
Abstract
To compare lighting levels in care facilities with local recommendations and determine their cross-sectional association with fall rate, we recruited residents (n = 126) from 12 long-term care facilities (mean ± SD age 85.1 ± 7.9 years; 64.3% female). Lighting levels were measured at different times in various areas within facilities, according to each resident’s movements and habitual use of light. Lighting fell short of focused activity recommendations in 57.7% of bedrooms and 68.5% of bathrooms (bathing and toileting areas); 22.8% and 41.9%, respectively, were also below general activity recommendations. Lower bedroom and overall lighting correlated with higher fall rates (all p < .05). Covariate-adjusted negative binomial models showed lighting in dining rooms (incidence rate ratio [IRR] = 0.92 (95% CI 0.87–0.98; p = .005) for 100 lux increase), bathrooms (IRR = 0.87 [0.78–0.98]; p = .016), and overall (IRR = 0.91 [0.83–1.00]; p = .03–.04) predicted lower fall rates. Areas used by care facility residents commonly have lower than recommended lighting levels, which increases fall risk.
• Lighting levels may influence falls in long-term residential care facilities for older people, yet there are few studies of lighting levels in this environment. This study quantifies lighting deficiencies in residential care and their impact on fall rates. • Lighting in long-term residential care facilities for older people was often below recommended levels, particularly in bedrooms and bathrooms. • Lower light exposure, overall and in bedrooms, was associated with higher fall rates among residents. In adjusted regression models, overall lower light exposure and that in dining rooms and bathrooms (bathing and toileting areas) predicted lower fall rates.
• By identifying that many areas within care facilities do not meet recommended lighting levels and that low lighting is associated with fall risk, our study highlights an actionable area for targeted interventions. • This is particularly important for residents with visual, cognitive, or physical impairments, which exacerbate the risk of poor lighting conditions.What this paper adds
Application of study findings
Introduction
Falls are a significant concern and major public health issue among older adults, particularly those residing in long-term residential care facilities. The consequences of falls can be severe, leading to injuries, loss of independence, and mortality (Carryer et al., 2017; Florence et al., 2018). As the global aging population grows, the prevalence of falls in residential care facilities has become an urgent and multifaceted challenge, with an estimated frequency ranging from 1.7 to 3.6 falls per person per year (Cameron et al., 2018; Wabe et al., 2022). Therefore, an in-depth understanding of the factors influencing falls is essential for creating a safe environment that reduces the risk of falls and upholds the autonomy of residents.
Adequate lighting is likely to be particularly important for fall prevention in residential care residents, who may also have age-related visual, cognitive, and physical impairments (De Lepeleire et al., 2007; Ramulu et al., 2021; Rimland et al., 2016; White et al., 2015). An upgrade of lighting in two New England care homes was recently reported to reduce fall rate by 43% compared to two control facilities (Grant et al., 2022). The photobiological effect of lighting is known as illuminance, which is the perceived intensity, to the human eye, of light hitting or passing through a surface, measured in lux (1 lux = 0.093 foot-candles). A lux is approximately equal to the illuminance produced on a surface area of 1 m2, 1 m from the light of a common wax candle (1 candela), emitted in a unit solid angle (steradian) (1 lumen) (CIE, 2020). Lux from natural sources ranges from 0.0001 for starlight on a moonless, overcast night; 0.002 on a moonless, clear night sky; 0.27 with a full moon overhead; 10 at twilight; 100 on a very dark overcast day; 1000 on an overcast day up to 10,000–25,000 in full daylight (not direct sun) (Schlyter, 2023).
Inter-relationships between physical function, vision, cognitive function, and lighting in fall etiology are complex. Vision, which requires adequate ambient light, plays an important role in perceiving environmental hazards and maintaining postural stability; adequate vision allows better identification of potential fall risks and more appropriate responses (Mehta et al., 2022; Saftari & Kwon, 2018). However, visual function is influenced by cognitive impairment, which can lead to difficulties in maintaining balance, coordinating walking, and accurately perceiving obstacles in the environment, potentially increasing the susceptibility to falls (Minta et al., 2023; Racey et al., 2021). Bright lighting directly enhances cognitive performance, and appropriate daytime lighting also indirectly improves cognitive function through improved sleep and reduced depression (Turner et al., 2010). Reduced mobility among older adults is a risk factor for falls (Jadczak et al., 2022; Kuo et al., 2022); attributes such as balance, gait, flexibility, and muscle strength can reduce fall risk in care homes (Bauman et al., 2014; Gulka et al., 2020; Hayashi et al., 2023; Scronce et al., 2020). It is unclear how these physical attributes might interact with levels of lighting and changing cognitive function to influence falls risk.
In recent years, lighting has become of more recognized importance in the design of long-term care facilities for older people (Deandrea et al., 2013; Figueiro et al., 2012; Grant et al., 2022). Adequate lighting is essential for creating a safe living environment, facilitating residents’ sleep, mental and cognitive health (Turner et al., 2010), and navigation (Tuaycharoen, 2020) and minimizing the risk of tripping and stumbling (Ramulu et al., 2021). In New Zealand, a building industry advisory group has developed sustainable building guidelines, which include specific lighting recommendations tailored to various activities (Level: The Authority on Sustainable Building, 2021For general household tasks like washing, lighting levels between 150 and 200 lux are advised. Focused activities such as reading require lighting levels ranging from 300 to 500 lux, while lighting levels between 800 and 1000 lux are recommended for concentrated activities like fine detail sewing. We have assessed the effectiveness of lighting in this study in relation to these guidelines.
Despite the acknowledged importance of lighting conditions, there are still limited data on lighting levels within care homes, or an understanding of how lighting affects fall risk in this environment, considering the role of fall risk factors such as reduced vision, physical and cognitive performance, and habitual mobility in modifying the effect of lighting on falls. Therefore, this study aimed to assess lighting levels in long-term residential care facilities for older people in relation to local guidelines and determine the bivariate cross-sectional association of lighting levels with fall risk in this environment and whether lighting predicted falling after adjusting for other risk factors.
Methods
Participants were long-term care residents 65 years or over, recruited as a subsample of the Staying Upright in Residential Care study, a randomized controlled trial of group exercise for falls reduction, involving 520 participants from 25 facilities (Taylor et al., 2024). Residents who were acutely unwell, immobile, or under psychogeriatric, respite, or palliative care were excluded. Participants who were able gave informed written consent before enrollment. For those unable to give informed consent, the facility clinical lead, with support of family, provided written consent. Ethical approval was obtained from the Northern B Health and Disability Ethics Committee, with additional lighting and life-space mobility measurements as a later amendment (18/NBT/151/AM06).
Methods of collection of demographic and health-related data have been previously described (Taylor et al., 2020). Briefly, falls were recorded using each facility’s incident report forms using routine, standardized reporting systems. Fall location, when available, was determined from incident descriptions. Baseline physical performance was measured using Short Physical Performance Battery (SPPB) (Guralnik et al., 1994), and cognitive function was measured using the Montreal Cognitive Assessment (MoCA) (Nasreddine et al., 2005). Other demographic and vision data were collected from the standardized minimum database used in residential care facilities in this country (the International Resident Assessment Instrument [interRAI] ;Long-Term Care Facilities assessment, interRAI™). The interRAI vision tool uses a 5-point scale: 0 adequate, 1 minimal difficulty, 2 moderate difficulty, 3 severe difficulty, and 4 no v
To measure lighting for this substudy, between August, 2021 and October, 2022 caregivers were asked to confirm the areas of the facility used by each participant and their usual use of available artificial lighting. For each participating resident, light was measured in the appropriate bedroom, bathroom(s) (including shower/bathing/toilet area(s)), dining room, lounge/activity area, and hallway(s). When a resident used multiple locations within an area category, for example, different toileting and bathing locations, a weighted average was calculated based upon the frequency of use. Light measurements were taken using Digitech-QM1587 light meters (Jaycar, Rydalmere, NSW, Australia). An average of six measurements taken on two occasions in the subjectively determined brightest spot, darkest spot (at least 1 m away from the wall), and center of each area was recorded for analysis. When data were missing, averages of the available measures were used.
Life-space mobility data were collected from caregivers for each participant using the Nursing Home Life-Space Diameter (NHLSD) tool (Tinetti & Ginter, 1990). This tool provides an index of overall habitual mobility based on the frequencies of movement within the resident’s room, unit, facility, and outside. As an addition to this tool, we assessed the specific frequency of visits to toilet/washing area (bathroom), dining room, and lounge/activity areas.
Fall-rate was calculated by dividing the number of falls by the total follow-up time for each participant (falls/person-year). Three overall indices of lighting were calculated: a simple average of all five areas, an average weighted for the frequency of use of each area category, and a weekly lighting-exposure index calculated as the sum for all areas of the multiple of lighting level and weekly visit frequency for each area.
The distribution of fall rates and light measures were skewed, so medians and interquartile range (IQR) were reported for descriptive data and non-parametric statistical tests were applied. Bootstrapping was used to obtain 95% confidence intervals for median estimates of lighting levels (Visalakshi & Jeyaseelan, 2014). Spearman’s correlation coefficients were reported for bivariate associations of average light measures for each area with fall rate. Differences in lighting levels between fallers and non-fallers were analyzed using the Mann–Whitney test.
Negative binomial regression models, offsetting the number of falls with person-years of follow-up, were used to assess whether lighting levels in each area and overall levels were associated with fall rates. The analyses were conducted without adjustment and then adjusted using backward stepwise regression (Pout ≥0.05) to derive a final model for each lighting area. The variables initially included in the adjusted analyses were age, gender, visual difficulty, physical performance, cognitive function, life-space diameter, and study allocation. With eight variables included in regression models, we estimated a required sample size of at least 120 (15 per variable). Data were analyzed using SPSS version 29.0 (IBM Corporation) with a level of statistical significance set to p < .05.
Results
Characteristics of the Study Population
Characteristics of Participants in the Substudy.
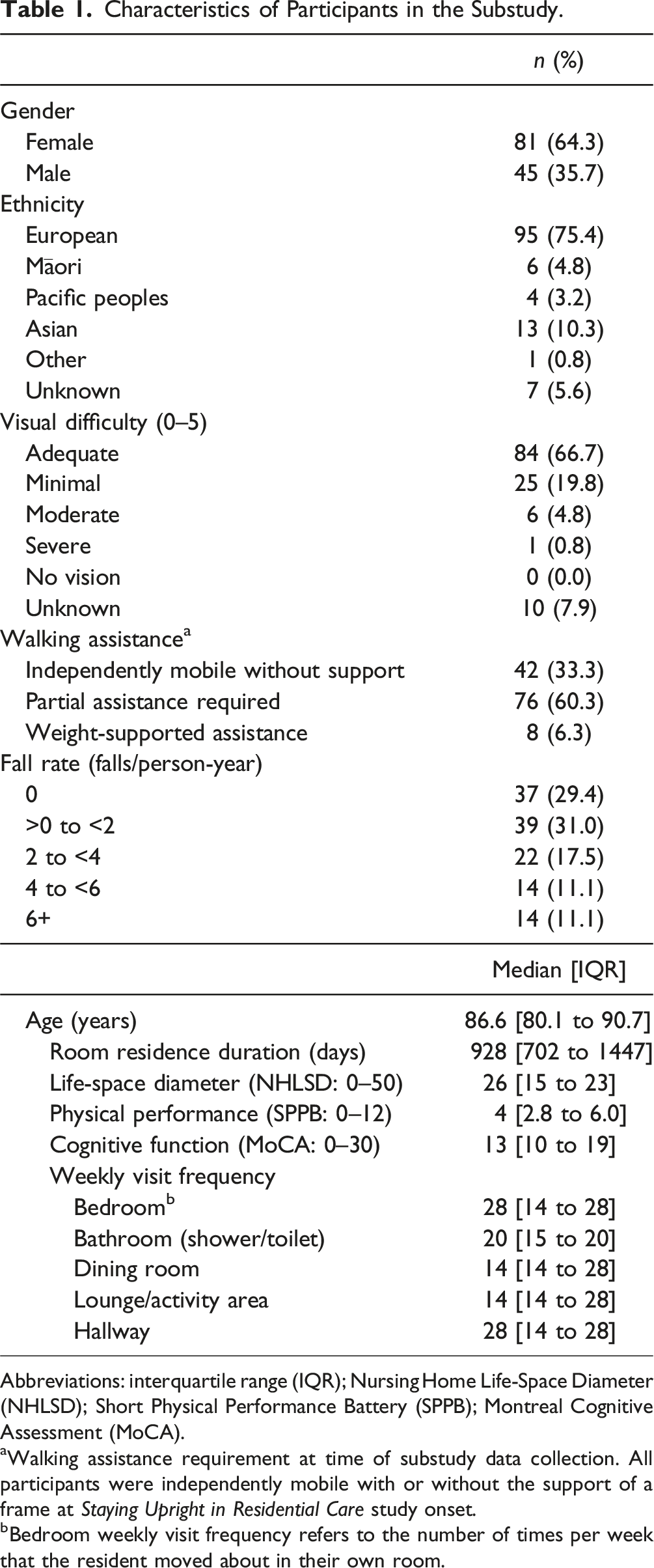
Abbreviations: interquartile range (IQR); Nursing Home Life-Space Diameter (NHLSD); Short Physical Performance Battery (SPPB); Montreal Cognitive Assessment (MoCA).
aWalking assistance requirement at time of substudy data collection. All participants were independently mobile with or without the support of a frame at Staying Upright in Residential Care study onset.
bBedroom weekly visit frequency refers to the number of times per week that the resident moved about in their own room.
Over the study follow-up period (median 1.82 years; IQR 1.26–2.03 years), 89 (70.6% of) participants fell a total of 823 times, between 1 and 225 times each. Fallers reported a median (IQR) of 4 falls (2–8) and a fall rate of 2.56 (1.24–4.98) falls per person-year. The overall fall rate (including fallers and non-fallers) was 1.28 (0.00–3.34).
Fall location could be ascertained for 481 falls (58%). Of these, over half (57.4%) occurred in the participant’s bedroom, 11.4% in the toilet or shower area (bathroom), 4.4% in the dining room, 9.6% in the lounge or activity area, 9.1% in a hallway or lobby, and the remaining 8.1% in another area inside or outside within the facility or away from the facility. The 61 bedroom fallers (48% of all participants) fell 3 times (1–5) with a bedroom fall rate of 1.41 (0.68–2.97) bedroom falls per person-year.
Lighting Levels
Median light levels for each facility area used by participants met or exceeded the recommended range of 150–200 lux for general activities, with an overall median (95% CI) of 386.3 [358.7–417.9] lux (Figure 1). Median levels of light in bedrooms 261.6 lux [210.8–307.6] and bathrooms 195.1 lux [148.9–247.1] fell below the recommended range of 300–500 lux for focused activities (Figure 1). Comparison of median light levels across different areas of the facilities used by participating residents. Error bars show 5th and 95th percentiles. Two data points (one each for bathroom and lounge) lie outside the y-axis limits and are not shown.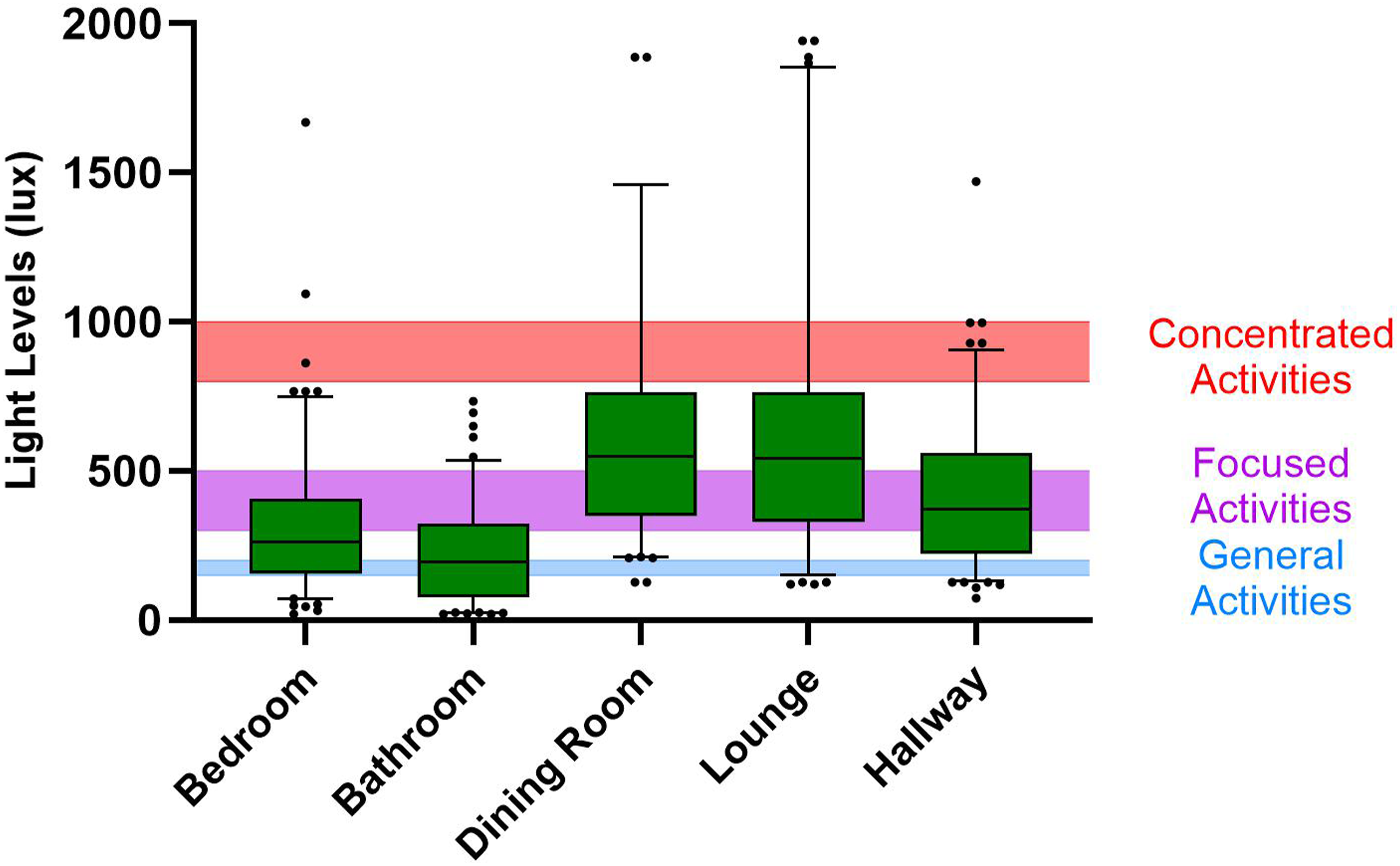
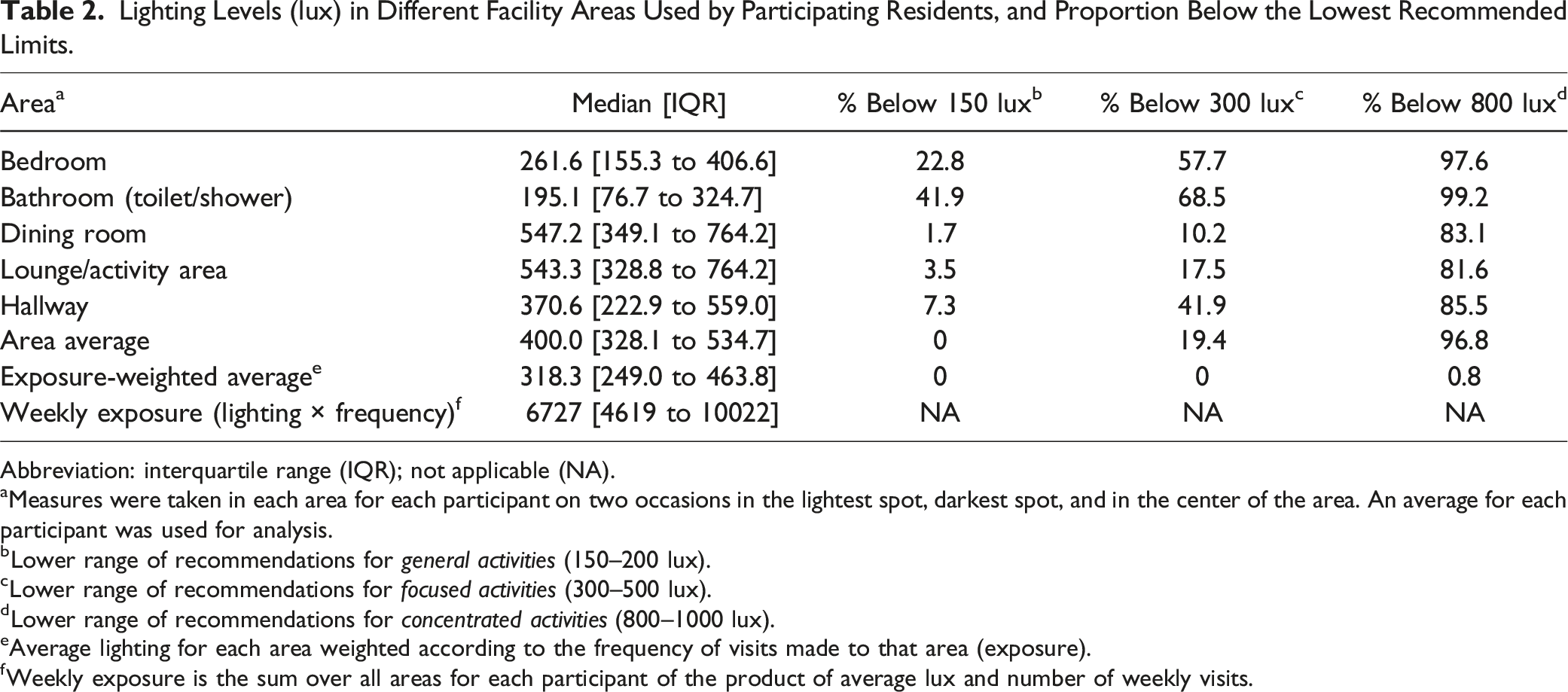
Lighting Levels (lux) in Different Facility Areas Used by Participating Residents, and Proportion Below the Lowest Recommended Limits.
Abbreviation: interquartile range (IQR); not applicable (NA).
aMeasures were taken in each area for each participant on two occasions in the lightest spot, darkest spot, and in the center of the area. An average for each participant was used for analysis.
bLower range of recommendations for general activities (150–200 lux).
cLower range of recommendations for focused activities (300–500 lux).
dLower range of recommendations for concentrated activities (800–1000 lux).
eAverage lighting for each area weighted according to the frequency of visits made to that area (exposure).
fWeekly exposure is the sum over all areas for each participant of the product of average lux and number of weekly visits.
Bivariate Associations Between Light Levels and Fall Rate
Lighting Levels as Predictors of Fall Rate in Unadjusted Negative Binomial Regression Models. a
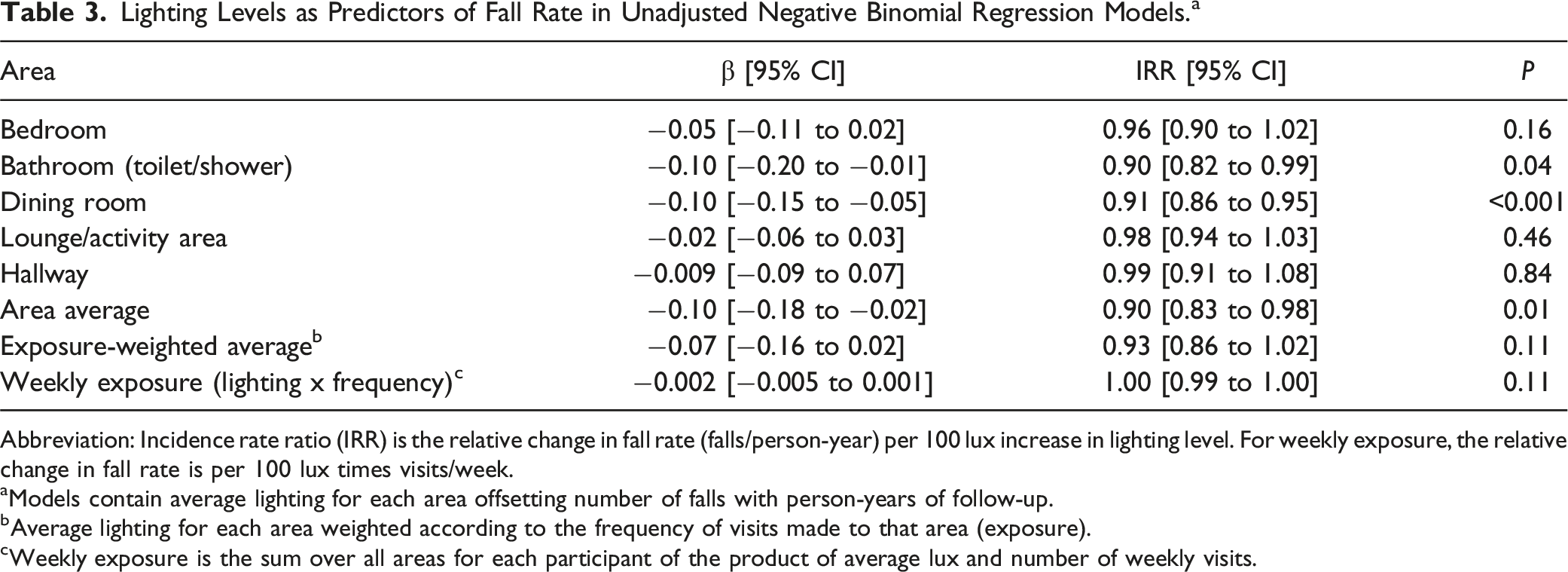
Abbreviation: Incidence rate ratio (IRR) is the relative change in fall rate (falls/person-year) per 100 lux increase in lighting level. For weekly exposure, the relative change in fall rate is per 100 lux times visits/week.
aModels contain average lighting for each area offsetting number of falls with person-years of follow-up.
bAverage lighting for each area weighted according to the frequency of visits made to that area (exposure).
cWeekly exposure is the sum over all areas for each participant of the product of average lux and number of weekly visits.
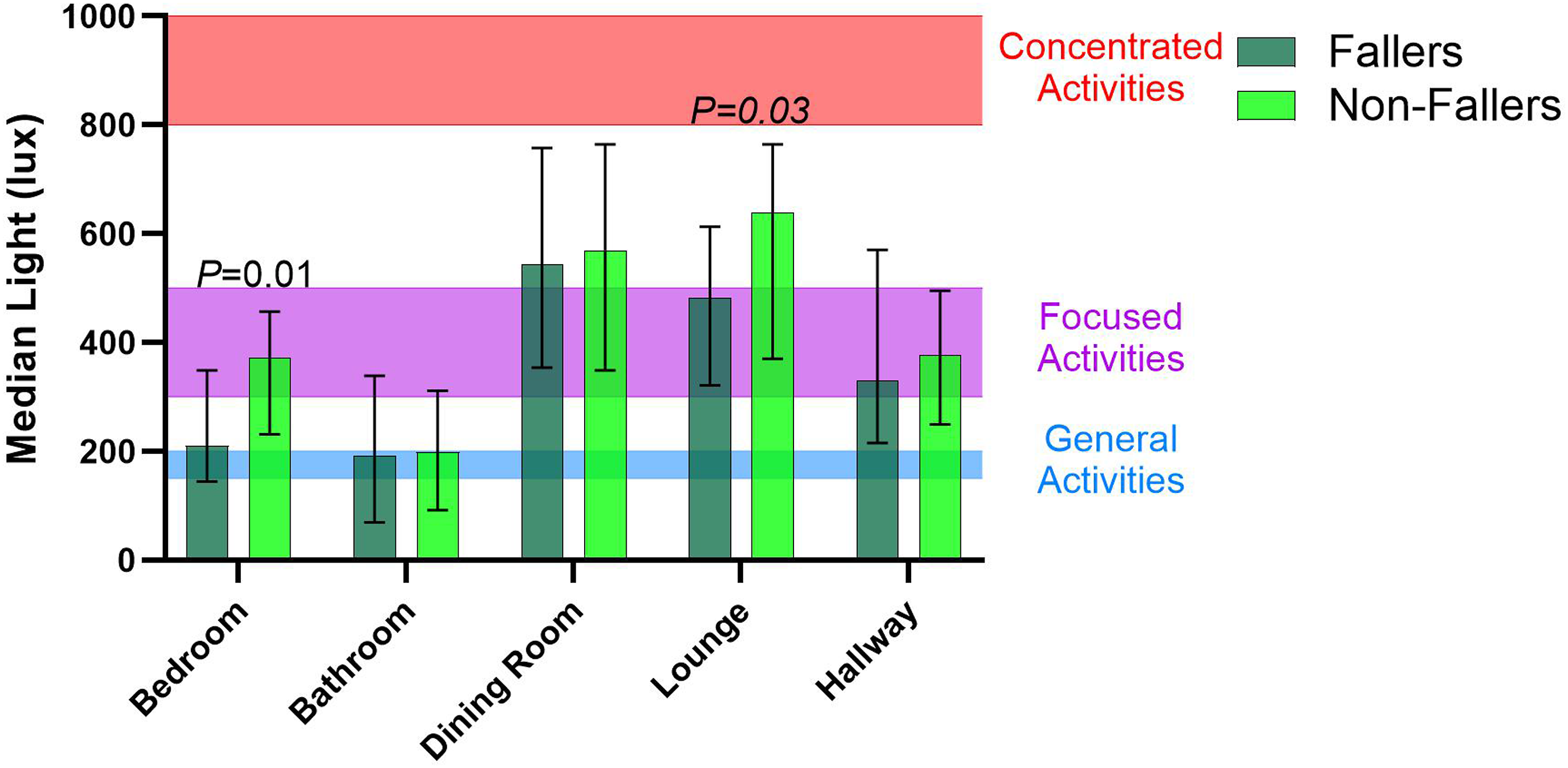
Comparison of light scores across the areas used by fallers and non-fallers. Error bars show interquartile range (IQR); p-values indicate significant differences between fallers and non-fallers.
There was no significant correlation between bedroom lighting and falls that occurred in the bedroom (rho = −0.04, p = .66), nor a difference in bedroom lighting between bedroom fallers and non-fallers (U = 1886, p = .98). Greater total weekly lighting exposure was correlated with a lower bedroom fall rate (rho = −0.19, p = .04) but was not different between fallers and non-fallers (U = 1623, p = .14).
Negative Binomial Regression Analysis for Independent Predictors of Falls
Final Models for Lighting Variables Significantly Predictive of Fall Rate.
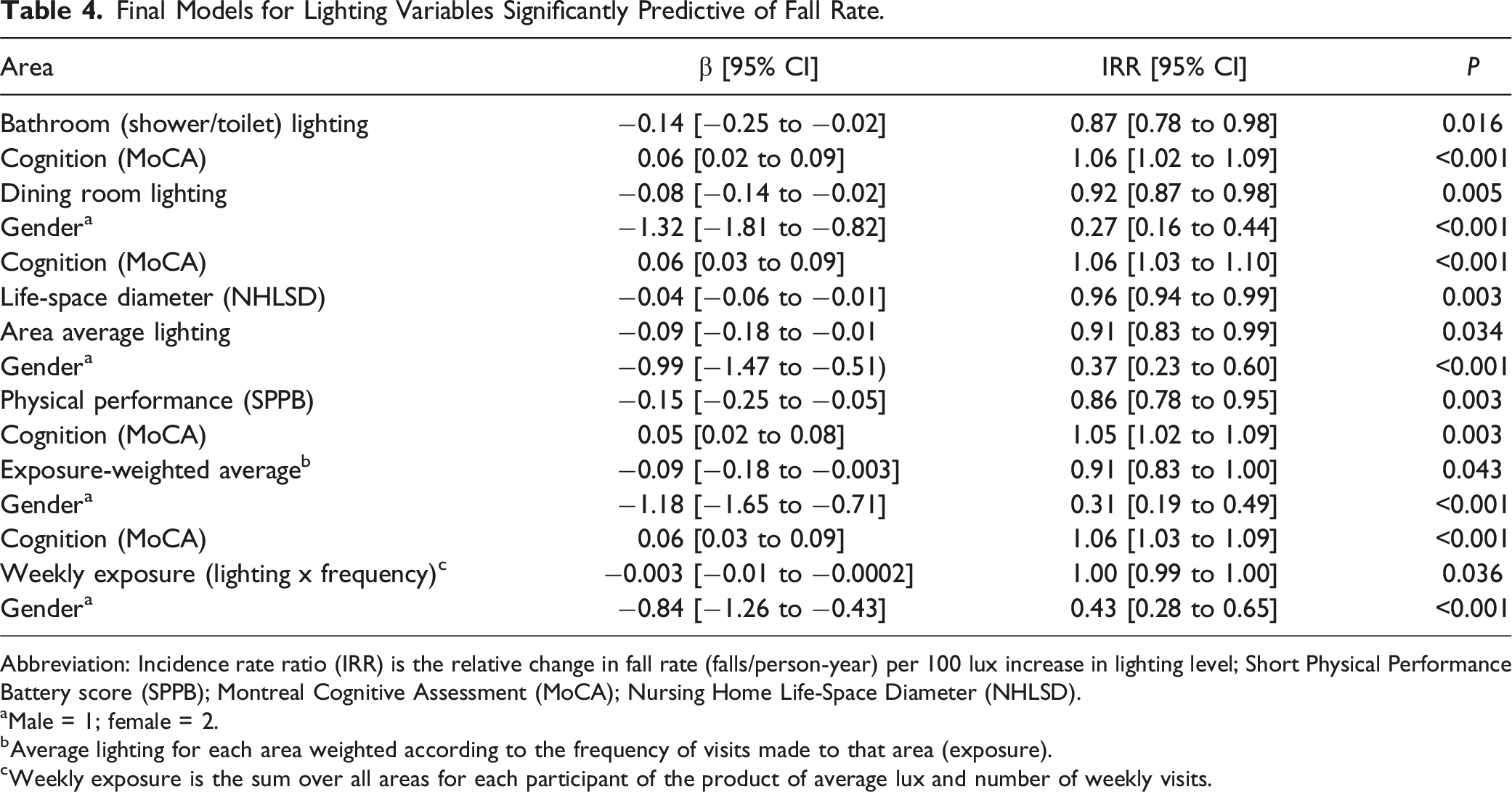
Abbreviation: Incidence rate ratio (IRR) is the relative change in fall rate (falls/person-year) per 100 lux increase in lighting level; Short Physical Performance Battery score (SPPB); Montreal Cognitive Assessment (MoCA); Nursing Home Life-Space Diameter (NHLSD).
aMale = 1; female = 2.
bAverage lighting for each area weighted according to the frequency of visits made to that area (exposure).
cWeekly exposure is the sum over all areas for each participant of the product of average lux and number of weekly visits.
When age, gender, visual difficulty, physical performance, cognitive function, life space diameter, and study allocation were included in backward stepwise regression models, lighting in bathrooms (p = .02) and dining rooms (p = .005), as well as average lighting (p = .03), exposure-weighted average lighting (p = .04), and weekly lighting exposure (p = .04), were retained in the final models as independent predictors of fall rate (Table 4).
Discussion
Our study provides evidence that lighting in long-term care facilities for older people is commonly below recommended levels and independently predicts falls. Though median levels of light exceeded the local recommendation for “general” activities, almost a quarter of bedrooms and over four in ten bathrooms (bathing and toileting areas) didn’t meet this standard. Most bedrooms and bathrooms failed to attain the brighter recommendation for “focused” activities, and lighting levels were frequently below this for other areas of care facilities. These findings are consistent with prior research emphasizing inadequate lighting conditions prevalent in residential care facilities (De Lepeleire et al., 2007; Grant et al., 2022; Sinoo et al., 2011).
The local guidelines that we have used here as benchmarks are designed for general building purposes and may not be appropriate for care homes. We have reported proportions of areas used by participants which recorded an average of six lighting measurements below 150 lux (general activities) and below 300 lux (focused activities). These thresholds are similar to adapted European standards for corridor, bathroom, and general room lighting used by De Lepeleire et al. (2007) though some authors have suggested that even higher lighting levels are required for people over 85 years. For example, Sinoo et al. (2011) have recommended that common rooms within care homes should be at least 750 lux. In this study, approximately one-quarter of dining rooms and lounge/activity areas would have met a 750-lux threshold, and very few bedrooms, bathrooms, or hallways.
In simple bivariate relationships, we found significant inverse associations between bedroom lighting and fall rates, and lower bedroom lighting levels in fallers versus non-fallers. Since long-term care residents moved about in their own rooms more frequently than other facility areas, apart from hallways which were visited an equivalent number of times per week, and this study found most falls were in bedrooms, addressing lighting in this area might be particularly important. However, we did not show that bedroom lighting was related to falling in the bedroom, albeit with reduced statistical power for this analysis. Furthermore, our regression analyses revealed more complex relationships, with greater lighting in dining rooms and, to a lesser degree, bathrooms and overall lighting indices, being protective of fall rates. Possibly, lighting in dining areas and bathrooms correlated with overall facility lighting, and so were the most strongly predictive of falls.
These findings align with previous studies that have emphasized the influence of lighting conditions on fall risk in other contexts, namely, in the home (Osibona et al., 2021; Ramulu et al., 2021) or hospital settings (Mazharizad et al., 2015). Inadequate lighting can pose significant fall risks by compromising visibility and increasing tripping hazards (Ticleanu, 2021), highlighting the importance of addressing lighting deficiencies in residential care facilities.
Improvement of lighting levels may require changes in building and interior design that optimize ambient light and include sufficient lighting infrastructure. Facility management should be alerted to the importance of installing bulbs with ample luminescence (Grant et al., 2022), and industry-targeted education could focus on improving habitual use of available lighting by care staff and residents, particularly within bedrooms and bathrooms. By prioritizing adherence to recommended lighting guidelines, care homes could reduce fall risk and proactively enhance safety.
Falls in the care home environment have multiple causes, which may interact with both mobility and lighting. Although the variables that were retained in our regression models with lighting levels, as independent predictors of fall rate, differed depending on the facility area, in all models either cognitive function, gender (with men having a higher fall rate than women), or both these variables were retained. Cognitive function has been previously shown to influence falling in older adults (Mirelman et al., 2012), and our results show that this relationship may remain irrespective of lighting levels.
Several limitations should be acknowledged in this study. Firstly, the sample size, while sufficient for overall analysis of fall rate predictors, may have constrained the ability to detect more subtle effects or associations. Due to COVID-related delays, only around half of the original facilities were approached to take part in the substudy. Furthermore, no data could be collected for some participants from participating facilities as they had died. Additionally, there may have been insufficient statistical power to determine whether lighting was specifically associated with falls in the same area. Because falls were established from incident report forms, we did not have precise data for the exact location of falls or lighting at that time. Variations in lighting in different parts of the same area, at different times of the day or of the year, and with differing weather conditions or use of artificial lighting may have obscured the relationship with falls. By addressing the relationship between lighting and fall rate in a larger study, a clearer picture of the multifaceted nature of fall risk in residential care facilities could be gained, allowing the development of effective targeted interventions and guidelines.
A final limitation is that in this study, we have measured only the degree of illumination in an area, which does not account for other features that aid visual perception of the environment. Low-level night lighting that enhances vertical and horizontal information, such as doorways and walking paths, has been shown to improve gait in older adults, compared to night lighting alone (Figueiro et al., 2011, 2012). A recent pilot study has shown promising, but not statistically significant, reductions in fall incidence in older people with dementia following installation of vertical and horizontal strip light-emitting-diode (LED) lighting around door frames (Zimmerman et al., 2024). Prospective observational studies or controlled trials that document fall rates following improvements to lighting levels, lighting that enhances visual cues, or educational interventions promoting the use of lights to prevent falls are needed.
In conclusion, this study identified suboptimal lighting in long-term care facilities for older people and an association of lower lighting levels with fall risk in this setting. Adequate lighting levels play an important role in reducing fall risk; residential care facilities should prioritize compliance with recommended lighting standards and enhance lighting infrastructure and education and training with respect to lighting to create a safer environment for residents. The multifactorial nature of fall-risk factors has been highlighted, emphasizing the importance of considering lighting as part of an integrated approach to reducing falls that helps foster mobility and independence while establishing a safer environment.
Supplemental Material
Supplemental Material - Shedding Light on Falls: The Effect of Lighting Levels on Fall Risk in Long-Term Residential Care Facilities
Supplemental Material for Shedding Light on Falls: The Effect of Lighting Levels on Fall Risk in Long-Term Residential Care Facilities by Yasaman Emad, Sonja P. Neef, Lynne Taylor, Ngaire Kerse, Alana Cavadino, Simon A. Moyes, Kate Comber, Xiaojing S. Wu, Janine Molloy, and Catherine J. Bacon in Journal of Applied Gerontology
Footnotes
Acknowledgments
The authors gratefully thank the residents, management, and staff from participating facilities who supported data collection.
Author Contributions
CJB, LT, NK, YE, and SN conceived and designed the study. LT, CJB, KC, YE, XW, and JM contributed to acquisition of subjects or data collection. YE, SN, CJB, AC, and SAM contributed to analysis and interpretation of data. YE, CJB, and SN drafted the work, and all authors critically reviewed it and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This original study was supported by the Health Research Council of New Zealand (Reference HRC 18-414). HOPE Foundation for Research on Ageing (New Zealand) supported a summer scholarship for SPN for cleaning and initial data analyses for this project. NK is the Joyce Cook Chair in Ageing Well, supported by the Joyce Cook Family Foundation, N.Z.
Clinical Trial Registration
Clinical Trial Registry number for overarching (original) study: ACTRN12618001827224.
Ethical Statement
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.