
Abstract
We evaluate the feasibility, acceptability, and potential effect of an acceptance and commitment therapy (ACT) tele-counselling program offered by a non-profit organization for care partners of persons with dementia (PWD) in a bilingual rural province. Thirty participants enrolled and one withdrew. Intervention group participants (n = 14) received 6–8 individual counselling sessions via telephone, videoconference, or text. Control group participants (n = 15) received two general support telephone calls from Alzheimer Society staff. Results indicated limited recruitment and adherence (completion) feasibility, although acceptability and usability were high. Significant within-group reductions in anxiety and stress symptoms (DASS-21) and burden (ZBI-12) in the intervention group were demonstrated, although the groups were not significantly different post-intervention. ACT tele-counselling may increase care partner access to mental health services, improve symptoms, and alleviate strain on Alzheimer Society staff, though a larger trial is needed with a longer duration, multiple ACT therapists, and additional recruitment efforts. Protocol registered at https://clinicaltrials.gov/study/NCT05385458.
Keywords
• A tailored ACT tele-counselling (phone modality) intervention demonstrates acceptability and preliminary efficacy at reducing anxiety, stress, and burden among Anglophone and Francophone care partners of persons with dementia. • Tele-counselling at no cost increases access for care partners of persons with dementia in rural areas. • Feasibility is limited by short study timelines (12 months or less) and lack of staff in minority-language, remote communities, and single-therapist availability. • Therapists working with care partners should consider offering ACT remotely to increase service availability. • Having a structured, therapist-led program within care partner organizations may increase accessibility for care partners and reduce emotional strain on staff. • Future studies should include multiple ACT-trained therapists and extend study timelines to 2–3 years and ensure staff are embedded in local communities to promote recruitment and enable program completion.What this paper adds
Applications of study findings
Introduction
There is a critical need for effective and accessible mental health services for care partners of persons living with dementia (PWD). Healthcare systems worldwide continue to rely heavily on family/friend care partners to provide unpaid care, although up to 75% of care partners experience depression or anxiety, and 44% experience distress related to caregiving (Omranifard et al., 2018). Unfortunately, barriers can make accessing mental health services difficult for care partners, particularly in rural and minority-language communities. Policymakers in Canada are calling on researchers and clinicians to leverage technology to improve equitable access to mental health services within urban and rural areas. Acceptance and commitment therapy (ACT) has shown promising results in improving mental health outcomes and may provide a feasible solution to increase access; however, no studies of ACT with care partners have been completed in Canada to date (Gloster et al., 2020).
While caregiving can be deeply rewarding, it is also associated with burden, stress, suicidal thoughts, and complicated grief (Omranifard et al., 2018). ACT helps individuals manage stressors by fostering acceptance, mindfulness, commitment, and behavior change, which enhance psychological flexibility and coping skills (Atefi et al., 2024). Psychological flexibility refers to staying present in the moment, accepting thoughts and emotions, and pursuing meaningful activities despite distress (Hayes et al., 2012; Plys et al., 2023). Increasing psychological flexibility reduces burden and depression, helping care partners manage losses related to dementia that are unchangeable or incurable (Plys et al., 2023). Unlike cognitive behavioral therapy (CBT), which challenges illogical thoughts, ACT encourages acceptance of logical yet distressing thoughts, emotions, and situations making it particularly suited for care partners of PWD.
Researchers from Europe and the United States (USA) have consistently demonstrated reduced symptoms of depression, anxiety, and stress in ACT studies (Gloster et al., 2020). However, most randomized control trials (RCTs) include in-person, face-to-face modalities which are often inaccessible in practice due to barriers such as caregiving responsibilities, rural isolation, and mental and dementia stigma (Giebel et al., 2022; Ye et al., 2023). Remote-delivered psychotherapy (e.g., text, telephone, and videoconference) can help overcome barriers and shows similar effects to in-person therapy (Lattie et al., 2022). Evidence for feasibility and acceptability of remote and in-person ACT interventions has been generated in the USA and Europe (Atefi et al., 2024; Ferreira et al., 2023; Scott et al., 2023). Generalizability in the Canadian context may be limited, however.
Hence, this study evaluates the acceptability, feasibility, and potential effect of the first ACT tele-counselling program launched in Canada by the Alzheimer Society of New Brunswick (AS), a branch of a national non-profit organization. New Brunswick is the only bilingual province in Canada with two official languages and has one of the most rapidly aging populations in the country. Harsh weather and rugged terrain limit transportation for 6 months of the year, make internet connectivity inconsistent, and create additional barriers to accessing mental health services (de Moissac & Bowen, 2017). Evidence is needed to inform a larger trial and will be useful to policymakers and health/social care providers seeking to implement remote mental health services including ACT.
Methods
Design
A mixed-methods, pilot feasibility, parallel RCT design was used (Creswell & Creswell, 2022). Participants were randomly assigned in a 1:1 ratio to ACT tele-counseling (intervention) or usual care (control). Recruitment followed a rolling basis, initiating the intervention or usual care between May and October 2023.
An Advisory Committee with five care partners of PWD collaborated with researchers on the study design and procedures. The principal investigator (PI), research assistant (RA), therapist, and participants were aware of group allocation. Two researchers blinded to group assignments completed randomization and outcome analyses. The PI had no direct contact with participants. This research was supported by a mental health innovation grant from Mental Health Research Canada and Research NB approved by the University of New Brunswick Research Ethics Board (Certificate #2022-055) and registered at https://clinicaltrials.gov/study/ NCT05385458. The CONSORT reporting guideline was followed (Schulz et al., 2010).
Participants
Inclusion criteria were (i) aged 19 years or older; (ii) French or English-speaking and reading; and (iii) providing unpaid emotional, physical, social, or financial care to a family member/friend with Alzheimer’s disease or a related dementia (diagnosis not required). Exclusion criteria were self-reported acute mental illness (e.g., schizophrenia) and/or severe distress scores on two or more DASS-21 subscales: depression (>21), anxiety (>14), and stress (>25) (Lovibond & Lovibond, 1995).
Participants were recruited through the Alzheimer Society (AS) and public advertisements. Interested individuals contacted the AS directly or were referred by AS staff/ volunteers. Initial eligibility screening was conducted by the RA. Participants completed the DASS-21 survey to confirm eligibility and provide baseline data. One researcher assessed DASS-21 scores for eligibility, and a second verified the results. Participants were compensated with a $25 gift card at both baseline (Time 1) and follow-up (Time 2). Interview participants received an additional $25. The study aimed to recruit 80 participants to allow a 25% attrition rate and a final sample of 40 participants, appropriate for pilot feasibility studies (Creswell & Creswell, 2022; Teresi et al., 2022).
Randomization
Eligible participants were randomly assigned to the ACT intervention or usual care group using a block randomization sequence (blocks of six) generated by an external researcher. The RA confirmed eligibility, managed allocation procedures, and informed participants of their group assignment via phone or email. Contact details were securely shared with the ACT therapist or AS staff for scheduling or usual care.
Intervention
ACT group participants received 6–8 individual tele-counseling sessions over 16–24 weeks using their preferred delivery method (videoconference, phone, or text), with sessions lasting 45–60 minutes. Sessions were audio-recorded to evaluate therapist fidelity to the intervention. The intervention was delivered by a bilingual licensed counseling therapist with knowledge of dementia, caregiving, and ACT employed by the AS. The therapist followed a standardized process, including reviewing the previous session, addressing participant concerns, and covering key ACT domains such as fostering acceptance and clarifying values (O’Neil et al., 2019).
Usual care group participants received two phone calls from AS staff, reflecting the standard services provided to new clients. Calls were conducted at week 1 and 16–20 weeks later and included AS service information, educational resources, and emotional support. Once completed, usual care group participants could participate in the ACT program.
Data Collection
Quantitative data were collected at baseline (Time 1) and 16–24 weeks later (Time 2) using self-reported questionnaires administered through LimeSurvey or by mail. Administrative data, such as attendance, were recorded by the therapist, AS staff, and the RA. Post-intervention qualitative data were gathered through participant interviews and an open-ended electronic survey distributed to AS staff. Demographic information was self-reported by participants.
Measures
Demographics
Participant characteristics were collected such as age, gender, race/ethnicity, preferred language, geographic region or residence, level of education, income, and previous/current use of mental health or support services. Similar care recipient data was collected as well as data to describe the caregiving relationship and activities, including relationship to the PWD, living situation, weekly hours caregiving, and estimated time since onset of dementia symptoms.
Feasibility, Fidelity, and Acceptability
Feasibility was indicated by recruitment and enrollment rates and participant and therapist fidelity (i.e., adherence) to the intervention protocol. Therapist fidelity was measured using an adapted version of the ACT-Fidelity Measure (O’Neil et al., 2019), achieving 86% inter-rater reliability between the therapist and a graduate student external to the study. The original 25-item ACT-FM demonstrated evidence for inter-rater reliability (ICC = 0.73, 95% CI, 0.6–0.93) in field tests (O’Neil et al., 2019). Acceptability was evaluated through retention rates, enrollment, and retention of participants with varying demographics (e.g., language, gender, and geographic region), and satisfaction with the intervention. Satisfaction and usability questionnaires were only administered to participants in the intervention group to understand acceptability of the ACT intervention specifically. All other questionnaires were completed by participants in both groups.
Client Satisfaction Questionnaire (CSQ-8)
The CSQ-8 is an eight-item tool designed to assess client satisfaction with services received (Attkisson & Greenfield, 1994). Each item evaluates different aspects of satisfaction, including how well the service met the client’s needs, the quality of service provided, and the likelihood of recommending the service to others. Responses are scored on a 4-point Likert scale (e.g., 1 = Poor to 4 = Excellent). Total score ranges from 8 to 32, with higher scores indicating greater satisfaction. Internal consistency across studies is α = .85 (Attkisson & Greenfield, 1994). Current study internal consistency was α = .89.
System Usability Scale (SUS)
The SUS is a 10-item questionnaire designed to evaluate the system/service usability with negative and positively worded items scored on a 5-point Likert scale (1 = Strongly Disagree to 5 = Strongly Agree) (Brooke, 2013). Responses are transformed into scores ranging from 0 to 100, with higher scores indicating better usability. Average usability is 68 and ≥ 80 is considered excellent (Lewis, 2018).
The SUS has evidence for internal consistency (typically α > .85) and concurrent validity when compared with other usability measures (Lewis, 2018). The Advisory Committee piloted the SUS and recommended clarifying terms such as “system” and “product.” Item-wording was adjusted to reference the tele-counselling modalities, for example, “I thought the videoconference method was easy to use”). Current study reliability was α = .84.
Potential Effect
Depression, Anxiety, and Stress Scale (DASS-21)
The DASS-21 is a 21-item measure designed to assess the severity of symptoms related to depression, anxiety, and stress (Lovibond & Lovibond, 1995). Participants rate symptom frequency in the past week on a 4-point scale (0 = Never to 3 = Almost Always). Summative subscale scores are calculated with higher scores indicating greater levels of distress (α = .78–.89) (Vahabi et al., 2022). Reliability for the three subscales were .92, .87, and .83.
Zarit Burden Interview—Short Version (ZBI-12)
The ZBI-12 is a 12-item tool measuring caregiver burden across three domains: caregiving impact on the caregiver’s life, feelings of guilt, and caregiving role frustration or embarrassment (Bédard et al., 2001). Statements such as “You feel stressed between caring for your relative and trying to meet other responsibilities” are rated on a 5-point Likert scale (0 = Never to 4 = Nearly Always). Reliability has been demonstrated (α = .87) and concurrent validity (Rho = .96 with the long-version) (Higginson et al., 2010). Total scores are summed, with higher scores reflecting greater perceptions of burden. In the current study α = .91.
Acceptance and Action Questionnaire (AAQ-2)
The AAQ-2 is a seven-item scale designed to assess psychological flexibility; the core mechanism and standard outcome measure of ACT (Hayes et al., 2012). Participants rate items like “Emotions cause problems in my life” on a 7-point scale (1 = Never True to 7 = Always True). Total scores are calculated by summing item responses, with higher scores indicating greater psychological inflexibility and experiential avoidance (Bond et al., 2011; Monestès & Villatte, 2011). Internal consistency (α = .84–.91) and test-retest reliability have been demonstrated (Bond et al., 2011). Reliability in the current study was α = .92.
Engagement in Meaningful Activities Survey (EMAS)
The EMAS is a 12-item measure that evaluates the extent to which participants’ daily activities align with their values and provide a sense of purpose (Goldberg et al., 2002; Lacroix et al., 2018). Statements like “The activities I do reflect the kind of person I am” are rated on 5-point scale (1 = Never to 5 = Always). Total scores are summed, with higher scores reflecting greater engagement in meaningful activities. The EMAS measures value-driven behavior (i.e., living according to one’s values), a goal of ACT. For care partners of PWD, meaningful activities can mitigate caregiving-related stress, increase quality of life, and promote well-being despite living with losses that are unchangeable as in dementia (Gloster et al., 2020). Goldberg et al. (2002) reported internal consistency (α = .86–.92) and validity. Reliability in the current study was α = .87.
Statistical Analysis
Quantitative data was analyzed using SPSS Statistics Version (29). Descriptive statistics were calculated for variables used to evaluate program feasibility, acceptability, and fidelity. Baseline differences in demographic and caregiving characteristics between control and intervention groups were examined using chi-square tests.
Given the pilot/feasibility nature of the study and resultant small sample size, we used separate within-groups, paired-sample t-tests to test for changes in outcome variables (i.e., DASS-21, ABI-12, AAQ-II, and EMAS) from pre- to post-intervention in intervention and usual care conditions. Independent samples t-tests were run to test for significant differences between conditions at post-intervention. Missing values analysis revealed 1.80% of data was missing at random. In line with suggestions from (Tabachnick & Fidell, 2019), who note that method of replacing missing data when <5% of the data does not dramatically alter analytic outcomes, missing data points were replaced using mean substitution. To assess whether relevant variables were correlated with intervention outcome, we conducted a series of correlations within intervention conditions. Change scores for each outcome variable were calculated by subtracting pre-intervention scores from post-intervention scores, and then correlated with demographic/caregiving variables.
Qualitative Analysis
Participant and staff feedback were analyzed using content analysis as outlined by Sandelowski (2010). To enhance credibility and dependability, two researchers independently analyzed three interview transcripts and open responses from two surveys, organizing the data and applying preliminary codes (i.e., labels). All researchers then met together for researcher triangulation to review and agree upon a coding framework with disagreements settled through discussion (Creswell & Creswell, 2022). Two researchers then completed coding all data using the agreed upon framework meeting regularly to discuss potential patterns and themes. Once complete, a descriptive summary of findings was generated, reviewed, and agreed upon by all researchers (Creswell & Creswell, 2022).
Results
Participant Characteristics
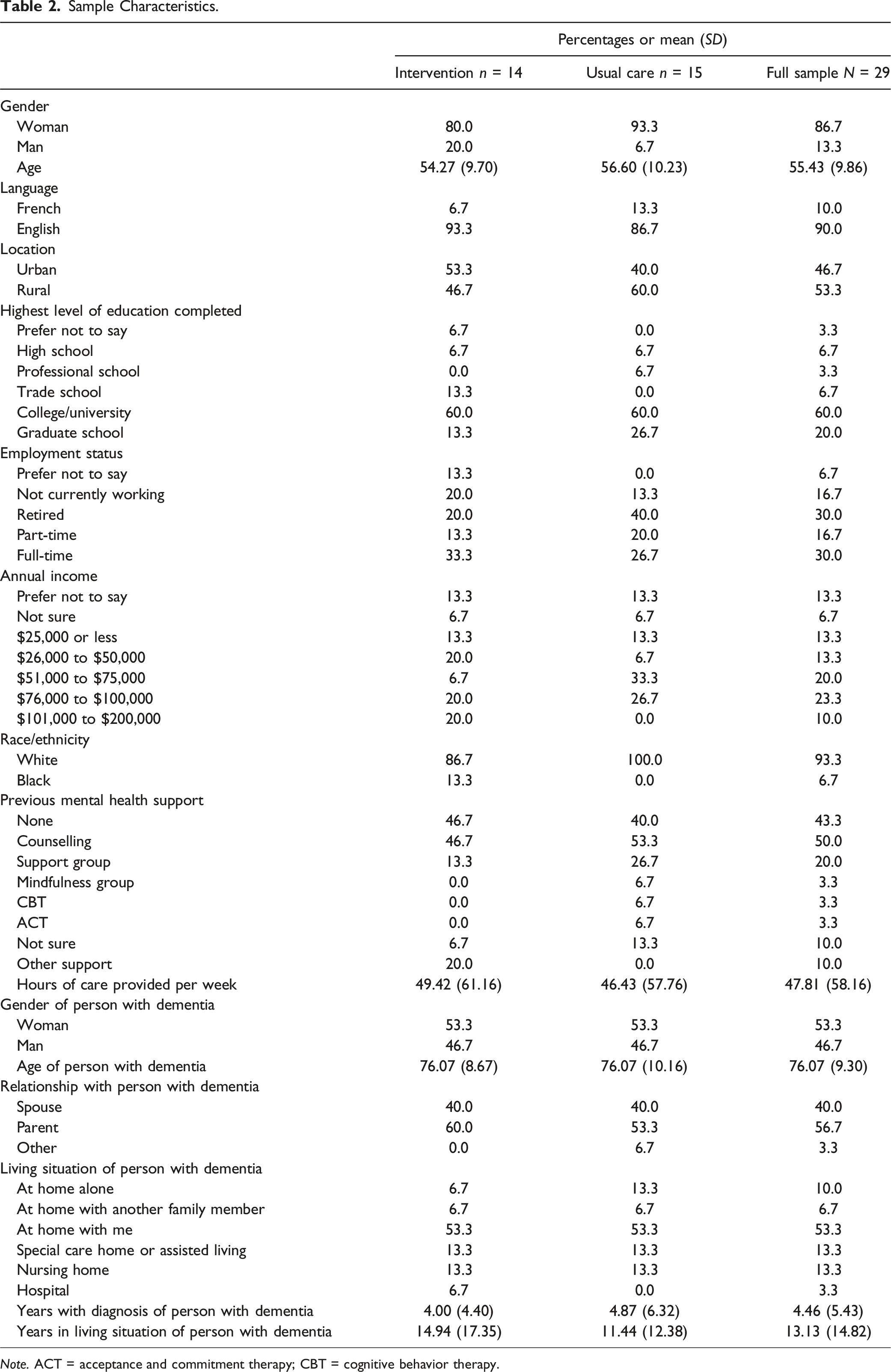
Thirty participants enrolled in the study. One participant withdrew from the ACT group after meeting with the therapist and mutually agreeing that trauma-focused counseling was required before ACT (see Figure 1). Data from 29 participants who completed both Time 1 and Time 2 data collection were analyzed. Participants were predominantly White (93.3%) women (86.7%), with a mean age of 55.43 years (SD = 9.86) (see Tables 1 and 2). Chi-square tests confirmed that randomization effectively balanced the intervention and usual care groups, with no significant differences in demographics or caregiving variables. Participant flow. The Consolidated Standards of Reporting Trials [CONSORT] flow diagram. Outcome Indicators. Sample Characteristics. Note. ACT = acceptance and commitment therapy; CBT = cognitive behavior therapy.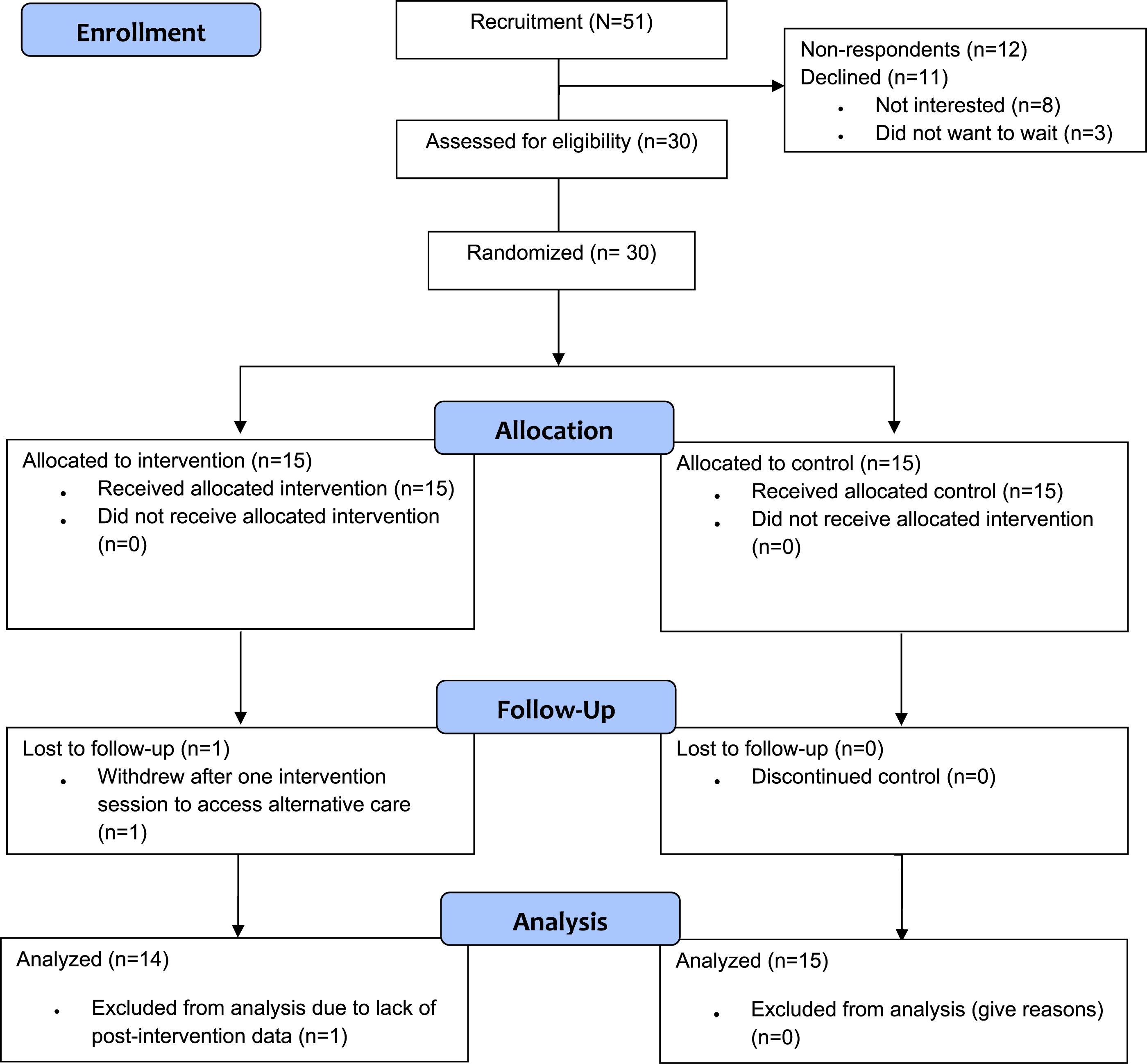

Within- and Between-Groups T-Tests for Study Outcome Variables.
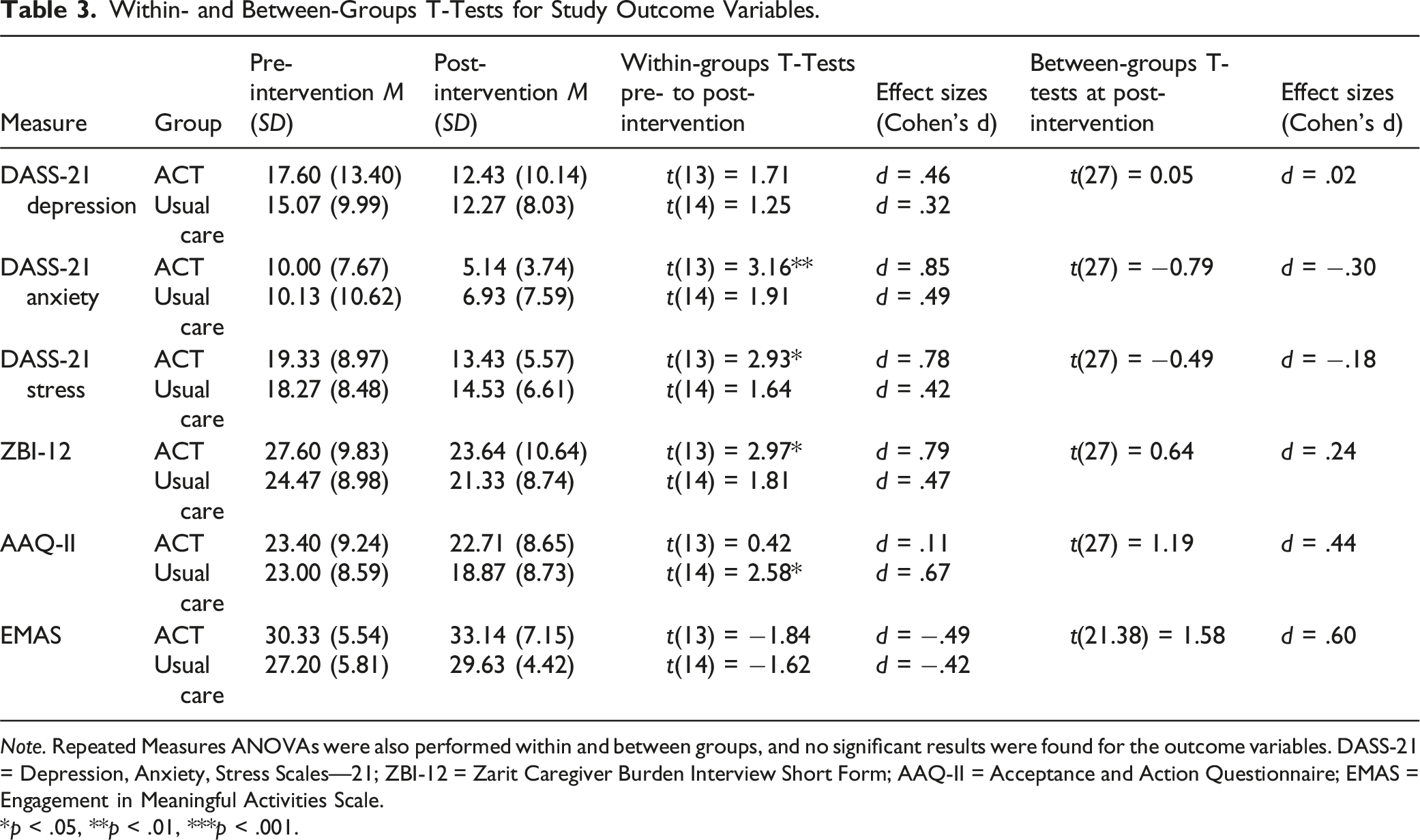
Note. Repeated Measures ANOVAs were also performed within and between groups, and no significant results were found for the outcome variables. DASS-21 = Depression, Anxiety, Stress Scales—21; ZBI-12 = Zarit Caregiver Burden Interview Short Form; AAQ-II = Acceptance and Action Questionnaire; EMAS = Engagement in Meaningful Activities Scale.
*p < .05, **p < .01, ***p < .001.
Feasibility, Fidelity, and Acceptability
During the 6-month rolling recruitment period, 51 care partners consented to share contact information with researchers through the AS, were referred to the ACT program, or contacted the AS after seeing a study advertisement. Nine did not respond after 2 weeks. Eleven declined via email, citing lack of interest (n = 8) or preference to start ACT immediately (n = 3) rather than risk placement in the wait-list control group. In total, 30 care partners met with the RA, were screened, and enrolled. Recruitment feasibility was limited, with a 58.8% (n = 30/51) recruitment rate, below the 80-participant target. The 73.2% (n = 30/41) enrolment rate moderately supports feasibility, despite not meeting the 80% target.
Therapist fidelity criteria were met in 84% of ACT sessions, demonstrating feasibility in addressing ACT domains for care partners of PWD (O’Neil et al., 2019). Among participants randomized to ACT, 62.5% completed the target 6–8 sessions within the study timeline. However, 35.7% (n = 5) who enrolled closer to the grant end date (October 2022) did not complete all sessions on time, finishing after Time 2 data collection.
Acceptability was high, with a 97% retention rate (n = 29) and over 50% of participants from rural areas. Most geographic regions were represented (n = 7/8, 87.5%), except for one distant Francophone community. However, targets for geographic (100%) and Francophone (30%) enrolment were not met. Participants reported high satisfaction with ACT tele-counseling (CSQ-8 mean = 3.67/4.0, SD = 0.46) (Attkisson & Greenfield, 1994), with 67% “very satisfied” and 33% “mostly satisfied.” Additionally, 75% would definitely recommend the program. The mean SUS usability score was 95.2%, indicating excellent usability, and 67% strongly agreed they would continue using technology for ACT access.
Potential Effect
Paired-sample t-tests within the intervention group revealed significant decreases in DASS-21 anxiety scores, t(13) = 3.16, p = .008; stress scores, t(13) = 2.93, p = .012; and ZBI-12 scores, t(13) = 2.97, p = .011. In contrast, participants in the usual care group experienced a significant worsening of AAQ-II scores from pre- to post-intervention, t(14) = 2.58, p = .022. Independent samples t-tests comparing post-intervention scores between the ACT and usual care groups did not identify significant differences across outcome variables.
We conducted sensitivity analyses excluding participants who completed less than six intervention sessions. These analyses included nine participants in the intervention condition. Paired-sample t-tests within the intervention group revealed only a significant decrease in DASS-21 anxiety scores, t(8) = 3.55, p = .008. As in the primary analysis, independent samples t-tests comparing post-intervention scores between the ACT and usual care groups did not result in significant differences across outcome variables.
Within the intervention group, correlation analyses showed that most variables (e.g., participant age and years since dementia diagnosis) were not significantly associated with outcome variable changes. However, the total number of intervention minutes was significantly correlated with changes in DASS-21 depression scores (r = −0.56, p < .05) and anxiety scores (r = −0.62, p < .05). These findings suggest that greater intervention exposure is linked to larger reductions in symptoms of depression and anxiety.
Perceptions of the Intervention
All ACT participants were invited to participate in telephone interviews, and eight agreed. These participants had an average age of 53.8 years (SD = 12.94, range = 29–70), were predominantly women (87.5%), lived in rural areas, and provided between 5 and 35 hours of care per week, primarily for a parent with dementia (62.5%). Additionally, five AS staff members who supported recruitment or conducted general support calls were invited to complete an open-ended survey, with three responding.
Acceptability
Participants described the ACT program as convenient, flexible, and particularly valuable for those in rural areas. One participant noted, “The telephone was definitely the right choice…just the convenience. I loved not having to miss work or arrange transportation” (ACT09). The remote delivery mode was perceived as reducing barriers, such as finding care for the PWD. However, some challenges were reported, including interruptions during sessions due to caregiving duties and the lack of visual cues during phone sessions: “That’s the most challenging part…over the phone…you don’t have the body language feedback” (ACT05). Additionally, some participants struggled to find a private space for sessions, with one explaining, “I’d either go to my car or find a quiet spot at work” (ACT23).
Perceived Benefits
Participants reported substantial mental health improvements, emphasizing skill-building and shifting perspectives. One participant shared, “I was struggling… but I’m a different person now. I’m physically and mentally so much better… [ACT] was hugely beneficial for me” (ACT14). Participants also valued the education provided on grief and personal reactions. Many highlighted improvements in empathy, with one noting, “[I could] look at this from somebody else’s point of view” (ACT01). Participants felt that improved mental health had a positive effect on the individuals they cared for, as one stated, “It made me realize [that] if I didn’t look after myself, I couldn’t look after my husband” (ACT29).
AS staff perceived the program reduced emotional strain in care partners, and benefited staff, and the healthcare system. Staff shared that care partners’ mental health needs were sometimes beyond the staff’s capacity and having the therapist-led program for referral to reduced staff’s moral/emotional distress. They also noted that the program helped extend the time care partners could manage caregiving at home, potentially reducing strain on the healthcare system.
Perceived Challenges
Participants and staff identified several challenges in implementing and accessing the ACT tele-counseling program. One of the most frequently mentioned difficulties was scheduling conflicts, as many care partners struggled to find uninterrupted time for therapy sessions while managing their caregiving responsibilities. Some participants also found it challenging to secure a private space for phone-based sessions, often resorting to taking calls in their cars or finding a quiet spot at work. Another challenge was the lack of visual interaction during phone sessions, which some participants felt made it harder to connect with the therapist. Without visual cues, it was sometimes difficult to gauge emotions or responses, which are integral to therapeutic conversations. Additionally, staff reported that limited therapist availability led to long wait times, sometimes delaying participants’ access to the intervention.
Barriers to Participation
Several barriers directly impacted recruitment and participation. A key issue was the absence and/or limited number of AS staff in Francophone communities, which resulted in minimal program outreach and recruitment support in those regions. A participant emphasized the need for greater outreach, stating, “We need to get the word out” (ACT09). This lack of presence may have contributed to lower enrollment among Francophone participants. Additionally, misconceptions about program eligibility created further barriers. Some care partners mistakenly believed they needed a formal dementia diagnosis for their loved one to qualify for participation, while others assumed the program was designed for the person with dementia rather than for caregivers themselves. One participant noted, “People think they need to suffer on their own until there’s some kind of official diagnosis” (ACT14). Access to technology and reliable connectivity also played a role in participation barriers. While most participants found phone-based therapy convenient, some experienced unreliable phone or internet service, particularly in rural areas. This occasionally disrupted sessions or made it difficult for participants to maintain consistent engagement.
Discussion
This study aimed to evaluate the feasibility and potential effect of ACT tele-counseling for care partners of PWD in a rural, bilingual Canadian province. Key findings included evidence for acceptability and potential effect of ACT tele-counselling among Anglophone and Francophone care partners in a rural Canadian context; reduced barriers to accessing mental health services; and feasibility challenges of recruitment and program completion important for informing future research and program expansion.
Recruitment was limited by the 6-month study timeline, constrained by grant funding, and the summer recruitment period. Despite enrolling participants from 7/8 regions in both official languages, fewer Francophone care partners (target: 30%) participated, and none were recruited from a large Francophone region lacking an AS Regional Coordinator—a key referral role. Achieving a diverse, representative sample remains challenging. Minority groups (e.g., language, culture, and ethnicity) often face healthcare access barriers, leading to service and research avoidance (de Moissac & Bowen, 2017; Garnett & Northwood, 2022; Gleibel et al., 2022). According to Garnett and Northwood (2022) community connections and leveraging networks facilitate minority recruitment, while gaps create barriers, such as the vacant AS position seen in the current study.
Intervention adherence/completion was challenged by reliance on a single-therapist who concurrently provided ACT tele-counselling for research participants and AS clients, as well as care partner desire for immediate access to ACT. AS staff emphasized the need for immediate access to mental health services as many care partners delay seeking help until they are in crisis. However, the therapist’s workload limited her availability and resulted in wait times for ACT within and outside of the study. Three potential participants declined to enroll due to concern that they would be allocated to the control group and could experience a longer wait time than as an AS client.
Limited therapist availability and wait times have been described as barriers to participation in other ACT studies (Durepos et al., 2023), and ACT may require a duration of 3 weeks between sessions to allow time for processing (Durepos et al., 2023; Hayes et al., 2012). A larger trial will therefore require additional resources to permit a longer study duration, additional therapists, and targeted presence of AS or other staff within all regions to promote recruitment.
Despite limitations, findings suggest ACT tele-counseling is acceptable and beneficial for Anglophone and Francophone care partners in rural and urban settings. Baseline ZBI-12, AAQ-2, and EMAS scores aligned with prior research, indicating high burden and low-to-moderate engagement in meaningful activities (Bédard et al., 2001; Fauth et al., 2022; Goldberg et al., 2002). Encouragingly, the intervention group showed significant reductions in anxiety, stress, and burden post-ACT. While between-group differences were not statistically significant, likely due to the small sample, the intervention group showed greater improvements. The control group improved in psychological flexibility (AAQ-2), suggesting general support had some benefit, but ACT’s structured approach was more effective across multiple outcomes.
Participants consistently reported that the program was accessible and flexible to care partner needs, particularly in rural areas where transportation and respite care can be significant barriers. The ability to access therapy remotely reduced logistical challenges and allowed participants to fit sessions into their daily routines. However, participants identified wait times due to therapist availability as an area for improvement. These findings align with existing literature on ACT with participants which describe flexibility, convenience, and remote delivery with minimal need for technology as increasing access to mental health services (Atefi et al., 2024; Durepos et al., 2023).
At the time of this study, no other AS branch in Canada offered a structured psychotherapy program for clients. While AS staff reported some administrative burden in implementing the study and ACT program, they also saw benefits for care partners, the healthcare system, and themselves. Staff noted that attending the ACT program likely improved care partners’ well-being, potentially delaying PWD admission to long-term care and easing strain on the healthcare system. Research has similarly linked care partners’ mental and physical health to PWD care quality and long-term care admission timing (Saragosa et al., 2022). An unexpected finding was AS staff’s perception that providing ACT tele-counselling internally reduced the emotional strain of supporting care partners without personal expertise or timely referral resources. Community service providers, including AS staff, have reported emotional and moral distress when system challenges prevent them from meeting client needs (Webber et al., 2022). Access to an internal mental health service may therefore benefit both staff and care partners.
Limitations
The study’s small sample size and geographic focus (a single province) limit the generalizability of its findings. Further, the small sample size means it is unclear if differences between primary and sensitivity analyses reflect the impact of the full intervention on outcomes (i.e., sensitivity analyses included only those who completed six or more intervention sessions) or more likely, limited power in the sensitivity analyses. Participants were predominantly younger, English-speaking, White women caring for a parent, which may not reflect the broader population of care partners. Those with acute mental illnesses were excluded, despite potentially benefiting from such interventions. Additionally, reliance on self-reported data from participants who were not blinded to their group assignment may have introduced social desirability bias. Further research is needed to validate these findings across diverse populations and settings.
Implications
This study highlights that an ACT tele-counseling program delivered by telephone is acceptable and likely benefits care partners of PWD living in rural and urban areas. However, recruitment feasibility was limited. A larger, multi-province trial is necessary to build on these findings. Such a study should extend the study period to 24–36 months, enabling more robust recruitment and adequate time for participants to complete the intervention. Efforts should be made to ensure AS staff (or similar partners) are positioned in remote and minority-language communities to facilitate connections and recruitment. In addition, increased resources are needed to employ multiple ACT-trained therapists, reduce wait times, and facilitate intervention completion.
The findings reinforce the potential value of ACT psychotherapy for care partners and suggest that ACT components can be delivered remotely (at least by telephone) by a trained therapist with perceived benefits. CBT remains the most widely available form of psychotherapy; however, therapists and mental health providers should consider offering ACT to care partners and providing services through remote modalities (Atefi et al., 2024). Implications for staff include integrating ACT-principles into existing programs and advocating for the provision of structured mental health support services within care partner organizations, to alleviate strain on staff and increase access to tailored support for referrals.
As dementia rates rise, accessible support for care partners is crucial. This study provides insights into scaling and sustaining ACT tele-counseling in a rural, bilingual setting, informing study timelines, therapist availability, and accessibility. Findings highlight ACT’s potential to improve caregiver well-being, reduce healthcare strain, and support advocacy for publicly funded tele-counseling. Integrating ACT into caregiver training could further expand access to quality mental health support.
Footnotes
Acknowledgments
The authors wish to thank the Community Advisory Committee who supported them during this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We received funding from Mental Health Research Canada (2022-2023); Research NB (2022-2023), and the Council of the Federation Award for Innovation in Mental Health and Addictions Care, 2022.