
Abstract
In this research we identified the training needs of paramedics in Australia regarding elder abuse identification and response. Ten qualitative interviews with paramedics and paramedic educators from each state and territory were conducted between January and March 2024. Participants encountered elder abuse in their professional capacity, often manifesting as neglect although responses were variable, influenced by the jurisdiction, whether the paramedic had specialist training, how much “scene time” was permitted, workload pressures, and if there were clear protocols and guidelines from the ambulance service on how to respond to elder abuse. The existing training was perceived as “patchy” and ad hoc, but participants offered recommendations for training content and preferred training delivery method in detecting and responding to elder abuse. Given population aging and increased use of ambulance services by older people, paramedics have a crucial role to play in elder abuse early detection and referral. This research presents a critical first step in addressing this gap.
Keywords
• This research adds to the sparse literature on paramedic responses to elder abuse. • Paramedics encounter elder abuse in their professional roles but their responses depend on the state they work in, whether they are trained in elder abuse or working with older people, how much “scene time” their ambulance service permits, workload pressures, and whether there are pre-existing protocols and guidelines on how to respond to elder abuse.
• Paramedics want training on signs and types of elder abuse, screening for abuse, and processes for reporting, referral, and supportive resources like hotlines. • They also want guidance on safely communicating concerns, handling situations where the older person refuses help, and addressing cases where the older person cannot communicate. • Participants preferred the training be online, self-paced, with interpersonal segments facilitated by subject-matter experts such as geriatricians.What this paper adds to existing literature
Applications of study findings to gerontological practice, policy and/or research
Elder abuse intensified in severity and occurrence amid the COVID-19 pandemic, yet numerous frontline health and emergency services lacked sufficient preparation to address this issue (Benbow et al., 2022; Elman et al., 2020). As other non-essential services were scaled back, a void emerged in promptly recognizing and addressing abuse, with emergency services frequently being the sole in-person presence for community-dwelling older adults (Elman et al., 2020, 2023; Liu & Delagrammatikas, 2021). However, studies have indicated that not all these professionals possessed the necessary training to detect elder abuse indicators and provide suitable referrals (Brijnath et al., 2024).
Paramedics were singled out as a workforce that needed additional support in identifying and responding to elder abuse (Brijnath et al., 2024). This is because paramedics are trusted frontline providers and more likely to be allowed into an older person’s home than the police. However, research has long indicated that paramedics lack training in elder abuse and are often unsure about how to respond to abuse (e.g., Jones et al., 1995; Namboodri et al., 1997; Rinker, 2009). In 1995, Jones et al. surveyed >500 paramedics and showed that while 68% saw a case of elder abuse in the previous 12 months, only 27% of these cases were reported. Nearly 15 years later, similar findings were made by Rinker (2009) whose survey of 272 paramedics found they did encounter cases of elder abuse in their work but 95% believed it was a social and not a medical problem. Qualitative studies involving paramedics and Emergency Medical Technicians (EMTs) in New York (Rosen et al., 2017) and Texas (Reingle Gonzalez et al., 2016) reported a range of barriers to elder abuse identification and response, including lack of paramedic protocols or training addressing elder abuse; inefficient systems for communicating concerns with hospital staff; time limitations; and lack of follow-up when concerns are reported. Consistently, for almost 30 years, research has highlighted the need for paramedics to be trained in identifying elder abuse (Jones et al., 1995; Namboodri et al., 1997; Rinker, 2009; Reingle Gonzalez et al., 2016; Rosen et al., 2017).
Training paramedics, including non-emergency patient transport staff, to recognize and respond to elder abuse is important because it creates a “window of opportunity” for early intervention to stop elder abuse, detect risk and adversity, facilitate referral to tertiary care, and even undertake rescue of highly vulnerable older people (as a post-facto intervention). Hence, to improve paramedics’ response to elder abuse, we undertook qualitative semi-structured interviews with them to identify their training needs in how to recognize and respond to elder abuse.
Methods
Context
The research was carried out in Australia, where the prevalence of elder abuse within the community stands at an estimated 14.8% (Qu et al., 2021). While there exists a National Plan to address elder abuse (Council of Attorneys-General, 2019), reporting of elder abuse is not mandatory and discrepancies prevail across jurisdictions concerning guardianship law, substitute decision-making (such as Powers of Attorney), and the functions and authorities of key agencies (Dow et al., 2022). The policy landscape is fragmented and the issue relatively under resourced (Chesterman, 2020; Dow et al., 2022). Consequently, responses to elder abuse vary among states, disproportionately affecting older individuals residing in rural areas, residential care facilities, those from diverse ethnic backgrounds, Indigenous communities, and/or individuals living with dementia (Mackell et al., 2023).
Reflecting these discrepancies at a practice level, paramedics have the practice possibility of early detection (primary prevention), responding immediately after abuse (secondary prevention), and post-abuse and rehabilitation (e.g., during non-emergency transport from hospital) (tertiary care) (Naidoo, 2017). Paramedics are prepared to respond to complex cases and are aware of the intersectionality inherent in such complexity. Their patient and practitioner safety strategy is to determine risk (R) to the client and themselves, recognize immediate or continuing unmet need (N) for safety, health care or referral, and to respond (R) appropriately in the client’s health and safety interest. This “Risk-Need-Responsivity” (RNR) model provides a pragmatic frame for paramedic practice of violence prevention across the lifespan (Naidoo, 2017). In the interest of autonomy and protection, paramedics may assess one’s capacity, competency, or coercive contexts that threaten autonomy and undermine help-seeking behavior.
Sampling and Recruitment
A qualitative descriptive approach (Doyle et al., 2020) was used to undertake one-to-one semi-structured interviews. Selection criteria were two years minimum frontline experience as a paramedic in Australia. Since each state in Australia has a jurisdictional ambulance service, thereby creating uniformity within each state, we used a purposive sampling framework and aimed to recruit at least one knowledge broker from each state and territory jurisdiction (n = 8) with additional participants sought from paramedic education and non-emergency patient transport services.
Recruitment occurred iteratively as follows: First, invitations to participate in the study were extended by NN and SS to the Australasian Council of Paramedicine Deans, and Australasian College of Paramedicine Working Group on Violence, Abuse and Neglect, respectively. Second, NN and SS also reached out to paramedics within their professional networks who might be suitable. Third, snowballing from primary participants occurred via an e-introduction to other prospective participants.
Procedure
Ethical approval was granted for this project by the University of Western Australia (Reference Number: 2023/ET000778). After giving written informed consent, semi-structured interviews were conducted using videoconferencing from January to March 2024 by a male researcher, Peter Feldman (MAsEv), with extensive experience in qualitative research in the health and community services sectors. Participants were asked about their encounters of and response to elder abuse situations, existing protocols, training around elder abuse, how paramedic responses to elder abuse could be improved, and preferred content and formats for further training (see Supplemental File 1). Interviewees were not provided with a copy of the discussion guide prior to interview. Interviews were up to 30 minutes duration, conducted in English, and audio recorded.
Analysis and Data Verification
Interview recordings were transcribed and analyzed using Braun and Clarke’s (2006) inductive and deductive thematic approach. Transcripts were not returned to participants for comment or correction. All transcripts were coded by PF using NVivo 14, guided by a coding schema independently reviewed by RM (see Supplemental File 2). Thematic analysis closely followed the topics addressed in the interview schedule, while allowing for new themes to arise from the data. One minor theme emerged that was unanticipated, relating to cross-cultural understandings of elder abuse within the Australian community. All major themes are explored below. As participants would be easily identifiable, we report minimum sociodemographic characteristics, excluding geographic details, to maintain confidentiality.
Results
There were 10 participants: Two each from Queensland and Victoria, and one from each of the remaining states and territories (New South Wales, South Australia, Western Australia, Tasmania, the Northern Territory, and the Australian Capital Territory). Participant’s mean age was 39.2, and six participants self-identified as men and four as women. At the time of interviewing, one participant was working in a rural and remote area. Participants’ years of experience working as paramedics (excluding years as paramedic educators) ranged from 2 to 26 years, with a median of 12.5 years. This is within the range of the median tenure for paramedics in Australia, which is 10–19 years (Thyer et al., 2024).
Participants spoke from their experiences as paramedics (5 participants) and paramedic educators (2 participants). Paramedic educators may be employed by ambulance services or ambulance service colleges (rather than paramedicine educators, employed by universities) and are tasked with on-the-job training of junior paramedics. Three participants were working as both paramedics and paramedic educators. Two paramedics in the sample identified as Extended Care Paramedics (ECPs), which are paramedics with advanced training who work with other health care providers to manage and treat people in their residences, including in aged care facilities (SA Ambulance Service, 2022).
Participants reported that paramedics encountered elder abuse, often neglect, in their work. Paramedics responses varied based on jurisdiction, paramedic type (general or ECP), scene time limits, workload pressures, and whether there were clear ambulance service protocols. Training was seen as inconsistent and ad hoc. Participants made several recommendations for change including providing adequate training in elder abuse identification and response; clear, detailed, and accessible guidelines for responding to elder abuse; and resources and tools for complex or unclear cases. The findings and recommendations are described below.
Encountering Elder Abuse on the Job
All participants recalled encountering suspected or actual elder abuse while working as a paramedic. Cases encountered mostly involved neglect where carers, often family members, intentionally withheld medication, and direct personal care: They had [paid] carers come in once a day for five days of the week and [the son] said it was a carer’s responsibility to toilet his mum but he wouldn't do it overnight and on the weekends, so she would go from Friday to Monday and either have to get there herself, which was almost physically impossible, or just soil herself, and he wouldn't change her pad or anything like that. He had left it up to her to manage her own medication, which was really unsafe because she really couldn't and [he] just was really not caring for her. (Participant 1 - Paramedic and Educator, female, aged 25–34).
Paramedics also spoke of encountering older people who were soiled for long periods of time in residential aged care facilities because of staff failures to assist with toileting or to regularly check on residents. In more extreme cases, paramedics encountered residents who had been left unassisted for many days, resulting in injuries: I have been to places where you would expect that they would have regular visits from staff, and patients have been found three or four days later, either on the floor, they’ve been there all weekend, in a shocking state. And there was no one who was able to go and see them. And this was in an elderly facility where they can live alone and by themselves [in independent living units]. (Participant 6 – Paramedic, male, aged 35–44).
While most cases of elder abuse encountered were deliberate, participants also said that abuse could unintentionally arise in cases where the older person was experiencing complex health conditions that required extensive support and the family carer was overwhelmed by this responsibility. In such cases, carer stress was a significant factor contributing to the neglect of older people, particularly where older people had complex needs or cognitive challenges such as dementia.
Current Responses to Elder Abuse
The primary response pathway for paramedics was to gather information and convey their concerns to hospital staff on delivery of the patient, whereupon further investigations and referrals were made. One interviewee, from Victoria, described a particularly streamlined notification process through a program on their laptop, which allowed them to request a referral for the patient to a special team within the ambulance service that responds to family violence. Paramedics also referred to police when appropriate: If it's safe to do so, the paramedics would be expected to ask the patient outright “Are you safe?”, “Do you have concerns for your welfare?” and ask some pointed questions. And if the responses are “Yes”, that there are concerns or “Yes” they feel as though they are being abused, or if there's clearly identified signs [of abuse] I guess the first thing they would do is convey that patient to hospital and identify that to the hospital staff and raise it to the notice of policing, and that would be just through our duty officer. (Participant 3 – Paramedic and Educator, male, aged 45–54).
An ECP, whose role required additional training in geriatric care, describes taking further direct action to address abuse in residential care settings. For example, transporting the victim out of the facility in response to signs of abuse; advising the facility management that conditions in the facility are unacceptable and constitute abuse; and reporting facilities to authorities if they do not comply to acceptable standards.
Time Pressures as a Barrier to an Effective Elder Abuse Response
Interviewees described that some, but not all, paramedics are expected to meet certain time-bound key performance indicators (KPIs) when responding to a call-out—that is, staying at scenarios for a designated maximum length of time. Some viewed such restrictions on their “scene time” as a barrier to addressing elder abuse. However, most emphasized that the ambulance services they worked for supported them taking extra time if they explained that they were assessing for or responding to abuse. Interviewees noted a cultural shift over the years that precipitated this greater level of support: Quality healthcare cannot occur if you're stringently linked to a scene time KPI. You need to individualize your scene time depending on what you find and refer to different pathways accordingly… I believe there's less criticism if you're spending quite a long time on [addressing elder abuse], now we're in the space where if that was right for the patient, then that was right for the [paramedic]. (Participant 8 – Educator, female, aged 25–34).
However, one participant flagged that despite having clear protocols for elder abuse, high caseloads and associated burnout contributed to paramedics struggling to identify abuse and respond to it. Two other participants also described facing pressure to spend as little time on scene as possible, due to limited resources: There is a massive focus on clearing jobs, so we're all under pressure. We don't have enough paramedics. We're always busy, but I think at the grassroots level there is support for this type of thing [responding to elder abuse]. What we don't get is, we don't get anything beyond the patient contact time, so it's not like I can get back to the station and then follow up on that report going through. Any type of reporting that would have to happen would be on my own time. (Participant 7 – Paramedic, male, aged 35–44).
By contrast, ECPs can spend more time with patients than other types of paramedics, and may therefore be better able to identify and respond to elder abuse: In my role as an extended care paramedic, [rather] than just an operational paramedic, due to the length of time that you spend with the patient, on average it tends to be anywhere from one to two hours. So, you're there for much longer, so I tended to find that I've picked up on things [signs of elder abuse] much more… I'm able to really assess the scope of perhaps the physical neglect. (Participant 4 – Paramedic, female, aged 25–34).
Training in Elder Abuse for Paramedics: Variable and Mostly Inadequate
Paramedics said that they received basic training on family violence, including elder abuse, during their formal education, and then once employed in the workforce, they could receive ad hoc in-house training from their state-based ambulance service. One participant reported receiving no training at all in elder abuse, while others reported taking part in family violence training that addressed elder abuse to a limited extent: We even ran a couple of scenarios, but the scenarios did focus more on children and women, but in terms of the training packages they would still mention that always keep in mind out for, you know, elder abuse, but…it wouldn't give us more insight I suppose into, like, what's elder-specific about it, as opposed to, let's say, women being abused. They [older people] can be financially [abused], yeah, all the same, but they didn't focus on specifically elder abuse. (Participant 2 – Paramedic, female, aged 25–34).
By contrast, ECPs were better equipped to identify and respond to elder abuse. Alongside being allocated greater time to spend with each case, ECPs received more thorough training and more exposure to hospital-based interventions: We've had subject matter experts and geriatricians present in our sort of extended care training on geriatrics and caring for them, and obviously elder abuse is one of the key things that are reviewed as well… [and] we work a lot in hospitals, so we tend to see the processes unfold there and how comprehensively some geriatricians or doctors will look at even small things [possible indicators of elder abuse]… a lot of our treatment pathways within extended care are specific to that clinical role focus on non-accidental injuries and the need to assess them… I would definitely say that extended care paramedics would recognize elder abuse probably more frequently than paramedics (Participant 4 – Paramedic, female, aged 25–34).
Three paramedic educators spoken to were not confident that education on elder abuse was being provided adequately or consistently enough by universities to be reasonably excluded from training programs within agencies. Lack of elder abuse training for paramedics was thought to be especially problematic for newer recruits, who are not able to lean on years of experience to assist in identifying or responding to elder abuse: We would definitely benefit from more training… A junior crew might be not sure what to do… if someone is in imminent danger, which we’re really good at doing [responding to], we will get the police straight away, no problems. I think it's the grey area, where it's not clear cut… we've got a very junior workforce, and a lot of these paramedics, you know, don't have much experience at the moment - couple of years at the most. (Participant 10 – Paramedic, male, aged 35–44).
One paramedicine educator was equivocal whether elder abuse training should be mandatory for current paramedics: I'm a bit wary of the word “mandatory.” There are so many arguments for and against it… every paramedic will view their role and responsibility differently, and I think the paramedics that we need to speak to are the ones that perhaps feel that some of these responsibilities [to detect and respond to elder abuse] fall outside of their role. (Participant 9 - Educator, male, aged 45–54).
Four participants expressed support for mandatory training for paramedics, pointing out that population aging will likely see increased rates of elder abuse, and that paramedics are well positioned to respond to elder abuse in community and institutional care settings. It was also argued that mandatory training, if conducted regularly, would be the most effective way to ensure that professional knowledge about elder abuse and appropriate responses are current.
Jurisdictional Differences on Guidelines for an Elder Abuse Response
Multiple interviewees said there was little, if any, official guidance around responding to elder abuse. Rather, what response (if any) that was offered was reliant on the discretion and knowledge of the paramedic responding to the scene: Our paramedics and, for that matter, our patient transport officers are likely to identify that there is a concern [with respect to elder abuse], but there's no set policy on what to do about it… they might report inwards or outwards, depending on their level of confidence to seek advice through management, be that frontline or operational management, or if they're more confident they may report directly to policing, but we don't have a set policy for what to do should one be concerned. (Participant 3 – Paramedic and Educator, male, aged 45–54).
As with training courses, there may be guidelines that touch on elder abuse, but refer to it in passing and do not address it in adequate detail. For example, guidelines concerning the treatment of older people in general or guidelines on responding to family violence: There's one [clinical practice guideline] around the older person, and I think that's relatively new. It talks about, like, how to assess them clinically, but there's no real mention of clinical, like, elder abuse concerns. It's more talking about, like, the fact that they've got different physiological needs. And then there's another one talking about understanding and responding to domestic and family violence but doesn't have a strong elder person focus. (Participant 1 – Paramedic and Educator, female, aged 25–34).
By contrast, some interviewees described clear processes in place for paramedics to report suspected elder abuse. However, there was a sense in which, even in jurisdictions where there are clear protocols for elder abuse, not all paramedics are sufficiently informed about them: We do have almost like a reference or protocol around elder abuse. So, it just highlights, you know, what it might look like and, like, a general approach to it. And there is… a [phone] number, as well as on top of that, we do have a reporting system… I think that some paramedics may not necessarily be as aware of the extent of it. (Participant 4 – Paramedic, female, aged 25–34).
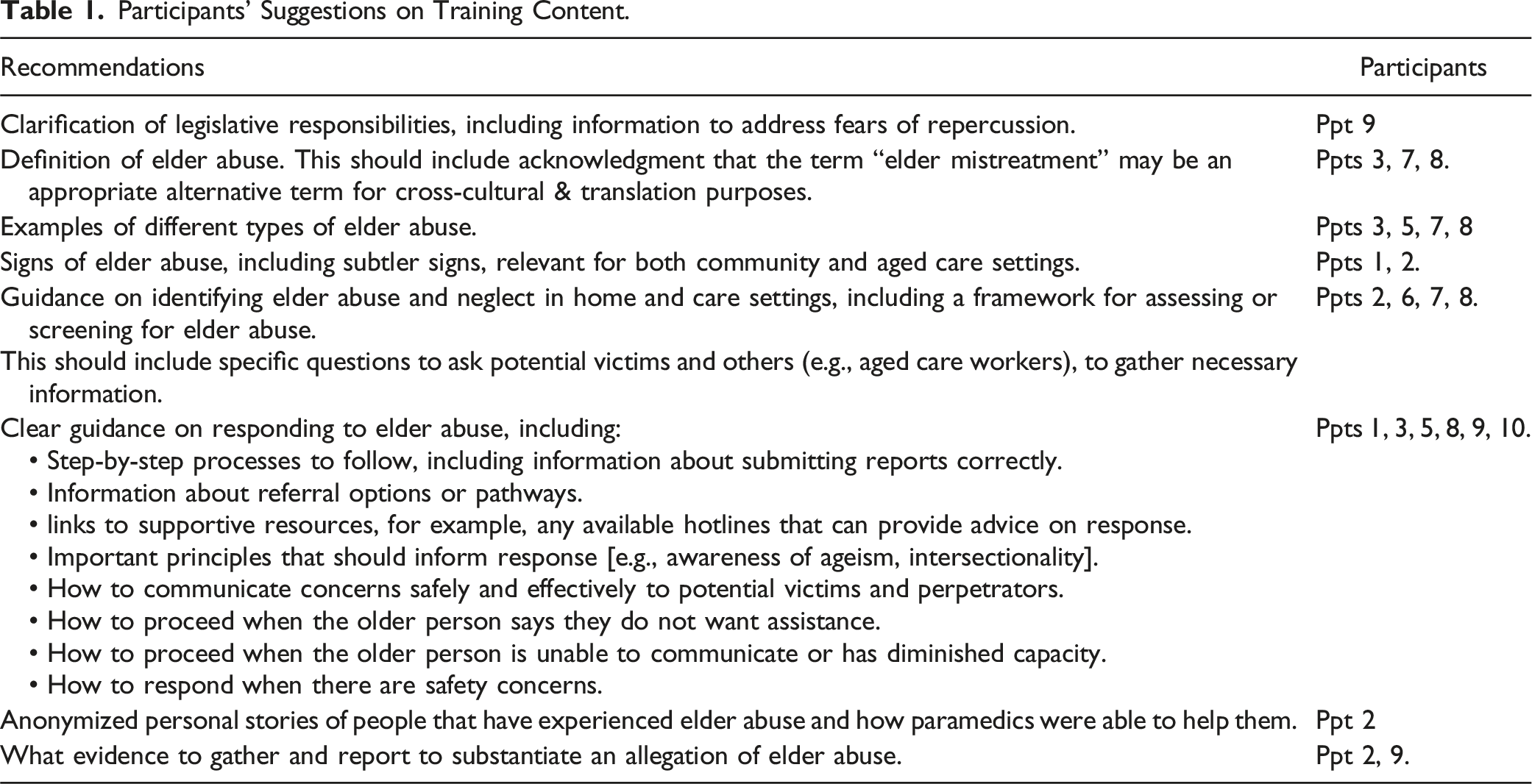
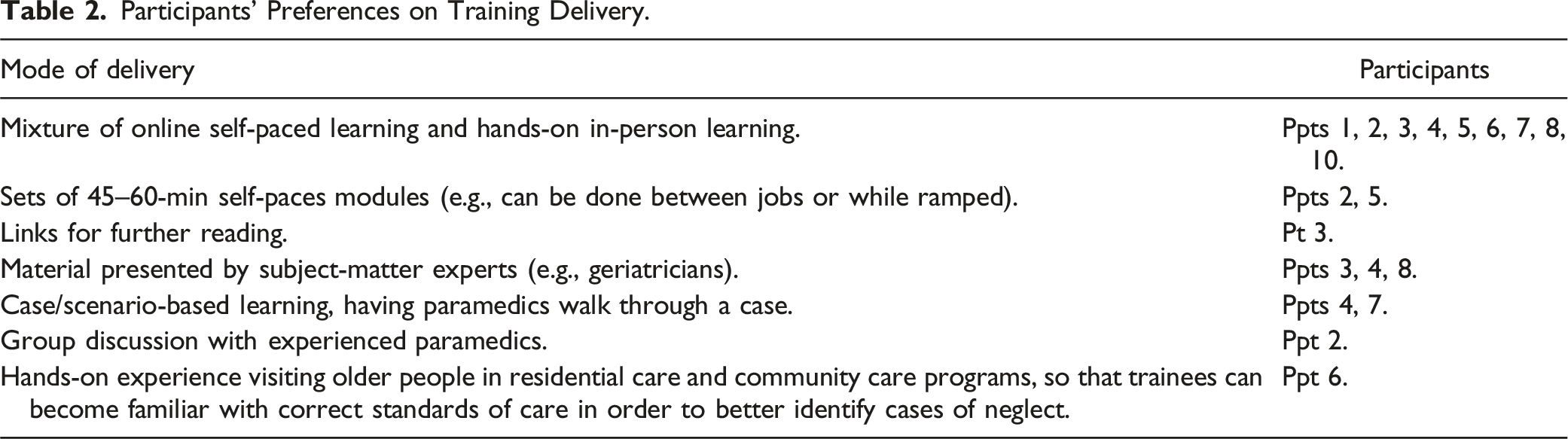
Participants’ Recommendations for Change
Participants’ Suggestions on Training Content.
Participants’ Preferences on Training Delivery.
Alongside training, interviewees supported the dissemination of detailed guidelines to inform paramedic responses to elder abuse, as well as other helpful tools and resources that account for nuanced and complex situations. Calls for strengthening guidelines to improve agency responses to elder abuse came particularly from jurisdictions where such guidelines were lacking. One participant suggested that the development of a phone line to provide specialist advice to paramedics would be helpful to advise paramedics uncertain about any matter, especially if they were concerned with the legal implications of alleging abuse: It would be good to ring up and talk to a specialist service and go, “Hey, we're currently in a situation, Mr. Smith is a 90-year-old male, there seems, it appears, some alleged abuse.” Because we also can't say “He's been abused” - we haven't witnessed it, we've only been told what we've been told, so we have to be very careful what we say and we have to be very careful what we document, because it's all alleged. (Participant 10 – Paramedic, male, aged 35–44).
Other helpful tools, particularly an app, were also suggested to allow paramedics to refresh their knowledge and understanding of elder abuse identification and response at any time: I would love for it [guidelines] to be like… “Here are your options for referral services: If this is going to be a transport make sure you get A, B, D and C with you as well,” and things like that… I'm not my best at night shift, so if I can just pull up my app and be like “Oh that's right, I need to do this”, that would be good. (Participant 2 – Paramedic, female, aged 25–34).
Finally, participants recommended paramedics be provided feedback on the outcomes of their reporting, with some expressing concern that they were not made aware of the outcomes of their reports of elder abuse to hospitals and were unsure if these reports were acted on at all. To improve feedback, participants suggested that reporting systems used by ambulance services should be regulated by the state governments to set clear expectations of healthcare services and improve accountability: We should have a reporting system that would tailor to reporting elder abuse and then having an outcome. But that probably needs to come from the State, from the State’s point of view, so from the Health Department itself… to say “Right, the expectation is - you identify elder abuse, you should be reporting it through Department of Communities”, and Department of Communities will generate reports that will then say, “Right, this is what the outcome was.” I sort of feel if there was going to be a process it needs to be tracked and there needs to be something that I can identify as “Alright it's in this process now with Department of Communities”. (Participant 7 – Paramedic, male, aged 35–44).
Discussion
In this study, we identified not only the desired training needs of paramedics regarding elder abuse identification and response but also their preferred learning methods. This is a novel finding insofar as such research has never been conducted previously in Australia and while overseas, mainly US-based, studies have consistently highlighted the need for training (Jones et al., 1995; Namboodri et al., 1997; Rinker, 2009; Reingle Gonzalez et al., 2016; Rosen et al., 2017), none have elaborated in such detail on the desired content and training delivery mechanisms.
Older people are frequent users of ambulance services given the association between ambulance transportation rates and increasing age (Lowthian et al., 2011). As such, paramedics are well placed to detect and make referrals for elder abuse because they can attend to injuries in community and care settings whilst also observing the living situations of older patients and their interactions with family and carers (Lowthian et al., 2011; Namboodri et al., 1997; Rosen et al., 2017). Given that many older people who are attended to by paramedics do not go on to be transported to hospitals, upskilling paramedics to identify signs of elder abuse and make appropriate referrals reduces the likelihood that older people experiencing abuse will be denied support and early intervention (Mosqueda & Khalili, 2024; Tiedemann et al., 2013). For these reasons, peak bodies such as the Australasian Council of Paramedicine Deans (2020) and Australasian College for Emergency Medicine (2020) support the implementation of training for paramedics on family and domestic violence, acknowledging elder abuse as a subtype of this wider problem.
Simultaneously, as suggested by participants of this research, extending training and guidelines on domestic and family violence—usually operationalized to address intimate partner violence—may not be adequate in improving elder abuse identification and response by paramedics. There are several reasons for this, such as differences in perpetrator profiles: While perpetrators of domestic and family violence are most commonly male intimate partners, perpetrators of elder abuse are often also adult children or other family members, and caregivers and other non-family individuals (Kilbane & Spira, 2010). Older victims may also have unique needs, particularly those living with dementia or other forms of cognitive impairment (Kilbane & Spira, 2010; Warren & Blundell, 2018). Older victims also face distinct barriers to disclosing abuse, for example, not wanting adult children who are perpetrators to face negative consequences (Dow et al., 2020). Therefore, to address elder abuse adequately, paramedic training and clinical practice guidelines should be specific to elder abuse. Such training and guidelines should also be nationally consistent, so that paramedics are clear on how to respond and so that older people who are victims of elder abuse are not geographically disadvantaged (Mackell et al., 2023).
Such training and guidelines should also include a consistent screening tool or method for identifying elder abuse; a need also identified in Gonzalez et al.’s work (2016). An elder abuse screening tool was developed in the USA for use by paramedics: The DETECT tool (Cannell et al., 2020), and a range of other elder abuse screening tools have been developed for use in community settings but have not been specifically tested with or indicated for use by paramedics. For example, the Elder Abuse Suspicion Index (EASI) from Canada (Yaffe et al., 2008); the Hwalek-Sengstock Elder Abuse Screening Test (HS-EAST) from the United States (Neale et al., 1991); the Vulnerability to Abuse Screening Scale (VASS) from Australia (Schofield & Mishra, 2003); and the Australian Elder Abuse Screening Instrument (AuSI) (Brijnath et al., 2022; Gahan et al., 2019). Further research is needed to test the validity of such tools for use by paramedics in the Australian context. All relate in varying extents of risk assessment, need appraisal and response potential to Naidoo’s (2017) RNR paramedic practice model.
There are multiple systemic barriers facing paramedics. This is a workforce under immense pressure due to increasing resource constraints and rising demand due to population ageing and increased community health awareness (Lowthian et al., 2011). In Australia and overseas, there are chronic workforce shortages, restrictions on “scene times,” and significant paramedic burnout and fatigue. These are systemic issues that go beyond elder abuse and require greater attention and investment by governments. Nevertheless, these barriers limit paramedic’s time and ability to detect and respond to elder abuse (Rosen et al., 2017). That all the paramedics we spoke to had encountered elder abuse is a testament to its relatively high prevalence in the Australian community (Qu et al., 2021); a finding also made in US studies (Jones et al., 1995; Rinker, 2009). While unsurprising, the frequency with which our participants mentioned attending to cases of neglect is higher compared to other services such as police and legal services (Brijnath et al., 2024). This suggests that paramedics may be one of the few services to respond to cases of neglect, which is often underreported to other agencies (Brijnath et al., 2021; Payne-James et al., 2023; Rinker, 2009).
Limitations
This research is limited by a small sample of ten frontline participants and paramedic educators. While they represent a national sample, if training were to be developed and implemented, a more representative sample of key stakeholders such as ambulance services, training providers, aged care providers, government, and peak paramedical associations should be consulted. Most importantly, older people should be involved in co-designing the training, and the voices of older people who have experienced abuse, should be privileged. Communications experts were not among those sampled. The role of the emergency communications center in crisis intervention and follow-up screening for recurring exposure to abuse or neglect is not addressed in this study.
Conclusion
Elder abuse is common in Australia and has devastating impacts on older people’s morbidity, if they survive. Paramedics have a crucial role to play in early detection and referral, especially because they are a trusted frontline responder that have a unique opportunity to observe conditions in the older person’s living environment. This is very important especially in cases where there is cognitive impairment and/or neglect. However, paramedics receive insufficient, if any, training on elder abuse and thus there may be missed opportunities for intervention. This study presents a first step in addressing this gap by identifying the training needs and preferred pedagogical approach paramedics desire to build capacity for greater responsiveness to older adults living with abuse or (more commonly) neglect. Paramedics may well be ‘sentinels’ for health security in such cases.
Supplemental Material
Supplemental Material - Strengthening the Frontline Response to Elder Abuse: Qualitative Insights From Australian Paramedics
Supplemental Material for Strengthening the Frontline Response to Elder Abuse: Qualitative Insights From Australian Paramedics by Navin Naidoo, Peter Feldman, Rachel Muoio, Simon Sawyer, and Bianca Brijnath in Journal of Applied Gerontology
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NN is an executive member of the Australian Council of Paramedicine Deans (ACPD) and immediate past Deputy Chair.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and publication of this article: The study data collection is funded, in part, by a Research Development Grant from the School of Health Sciences, Western Sydney University. The grant holder is NN and NARI is the service provider, by formal agreement.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.