
Abstract
This scoping review, following Levac et al.’s methodology, examines the implementation and impact of relationship-centered care (RCC) in long-term care (LTC) settings for older adults. Peer-reviewed articles from AgeLine, CINAHL Complete, MEDLINE, PsycINFO, and Web of Science were included if published after 2000, involved older adults in LTC homes, focused on RCC, and conducted in Australia, Europe, New Zealand, or North America. Key findings were organized using inductive content analysis, and 41 empirical studies with qualitative, quantitative, and mixed-methods designs were included. Three categories emerged: (1) Core Practices of RCC—relationship building and reciprocal exchange; (2) Transformative Impacts of RCC—improved care quality and collaboration; and (3) Pathways and Roadblocks to RCC—individual and organizational factors. By understanding the key elements, facilitators, and barriers of RCC, policymakers and practitioners can develop targeted strategies to improve care experiences and outcomes for residents, families, staff, and all others involved in LTC.
• Deepens understanding of RCC in LTC through practical examples, connecting theory to practice. • Presents a comprehensive synthesis of empirical studies, highlighting RCC’s benefits and challenges. • Provides a framework to develop strategies for enhancing care experiences and outcomes in LTC.
• Guides LTC practitioners on RCC strategies to build meaningful relationships and improve care quality. • Advises policymakers on supportive policies that overcome RCC barriers, promoting holistic geriatric care. • Identifies gaps in RCC research, such as its impact on diverse populations, suggesting future research directions.What this paper adds
Applications of findings
Introduction
The global population over 60 is projected to double from 12% to 22% between 2015 and 2050 (WHO, 2022). As people age and experience physical or cognitive decline, they may require daily assistance with tasks like bathing, dressing, housekeeping, meal preparation, and medical support (WHO, 2024). Long-term care (LTC) services address these needs, helping individuals with significant physical or cognitive challenges maintain their functional abilities and dignity. LTC services also support social participation and manage chronic conditions through community-based nursing, physical therapy, and palliative care. The World Health Organization emphasizes incorporating person-centered care (PCC) principles into all LTC services to respect and meet individuals’ unique needs, ultimately enhancing overall care quality (Perracini et al., 2022; WHO, 2024).
PCC, a model that emphasizes the holistic needs and preferences of those receiving care, became prominent with culture change movement, advocating a shift from strictly biomedical models to biopsychosocial approaches that prioritize residents’ autonomy and quality of life (QoL) in LTC settings (Bhattacharyya et al., 2022; Fazio et al., 2018; Kitwood, 1997). While the culture change movement encourages strong, cooperative bonds among residents, families, caregivers, and the community (Cornelison, 2016), PCC sometimes overemphasizes residents’ independence, potentially overlooking the essential interconnections vital to effective care relationships. To address these limitations, relationship-centered care (RCC) builds on the principles of PCC by placing a stronger emphasis on interpersonal bonds and positive, reciprocal relationships as fundamental to quality care (Hirschmann & Schlair, 2020; Nolan et al., 2004).
Introduced by Tresolini and the Pew-Fetzer Task Force (1994) after a review of the US healthcare system, RCC promotes a shift from disease-focused care to an approach that considers social, economic, environmental, and cultural contexts (Nolan et al., 2006, 2008). RCC emphasizes personal experiences with illness and relationship-building as core to therapeutic and healing processes. It views care as a relationship-building process rooted in trust and reciprocity. Key elements include clinical expertise for compassionate care, effective teamwork and interdisciplinary communication for respect and clarity, and continuity of staff and family relationships to support a positive LTC environment (Nolan et al., 2008).
Foundational Frameworks
The concept of RCC in LTC is grounded in well-established theoretical perspectives that emphasize the value of interpersonal relationships in care environments. Frameworks like Nolan et al.'s Senses Framework (2004, 2006, 2008) and Dewar's Caring Coversations (2011) advocate for enhancing care quality in LTC homes through meaningful relationships.
Developed by Nolan and colleagues in 1997 and refined over 20 years, the Senses Framework enhances RCC by addressing the needs of all involved in care, focusing on both subjective and perceptual elements (Nolan et al., 2006, 2008). The framework’s six principles are creating a sense of safety (Security), valuing personal histories (Continuity), fostering community (Belonging), encouraging purposeful activity (Purpose), supporting personal goals (Fulfillment), and recognizing individual contributions (Significance). These principles make the Senses Framework a valuable tool for fostering an inclusive and effective LTC environment.
The Caring Conversations framework supports RCC by promoting compassionate, dignified interactions among staff, older adults, and families (Dewar, 2011; Dewar & Nolan, 2013). It includes seven components: addressing sensitive topics (Be Courageous), showing empathy (Connect Emotionally), demonstrating interest (Be Curious), respecting differing viewpoints (Consider Other Perspectives), collaborating (Collaborate), finding mutually acceptable solutions (Compromise), and acknowledging efforts (Celebrate). These elements are vital for skilled interactions, supporting the six senses and advancing RCC (Dewar, 2011; Dewar & Nolan, 2013). The Senses Framework and Caring Conversations highlight the importance of compassionate interactions and holistic support, framing RCC as essential to high-quality care. Both emphasize relationship-building as central to quality care, reinforcing RCC’s focus on this review.
Current Gaps
To date, scoping reviews on RCC have predominantly focused on broader healthcare contexts. Lamph et al. (2023) examined relational practices in health, criminal justice, education, and social work, noting definitional ambiguities among practitioners, policymakers, and academics. A recent review by Fox et al. (2024) focused on relational collaboration within healthcare teams, emphasizing the need for a supportive team culture and organizational support to enhance worker well-being. Another scoping review emphasized the central role of relationships in delivering quality care, with the concept of RCC being influenced by theories of sociology, social psychology, and psychiatry (Soklaridis et al., 2016). However, a major gap remains in understanding RCC specifically in LTC for older adults, especially in personal areas like continence care. Bhattacharyya, Morgan, and Burgess (2022) developed a framework showing that resident satisfaction in nursing homes is driven by autonomy, meaningful activities, and social interaction—factors essential to quality of life, yet often overlooked in LTC assessments. Their findings stress that resident satisfaction extends beyond clinical care, involving environmental, psychological, and relational aspects. Thus, further investigation is needed to map RCC-specific practices and resident-centered perspectives in LTC settings and address current knowledge gaps.
This review aims to fill these gaps by focusing specifically on RCC in LTC, examining current practices, challenges, and limitations to provide a comprehensive view of RCC’s role in enhancing well-being. By assessing RCC’s contributions to LTC, this study enriches the literature, identifying key relational practices and the facilitators and barriers affecting RCC implementation.
Objective and Research Questions
This scoping review aims to explore the scope and depth of existing knowledge on RCC in LTC settings for older adults, examining its implications, benefits, and challenges. The following questions guide this review: 1. What practices constitute RCC in the context of LTC for older adults? 2. What are the outcomes of RCC in LTC settings? 3. What are the facilitators and barriers of implementing RCC in LTC settings?
Methods
Scoping review, a form of knowledge synthesis, explores research questions by systematically reviewing, selecting, and summarizing relevant literature to map key concepts, a variety of evidence, and research gaps (Colquhoun et al., 2014). This study follows the framework developed by Levac et al. (2010), to investigate RCC for older adults in LTC settings. The following steps are included in the framework: (i) developing the research question, (ii) establishing pertinent studies, (iii) selecting the studies, (iv) charting the data, (v) synthesizing and reporting the results, and (vi) consulting stakeholders to enhance the review’s relevance and applicability (Levac et al., 2010, 3).
Developing the Research Question
The three primary research questions guiding this scoping review have been outlined earlier. The target population for this review is older adults residing in LTC homes, and the concept is RCC approaches. As introduced earlier, RCC is an approach that views relationships as essential to therapeutic and high-quality care, emphasizing interactive and reciprocal exchanges among residents, their relatives, and care staff (Nolan et al., 2006; Ryan et al., 2008).
Establishing Pertinent Studies
The research questions focus on exploring RCC for older adults in LTC settings. Other care approaches that predate RCC, such as PCC, which focuses on the overall needs and individual preferences of care recipients, were considered beyond the scope of this review. With the guidance of supervisor who has content (e.g., RCC research) and methodological (e.g., review and analysis) expertise, this scoping review was conducted as part of a dissertation project. An experienced social science librarian provided expertise in refining search terms and strategy for selecting the studies.
Search Terms and Search Strings.

Selecting the Studies
Following the database searches, relevant study citations were collated and uploaded into Covidence, which is an online software program to manage systematic reviews efficiently (Babineau, 2014). After removing the duplicates, the first and second author independently screened titles and abstracts based on inclusion/exclusion criteria. To ensure consistency and clarity, the researchers reviewed the inclusion and exclusion criteria together regularly, discussing any points of potential ambiguity. The full text articles were then retrieved and assessed in detail against the inclusion criteria. Any unresolved conflicts or concerns that arose at each stage of the study selection process were resolved through discussions between the lead researcher and the second author. Reasons for exclusion of studies at each stage are recorded in Covidence and reported in the scoping review. The search results and the study selection process are detailed using a Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for scoping review (PRISMA-ScR) flow diagram (Tricco et al., 2018) (see Figure 1 below). Flow diagram of study identification and selection.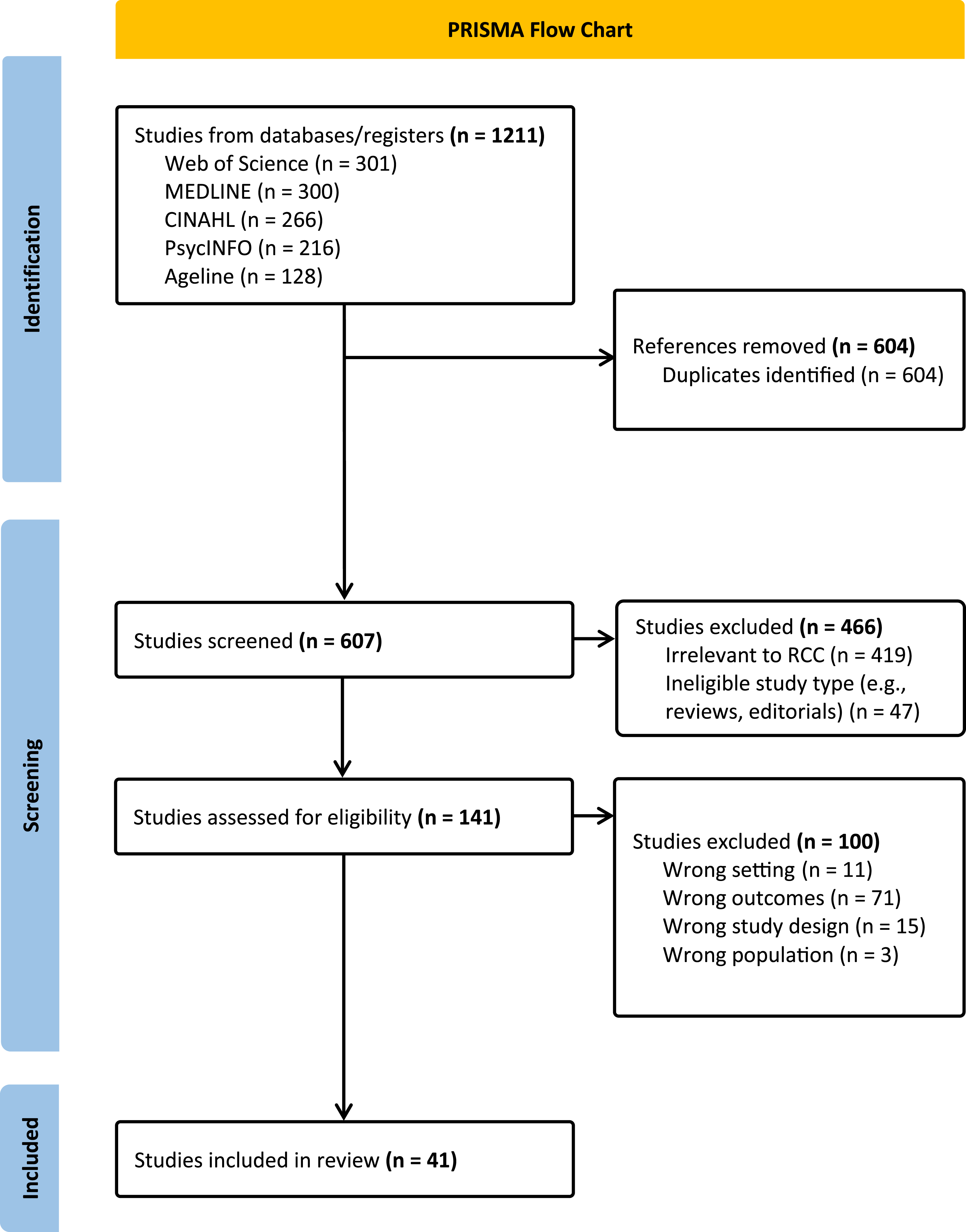
The inclusion criteria for peer-reviewed journal articles were (i) population: older adults in LTC homes; (ii) concept: RCC or related concepts, such as care relationships and relational care; (iii) publication date range: 2000–2024; (iv) language: English; and (v) empirical research only. The term “older adults” allowed broader inclusion, while the 2000–2024 range captured relevant, contemporary RCC research in LTC. Diverse study designs—quantitative, qualitative, and mixed methods—were included to map the full breadth of evidence in this interdisciplinary field (Arksey & O’Malley, 2005; Joanna Briggs Institute, 2020).
Exclusions were (i) studies in acute care hospitals, ambulatory care, assisted living, or community-dwelling settings; (ii) research conducted outside Australia, Europe, New Zealand, or North America; and (iii) non-empirical or non–peer-reviewed studies. LTC settings were chosen to focus on high-dependency care, excluding assisted living facilities (ALFs) due to their lower care levels. Including ALFs could have broadened RCC insights across the care continuum, but the exclusion enabled targeted analysis of RCC in intensive care contexts. Reference lists of included studies were also hand-searched to identify additional relevant studies.
Data Charting
Data Chart of Articles Included in the Scoping Review.

Collecting, Synthesizing, and Reporting the Results
Inductive content analysis was used to systematically describe and interpret findings. As a research method, content analysis allows for systematic description of phenomena and deeper insights into the data (Elo & Kyngäs, 2008). The process involved (i) open coding (the first author reviewed texts to establish initial headings); (ii) category development (grouping these codes into broader categories); and (iii) abstraction (refining groups into overarching categories). The second author reviewed and adjusted codes, achieving consensus on final categories. NVivo 12 supported the iterative analysis (Zamawe, 2015).
Consulting Stakeholders
To enhance the review’s relevance, we consulted RCC and LTC experts, who reviewed our research question, methods, and preliminary findings via virtual meetings and email. Their insights helped us refine categories, identify key studies, and align our analysis with current LTC needs.
Results
Out of 1211 articles initially identified, 1070 were excluded after removing duplicates and screening titles and abstracts. This left 141 articles for evaluation against inclusion and exclusion criteria. In total, 41 articles were reviewed to explore RCC approaches for older adults in LTC settings (see Figure 1 for the Flow Diagram of Study Identification and Selection). Table 2 provides a summary of selected study characteristics for this scoping review. As shown in Figure 2, 26 studies employed qualitative methods, eight quantitative, and seven mixed methods. The studies were in Canada (13), the United States (3), Europe (21), Australia (3), and one in both Canada and Sweden. Identified articles distributed by study methods and location.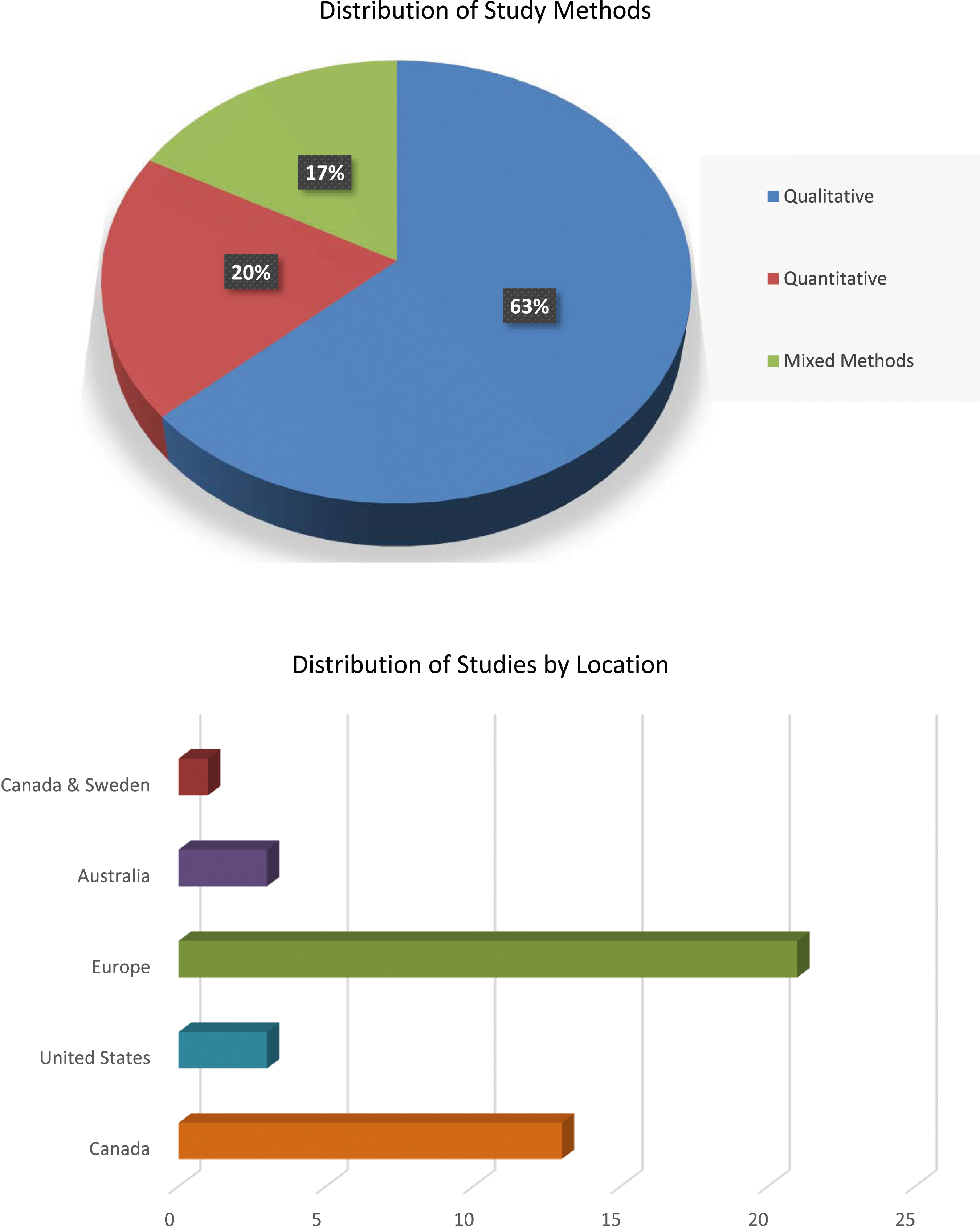
Findings
Synthesis of Key Findings From the Scoping Review.
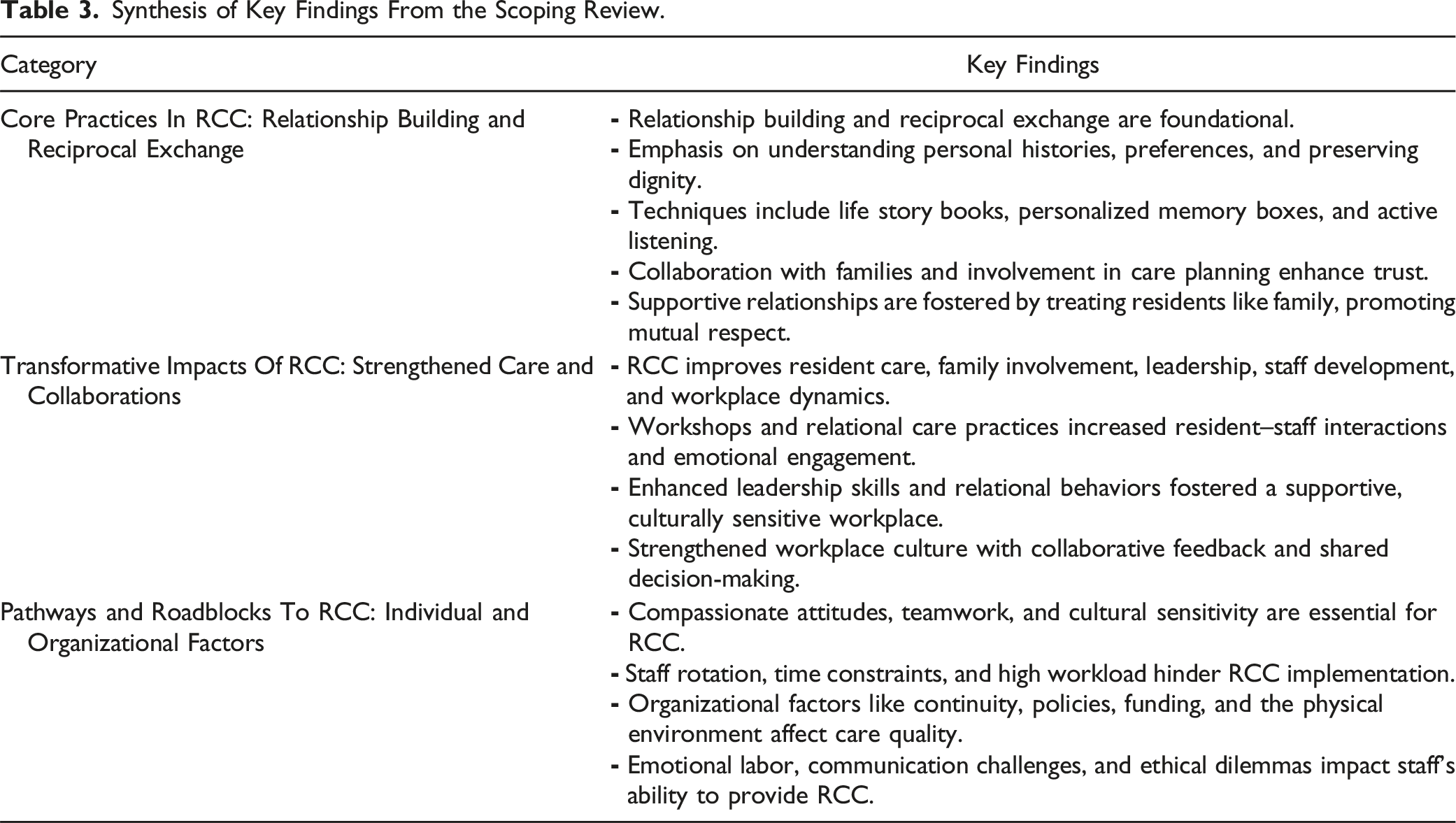
Core Practices in RCC: Relationship Building and Reciprocal Exchange
The foundation of RCC in LTC is built on relationship building and reciprocal exchange. This approach emphasizes understanding residents’ personal histories and preferences, preserving dignity while fostering trust, rapport, and supportive relationships and collaboration.
Understanding Personal Histories and Preferences
Relational care in LTC settings began with a deep understanding of residents’ personal histories and preferences. Staff document residents’ shared life experiences, cultural beliefs, and family bonds in life story books, which provided valuable insights into each resident (Wills & Day, 2008). Similarly, creating personalized memory boxes for residents with dementia, allowed staff to seamlessly integrate meaningful moments from residents’ past into daily routines, thereby strengthening relationships (Compton et al., 2022; Wilson et al., 2013). Such documentation was crucial for fostering personalized and empathetic care, creating an environment where residents felt understood and respected, ultimately enhancing their dignity and emotional well-being.
Preserving Dignity while Building Trust and Rapport
Preserving residents’ dignity while establishing and maintaining trust and rapport was essential for effective relational care. Residents’ relatives emphasized the importance of preserving dignity and autonomy by recognizing residents’ relational humanity and addressing their emotional needs (Heggestad et al., 2015; Marquis et al., 2004). Staff engaged in active listening, maintained curiosity, and involved families in care planning to better understand residents’ preferences and build strong, trust-based relationships (Andersen & Spiers, 2016; Barken & Lowndes, 2018; Dewar & MacBride, 2017; Walsh & Shutes, 2013). Moving beyond standardized care plans, staff needed to use their experiential knowledge and flexible approaches in care delivery, along with providing personalized care that respected residents’ dignity and emotional needs to foster mutual trust and connections (Andersen & Spiers, 2016; Dunn & Moore, 2016; Molterer et al., 2020; Walsh & Shutes, 2013). During the COVID-19 pandemic, customizing activities to align with residents’ identities and fostering one-on-one interactions were particularly important in strengthening connections between residents and staff (Dohmen et al., 2022). In dementia care, empathy and an appreciative approach were particularly crucial, as meeting deeper emotional needs extended beyond merely completing tasks (Watson, 2019).
Fostering Supportive Relationships and Collaboration
Collaborative efforts and reciprocal engagement were vital for effective relational care. Treating residents like family enhanced emotional well-being and fostered supportive relationships among residents, families, and staff (Allison et al., 2019). Many residents perceived staff members as friends, with approximately 70% forming such bonds (Compton et al., 2022). Staff across various roles, including dietary, housekeeping, and administrative, were crucial in initiating and sustaining these supportive relationships (Barken & Lowndes, 2018; Marquis et al., 2004; Wilson & Davies, 2009). Care staff, such as nurse practitioners (NPs), played a crucial role in involving residents and their families in decision-making, fostering a sense of importance for residents and engagement for families (Dewar et al., 2019; Ploeg et al., 2013). Staff also recognized and facilitated relationships between residents and their significant others, promoting well-being, nurturing reciprocal relationships, and fostering a harmonious community within LTC settings (Dohmen et al., 2022).
Care managers and staffs’ ongoing commitment and dedication to their roles, a strong sense of curiosity, openness and respect for colleagues’ diverse cultures, cultural sensitivity in teamwork, and self-reflection further promoted collaboration and relational care in LTC settings (Dewar et al., 2019; Dewar & MacBride, 2017; Sellevold et al., 2020). Active participation from relatives in care activities lead to meaningful contributions, collaboration, and a sense of reciprocity, highlighting the interconnectedness and shared responsibility within the caregiving environment (Aveyard & Davies, 2006; Wilson, 2009). Care relationships in LTC homes were multifaceted, encompassing need-oriented, friendship-like, familial, and reciprocal dynamics (Walsh & Shutes, 2013). Hradcová (2017) and Watson (2019) also emphasized the importance of reciprocal exchanges of emotions and needs in care relationships, particularly for residents with dementia.
Moreover, empathetic approaches fostered communal routines based on individual preferences (e.g., bedtime or bath time), promoting shared understanding among residents, families, and staff (Wilson & Davies, 2009). This shared understanding empowered residents to anticipate each other’s needs, fostering acts of reciprocity and negotiation while enabling families to appreciate staff’s efforts in meeting everyone’s needs (Wilson & Davies, 2009). Therefore, recognizing the roles and contributions of all stakeholders, including staff, residents, and families, was integral to an authentic relational care approach (Wilson & Davies, 2009).
Transformative Impacts of RCC: Strengthened Care and Collaborations
The transformative impacts of RCC are evident in the improved care and enhanced collaborations in LTC settings. RCC significantly enhances resident care, family involvement, leadership and staff development, workplace dynamics, and the delivery of culturally sensitive care.
Impact on Resident Care and Family Involvement
RCC significantly increased interactions and enhanced connections between staff, residents, and relatives. Workshops based on RCC principles led to a significant increase in meaningful resident interactions and participation in leisure activities (Wilson et al., 2013). Caring Conversations heightened staff awareness of effective human interactions and fostered emotional engagement with residents, families, and colleagues (Dewar & MacBride, 2017). Consistent relationships with staff also fostered a sense of security among residents (Watson, 2019).
Meaningful interactions, characterized by positive engagement, empathetic care, and strong rapport, reinforced residents’ sense of individuality (Heggestad et al., 2015) and improved their perceptions of care quality (McGilton et al., 2003). Residents’ positive views of relational care and staff engagement in relational behaviors were further associated with enhanced relationships and meaningful connections (McGilton et al., 2003). Increased relational behaviors among staff correlated with reduced levels of anxiety, fear, and sadness among residents, highlighting a positive impact on residents’ emotional well-being (McGilton et al., 2012).
Family involvement in daily life and decision-making significantly contributed to the social and emotional well-being of residents, especially those with dementia (Allison et al., 2019; Dewar et al., 2019; Marquis et al., 2004; Sellevold et al., 2019). Family participation in decision-making, as well as staff–family and resident–resident relationships, helped foster a homelike atmosphere in LTC settings for residents and families (Chamberlain et al., 2017). Relational care also helped relatives cope with the emotional challenges of placing loved ones in LTC, providing crucial support during end-of-life situations (Aveyard & Davies, 2006).
Leadership and Staff Development
RCC-based interventions have led to substantial improvements in LTC managers’ skills. Managers reported a 20% increase in active listening skills and a 16% increase in management and leadership abilities (Dewar et al., 2019). Additionally, staff empowerment increased from 63% to 96%, and managers’ ability to influence improved from 57% to 91% (Dewar et al., 2019). Managers also developed an enhanced comprehension of care culture (96%) and increased confidence, which led to personal growth and positive transformations in resident care, staff interactions, and residents’ QoL (Dewar et al., 2019). Embracing reflective practices allowed managers to gain self-awareness of their assumptions, facilitating relational leadership (Banerjee et al., 2021; Dewar et al., 2019). Managers began exploring new conversational approaches that promoted inclusive dialogue, collaborative ideas, and shared ownership of initiatives involving residents and relatives (Dewar et al., 2019). In turn, relational leadership empowered others, fostered shared understanding and collaboration, provided a sense of security and belonging, and promoted a culturally sensitive and positive organizational culture (Banerjee et al., 2021; Dewar et al., 2019; Heggestad et al., 2015; Sion et al., 2020; Watson, 2019).
Through self-reflection and group discussions facilitated by the relational care approach, care staff felt empowered to ask questions, express emotions, voice concerns openly, bridge hierarchical divides, and foster mutual understanding (Banerjee et al., 2021; Dewar et al., 2019; Dewar & MacBride, 2017). This empowerment nurtured respect, communication, problem-solving abilities, empathy, and overall professional development (Banerjee et al., 2021; Dewar & MacBride, 2017; Sellevold et al., 2019). Personalized caregiving interactions facilitated by RCC enhanced information continuity and communication among staff, positively influencing their sense of purpose and identity (Goodman et al., 2015; Gordon et al., 2018; Jablonski-Jaudon et al., 2016; Talbot & Brewer, 2016).
Enhanced Workplace Dynamics
Emotional sharing in the workplace improved understanding, communication, and conflict resolution, leading to better collaborative engagement (Dewar et al., 2019; Marquis et al., 2004). Collaborative efforts among staff from various units cultivated teamwork, enhanced communication regarding resident care, and contributed to staff feeling more valued by colleagues and families (Wilson et al., 2013). Collaborative efforts, in turn, enabled detailed and comprehensive feedback, fostering a culture of change and improvement, shared decision-making, and meaningful involvement within and beyond LTC homes (Aveyard & Davies, 2006; Cranley et al., 2020; Dewar et al., 2019). Staff also felt empowered to influence organizational policies and practices, leading to improved care practices and a more supportive and collaborative workplace culture (Banerjee et al., 2021). Staff perceived the development of strong relationships through relational care as one of the most fulfilling aspects of their work (Banerjee et al., 2015). Collaborative efforts, particularly between staff and relatives, fostered mutual respect and appreciation, which were essential prerequisites for building meaningful connections (Barken & Lowndes, 2018).
Culturally Sensitive Care
RCC honored and integrated cultural particularities into caregiving practices. The relational model of care embraced cultural nuances by accommodating cultural practices, providing access to religious support (e.g., rabbinical support), and using native language terms (Allison et al., 2019). Staff used terms of endearment in residents’ native languages, such as Russian words like diragaya and diragoy for “darling” and Yiddish terms like mamale or mamishka for “mother,” to strengthen familial bonds with residents (Allison et al., 2019). Multilingual staff practiced culturally sensitive care by communicating in the residents’ preferred languages (Allison et al., 2019).
Cultural understanding among staff about their diverse backgrounds also enriched teamwork and enhanced care delivery (Sellevold et al., 2019). This culturally sensitive approach ensured that care practices were respectful and inclusive, fostering a supportive environment for both residents and staff (Sellevold et al., 2019).
Pathways and Roadblocks to RCC: Individual and Organizational Factors
Implementing RCC in LTC settings is influenced by individual factors, such as compassion, teamwork, communication, and stress management, and organizational factors like continuity of care, funding, policies, and the physical environment.
Compassionate and Respectful Attitudes
Studies have shown that the attitudes and behaviors of staff significantly impact the quality of relational care provided to residents, particularly those with dementia. Compton et al. (2022), Heggestad et al. (2015), Hradcová (2017), Marquis et al. (2004), and Ploeg et al. (2013) found that respectful and compassionate attitudes, along with staff knowledge and competencies, enhanced the care experience for families and residents. Sellevold et al. (2019) emphasized the importance of respectful communication, including self-awareness, patience, politeness, and sensitivity, in creating a nurturing and secure environment. Additionally, staff’s deep understanding of residents’ health conditions fostered comfort and trust, essential for RCC (Ploeg et al., 2013).
Collaboration and Teamwork
Effective collaboration and teamwork, founded on mutual trust, were essential for promoting relational care. Strong team relationships, family trust, and positive rapport with residents were crucial for shared decision-making and implementing a relational approach (Aveyard & Davies, 2006; Cranley et al., 2020). Goodman et al. (2015) and Sellevold et al. (2019) highlighted the importance of collaborative team efforts. Cultivating mutual respect between families and staff through meaningful interactions and effective feedback improved the care experience for residents and their families, particularly during end-of-life processes (Barken & Lowndes, 2018; Marquis et al., 2004).
Continuity of Care and Staffing Issues
Continuity of healthcare staff and the overall care team significantly facilitated positive relationships, improved coordination, and reduced staff turnover (Gordon et al., 2018; McGilton et al., 2003; Watson, 2019). Conversely, staff rotation policies disrupted relationships and strained interactions with families (Watson, 2019). Leadership played an instrumental role in prioritizing relational care, while a focus on safety protocols and paperwork led to more transactional relationships (Wilson, 2009). The COVID-19 pandemic further challenged the maintenance of relational care due to necessary safety measures, such as physical and social distancing (Dohmen et al., 2022; Rutten et al., 2022). Collaborative efforts between volunteers, such as families, and staff helped mitigate some of these challenges, including residents eating alone at mealtimes (Keller et al., 2021).
Insufficient staffing hindered the implementation of RCC in LTC settings, especially during mealtimes, reducing relational behaviors (Compton et al., 2022; Hradcová, 2017; Marquis et al., 2004; McGilton et al., 2012; Trinca et al., 2021; Wu et al., 2018). Staffing shortages negatively impacted communication and trust between care workers and management, contributing to caregiver fatigue and limiting meaningful interactions with residents (Banerjee et al., 2015; Dunn & Moore, 2016). Frequent staff turnover and low engagement discouraged residents from sharing personal stories and led to low family satisfaction regarding residents’ needs (Compton et al., 2022). Further, staff turnover reduced interactions among residents and family satisfaction, highlighting the importance of dedicated and consistent staff time for effective RCC (Compton et al., 2022; Goodman et al., 2015).
Challenges in Acknowledgement and Communication
When providing relational care, there were ongoing challenges in recognizing residents’ humanity and navigating ethical dilemmas among healthcare providers. McGilton et al. (2012) observed that staff behaviors were more relational with cooperative residents during activities such as morning care and mealtimes. However, residents with dementia who had limited verbal communication often experienced difficulties in being acknowledged as relational human beings (Heggestad et al., 2015; McGilton et al., 2012). This underscored the need for staff to possess strong communications skills, including those related to interactions with residents with dementia, to ensure all residents feel recognized and respected (Heggestad et al., 2015; Hradcová, 2017).
Healthcare providers often felt vulnerable when addressing ethical challenges in dementia care, hesitating to discuss these issues with colleagues due to fears of judgment, which negatively impacted their professional self-esteem (Sellevold et al., 2019). Additionally, providers with minority language backgrounds struggled with communication issues, leading to potential misunderstandings (Sellevold et al., 2019). Cultural differences in perspectives on elderly care also resulted in conflicts and tensions among providers (Sellevold et al., 2019).
Workload and Emotional Strain
Routine- and task-oriented environments, along with time constraints, presented significant obstacles to promoting relational care, often leading to neglected resident needs and dignity (Daly & Szebehely, 2012; Dunn & Moore, 2016; Heggestad et al., 2015; Jones & Moyle, 2016; Talbot & Brewer, 2016). These routine tasks often led to depersonalized care and job dissatisfaction due to their focus on efficiency, whereas an integrated model involving staff in a broad range of activities, including relational and domestic tasks, promoted a more holistic approach to LTC (Banerjee et al., 2015; Daly & Szebehely, 2012; Wilson & Davies, 2009). Additionally, high workloads, excessive paperwork, perceived lack of management support, and hierarchical care structures created power imbalances and tensions among care workers (Andersen & Spiers, 2016; Banerjee et al., 2015, 2021; Heggestad et al., 2015; Hradcová, 2017; Jones & Moyle, 2016; Walsh & Shutes, 2013). Care aides’ dual roles of balancing resident well-being and supporting professionals also contributed to work overload (Andersen & Spiers, 2016).
The emotional labor inherent in caregiving roles highlighted the complexity of balancing emotional demands with physical care needs and professional standards (Andersen & Spiers, 2016; Daly & Szebehely, 2012; Talbot & Brewer, 2016; Watson, 2019). Staff often felt stressed and dissatisfied due to unrealistic family demands (Andersen & Spiers, 2016; Dohmen et al., 2022; Jones & Moyle, 2016). Balancing residents’ preferences with biomedical care standards was a significant challenge (Dewar & MacBride, 2017; Dunn & Moore, 2016) that worsened during COVID-19, as staff enforced isolation measures, further increasing emotional distress (Dohmen et al., 2022).
Organizational and Environmental Challenges
Inadequate funding and policies often hindered the implementation of relational care, creating a challenging work environment and concerns about care quality (Banerjee et al., 2015; Daly & Szebehely, 2012; Marquis et al., 2004). Tensions within organizational documents in LTC settings complicated the implementation of relational care, highlighting conflicts between personalized care ideals and regulatory pressures (Venturato et al., 2013). Banerjee et al. (2015) and Hradcová (2017) underscored discrepancies between documented care practices and the real-life experiences of residents and care workers due to diverse interpretations of care across contexts and relationships.
The physical environment of care facilities significantly influenced relationships among residents, families, and staff. A homelike environment, with private areas for family interactions, fostered strong connections and overall satisfaction (Marquis et al., 2004; Wilson, 2009). In contrast, poor facility layout and a bustling environment disrupted care and hindered the implementation of RCC (Keller et al., 2021; Watson, 2019; Wilson, 2009). Additionally, technology offered opportunities to enhance care practices and improve resident well-being (Eyers et al., 2013).
Discussion
This scoping review examines current knowledge on RCC in LTC for older adults, identifying essential practices such as personalized engagement, empathy, and family involvement. Rooted in Nolan et al.'s (2004, 2006, 2008) Senses Framework and Dewar’s (2011) Caring Conversations framework, RCC emphasizes relational interactions to improve care quality and resident well-being. The Senses Framework’s six principles—Security, Continuity, Belonging, Purpose, Fulfillment, and Significance—underscore the importance of LTC environments that address residents’ physical, emotional, psychological, and social needs. Practices like honoring residents’ histories, building trust, and involving family in care decisions (Barken & Lowndes, 2018; Compton et al., 2022; Wilson et al., 2013) support these principles, especially Continuity, Belonging, and Security.
Our findings show that core RCC practices, such as preserving residents’ dignity and involving family, align with the Senses Framework and reinforce existing PCC research (Opperta et al., 2018; Schenell et al., 2020). The Caring Conversations framework further enhances RCC by fostering empathy, curiosity, and openness, transforming routine interactions into meaningful connections. However, structural issues in LTC—such as high staff turnover, regulatory constraints, and heavy workloads—often hinder the consistent application of these principles. These barriers limit staff engagement in relational practices, reducing RCC’s impact on resident well-being (Banerjee et al., 2021; Compton et al., 2022).
RCC has transformative impacts on resident well-being and family empowerment (Allison et al., 2019; Chamberlain et al., 2017), aligning with the Senses and Caring Conversations frameworks’ focus on inclusive, supportive environments. Research shows that meaningful relationships boost residents’ emotional well-being, improve care quality, and enhance family satisfaction (Hayward et al., 2022; Schenell et al., 2020; Sjögren et al., 2013). However, this review raises concerns about whether LTC environments consistently have the resources to fully support RCC. Family empowerment aligns with Belonging and Collaboration; however, limited resources and rigid protocols often hinder involvement, especially in institutionalized settings (Bhattacharyya et al., 2022; Söderman et al., 2018; Thompson et al., 2021). This highlights the need to assess the feasibility of implementing these frameworks in resource-limited LTC settings and to study potential adverse outcomes. While this review highlights RCC’s benefits, gaps remain in addressing potential adverse outcomes in LTC, warranting further study.
The pathways and roadblocks to implementing RCC underscore both its potential and the complexity of establishing meaningful relational care in LTC settings. The Senses Framework and the Caring Conversations framework highlight the importance of supportive leadership, continuity, empathy, and collaboration as foundational to RCC. However, our findings reveal a tension between these relational ideals and the practical challenges of LTC environments. While relational skills and compassionate attitudes are vital, without targeted organizational changes to support manageable workloads and sustainable practices, the transformative potential of RCC may remain aspirational (Compton et al., 2022).
The COVID-19 pandemic highlighted challenges in RCC as infection control measures often conflicted with the Senses of Belonging and Continuity, disrupting routines and restricting family visits, which weakened residents’ sense of security and connection (Iyamu et al., 2023). The LTC sector must balance infection control with RCC’s holistic principles to support resident well-being and relational care. This review, alongside prior research (Backman et al., 2021; du Toit et al., 2020; Rutten et al., 2021), underscores the importance of supportive leadership and stakeholder engagement in strengthening RCC, fostering resilience, and realizing the Senses and Caring Conversations ideals.
Grounding these findings in the Senses Framework and Caring Conversations illuminates both the promise and limitations of RCC in LTC. While these frameworks present a compelling vision for relationship-centered environments, they also highlight the need for practical policy and structural changes to make relational ideals achievable and sustainable within LTC settings.
Implications for Policy and Practice
The scoping review suggests key policy and practice implications based on broad findings. Comprehensive staff training can foster compassion, effective communication, and understanding of residents’ histories, enhancing reciprocal relationships (Compton et al., 2022; Heggestad et al., 2015). Policies promoting teamwork and family involvement may improve shared decision-making and create a homelike environment (Allison et al., 2019; Dewar et al., 2019). Lessons from COVID-19 can inform RCC improvements, such as technology use, refined staff rotation, and infection control (Eyers et al., 2013; Iyamu et al., 2023). Addressing systemic barriers in LTC can further enhance care outcomes and foster a collaborative environment for residents, families, and staff.
Limitations
The inclusion criteria focused on studies from Australia, Europe, New Zealand, and North America to enable a targeted analysis of regions with similar LTC systems (European Observatory on Health Systems and Policies, 2021; OECD, 2021). However, due to each country’s unique approach, findings should be interpreted cautiously. While including other regions would increase diversity, this review was limited to Western contexts, as addressing healthcare system heterogeneity was beyond its scope. Additionally, the absence of reported disadvantages of RCC in current literature limits a comprehensive assessment of its impact, highlighting a need for further research on potential drawbacks. Quality assessment was not conducted in line with the scoping review’s purpose to broadly map existing literature (Joanna Briggs Institute, 2020), a limitation that calls for cautious interpretation of policy and practice recommendations.
Future Research
Future research needs to engage diverse participants—residents, families, and healthcare providers—using varied methods to fully capture RCC practices and impacts (Compton et al., 2022; Cranley et al., 2020). Including diverse ethnic groups is essential for culturally sensitive and equitable RCC, as examining RCC across cultural contexts can reveal its adaptability, benefits, and challenges (Sellevold et al., 2019). Further research on potential adverse outcomes is also needed to understand RCC’s full impact across settings beyond LTC, such as ALFs and community-dwelling environments.
Conclusion
This scoping review examined RCC in LTC settings for older adults, highlighting core practices, transformative impacts, and implementation challenges. It reveals a growing body of evidence on RCC’s positive outcomes, alongside significant gaps regarding potential adverse effects and persistent barriers to implementation. Overall, this review offers a comprehensive foundation on RCC’s key elements, benefits, and challenges, providing valuable insights for future research and practice to improve care experiences.
Footnotes
Author Contributions
The scoping review was conducted by the first author, with the second author contributing by refining the research questions, search strategies, databases, and study selection process, as well as making substantial contributions to the editing and revision of the manuscript. Both authors have read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Alzheimer Society of British Columbia and the Social Sciences and Humanities Research Council of Canada [grant number 752-2022-1977].