
Abstract
Our study employed a six-step meta-synthesis approach to understand quality aspects of virtual healthcare trajectories and identify effective strategies for older adults with preventable chronic conditions across the world. Review of twenty-one articles revealed four key themes: functionality of virtual healthcare, equity in service delivery, satisfaction with care, and cost-effectiveness. Despite the challenges posed by technological and clinical complexities, virtual healthcare initiatives have significantly improved accessibility and availability of health services, thereby reducing disparities. Notably, telehealth saved an average of 166-minutes of travel time, demonstrating a clear benefit of virtual healthcare. While all parties expressed satisfaction with virtual healthcare, several challenges were reported, including a digital divide, limited access to digital devices, absence of a multidisciplinary approach, and lack of rural-specific programs.
Keywords
• Our review extends understanding of the quality issues of virtual healthcare for older adults with preventable chronic conditions. • Benefits are evident, but technological and clinical complexities reduce the effectiveness of virtual healthcare. • Barriers include digital divide, limited access to digital devices, absence of a multidisciplinary approach, and lack of rural-specific programs.
• Our review suggests reducing technological complexities and improves digital literacy for successful implementation of virtual healthcare. • Our review highlights that it is important to identify the needs of older adults with preventable chronic conditions at different stages of their healthcare trajectories and to partner with these patients and their families to enhance effectiveness of virtual healthcare.What this paper adds
Applications of study findings
Introduction
Chronic disease is the primary reason for morbidity, mortality, utilization of health services, and the overall cost burden on healthcare systems across the world (Breadon et al., 2023; Islam and GBD 2019 Australia Collaborators, 2023; Wang, Liu et al., 2021). Lasting for at least 6 months, chronic conditions—such as cancer, heart disease, stroke, chronic lung disease, and diabetes—account for 74% of global deaths (Wang, Liu et al., 2021). Despite the complexity of causes and nature of such diseases, certain chronic conditions, like musculoskeletal conditions, cardiovascular diseases, diabetes, mental health, and neurological disorders, can be prevented (referred to as preventable chronic conditions throughout this article) through improved access to screening, treatment, and rehabilitation (Greenberg & Pi-Sunyer, 2019; Mas et al., 2018). Clinicians and the broader health system can provide healthcare services virtually to patients, nationally and internationally (Ferguson et al., 2021; Hutchings et al., 2021). Older adults with preventable chronic conditions (OAPCC) are a growing segment of this demographic (Greenberg & Pi-Sunyer, 2019; Mas et al., 2018). However, quality aspects of virtual healthcare (VHC) delivery for preventable chronic diseases have not yet been meaningfully investigated.
Virtual healthcare (VHC) describes remote interactions between patients and their healthcare providers, facilitated through various communication and information technologies to enhance patient care (Ferry et al., 2021; Liddy et al., 2022; Singer et al., 2022). According to the WHO (2021), VHC involves securely utilizing information and communication technologies to support health-related activities, encompassing service delivery, surveillance, education, and research. The multifaceted approach to VHC contains several components, such as live synchronous audio-video telemedicine, asynchronous store-and-forward care, electronic consultations, telephone visits, portal messaging, remote patient monitoring, pre-visit planning, interactive care plans, advanced care at home, and more, reflecting the rapidly evolving nature of this field (Demaerschalk et al., 2022; WHO, 2022). Additionally, VHC can be defined as a real-time video consultation with healthcare providers conducted over the Internet, a trend expected to continue to grow with the increasing use of mobile devices, rise of AI, and rising patient demand for convenient and immediate access to healthcare services (Gordon et al., 2017; Li et al., 2022).
While available international evidence presents a mixed outcome, many studies reported that VHC for chronic diseases can be as effective as, if not more effective than, traditional face-to-face care provided in a healthcare setting (Bajgain et al., 2023; Ferry et al., 2021). Clinical benefits identified in the research include improvements in heart failure symptoms, chronic respiratory symptoms, glycemic control in diabetes, blood pressure in hypertensive patients, quality of life, mental health, and reductions in deaths and hospitalizations (Demaerschalk et al., 2022; Ferguson et al., 2021; Li et al., 2022). Non-clinical benefits of virtual care include improved appointment attendance, increased patient knowledge and self-management, and patients feeling more supported (Gao et al., 2023). Frontline healthcare providers have recognized other non-clinical benefits including improved access to care, particularly for older adults with chronic conditions, who often face challenges related to mobility, transportation, and regular healthcare visits (Goldberg et al., 2022). For example, older adults have reported experiencing improved access to care, greater time efficiency, and enhanced self-management capabilities through telehealth initiatives (Savira et al., 2023). Telemonitoring and device utilization emerge as suitable options for interventions focused on self-management and monitoring, especially for older adults with chronic conditions (Savira et al., 2023). The research findings also underscore the potential benefits of virtual visits for older adults residing at home, enhancing social inclusion and medication compliance (Savira et al., 2023). Both users and clinicians have expressed satisfaction with virtual visits as a suitable means of delivering in-home care to older adults (Bajgain et al., 2023; Li et al., 2022).
OAPCC often require ongoing monitoring, medication management, and regular check-ups, which can be burdensome for older patients, family carers, and health systems (Mas et al., 2018). VHC presents an opportunity to address these challenges by providing a convenient and accessible means of delivering healthcare services and support (Savira et al., 2023). However, the adoption and successful implementation of VHC for OAPCC and their family carers are influenced by a range of factors. These factors—such as knowledge and willingness among patients and family carers, access to digital technologies, internet connection, and support to set up virtual visits—act as barriers that hinder the uptake of VHC or as facilitators that promote its adoption and use (Savira et al., 2023; Wang, Fu et al., 2021; Zaman et al., 2022). Programs based on a VHC delivery model use various approaches and have demonstrated varying levels of success, indicating that further research is necessary to better understand the most effective models for managing chronic diseases (Demaerschalk et al., 2023; Smithson et al., 2021).
Current scoping and systematic reviews have been constrained to identifying enablers and barriers to VHC delivery among older adults with chronic conditions (Savira et al., 2023; Wang, Fu et al., 2021; Zaman et al., 2022). Beyond this point; we aim to synthesize the quality aspects of VHC for OAPCC.
Review Questions
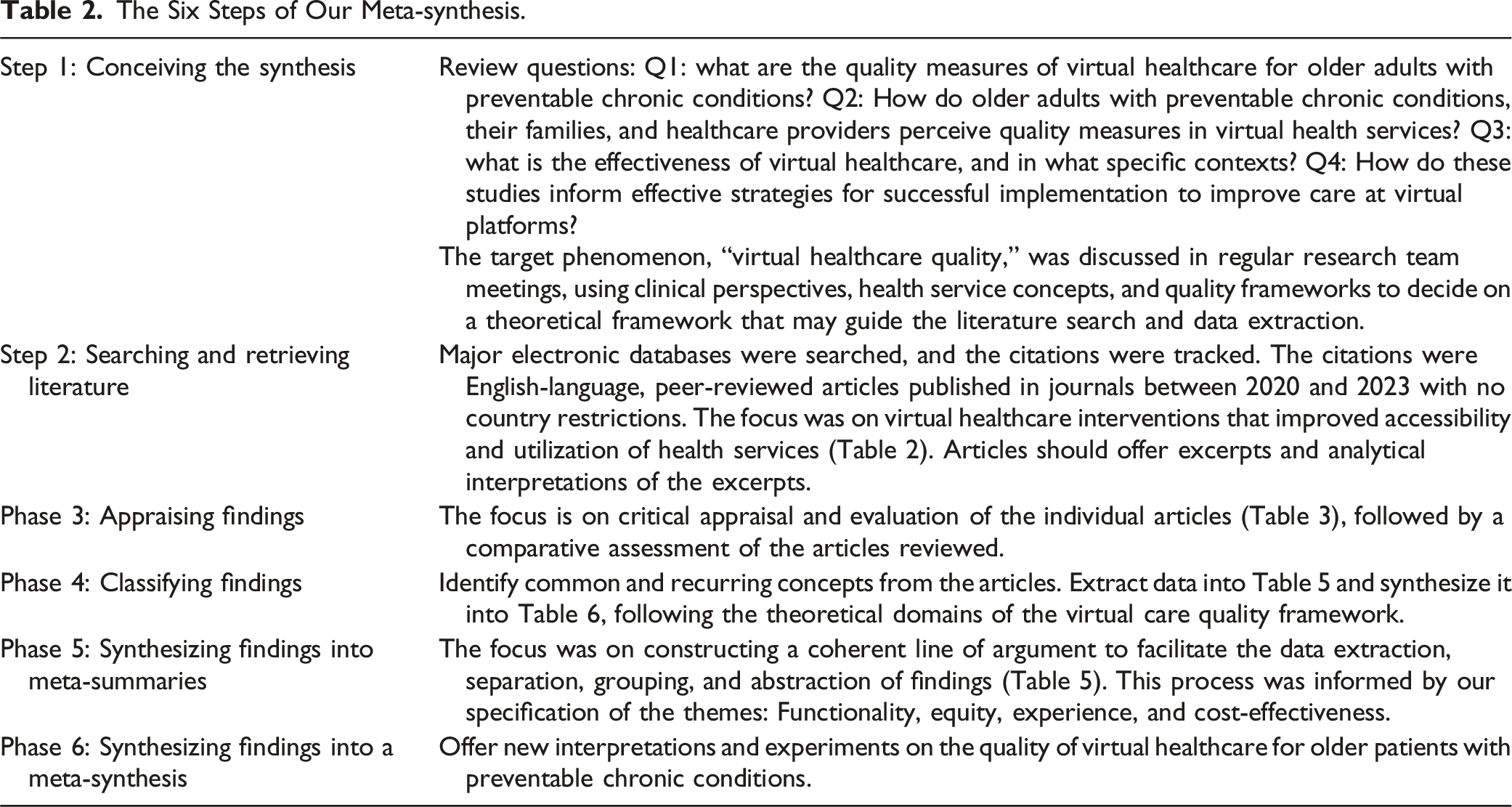
Our meta-synthesis aimed at understanding how quality measures are incorporated in designing and delivering VHC for OAPCC. The PICO framework was employed to formulate the review questions (Schardt et al., 2007).
P (Population) – Older adults with preventable chronic conditions
I (Intervention) – Virtual healthcare
C (Comparison) – not applicable
O (Outcomes) – Implementation: quality in service design and delivery; and Effectiveness: equity and satisfaction with care
Four main questions guided our meta-synthesis: Q1: How do the studies describe the quality measures of VHC for OAPCC? Q2: How do OAPCC, their families, and healthcare providers perceive quality measures in VHC? Q3: How do these studies describe the effectiveness of VHC, and in what specific contexts? Q4: How do these studies inform effective strategies for successful implementation to improve care at virtual platforms?
Theoretical framework
Description of the VCQF.
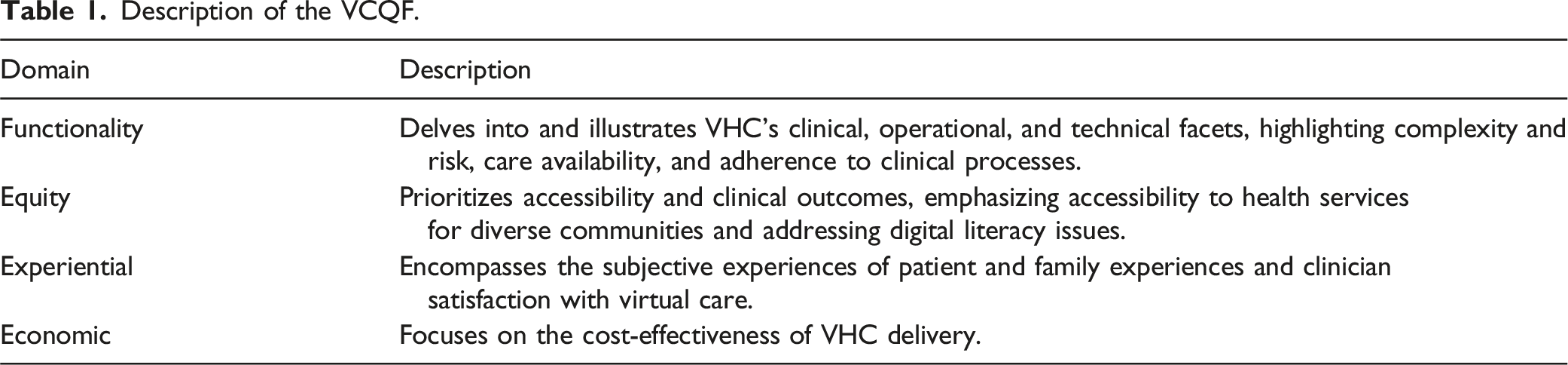
This VCQF draws from established guidelines and advances a comprehensive understanding of the nuanced dynamics that may describe the implementation and effectiveness of VHC for OAPCC.
Methods and Materials
The Six Steps of Our Meta-synthesis.
Search Strategy
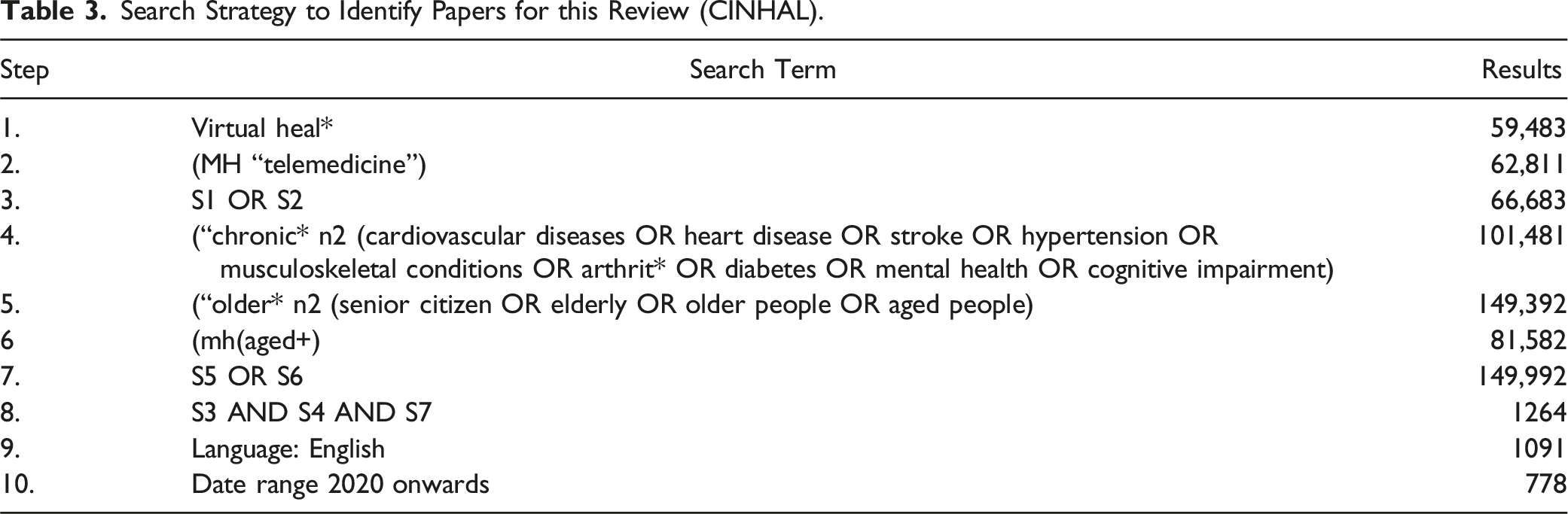
Following the PRISMA guidelines, the articles were identified using a systematic search in MEDLINE EBSCO, PUBMED, PROQUEST, CINHAL, and SCOPUS (See Supplemental File 1: PRISMA Checklist) (Page et al., 2021). A combination of MeSH headings and relevant concepts (or any of their variants) was used in key search areas: virtual healthcare, preventable chronic conditions, and older adults and family carers (the full search strategy in CINHAL is available in Table 3). The CLUSTER model was also employed to track sibling studies and citations for supplementary references (Booth et al., 2013).
- Searches were limited to publications between 2020 and 2023 to ensure study findings were contemporary and reflected best practice guidelines; - Articles published in peer-reviewed journals; - Only articles written in English; - Multiple articles were considered from one empirical study; - Interpretative qualitative research, that is, articles presenting quotes and analytical interpretations of findings; - Papers reporting VHC for OAPCC; - Studies focus on the experiences of OAPCC and/or family carers and/or healthcare providers. Studies were excluded if they did not report on VHC from the perspectives of OAPCC, their family carers, and/or healthcare providers. VHC targeting all chronic conditions and complex care needs was not excluded from this review unless they specifically excluded the targeted preventable chronic conditions. Any discrepancies were discussed and resolved within the review team. Search Strategy to Identify Papers for this Review (CINHAL).Box 1. Inclusion and Exclusion Criteria
Quality Appraisal
Mixed Method Appraisal Tool Scores for the Selected Studies.

Data Extraction and Synthesis
Two reviewers, MH and SJ, read articles and recorded the extracted data separately into Excel spreadsheets, carefully cross-checking any discrepancies (See Supplemental File 2: Table 5 Summary of selected studies). The extracted data included study characteristics (author, year, country of origin, study objectives and design, and study participants) and VHC (type of interventions, experience with virtual care). Deductive-reflexive thematic data synthesis was applied since meta-synthesis is about classification and abstracting findings (Braun & Clarke, 2019, 2020). The second and third stage categories from targeted findings were independently identified by reviewers MH and SJ, and an abstract integration of themes and sub-themes was obtained via critical reflections on the VCQF (Demaerschalk et al., 2023). A matrix to display studies (identified by authors) against the concepts was developed (See Supplemental File 3: Table 6 Synthesis of study findings).
Identification of Effective Strategies and Solutions
Firstly, a comprehensive list of potential effective strategies and solutions was derived from the current evidence. Secondly, the compiled strategies were then further refined by removing overlapping strategies and grouping strategies into broader categories (See Supplemental File 4: Table 7 Recommendations). SP drafted the table and MH reviewed the table.
Results—Theoretical and Analytical Interpretations
Twenty-one articles were reviewed. The majority of the studies were conducted in the United States (n = 12), followed by Australia (n = 3), Canada (n = 2), Europe (n = 3), and Asia (n = 1). The study designs varied, with a mix of qualitative (n = 10), mixed methods (n = 9), and quantitative analyses with qualitative feedback (n = 2). A total of 1005 participants were involved in these studies, with a focus on older adults living with a range of preventable chronic conditions, including cardiovascular diseases, obesity, hypertension, chronic pain, diabetes, cognitive decline, and dementia. The interventions varied from generalized telehealth and eHealth platforms to more specific interventions like mobile health obesity wellness interventions, technology-based weight management programs, and sensor-based in-home exercise systems. Apart from detailing virtual health services’ origins, focuses, and designs, the meta-synthesis of stakeholders’ perceptions of VHC unveiled the following themes (Figure 1). PRISMA 2020 flow diagram of systematic search and selection process.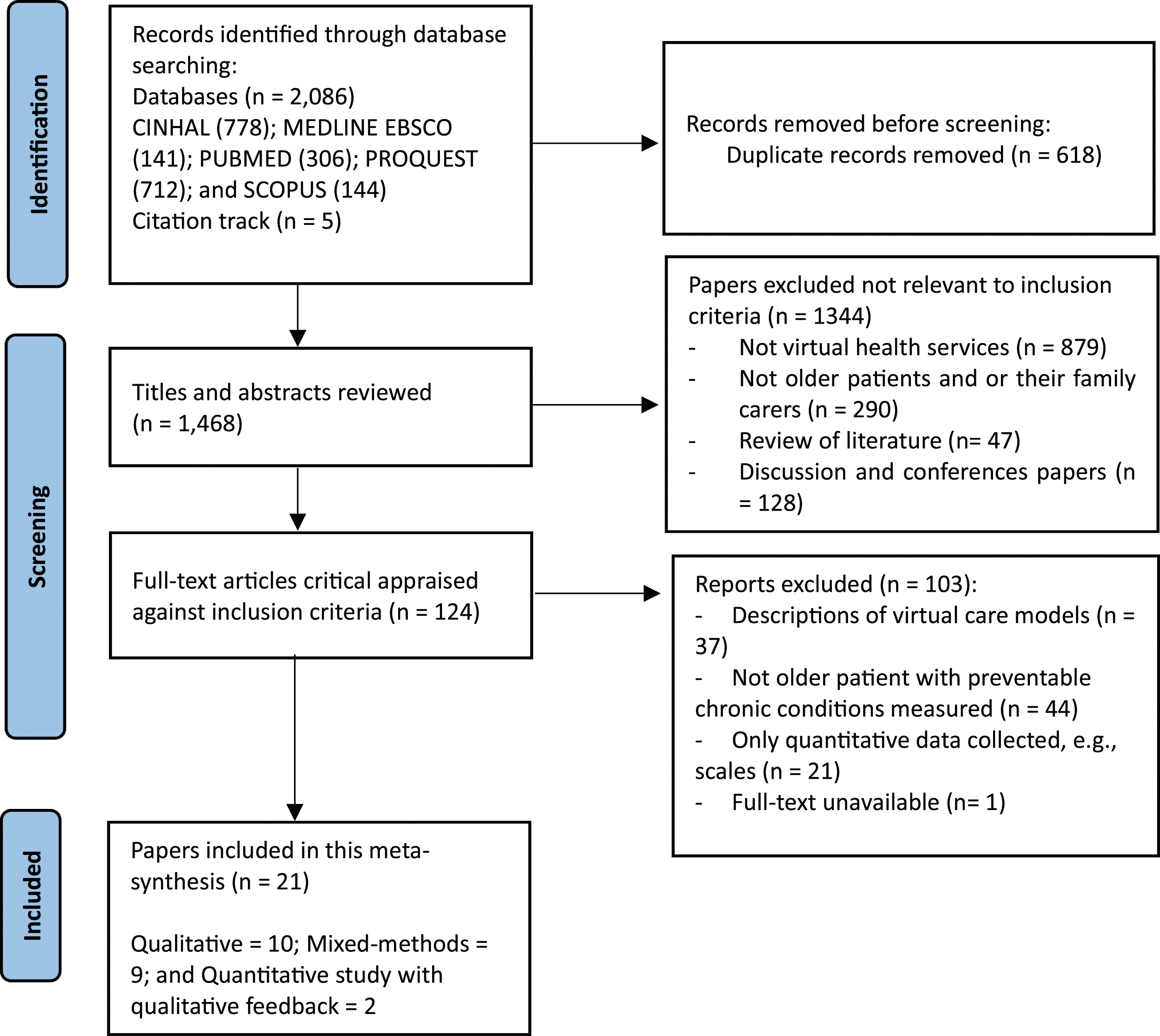
Theme 1: Functionality of Virtual Healthcare
Across the studies reviewed, OAPCC experienced technological and clinical complexities in accessing healthcare virtually, and these complexities were echoed in the voices of healthcare staff who provided them with care virtually. Older adults appreciated telemedicine overall but expressed frustration with various VHC platforms and their usability (Ailabouni et al., 2022; Batsis et al., 2020; O’Shea et al., 2020). Contrasting experiences exemplify this dichotomy; some older adults successfully navigated digital platforms (Iyer et al., 2021), while others feel alienated by technological advancements and limitations (Coorey et al., 2020; Yu et al., 2021). For example: “I’m not into computers... I have neuropathy, and sometimes I miss things on the computer.” Older adult “That is if you can read it [medication information] because the writing is so small.” Older adult
The benefits of live video-conferencing software were documented in several studies, whereas user interface design and network reliability remained complex issues for this cohort (Doorley et al., 2022; Gately et al., 2022; Hawley et al., 2020; Iyer et al., 2021; Lan & Chen, 2022). Innovative solutions, such as the tele-Exergame system and the personalization of VHC, for example, avatars and storytelling and hands-on training reduced technological complexities for OAPCC (Park et al., 2022; Schoenthaler et al., 2020; Watt et al., 2022). However, the need for familial or professional support in technology use emerged as a recurrent theme in avoiding technical complexities (Yadav et al., 2021). “To see my 96-year-old dad working an iPad because he’s had somebody take the time to show him how to use it is amazing.” Family carer “The main issue is that if you don’t have a family member familiar with the technology, you’re going to spend a lot of time.” Healthcare staff
Clinical complexity equally challenged virtual health services delivery, as these older adults struggled with managing extensive medication treatments and expressed the need for comprehensive care that extends beyond physical health to include psychological well-being and social connectedness (Ailabouni et al., 2022; Batsis et al., 2020). Age-related physiological and cognitive declines exacerbated these issues (Haynes et al., 2023), making adopting VHC challenging for them. Associated risk factors included these older adults’ perceptions of real healthcare and their varying needs, including skills for technology access (Batsis et al., 2021; Weems et al., 2021). “Well, the last doctor I saw... was the first time that I had actually seen a doctor taking real care and looking and thinking.” Older adult “I guess I would like somebody [pharmacist] to sit down with me and go through the medication list...” Older adult “Difficulty with technology setup and usage: ‘... one person didn’t show up ... they had technical challenges and wasn’t able to set up...’” Healthcare staff “...it means standing at a window and I can’t stand very well right now because of my leg…” Older adult
The suitability of virtual platforms for certain chronic care interventions was also not confirmed.
All studies reported increased healthcare support for preventable chronic conditions due to virtual platforms. For example, Park et al. (2022) and Lindberg et al. (2021) highlighted the potential for telehealth to increase access to specialist care remotely. However, in some studies, older adults reported being overwhelmed by the administrative system retracted their access (Gately et al., 2022; Weems et al., 2021). Availability of care is a key component of the domain functionality in the Virtual Care Quality Framework. Specifically in the context of rural health, workforce shortages and the absence of rural-specific programs have influenced the availability of VHC in rural locations (Batsis et al., 2021). This is further explored under the domain equity.
In examining the functionality of VHC, nine studies reported on these older adults’ adherence to clinical processes. Adherence to clinical processes emerged across different domains of VHC provision, such as trust in healthcare providers, the use of technology in treatments, and medication management and compliance. Some studies revealed a nuanced landscape where trust was foundational yet challenged by the VHC platforms (Akenine et al., 2020; Schoenthaler et al., 2020). Preference for familiar providers and non-verbal communication were important to establish a meaningful virtual interaction. However, several studies reported a positive patient experience with telehealth interventions, with older patients feeling cared for and noting little difference from in-person visits (Ailabouni et al., 2022; Batsis et al., 2021; Coorey et al., 2020; Iyer et al., 2021). The ease and user-friendliness of technology-enabled more personal connections through platforms like FaceTime and enhanced patients’ comfort and engagement in virtual visits (Doorley et al., 2022; Gately et al., 2022). For example: “I did not think of that. Same thing, I don’t use Skype, but that’s a technological advance that—that’s really helpful and I think the videoconferencing—you can reach more people and we can, in a rural area, be able to participate without making an excuse.” Older adult
Medication management and non-compliance is linked to adherence to clinical processes as part of functionality. Both emerged as concerns in properly functioning VHC. Studies also reported a lack of digital support for medication management, an operational or technical facet of functionality (Ailabouni et al., 2022; Schoenthaler et al., 2020). This was compounded by patient non-compliance due to forgetfulness and concerns over adverse effects, further impacting adherence to clinical processes.
Theme 2: Equity in Service Delivery
Several studies highlighted the equity in virtual service provision, examining telemedicine’s role, barriers to access, and the empowerment of older adults. All participant groups across the studies agreed that virtual platforms address accessibility and availability of health services, thereby reducing disparities in utilizing available resources. Telemedicine provided more time for patient-doctor interaction and helped overcome resource scarcity and workforce shortages, especially in rural areas (Ailabouni et al., 2022; Batsis et al., 2021). These observations were reinforced by the findings of Hawley et al. (2020), where older adults reported substantial reductions in travel burdens during telehealth visits, particularly for those who previously travelled distances for in-person care. For example: “Prefer phone calls, more personal, know who you’re talking to.” Older adult
Factors that created inequality in VHC delivery for preventable chronic conditions include a lack of access to appropriate devices, an absence of a multidisciplinary approach, a lack of rural-specific healthcare programs, and the quality of online information. Whereas Coorey et al. (2020) demonstrated the widespread availability of technology, in the studies by Gately et al. (2022) and Weems et al. (2021), older adults and their families commented on their inaccessibility to the internet and modern devices such as tablets and smartphones. “...if we could provide them (older adults) with a tablet or a laptop... there is that gap of the people that really would like to join, but that they’re not able to.” Family carer
Some older adults described the lack of multidisciplinary virtual care because of the involvement of independent insurance providers (Ailabouni et al., 2022; Batsis et al., 2020). In addition, few others experienced that their virtual visits with healthcare staff were only used to refer them to a specialist (Ailabouni et al., 2022). “A lot of doctors now seem to just slough you off by referring you to somebody else (specialist).” Older adult
While Hawley et al. (2020) found that the majority of their study’s respondents were interested in telehealth visits, Batsis et al. (2020, 2021) reported the suffering of rural older adults in accessing virtual care due to a complex-built health system, lower healthcare access, and a lack of rural-specific virtual care programs that consider social connectedness. Furthermore, older adults shared their struggles with discerning the reliability of health information, indicating a perceived digital division between new and old generations from the older person’s perspective (Akenine et al., 2020; Batsis et al., 2021). “Young people surf and search much more online than the elderly. Older adults have much more difficulty judging what information is good quality and what isn’t.” Older adult “Can’t use the computer, no one to teach me to use it at the moment.” Older adult
Akenine et al. (2020) suggested the need for easily navigable, high-quality information sources, supported by Yu et al. (2021), who emphasized practical and reliable resources.
In fourteen studies, older adults and healthcare staff drew on the patients’ capability building to bridge the gaps in accessing VHC in terms of acceptance of technology and increased health literacy. Batsis et al. (2021) rejected the perception of older adults’ inability to use remote monitoring and video-conferencing technologies, and recently, Haynes et al. (2023) presented a narrative of technology adaptation, showing older adults improved their tech skills over time. “Our approach provided informative feasibility data that could help structure a large-scale intervention. First, we provide that older adults can engage in the use of remote monitoring and video-conferencing, dispelling major misconceptions that this group has difficulty in using technology.” Authors
Despite the self-reported acceptance and adaptation of technology, interviews, and focus groups with stakeholders revealed the importance of continuous patient education on symptom recognition (Akenine et al., 2020), communication skills development (Ailabouni et al., 2022; Batsis et al., 2020), and confidence in telehealth visits (Batsis et al., 2020; Coorey et al., 2020; Hawley et al., 2020). “Well I … No, for me, I mean, it’s embarrassing. My computer skills are so limited.” Healthcare staff
Theme 3: Satisfaction with Care
Older adults and their family satisfaction with VHC was assessed in fourteen studies. In these studies, OAPCC consistently reported limited computer skills, anxiety, and reluctance to adopt new technologies. Some older adults also voiced concerns about the plethora of information influencing their ability to navigate healthcare services (Coorey et al., 2020). Family carer participants in a study expressed doubts regarding the adequacy of virtual assessments in chronic care (Watt et al., 2022). “I think that really matters with older people because … I think [they] need a more detailed kind of assessment. And I just don’t know how that’s possible with a virtual meeting.” Family carer
However, personal anecdotes of older adults confirmed the practical advantages of VHC, such as convenience, reducing the risk of infections, and maintaining family connections (Gately et al., 2022; Iyer et al., 2021, 2023). Examples included the benefits of 6-week in-home exergaming exercises in improving the cognition and anxiety level of older adults with dementia and reducing COVID-19 exposure risks as a significant advantage of telemedicine (Park et al., 2022; Raj et al., 2022). “It’s been a good experience and saved us worry about potential exposure to COVID in a medical setting…” Older adult “Especially now in the pandemic, I would much rather prefer the telephone conversations.” Family carer “Continuous, motivational texts...very encouraging.” Older adult
The last quote resonates with the findings of Park et al. (2022), who found telehealth as effective as face-to-face rehabilitation for chronic pain. Satisfaction with VHC among older adults was influenced by self-motivation, health consciousness, and digital literacy (Coorey et al., 2020).
While family carers were concerned about virtual assessments, healthcare staff satisfaction was found to be closely tied to technology use in health service delivery. Some healthcare staff pointed out the convenience of virtual assessments specifically for addressing cognition but not for mobility issues. “But if you’re doing cognition, it may be easier to do virtual assessment than it is to do one for falls or mobility issues...” Healthcare staff
Provider dissatisfaction about logistical and practical considerations, such as scheduling difficulties and the need for family carers’ involvement during telehealth visits, were noted by Batsis et al. (2020) and Raj et al. (2022). Healthcare staff also reported dissatisfaction in setting up virtual visits due to time and resource constraints (Schoenthaler et al., 2020; Watt et al., 2022). “You start talking about going through the tool and the tool takes twenty minutes.” Healthcare staff “Well, now there’s a barrier because our administrative assistant systems are overwhelmed … we don’t have the resources we need in order to actually set up these virtual visits.” Healthcare staff
Theme 4: Cost-effectiveness
The cost-effectiveness of VHC was described in four studies. In Batsis et al.’s (2020, 2021) studies, focus group participants highlighted that VHC eased their challenge of travelling long distances for treatment. Older adults echoed this sentiment in 2021, noting the accessibility of medical interventions through Modernising Our Workforce for Innovation (MOWI) components and the consequent reduction in excuses for not maintaining health. In addition, telemedicine and remote monitoring via wearable devices surmounted the scarcity of resources, the absence of initiatives, and workforce shortages in chronic care (Batsis et al., 2021). Telehealth saved an average of 166 minutes of travel time for older adults (Hawley et al., 2020). This finding was reinforced by Iyer et al. (2023), where a participant expressed gratitude for the time saved that would otherwise have been spent on half a day’s preparation and travel (Iyer et al., 2023), thus allowing patients to maintain their normal routines at home. “I was very grateful, because it would have been like a half a day. So, it saved me several hours, because you get up, get prepared. We really didn’t have to do anything; we followed our normal routine and just stay here at home.” Older adult
The study by Iyer et al. (2023) noted that VHC can be particularly beneficial for individuals with limited income, helping to save money and pre-visits stress. “It saves money when you have a limited income...” Older adult “Tele-dementia care avoids routine disruption and pre-visit stress, saves several hours.” Healthcare staff
Recommendations to Improve Virtual Health Care for OAPCC
Supplemental File 4 (Table 7) presents an overview of recommendations to improve VHC for OPACC. First, digital health literacy training should be developed to enhance patients’ ability to navigate VHC, with continuous education on symptom recognition, telehealth communication and confidence building. Personalization, such as integrating avatars and storytelling, can increase engagement, while reducing technological complexity through gaming and hands-on training. Family or professional support systems during VHC consultations are recommended to ensure patient comfort and assist with technology use. Clear protocols are necessary to determine when VHC is appropriate and when it is not, particularly for chronic care interventions. Rural-specific programs should be developed to increase access, equity, and social connectedness. Building trust with familiar healthcare providers and using non-verbal communication can enhance the effectiveness of virtual care. New models VHC are needed to address issues like medication management. Promoting the benefits of VHC—such as reduced travel time, optimized resource use, workforce efficiency, convenience, and lower infection risks—can help address equity issues and drive broader adoption. Ensuring access to digital devices for underserved populations and improving the quality of online information are also critical. Multidisciplinary VHC teams can provide comprehensive care, and insurance companies could consider supporting future multidisciplinary care VHC settings. Program designs should consider varying levels of patient motivation, health consciousness, digital literacy, and ensure logistical and practical issues such as scheduling times are clearly defined. A dedicated budget for telemedicine and remote monitoring can address workforce shortages and resource scarcity.
Discussion
Our meta-synthesis builds on the existing scoping reviews, which have illuminated the complex landscape of VHC for OAPCC (Gao et al., 2023; Savira et al., 2023). These scoping reviews identified multiple forces influencing the quality of virtual healthcare: (i) patients’ physical conditions; (ii) patient education/training for using technology; (iii) lack of motivation among health service providers; and (iv) staffing and legislation issues. We have expanded this exploration to focus on preventable chronic conditions and explored scenarios where older adults, their families, and healthcare providers respond to quality aspects of VAC. As expected, our review revealed that OAPCC often welcome technological advancement in health service delivery. However, the potential for VHC is tempered by the realities of the digital divide, necessitating targeted solutions to ensure equitable access, especially for those from rural or underprivileged backgrounds (Frydman et al., 2022). Resources and strategies available to them—not always evenly distributed—largely resemble “one-size-fits-all” measures that may not adequately address the challenges faced by this demographic. By applying the Mayo Clinic’s VCQF (Demaerschalk et al., 2023), we can better understand how to address these challenges and optimize VHC for OAPCC. Furthermore, the framework provided useful to translate the evidence into recommendations to improve virtual health care service design, delivery, and practical implementation for older people with chronic conditions. To our knowledge, this is the first study to do so.
The VCQF’s functionality domain examines VHC’s clinical, operational, and technical aspects (Demaerschalk et al., 2023). Our findings highlight that while telemedicine offers convenience, OAPCC often face technological barriers. Innovative solutions like the tele-Exergame system and personalized VHC, such as avatars, have shown promise in reducing these challenges (Chanpimol et al., 2020; Orta Portillo et al., 2023). However, ongoing support and training for patients and providers are essential to improve usage and effectiveness of virtual platforms (Haleem et al., 2021). The VCQF’s equity domain ensures that all patients have access to VHC, regardless of their socioeconomic status or geographic location (Demaerschalk et al., 2023). Our review found telemedicine has improved access to healthcare for rural and underserved populations by reducing travel burdens and addressing workforce shortages. However, disparities persist due to the digital divide, which requires targeted policies to enhance digital literacy and provide affordable technological solutions (Saeed & Masters, 2021). Addressing these inequities is important to ensure that VHC is accessible to all older adults including OAPCC.
The VCQF’s experiential domain encompasses the subjective experiences of patients, families, and clinicians (Demaerschalk et al., 2023). Our synthesis indicates high satisfaction among patients and providers due to the convenience and reduced risk of infections during the COVID-19 pandemic and beyond. However, concerns about the adequacy of virtual assessments for complex conditions and the need for more integrated and personalized care persist (Nene et al., 2023). Complex care requires a multidisciplinary approach, but barriers like independent insurance providers (Ailabouni et al., 2022; Batsis et al., 2020) and predominantly siloed structures in healthcare education and workplaces often carry over into virtual healthcare settings, hindering effective team-based collaboration. Continuous education and training for patients and providers are essential to improve confidence and engagement in VHC (Curran et al., 2023). Finally, cost-effectiveness evaluates the economic benefits of VHC. One study showed significant time savings for OAPCC, with telemedicine reducing an average of 166 minutes of travel time (Hawley et al., 2020). This not only alleviates the burden on patients but also enhances the efficiency of healthcare delivery. Additionally, VHC can reduce healthcare costs by preventing hospitalizations and enabling timely interventions (Demaerschalk et al., 2023; Snoswell et al., 2020).
VHC efficiently addresses care needs of OAPCC, capitalizing on the potential for early intervention and ongoing management (Clarke et al., 2017). Conditions such as prediabetes, early-stage hypertension, and hyperlipidemia often require continuous monitoring and lifestyle adjustments that can be significantly supported through virtual technologies (Fundoiano-Hershcovitz et al., 2022). By implementing telehealth solutions, healthcare providers can deliver preventive care that is both proactive and reactive to the nuances of these conditions.
VHC platforms offer a host of services that are essential for managing preventable conditions, starting with virtual screenings and assessments (Mehraeen et al., 2023). These tools enable collecting and analyzing health data without frequent physical visits, making regular monitoring achievable. For instance, mobile health apps can prompt patients to check their blood pressure and blood glucose levels, automatically transmitting data to their healthcare providers (Oh et al., 2022). This seamless exchange of information ensures that any necessary adjustments in medication or diet can be swiftly implemented, halting the progression of conditions that could otherwise lead to more severe health issues.
Furthermore, virtual platforms are pivotal in promoting personalized patient education and engagement, which are keys to the self-management of preventable conditions (Sawesi et al., 2016). Through virtual consultations, healthcare providers can provide tailored advice on diet, physical activity, and lifestyle changes specific to the individual’s health status and needs. This personalized approach not only boosts the effectiveness of preventive measures but also cultivates a deeper understanding and commitment on the part of the patient, leading to improved health outcomes (Gaffney & Hamiduzzaman, 2022). Additionally, VHC can extend to include specialized telerehabilitation for older adults who are managing the aftermath of events like strokes or surgical procedures related to their chronic conditions. These services provide patients access to physiotherapy and other rehabilitative sessions through video conferencing, enabling consistent, supervised recovery routines without the logistical challenges of travelling to healthcare facilities. By integrating these virtual services into the standard care protocols, healthcare systems can offer a more responsive and adaptable approach to preventing and managing chronic conditions in older adults (Savira et al., 2023). This model not only maximizes the efficiency of health service delivery but also aligns closely with the needs and lifestyles of the elderly population, ensuring that preventive care is accessible and practical.
For older adults, the distinction between general health services for chronic diseases and those designed for preventable chronic conditions is crucial in optimizing care and improving outcomes (Grover & Joshi, 2014). General health services often focus on managing symptoms and complications of established chronic diseases such as heart failure, advanced diabetes, and chronic obstructive pulmonary disease (Anekwe & Rahkovsky, 2018). These services typically emphasize medication management, routine monitoring, and acute exacerbations, reflecting a reactive approach to health complications arising from such conditions. In contrast, health services for preventable chronic conditions, such as prediabetes, early-stage hypertension, and osteoporosis, adopt a proactive strategy (Sadiq, 2023). These services prioritize early detection through regular screenings, preventive treatments, and comprehensive lifestyle interventions to halt disease progression. VHC platforms enhance this approach by facilitating continuous remote monitoring and personalized care plans, which can adjust treatments as needed before conditions worsen. This tailored approach aligns with the need for more frequent and specific interventions. It empowers older adults through self-management tools and educational resources that are integral to preventing the escalation of these conditions (Burton et al., 2022).
Screening and early detection form the cornerstone of managing preventable chronic conditions (Fragala et al., 2019). Virtual health services facilitate these processes through technologies that enable remote monitoring and data collection. For instance, wearable devices can track vital signs, blood sugar levels, and other physiological metrics critical for the early detection of diabetes and hypertension (Alhaddad et al., 2022). These devices can alert both the patient and healthcare provider to abnormalities that may indicate the onset or progression of a condition (Alhaddad et al., 2022). Virtual platforms can thus ensure timely intervention, turning screening from a periodic to a continuous process. This shift is crucial for older adults who benefit significantly from immediate healthcare regimen adjustments, potentially reducing the need for more intensive treatments.
Effective integration of VHC within standard healthcare protocols is essential. Policy frameworks must support this integration by providing adequate funding, training, and infrastructural investments to ensure that virtual services are as robust as traditional care approaches (Srivastava et al., 2023). Additionally, regulatory standards require updates to reflect the specific requirements of VHC, focusing on privacy, data security, interoperability of systems, and cross-jurisdictional practice and standardization. In addition, ongoing training for healthcare providers and healthcare students is crucial to use virtual health technologies effectively (Curran et al., 2023). This training should cover technical skills, patient engagement strategies, and the application of data analytics to personalize care (Sadiq, 2023). Furthermore, embedding virtual health care skills training and guidelines into medical programs and other health programs is essential to prepare the future health workforce (Pit et al., 2021). VHC should prioritize integration and patient-centered care, utilizing user-friendly technologies and providing flexible communication options.
Conclusions
This meta-synthesis has demonstrated that VHC holds transformative potential for managing preventable chronic conditions among older adults. By enhancing accessibility and allowing for timely interventions, virtual care can significantly reduce the burdens on both patients and healthcare systems. Effective implementation, however, requires supportive health policies that ensure virtual services are robust and sustainable. This includes updating regulatory standards to secure patient data and adapting reimbursement policies to promote the adoption of virtual care. Clinically, providers must be well-trained in VHC’s technical and patient engagement aspects to deliver effective, personalised care. Mayo Clinic’s Virtual Care Quality Framework can be used to move beyond problem description and provide scientific evidence to improve care and identify effective strategies for successful implementation. Future research should focus on long-term outcomes and the continuous improvement of VHC technologies. Ultimately, integrating virtual care into existing health frameworks can significantly improve the quality of life for older adults while making health systems more efficient and responsive.
Supplemental Material
Supplemental Material - Virtual Healthcare for Older Adults With Preventable Chronic Conditions: A Meta-synthesis of Quality Aspects
Supplemental Material for Virtual Healthcare for Older Adults With Preventable Chronic Conditions: A Meta-synthesis of Quality Aspects by Mohammad Hamiduzzaman, Harry James Gaffney, Shruti Jindal, Mahua Patra, Raghavendra Gudur, Sabrina Pit, and Aziz Rahman in Journal of Applied Gerontology
Supplemental Material
Supplemental Material - Virtual Healthcare for Older Adults With Preventable Chronic Conditions: A Meta-synthesis of Quality Aspects
Supplemental Material for Virtual Healthcare for Older Adults With Preventable Chronic Conditions: A Meta-synthesis of Quality Aspects by Mohammad Hamiduzzaman, Harry James Gaffney, Shruti Jindal, Mahua Patra, Raghavendra Gudur, Sabrina Pit, and Aziz Rahman in Journal of Applied Gerontology
Supplemental Material
Supplemental Material - Virtual Healthcare for Older Adults With Preventable Chronic Conditions: A Meta-synthesis of Quality Aspects
Supplemental Material for Virtual Healthcare for Older Adults With Preventable Chronic Conditions: A Meta-synthesis of Quality Aspects by Mohammad Hamiduzzaman, Harry James Gaffney, Shruti Jindal, Mahua Patra, Raghavendra Gudur, Sabrina Pit, and Aziz Rahman in Journal of Applied Gerontology
Supplemental Material
Supplemental Material - Virtual Healthcare for Older Adults With Preventable Chronic Conditions: A Meta-synthesis of Quality Aspects
Supplemental Material for Virtual Healthcare for Older Adults With Preventable Chronic Conditions: A Meta-synthesis of Quality Aspects by Mohammad Hamiduzzaman, Harry James Gaffney, Shruti Jindal, Mahua Patra, Raghavendra Gudur, Sabrina Pit, and Aziz Rahman in Journal of Applied Gerontology
Footnotes
Author Contributions
Mohammad Hamiduzzaman: Conceptualization, Methodology, Data curation, Project Administration, Formal analysis, Visualization, Writing – original draft. Harry Gaffney: Formal analysis, Writing – original draft, Writing – review & editing, Validation. Shruti Jindal: Data curation, Visualization, Writing – review & editing. Mahua Patra: Data curation, Visualization, Writing – review & editing. Raghavendra Gudur: Conceptualization, Writing – review & editing, Validation. Sabrina Pit: Conceptualization, Writing – review & editing, Validation. Aziz Rahman: Conceptualization, Writing – review & editing, Validation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.