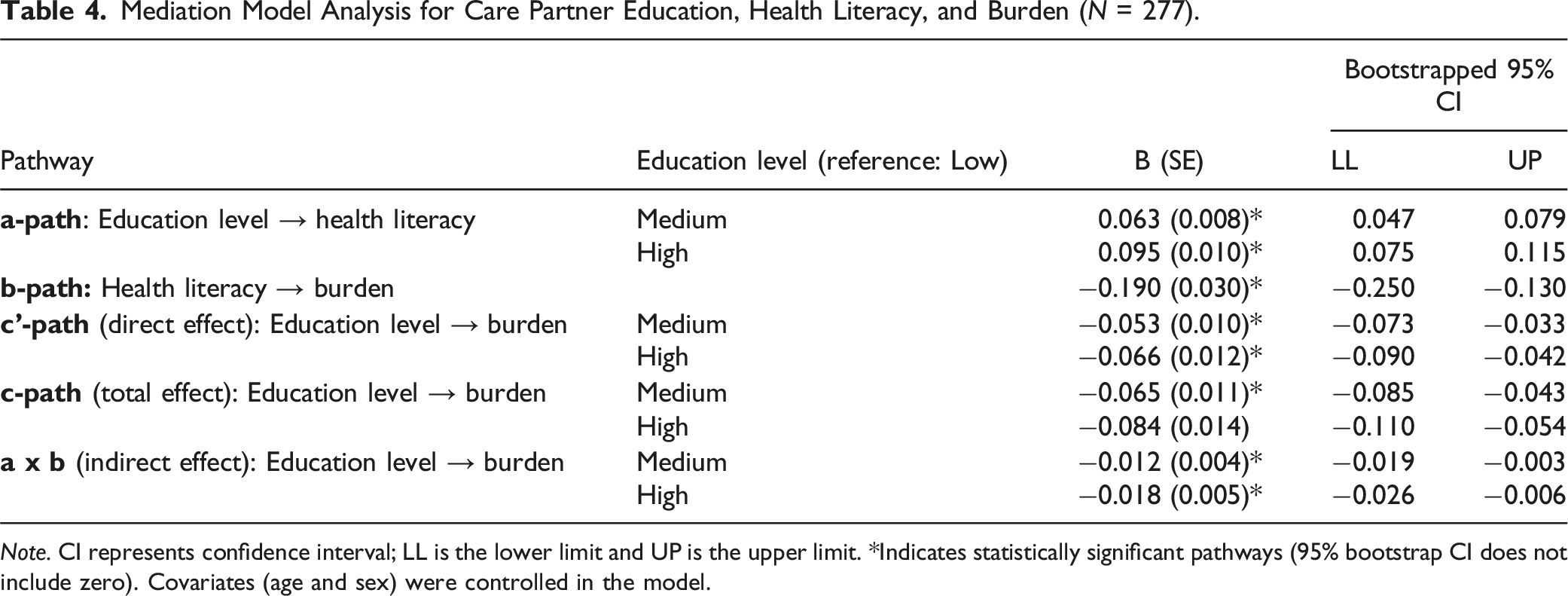
Note. CI represents confidence interval; LL is the lower limit and UP is the upper limit. *Indicates statistically significant pathways (95% bootstrap CI does not include zero). Covariates (age and sex) were controlled in the model.
The total effect (c-path) of education on burden was significant, with medium (B = −0.065, p = <.001) and high (B = −0.084, p = <.001) education levels associated with lower care partner burden. Including health literacy in the model reduced the direct effect (c’-path) of education on burden, though the relationship remained statistically significant (medium education: B = −0.053, p = .015; high education: B = −0.066, p = .006).
The indirect effect (a × b) of education on burden through health literacy was significant for both medium education (B = −0.012; 95% CI = −0.019, −0.003) and high education (B = −0.018; 95% CI = −0.026, −0.006), indicating partial mediation. These mediation effects accounted for 18.5% of the total effect for medium education level and 21.4% for high education level, suggesting that higher education levels were associated with better health literacy, which in turn was linked to lower care partner burden.
Discussion
The present study examined the role of care partner health literacy in the relationship between education level and burden at hospital discharge. Our hypothesis was partially supported, showing that higher care partner education levels were associated with lower burden, with this relationship partially mediated by care partner health literacy. The findings indicate that health literacy plays a critical role in how care partners interpret discharge instructions, communicate with hospital staff, and make decisions about managing care at home. These demands extend beyond comprehension alone and require care partners to apply information in real time, often under stress and with limited support. For those with lower education, limited health literacy may constrain their capacity to ask questions, advocate for the patient, or navigate care systems, contributing to greater burden. These insights support the design of discharge processes that promote not only informational access but also confidence and preparedness in the caregiving role, which may help reduce burden experienced during this transition.
The results align with prior research showing that higher education levels are linked to lower burden (García-Martín et al., 2023; Putri et al., 2022; Teahan et al., 2021). This study also found that higher health literacy is associated with lower burden, consistent with previous research involving care partners in different settings (Häikiö et al., 2020; Yuen et al., 2018). Further supporting this association, international studies using various methodologies have linked health literacy to improved decision-making, health-promoting behaviors, and overall well-being across diverse populations, including older adults, nurses, and hospitalized patients (Khammarnia et al., 2018; Mehralian et al., 2023; Yusefi et al., 2019; Yusefi et al., 2022). While these studies highlight the broader impact of health literacy on healthcare engagement and well-being, this study adds a novel contribution by identifying health literacy as a pathway through which educational disparities affect care partner burden specifically during hospital discharge. The findings underscore the need for interventions that address disparities in education and literacy to reduce care partner burden during this critical transition. Future research should use a longitudinal approach to examine the mediating role of care partner health literacy on the relationship between education and burden over time, beyond the immediate hospital discharge period.
Health literacy demonstrated a modest mediating effect (18.5% for medium education and 21.4% for high education) on the relationship between care partner education and burden, highlighting its role as one pathway which education influences care partner burden. However, this mediation effect also suggests that other factors may influence the relationship between care partner education and burden during hospital discharge. Care partner factors, including quality of life, emotional well-being, and the time spent managing medical information or coordinating care, may further impact this relationship (Häikiö et al., 2020; Jansen et al., 2018; Li et al., 2020; Lin et al., 2019; Putri et al., 2022). Patient factors, such as dementia severity, behavioral and psychological symptoms, and declines in physical function during hospitalization, could also contribute to this relationship (Kuzmik, 2023; Kuzmik et al., 2024; Lorini et al., 2023; Putri et al., 2022; Steinsheim et al., 2023). Additionally, aspects of the hospital environment, such as the quality of communication with healthcare providers and the availability of discharge planning support, may play a crucial role (Gaugler et al., 2023; Jansen et al., 2018). Thus, future research should examine contextual factors to provide a more comprehensive understanding of the relationship between care partner education, health literacy, and burden at hospital discharge.
Although multiple factors contribute to care partner burden, our findings also highlight the important role of health literacy in shaping the dementia caregiving experience at hospital discharge. Care partners with lower education and limited health literacy may have difficulty understanding treatment plans, managing post-discharge care, and addressing the care receiver’s behavioral symptoms, all of which contribute to greater stress and burden (Gaugler et al., 2023; Jansen et al., 2018; Putri et al., 2022). These challenges suggest that health literacy plays a significant role in how effectively care partners engage with healthcare providers, navigate care transitions, and support both the patient and their own well-being. Recognizing these caregiving difficulties can inform strategies to enhance dementia care partner education and improve health outcomes during this critical transition.
The study findings highlight the need for targeted interventions to improve health literacy among care partners, particularly those with lower education levels. Hospitals should integrate health literacy assessments into discharge planning to identify care partners at greater risk of burden and provide tailored, accessible support. Practical strategies informed by these findings include simplifying discharge instructions using plain language and visual aids, offering structured training programs to enhance caregiving skills, and implementing caregiver-centered communication tools to better prepare care partners for their roles. Applying these approaches into post-discharge care plans may reduce caregiving burden and improve both care partner well-being and patient outcomes.
Strengths and Limitations
This study provides valuable insights into the mechanisms connecting dementia care partner education, health literacy, and burden during a critical yet underexplored transition period. Focusing on a vulnerable population, it is among the few studies to explore this topic and included a sizable cohort of dementia care partners.
This research was limited by the cross-sectional design, which restricts the ability to establish causality. The sample primarily consisted of non-Hispanic White and Black care partners, limiting generalizability to other populations. Future research should examine additional potential mediators, such as social support and emotional resilience, to fully understand the complex interplay between care partner education, health literacy, and burden.
Conclusion
By identifying health literacy as a partial mediator in the relationship between care partner education and burden, this study underscores the importance of addressing education and literacy disparities to support care partners. Tailored interventions that enhance health literacy, such as simplified discharge instructions, care partner training programs, and access to clear communication tools, may serve as key strategies for reducing burden during hospital discharge. Future research should prioritize diverse samples and geographic contexts to ensure these findings are relevant to a broad range of care partner populations.
Footnotes
Acknowledgments
The authors would like to thank the participants for their contributions to this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The parent study was supported by the National Institute of Aging (NIA) under grant R01AG054425. The contents of the article are solely the responsibility of the authors and do not necessarily represent the official views of the NIH/NIA.