
Abstract
In the United States, spouses provide 17% of in-home care for people living with dementia. Negative impacts of dementia care on spouses/partners are well-documented, but we lack information about the holistic experience for spouses/partners. We conducted a secondary thematic analysis of data from two observational studies about everyday music engagement and dementia care at home. In this paper, we report on experiences of dementia care from the perspectives of spouses/partners. Participants included 15 people living with dementia (20% women, 20% people of color); 15 spouses/partners (73% women, 27% people of color). Individual experiences varied, but underlying patterns emerged: 1) Caregiving approaches were grounded in loyalty and commitment 2) Spouses
• Insight on the lived experiences of spouses and partners providing dementia care at home • Identification of common challenges as well as sources of motivation and meaning among spousal/partner caregivers • Social perspective on spousal/partner dementia caregiving beyond well-documented adverse health effects
• Reflecting on early life experiences and values can help guide spouses/partners through complex caregiving decisions • Small gestures from the person living with dementia present spouses/partners with the opportunity to reminisce on their relationship and rediscover their reasons for providing care • A deeper understanding of both positive and negative aspects of the caregiving experience may help clinicians better support spouses and partners providing dementia careWhat this paper adds
Applications of study findings
Introduction
In the United States (US), an estimated 6.9 million people live with Alzheimer’s disease and related dementias, cared for by nearly 11 million unpaid care partners (Alzheimer’s Association, 2024). While on average Alzheimer’s disease has a progression of 4–8 years, some may live with the disease for up to 20 years. Dementia has a significant impact not only on people living with the disease, but on families and communities connected to people living with dementia (Alzheimer’s Association, 2024). Most people living with dementia reside at home (Alzheimer’s Association, 2024) and spouses provide 17% of unpaid dementia care (Kasper et al., 2015).
Given their age, relationship to the person living with dementia, and personal health concerns, spouses/partners are uniquely vulnerable to the emotional and physical burdens of dementia caregiving. Spouses of people living with dementia face higher mortality rates, depression, and cognitive decline when compared to non-caregiving spouses (Adams, 2008; Norton et al., 2010). A growing body of literature has started to focus on the lived experiences of caregiving, which describe adverse health effects of dementia caregiving on spouses/partners. Dementia both challenged and preserved notions of togetherness within new notions of “me” and “us,” in daily life and in thoughts about a changed future (Hammar et al., 2021; Meyer et al., 2016; Swall et al., 2020). Barriers faced by many spouse/partner caregivers include difficulty acknowledging their unmet emotional support needs, reluctance to take time away from the caregiving role (Tatangelo et al., 2018), and at times feeling like a carer first and a person second (Hammar et al., 2021).
Although there is extensive literature on the burden of dementia caregiving (Cheng, 2017), people who engage in caregiving also report positive aspects of caring for people living with dementia, including feelings of gratification, mutual appreciation, and life purpose (Yu et al., 2018). However, few studies (Shim et al., 2013; Yu et al., 2018) have examined how spouses find both challenges and meaning in their dementia caregiving experiences and even fewer have addressed the experiences of non-heterosexual spouses/partners, domestic partners who are not married, or have used mixed methods and longitudinal qualitative approaches.
In this study, we sought to explore dementia caregiving experiences from the perspective of spouses/partners. We synthesized data from two observational, in-home studies of music and everyday life in dementia caregiving relationships to address two research questions: 1) How do spouses/partners navigate relationship changes occurring after one person develops dementia? 2) How do underlying values, beliefs, and experiences shape approaches to caregiving? In this paper, we identify common motivating factors and greatest challenges associated with how and why spouses/partners provide in-home care for their loved one living with dementia.
Methods
Overview
We synthesized data from two in-home, mixed-methods studies of dementia caregiving to explore the motivations for and experiences of dementia care from the perspectives of spouses/partners. Both studies examined the role of usual music activities in everyday life for people living with dementia and both their care partners. Music and Dementia Study 1 (MDS1) involved 3 visits over 2–10 weeks with a highly diverse sample of 21 dyads in 2018–2020, prior to the COVID pandemic (Allison et al., 2022, 2023; Kotwal et al., 2024). Music and Dementia Study 2 (MDS2) followed 17 dyads up to 2 years (2021–2024) to assess changes with dementia progression. MDS2 study procedures took place during the COVID pandemic. Due to increased barriers to research participation during the pandemic, MDS2 consisted of a disproportionately white, highly educated sample. Both studies were approved by the University of California, San Francisco Institutional Review Board (Protocols 18-25894 and 19-28435). We synthesized the data from both studies (detailed in the Unified Data Analysis sub-section below) (Kotwal et al., 2024). We chose to examine both data sets together to leverage the strengths of each: the greater diversity of the MDS1 sample and the longitudinal follow-up of MDS2. The study periods, pre-pandemic and during COVID, provided a natural comparator that enabled us to validate findings across drastically different social circumstances.
MDS1 focused on dementia caregiving relationships and the impact of functional status through the lens of music engagement. In MDS1, although 3 visits over 10 weeks could be considered longitudinal follow-up, the duration of the study was too short to assess changes due to dementia progression. MDS2, in contrast, was a two-year longitudinal ethnography that aimed to study the impact of dementia progression on caregiving relationships and music engagement over time.
For both parent studies, participants included people living with dementia in the San Francisco Bay Area of the United States (U.S.). Eligible participants included: people living with dementia (any stage) who spoke English and had a live-in family or professional care partner, paid or unpaid. Eligible care partners spoke English and functioned as the primary care partner.
Both MDS1 and MDS2 used a mixed methods approach. In MDS1, the study team collected structured data, including demographics and validated measures of functional status (Katz et al., 1970), dementia severity (Sclan & Reisberg, 1992), and caregiver burden (Bédard et al., 2001). Study team members conducted semi-structured interviews and participant observation using interview and observation guides developed and field-tested by JG, TA, HS, MH, KZ, AR, and AS. Visits were audio recorded and professionally transcribed; fieldnotes were written after each visit. These researchers used ethnographic analysis to inductively code the data (Emerson et al., 2011; Schensul & LeCompte, 2012) and create a comprehensive codebook with the full interprofessional research team. The codebook was applied to the transcripts using ATLAS.ti software (ATLAS.ti, 2022). The detailed methods used in MDS1 have been published previously (Allison et al., 2023), consistent with the Consolidated Criteria for Reporting Qualitative Research (Tong et al., 2007).
MDS2 was designed using the same participant inclusion/exclusion criteria, recruitment methods, data collection, and analytical methods as MDS1 to facilitate future study using both data sets, but study procedures required multiple modifications. In the early stages of the COVID-19 pandemic, all study procedures for MDS2 were converted to telephone or video. Home visits began once COVID physical distancing requirements became less restrictive.
In MDS1, two PhD-level ethnomusicology researchers (TA and JG) and a Masters-level psychology researcher (AR) conducted data collection and analysis. In MDS2, data were collected by two ethnographers, a geriatrician/ethnomusicologist (TA) and a medical anthropologist (KZ), or by research team members (HS and MH) trained in study procedures by the ethnographers. We used the same IRB-approved method for assessing capacity to consent to research for both studies.
Unified Data Analysis
The parent studies were designed to investigate large research questions because there was little known about everyday life and music engagement in the homes of people living with dementia. As we followed participants over the first year of MDS2, recurrent patterns began to emerge among spouses/partners. Two new research questions helped to focus our understanding of spouses/partners: 1) How do spouses/partners navigate the relationship changes that occur when one person develops dementia? 2) How do underlying values, beliefs, and experiences shape approaches to caregiving? These new research questions are the focus of the unified data analysis described in this paper.
The data corpus (Braun & Clarke, 2006) for the two studies included baseline demographics, a brief questionnaire, validated measures, semi-structured interviews, and over 2645 pages of interview transcripts, fieldnotes, and analytical memos for both studies. MDS2 also included interim telephone follow-up calls to collect intercurrent events including hospitalizations, death, changes in the caregiving team, new music activities, and special holidays. Much of the data for both studies did not include spouses/partners; not all the data could be harmonized. The data set for this paper, therefore, was restricted to spousal/partner dyads across MDS1 and MDS2 and included demographic information and interview transcripts for visits with spousal/partner dyads across both studies 1 . We have provided an updated COREQ checklist as Supplemental File 1 (Tong et al., 2007)
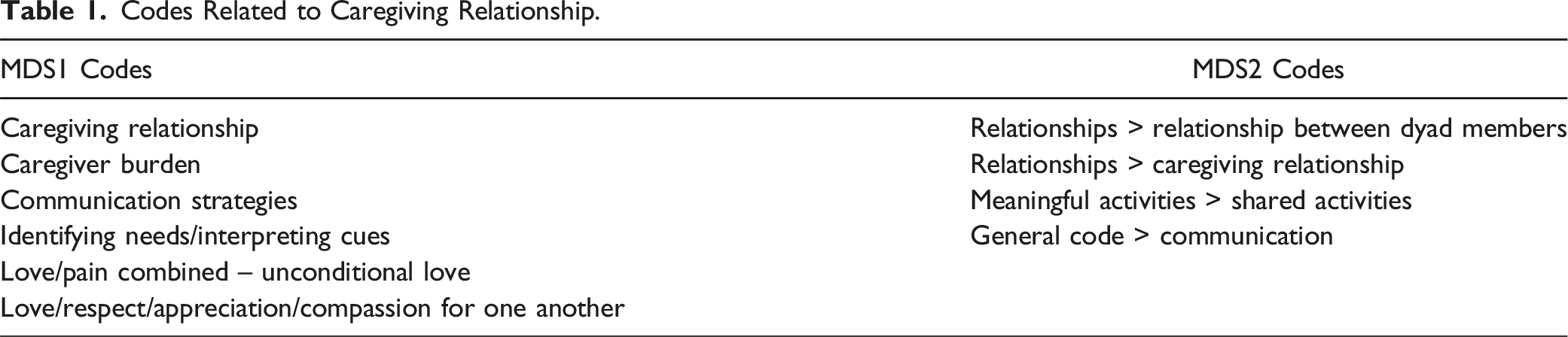
First, the two codebooks were compared and found to have distinct differences. Second, all codes relevant to the dyadic relationship, care support systems, and caregiving strategies were extracted from the ATLAS.ti databases for further analysis (Table 1). Third, the coded segments (i.e., quotes) within those codes were extracted from the two ATLAS.ti databases, and the resulting unified data set was examined using thematic analysis (Braun & Clarke, 2006, 2014). Fieldnotes and telephone follow-up calls were selectively reviewed to enrich the analysis. See Figure 1 for a flow diagram of the unified data analysis. Flow diagram of unified data set construction and analysis. Codes Related to Caregiving Relationship.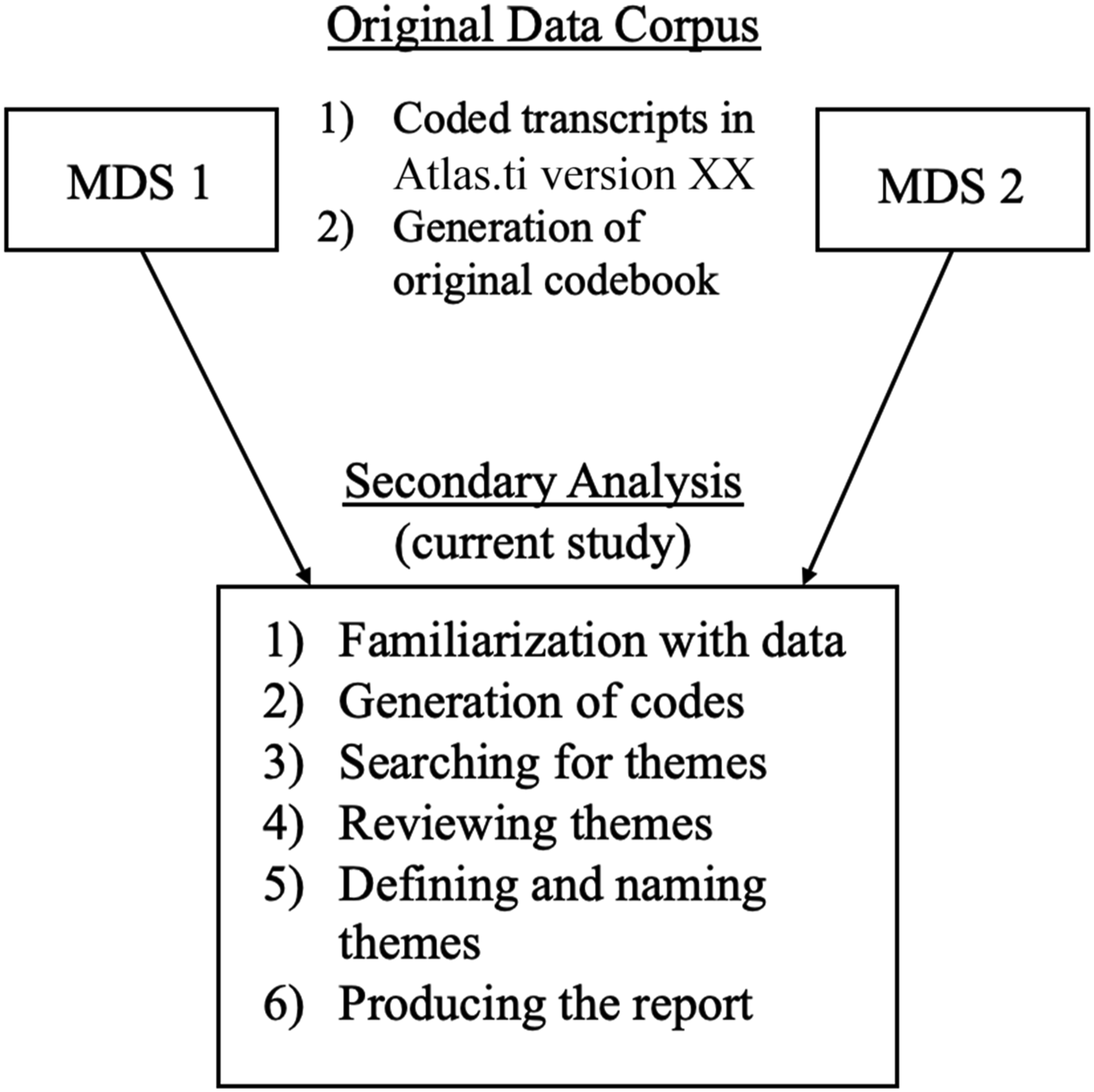
Results
Participants
Participant Demographics.
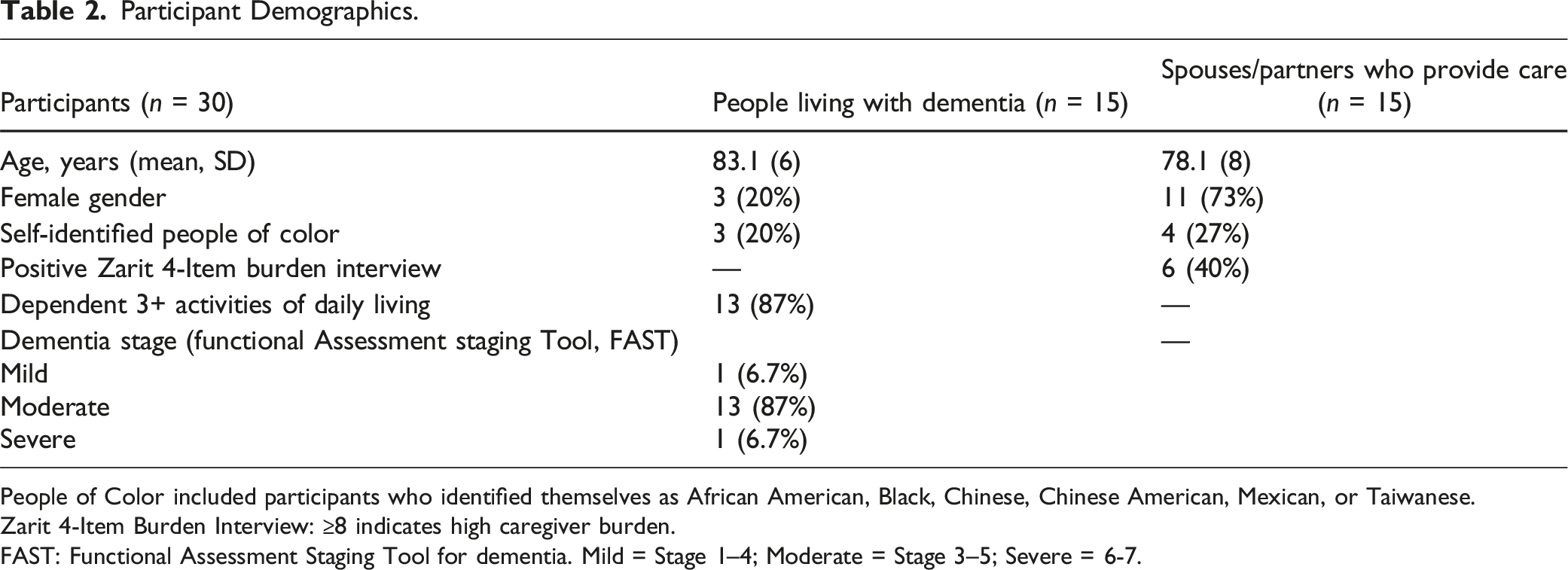
People of Color included participants who identified themselves as African American, Black, Chinese, Chinese American, Mexican, or Taiwanese.
Zarit 4-Item Burden Interview: ≥8 indicates high caregiver burden.
FAST: Functional Assessment Staging Tool for dementia. Mild = Stage 1–4; Moderate = Stage 3–5; Severe = 6-7.
Themes
Themes Generated From Unified Analysis of the 15 Dyads.
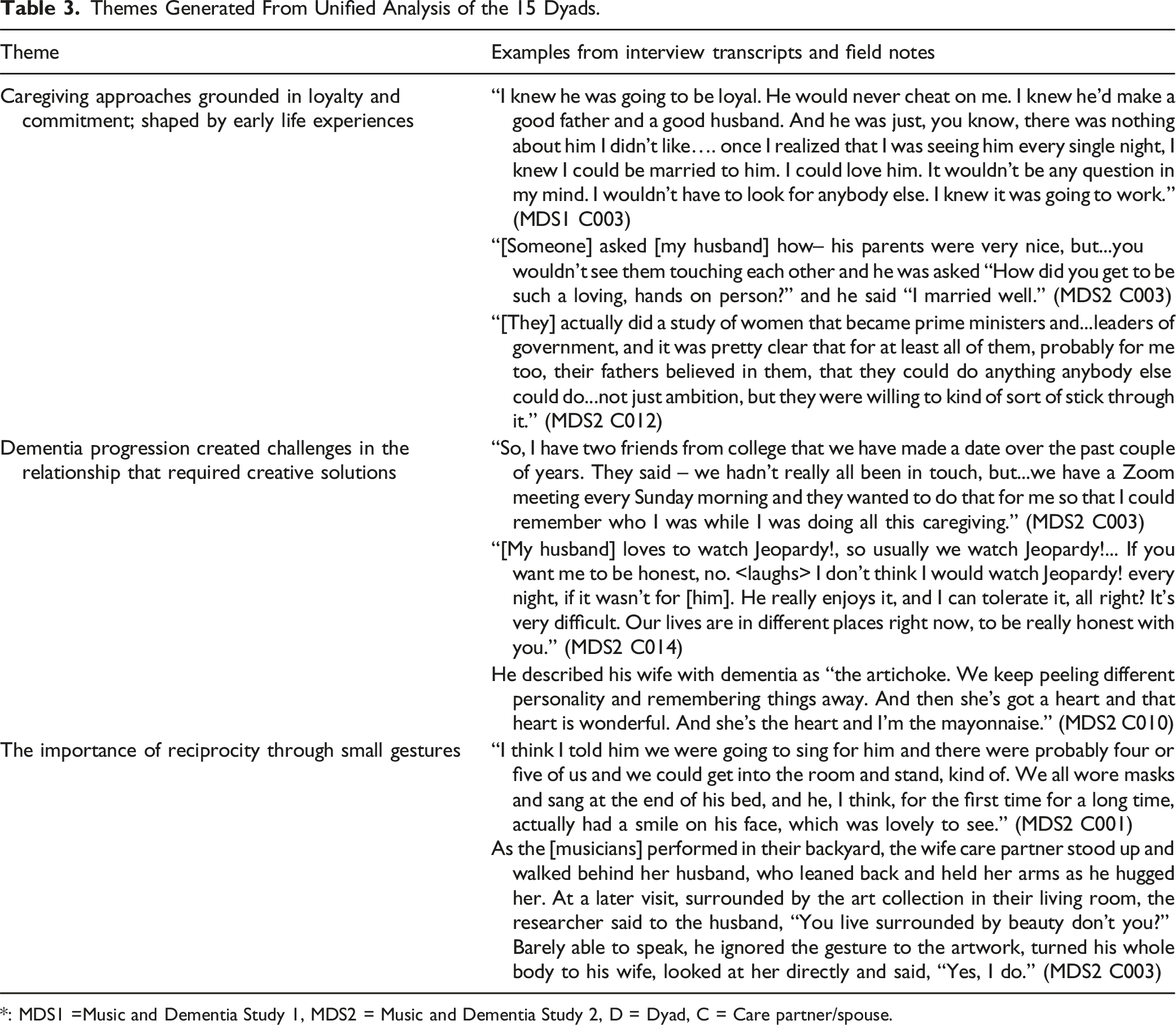
*: MDS1 =Music and Dementia Study 1, MDS2 = Music and Dementia Study 2, D = Dyad, C = Care partner/spouse.
Theme 1: Caregiving Approach Grounded in Loyalty and Commitment
Most care partners discussed devotion to the person living with dementia and their relationship when asked about their decision to take on the care partner role. During a home visit with one of the dyads (MDS2 D022), the wife expressed wishing that more care partners took pride in their role rather than seeing it as a burden. She wished that “more caregivers appreciate the fact that they're gaining, too. It's not just giving. They're gaining…I love this song [(I Love You) For Sentimental Reasons (Watson & Best, 1945)] the most because the one line that says, ‘I never feel lonely when you're in sight.’ That's very touching and very true.” (Wife, 65-year relationship)
During a subsequent home visit, we asked her why she had retired from her role as CEO in order to remain at home with her husband. At first, she simply said “I made a promise three years ago when he was starting to get sick that I will always be here to protect him, and I aim to fulfill my promise. Not just the wedding vows.” During a follow-up visit the following year, we discussed the notion of promise again. She explained that in the early stages of dementia progression, “[her husband] was so scared. He asked me to promise him that I would keep him under guard.” Over the course of several home visits, this wife care partner emphasized pride in her role as a caregiver and often returned to the promise she made to both her husband and herself.
Commitment Shaped by Family Dynamics or Early-Life Experiences
When probed about their motivations for caregiving, spouses/partners discussed family dynamics and early-life experiences as shaping their commitment. Several care partners identified prior formative experiences caring for aging parents. During a home visit with MDS1 D006 (husbands, 30+ year relationship), study team members observed as MDS1 D006 prepared dinner while dealing with a complex medication regimen. As he cooked, the husband care partner explained how he cared for his mother-in-law for over four years: “She had dementia, and she needed a lot of watching after.” The husband with dementia interjected repeatedly, “never a complaint,” as the care partner husband described first caring for his mother-in-law and then for his spouse. “I did manage to keep a really good, honestly cheerful disposition,” the husband care partner explained. “I never snapped at her except the closest thing–well, it was just one time we told her ‘No, you can’t have a milkshake.’ That’s about as abusive as we got.” Despite the challenges of caring for both his husband and mother-in-law while tending to his own health issues, this care partner maintained a positive attitude and a commitment to caring for his family members. In a different example (MDS2 D012), a wife care partner shared an experience from childhood. She stated feeling emboldened by her father’s belief that she could do anything she set her mind to, and this self-assuredness, she said, carried over to her roles as professor, administrator, and then care partner (See Table 3). Several participants also discussed early marriage dynamics with the person living with dementia, explaining how decades of equal partnership inspired their decision to provide care. Another wife care partner (MDS2 C015) detailed her marital values, stating: We abided by the three Cs…cooperation, commitment, and compromise… it wasn't popular in the days we got married, in 1955, but we didn't ‘genderize’ any chore we bumped into that had to be done…he would change diapers, I would mow the lawns…the first guy on the job was the one to take care of it because you waste time arguing over whose job it is, and we had six kids, we couldn't waste that kind of time. (Wife, 68-year relationship)
In addition, some participants shared specific familial or parental experiences as examples of what not to do. In one example, a husband care partner (MDS2 C006) reflected on the impact of his parents’ divorce when he was a child. He was determined to be different from his parents by honoring his marital commitment, which he now defined by his role as a care partner: “I took a vow.” He then explained why he was no longer a surgeon and researcher, but now a full-time care partner for his wife: I'm going to the grave. I made the promise and I'm not going to--if it's me first, that's fine. But I'm going to do it. I'm going to do it as long as I can in this setting, God willing. And if I can't, we'll do it in some other setting, but I'm going to be here and I'm going to do it.... in this day and age it seems that everyone--even if they've been in a long-time situation, they kind of feel that they now want to go fly on their own or whatever… you know, you made a vow. I'm not being religious, I'm just saying you said, ‘Yes, I will,’ what's that really mean? (Husband, 70-year relationship)
In a similar example, a wife care partner explained that her father’s lack of dependability made her more appreciative of her husband’s reliability and even more dedicated to her role as his care partner (MDS1 C022). In these cases, participants reported feeling determined to correct their parents’ mistakes through their own approach to partnership, love, and caregiving. The same wife care partner (MDS2 C022) also drew on her experiences with motherhood when discussing her caregiving role: I wasn’t complaining. I was just saying that [caregiving] was hard on me physically, and my daughter-in-law said to my son “I could never do that for you…” I said “Ohh. Why can’t you do that? Because you did it for your three children. You didn't complain. You changed their diapers, so it’s the same thing. Why is it not the same thing? Tell me because I felt that way. I did it for my children… (Wife, 65-year relationship)
Spouses/partners frequently cited loyalty and commitment as driving factors behind their decision to serve as primary dementia caregiver. Over time in MDS2, however, spouses/partners delved into the formative experiences that laid the groundwork for these values.
Theme 2: Dementia Progression Created Challenges in the Relationship
Across all dyads, care partners expressed feeling a sense of commitment that motivated them through the more challenging aspects of dementia caregiving, as well as feeling trapped and isolated by the caregiving role at times. At their lowest points, they cited loss of identity as an outcome of taking on this role. One participant attributed her relationship challenges to differences in age and health status compared to her spouse, explaining that “our lives are in different places right now, to be really honest with you. And I love [my spouse], and I’m dedicated to him, but… [laughs] sometimes I wish I was doing something else.” (Wife, 37-year relationship – MDS2 C014)
A different wife care partner struggled to get her previously clean-shaven husband to even take a shower. At our last visit, she was delighted to have succeeded. Well, it took many years. <laughter> It did. Two years. Geez, I should try to remember that, huh? That was important… He needs the cap that has the shampoo or whatever, the lather, you don’t get it wet with water [instead of a shower]. We started out with that. He didn’t want to do it. He finally did it and guess what? I think he felt a little better. And then from there we went on and I told him, “You have an appointment Friday.” I always use the appointment thing. “We have to get out of this house. If you walk out that way, you’re gonna scare people. You’re starting to look really like Santa Claus with the white beard. I mean seriously.” <laughter> So he said-- I think maybe even a Seroquel might have been involved at that time. Sort of calmed him down. Or maybe it was the Haloperidol. I don’t even know anymore. Whatever it was it calmed him down and he-- I don’t know…. So then my son happened to be here…. [My son] cut [my husband’s] hair, and I thought it was okay, you know. And then afterwards [my husband said], “Well, I want it shaved.” …And he actually, himself, went into the bathroom and sat on the chair and said, “I want it shaved.” … And then he looked at himself in the mirror and I think he liked what he saw. I mean doesn’t he look totally different?
In several instances, care partners grieved the loss of what their lives may have looked like without the dementia diagnosis. One care partner (MDS2 C010) stated: We’re mostly isolated, really. When you have someone who is not as communicative as [my wife] it’s hard… close friends of ours traveled to Europe and do all kinds of things that we can’t do. You know? Or would love to do…I mean we live a different life than we had planned, but it’s fun. I think we have fun together.” (Husband, 60-year relationship)
Despite differences in support systems, length of relationship, and years providing care, all care partners expressed some form of challenge or frustration associated with their changing relationships. Yet, as MDS2 C010 emphasized, care partners also strived to maintain a positive outlook despite challenges, highlighting the complex and bittersweet nature of caring for a spouse living with dementia.
Theme 3: As Dementia Progressed, Care Partners Found Meaning in Small Gestures
In the face of caregiving-related challenges, spouses/partners reported feeling especially grateful for small gestures. They shared how they interpreted verbal and non-verbal gestures as reciprocation of the love and care they provided to the person living with dementia. Although individual gestures were small, they could incite deep and complex feelings. Some participants described reminiscence for the life they shared before the progression of dementia, such as a husband care partner who shared what happened after he recreated a romantic dinner from their early courtship. He described the success of the dinner saying, “And then he looked at me…and he got up and walked over to me and gave me a big kiss and it was like I actually did it!” (MDS1 C006). Another husband care partner described how small gestures replaced words after his wife lost the ability to state her feelings: “you know how a child–you might be holding a child's hand? And the only thing they can reach is your arm, so they'll give you a kiss on the arm or something. She does that. So I know she feels pretty secure” (Husband, 25-year relationship MDS1 C009). The same care partner who spoke about her commitment was eager to share moments of reciprocity with her husband: “Nothing makes sense anymore. But sometimes it does!” While helping him dress, she explained, “…he suddenly grabbed my hand…[and] planted a big fat kiss here. That’s 2 years first time.” After she applied his lotion, her husband asked “’have you finished caressing me? Have you had enough?’ And then he starts laughing [chuckles], really loud. Which means he knows he cracked a joke.” (Wife, 65-year relationship – MDS2 C022) Although these moments were sometimes fleeting and did not change the reality of dementia caregiving needs, care partners expressed how they served as bright spots and opportunities to connect with their spouse/partner living with dementia. These moments allowed care partners to reminisce on the qualities they know and love about their partners.
Additional Findings
Despite personal beliefs, values, and commitment, caregiving needs sometimes outstripped resources. Three spouses who were deeply committed to care at home had to place their loved ones in an assisted living facility because they were medically and physically unable to continue providing care, and one domestic partner had to move out to make room for two professional caregivers who could manage her partner’s significant physical needs. One wife care partner remained in contact with the study’s principal investigator, describing how she visited the assisted living facility regularly and how good it felt to see her husband in a better mental state (kind rather than angry) and to have time to engage in her other caregiving roles, such as walking her dog and caring for grandchildren. Another wife care partner remained in the study. We observed how she carried her values to the assisted living facility, visiting regularly when it was possible during the pandemic and bringing members of their church choir to sing with the husband who, at that point, was on hospice with end-stage dementia. All five of them expressed relief at how much easier it was to attend to their own significant health needs once no longer primarily responsible for the spouse/partner living with dementia. As a clinician, one researcher (TA) observed how much healthier three of the spouses/partners appeared following the transition.
Discussion
Spousal/partner caregiving support has become recognized as a central priority in dementia care (Alzheimer’s Association, 2024; Alzheimer’s Foundation of America, 2023). Since everyday caregiving experiences take place in the privacy of the home, there is limited literature about everyday caregiving and few studies on everyday caregiving that apply longitudinal qualitative research approaches. We synthesized data from two in-home, mixed methods studies to better understand everyday experiences and their significance for care partners. Larger themes emerged from a complex, bittersweet set of stories and observations over time. We found common features underlying the care provided by spouses/partners, including challenges and motivators guided by notions of loyalty and commitment. Care partners identified prior, early childhood experiences and beliefs about the importance of loyalty as drivers of their desire to keep a spouse/partner at home. As cognition and function declined, care partners found the relationship increasingly difficult. They shared the feeling of being stuck as well as the loss of identity and freedom. This finding follows what Westrelin et al. (2024) describe in their study on spousal caregivers of partners living with dementia, in which spouses perceived changes not only in their partner but also in themselves and oscillated between their identity as a caregiver and as a spouse, highlighting the dynamic nature of caregiver identity construction within the context of caring for a partner living with dementia. At the same time, care partners identified specific gestures of love and reciprocity that sustained them and reminded them of the underlying relationship as dementia progressed and function declined. Across the dyads, care partners cited marital vows and lifelong promises as the driving force behind their daily commitment to their spouses/partners living with dementia.
Although the literature is clear about the adverse health effects of dementia caregiving on spouses/partners, less is known about the ways in which caregiving creates meaning in the lives of spouses. Despite the difficulty of dementia caregiving, there remained a place for small gestures of connection and moments of joy, even when such moments carried mixed emotions. Most important: in the literature on caregiving, there is no questioning of what it means to be in a committed relationship in this context; our findings demonstrate the complexity of long relationships in the context of dementia. Small moments of joy such as those described by our participants have been characterized previously in the literature both as professional reciprocity with nursing (Adams & Sharp, 2013) and as interprofessional reciprocity when it occurs across clinical teams and families in the nursing home (Allison et al., 2019). Our additional finding that spouses/partners expressed relief at being able to attend to their own health needs once no longer primarily responsible for dementia care builds on one prior longitudinal, exploratory qualitative study. Per the study, spousal caregivers providing care to a partner with dementia living in a resident care facility described a central notion of “together but apart” (Hemingway et al., 2016). Our study supports what is known in the literature but expands this into the home setting and draws from two larger studies that use mixed methods and longitudinal approaches. Thus, our findings contribute to a broader shift in how aging in relationships is viewed and studied.
This study provides a window into the daily lives of people living with dementia and that of their spouses/partners, populations that require an increasingly high level of support from providers and their communities. This study provides one piece of the puzzle within a larger context of dementia care and partner/spousal caregiving support.
There are both limitations and strengths to the methodological approaches used in our study. The smaller sample size and single location (San Francisco Bay Area) is typical within qualitative studies. Findings are not intended to be generalizable. However, longitudinal follow-up and in-home data collection allowed us to observe changes over time and to triangulate participants’ interview statements with their observed interactions. Our approach allowed for depth of data collection, rather than breadth of data collection. Secondary analysis of qualitative data is typically conducted for the purposes of examining new questions which are closely related to or extend the primary study questions, expanding the findings from the original data. Thus, although the analysis presented in this paper was not the original aim of the 2 parent studies, our rigorous and systematic secondary analysis approach produced rich results.
Implications
This collection of dementia caregiving experiences lays the groundwork for researchers and clinicians hoping to improve the state of dementia care. These findings may inspire additional studies of protective versus harmful factors among partners/spouses providing dementia care, the effectiveness of need-specific resources, or the potential benefits of support groups and opportunities for spouses/partners to share their experiences.
Personal stories help providers, social workers, and other care team members better understand the unique burden of dementia caregiving on spouses/partners who provide care. This work sheds light on the challenges of providing care as well as gratifying moments that support and sustain their relationships. We can support spouses/partners in their primary caregiving role by bearing witness and making them feel seen, normalizing and validating their needs for support. We encourage care teams to find ways to ask care partners about both their challenges and the small gestures of reciprocity as we help them navigate changes in relationship, prioritize small moments, and reflect on their reasons for providing care.
Supplemental Material
Supplemental Material - “I aim to Fulfill My Promise”: Dementia Caregiving From the Perspective of Spouses and Partners
Supplemental Material for “I aim to Fulfill My Promise”: Dementia Caregiving From the Perspective of Spouses and Partners by Haley M. Shiff, Theresa A. Allison, Madina Halim, Kenneth E. Covinsky, Alexander K. Smith, Deborah E. Barnes, Jennie M. Gubner, and Kara Zamora in Journal of Applied Gerontology
Footnotes
Acknowledgments
The authors would like to acknowledge the generous gift of time and energy from the anonymous participants in these two research projects and for allowing us to enter their homes and their lives. We appreciate the skill and effort of research team members Annette Rodriguez and Sarah Ngo, and the mentorship of Kristine Yaffe and Julene K. Johnson.
Author Contributions
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Barnes is Chief Science Advisor, co-founder, and shareholder of Together Senior Health. She also is a co-inventor of the Preventing Loss of Independence through Exercise (PLIÉ) and Paired PLIÉ programs and has the potential to earn royalties. The other authors have no conflict of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Aging at the National Institutes of Health (K23AG062613 and RF1AG082292-01A1 to T.A.A., P30AG044281-06S1 to K.E.C., K24AG068312 to A.K.S.). This research was funded by The Medical Student Training in Aging Research Program and the National Institute on Aging (T35AG026736). This research was also supported by a grant from the Osher Center for Integrative Medicine at the University of California, San Francisco. Sponsors played no role in the data collection, analysis, or preparation of this manuscript. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.