
Abstract
This study examined associations between three levels of social exclusion and quality of life in the Australian oldest old. We performed cross-sectional analyses of the Household, Income and Labour Dynamics in Australia data using 203 participants aged ≥85. Principal component analysis was used to construct social exclusion variables at an individual level (lack of supportive relationships), neighborhood level (disadvantaged neighborhood social climates), and community level (community disengagement). Quality of life was assessed using physical and mental component summary scores of SF-36. Multiple linear regression analysis was performed separately for men and women. Lack of supportive relationships was negatively associated with physical and mental quality of life in all participants. Among men, community disengagement was associated with low physical quality of life. Policies to reduce social exclusion in this age group should focus on improving supportive relationships to enhance quality of life, rather than neighborhood or community levels.
• Different levels of social exclusion affect men and women differently. • This study provides further evidence for the importance of supportive relationships at an individual level for quality of life in the oldest old. • Neighborhood social climates are not associated with poor quality of life.
• The individual level of social exclusion needs to be prioritized more to improve older people’s quality of life than neighborhood and community levels of social exclusion. • Men may benefit from community engagement interventions in the physical quality of life.What this paper adds
Applications of study findings
Introduction
In many countries around the world, life expectancy is increasing (Australian Bureau of Statistics, 2018; World Health Organization, 2015). In Australia, the number of people over 85 is projected to double between 2017 and 2042, reaching more than one million people (Australian Bureau of Statistics, 2018). Several factors have contributed to increasing life expectancy, including improved healthcare services and medical treatment and declining child mortality (Brown, 2015). While increasing life expectancy is a positive development, it carries a responsibility to optimize the quality of life and social participation of older people (Key & Culliney, 2018).
There is evidence that older people are vulnerable to social exclusion (Kneale, 2012). Social exclusion is a multidimensional concept that results in people being disconnected from society (Huisman & van Tilburg, 2021). It exacerbates inequality, reduces social participation (Huisman & van Tilburg, 2021), and is associated with lower quality of life (Levitas et al., 2007). Social exclusion has negative effects on the health of older people, in particular their mental health (Santini et al., 2020). The multidimensional nature of social exclusion means that it may affect mental health in older people through different pathways. For example, social disconnectedness (assessed by small social networks and infrequent social interaction) and perceptions of social isolation (assessed by loneliness) have been found to be related to more depression and anxiety symptom severity in community-dwelling older adults (Santini et al., 2020). Evidence points to the key role of the older person’s “perception” of isolation for mental health, rather than simply the size of social networks and frequency of social interactions. Older adults who perceive that the meaning and quality of social relationships are poor are at a greater risk of depression and anxiety (Santini et al., 2020).
In Australia, social exclusion has previously been examined in relation to measures of socioeconomic status in men and women. For instance, Paine, Rachele et al. (2022) found that men and women with lower completed education had higher levels of social exclusion, suggesting that education is beneficial for maintaining social connection. Interestingly, the authors assessed social exclusion in this case by the degree of community disengagement. In so doing, they highlighted that social exclusion may exist at different levels, from lack of supportive relationships (individual level) to disadvantaged neighborhood social climates (neighborhood level) through to community disengagement (community level) (Paine, Rachele et al., 2022). These levels of social exclusion are consistent with the contested definition of social exclusion in the literature (Walsh et al., 2017). Importantly, they provide a more nuanced understanding of the construct of social exclusion, suggesting that the experiences of social exclusion differ between men and women. These gender differences are feasible because of differences between men and women in participation in employment, family and domestic responsibilities, and gender power imbalances during the life course. An important limitation of this study is that it did not examine whether these levels of social exclusion were associated with quality of life in men and women.
Another qualitative study of social exclusion in older Australians reported that people aged 80 and over living in government housing can be satisfied with their lives even though they have social exclusion (Paine, Lowe et al., 2022). A thematic analysis showed supportive relationships and neighborhood cohesion as factors impacting social exclusion. Although this study provides valuable perspectives from advanced-aged people, it did not examine quality of life. Moreover, the participants may not represent vulnerable older Australians due to the study design (e.g., door-knocking recruitment). This underlines that further investigations of different levels of social exclusion and quality of life with representative samples of older Australians are needed.
Quality of life is a critical element in healthy aging (Engelen et al., 2022). The World Health Organization defines quality of life as “individuals’ perceptions of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns” (World Health Organization, 2012, p. 11). It is a complex concept that combines subjective and objective perspectives and involves social, material, physical, and emotional well-being, life conditions, and personal values and satisfaction (Felce & Perry, 1995). Quality of life can be measured by scaling tools from which scores can be generated, such as 36-item short-form (SF-36) and Euro-QoL 5-Dimensions, which are common generic questionnaires for use in the adult population (Haraldstad et al., 2019).
There is evidence that older people are vulnerable to reduced quality of life owing to such factors as increased risk of chronic diseases (Gündoğdu et al., 2019) and loss of independence (Netuveli & Blane, 2008). Furthermore, older people (65 years and older) reported lower quality of life when they had to depend on others because of functional limitations (Netuveli & Blane, 2008). Previous studies of social exclusion and quality of life in older people have found that older people perceived a declining quality of life when they had reduced social contacts and activities through the deaths of family and friends (Netuveli & Blane, 2008). However, previous studies have not investigated social exclusion at individual, neighborhood, and community levels in relation to quality of life. They have also not examined whether these relationships differ between men and women, which is important given that the experience of men and women of social exclusion may differ. Examining the association of levels of social exclusion, such as lack of supportive relationships, disadvantaged neighborhood social climates, and community disengagement, and quality of life in men and women will provide a more nuanced understanding to inform policy interventions. The negative impacts of social exclusion are expected to be greater in the oldest old, who are more likely to be single or widowed, financially constrained, and have decreased physical capability. Thus, this study aimed to examine the association between social exclusion and quality of life in people aged 85 years and older using the Household, Income and Labour Dynamics in Australia (HILDA) data. The objectives were, in people aged 85 years and older, to (1) identify whether levels of social exclusion are associated with quality of life and (2) determine the differences in the association of social exclusion and quality of life between men and women.
Methods
Data
This is a cross-sectional examination of the relationship between social exclusion and quality of life in people aged 85 years and older living in Australia using secondary quantitative data from the HILDA dataset (Department of Social Services, 2022). The HILDA survey is an ongoing Australian government-funded national household-based study that started in 2001. It follows up more than 17,000 Australians annually. Wave 1 collected data to represent Australian households from 13,969 respondents in 7682 households in 2001. Wave 11 added 5462 individuals from 2153 households in 2011. All people aged 15 years and over are invited to participate in the survey within a household, and they are allowed to enter and exit anytime. The details of the sample selection are published elsewhere (Watson and Wooden, 2002). Data are collected through household questionnaires and a combination of individual self-administered questionnaires and telephone and face-to-face interviews. The survey data provides information about general, physical, and mental health, well-being, personal characteristics as well as work-related factors and financial status. The HILDA team provides assurances of data quality (Summerfield et al., 2021). In the current study, the data from wave 20 of the self-completed questionnaires (collected between 4 August 2020 and 7 February 2021) were used because it was the latest available data that included social exclusion variables at the time of the research. In this study, sex refers to biological attributes and is categorized as men and women. Approval to use deidentified secondary data of the HILDA was obtained from the Australian Catholic University Human Research Ethics Committee (register number: 2023-3249N).
Analysis
A principal component analysis (PCA) with Varimax rotation was used to reduce the dimensionality of input variables, namely, social exclusion of lack of supportive relationships and disadvantaged neighborhood social climates. Components with eigenvalues greater than one were included in the analysis. Principal components were generated, which were weighted scores of the input variables. Cross-loaded variables were excluded. The PCA was used to inform the multiple linear regression analysis.
Measures
Social Exclusion Measures
Social exclusion measures and scores were developed following the methods outlined in Paine, Rachele et al. (2022). They included three levels: lack of supportive relationships, disadvantaged neighborhood social climate, and community disengagement.
Lack of Supportive Relationships
Final Component Loadings for the HILDA Survey Items Measuring the Lack of Supportive Relationships.
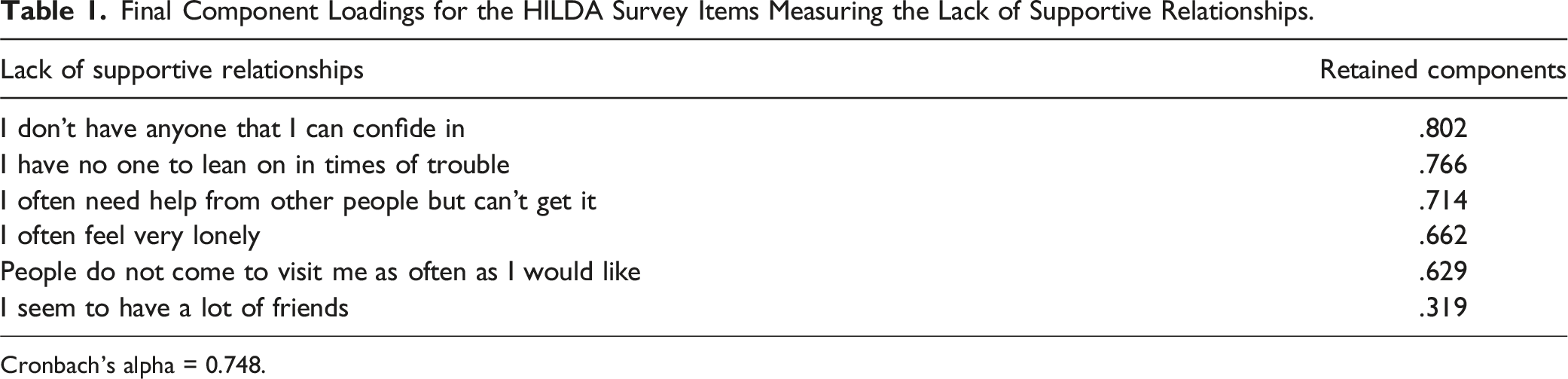
Cronbach's alpha = 0.748.
Disadvantaged Neighborhood Social Climates
Final Component Loadings for the HILDA Survey Items Measuring Disadvantaged Neighborhood Social Climates.
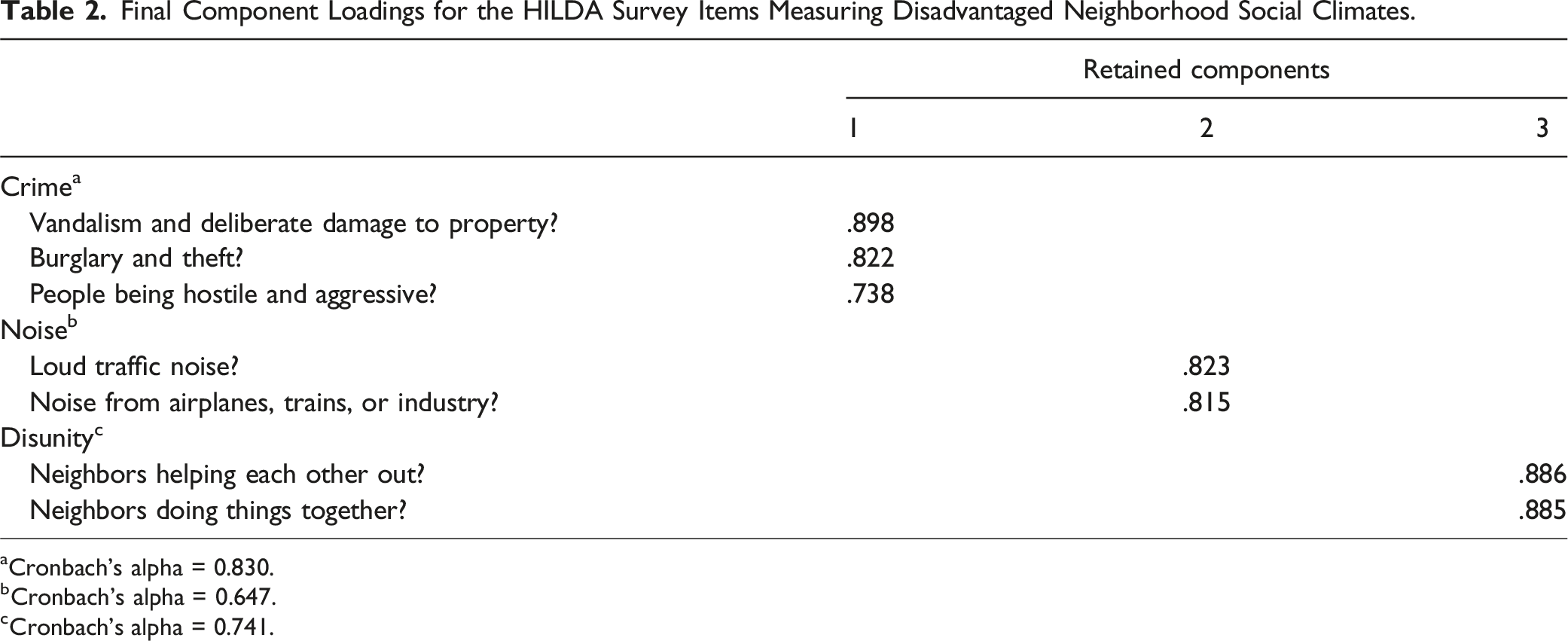
aCronbach's alpha = 0.830.
bCronbach's alpha = 0.647.
cCronbach's alpha = 0.741.
Community Disengagement
A scale of community disengagement was developed by summing two items in the B22 survey section (Melbourne Institute: Applied Economic & Social Research, 2020) with a 7-point Likert scale ranging from every day or most days (1) to not at all (7). Two items were activities that people had to leave the house, such as going to museums and going to the movies and other events. Higher scores refer to higher disengagement in the community, meaning higher vulnerability to social exclusion.
Quality of Life Measures
Quality of life was assessed using the SF-36 in the HILDA survey. SF-36 is commonly used to measure the generic quality of life with good reliability and validity (Haraldstad et al., 2019; McHorney et al., 1994). SF-36 yields two summary scores: physical component summary (PCS) and mental component summary (MCS) scores (Ware et al., 1994). Following the manual (Ware et al., 1994), PCS and MCS scores were generated for each participant. Individual PCS and MCS scores were not generated if data were missing on any of the eight domains as recommended (Ware et al., 1994).
Sociodemographic Characteristic Measures
The sociodemographic characteristic measurements were age, household composition, country of birth, housing tenure, annual income, level of education, and area disadvantage, following the methods of Paine, Rachele et al. (2022). The household composition was coded into two categories: “do not live alone” and “live alone.” Country of birth was used to indicate English proficiency and categorized whether respondents were born in English-speaking countries. Housing tenure was categorized from three questions: (1) own/currently paying off mortgage, (2) rent or pay board, and (3) live here rent free. The first category was coded into “own home” and the latter two were coded into “not own home.” Annual income was based on total household disposable income and categorized into quantiles. The level of education was derived from the highest education level achieved and coded into two categories: year 11 and below and year 12 and higher (including tertiary education). Area disadvantage was based on Socio-Economic Indexes for Areas developed by the Australian Bureau of Statistics (2022) and coded into most disadvantage (Quintile 5) and least disadvantage (Quintiles 1–4).
Regression Analysis
Data for participants aged 85 years and older who responded to the HILDA self-reported survey were extracted from wave 20 dataset (n = 391 [163 men and 228 women]). Those with missing data for variables of social exclusion and quality of life were excluded leaving 203 (81 men and 122 women) included in the analysis. Multiple linear regression was undertaken to investigate the association between social exclusion (independent variables) and quality of life (dependent variables), controlling for sociodemographic characteristics (covariates). Men and women were assessed separately. Data were analyzed using IBM SPSS Statistics Version 28.0.1. p-Values less than 0.05 were regarded as statistically significant.
Results
Sociodemographic Characteristics
Descriptive Summary of Participants−Sociodemographic Characteristics and Social Exclusion and Quality of Life Scores (Australians Aged 85–99).
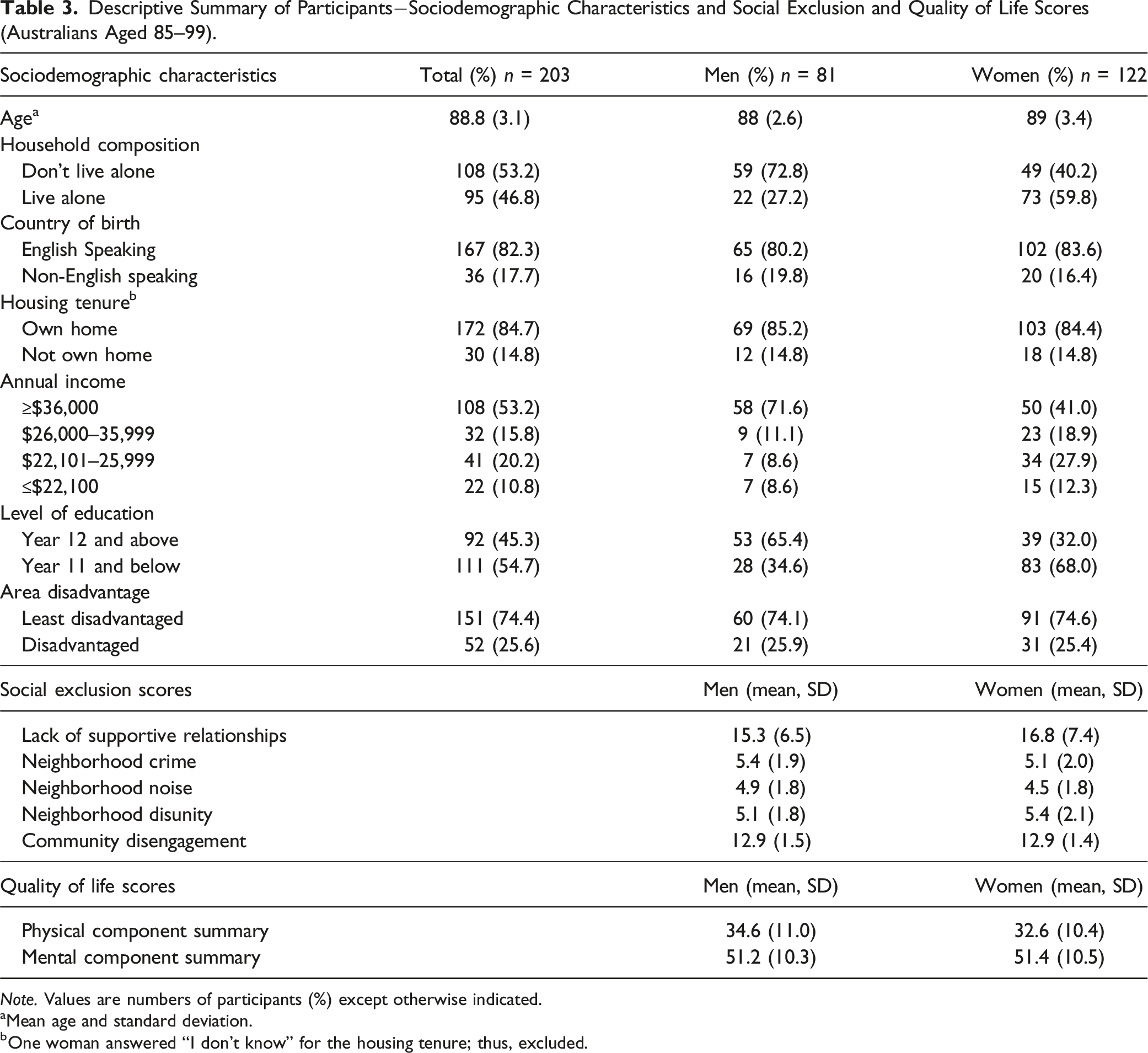
Note. Values are numbers of participants (%) except otherwise indicated.
aMean age and standard deviation.
bOne woman answered “I don’t know” for the housing tenure; thus, excluded.
Objective 1: The Associations of Social Exclusion and Quality of Life in Participants
Unadjusted and Adjusted Multiple Linear Regression Analyses for Predictions of Quality of Life (Men).
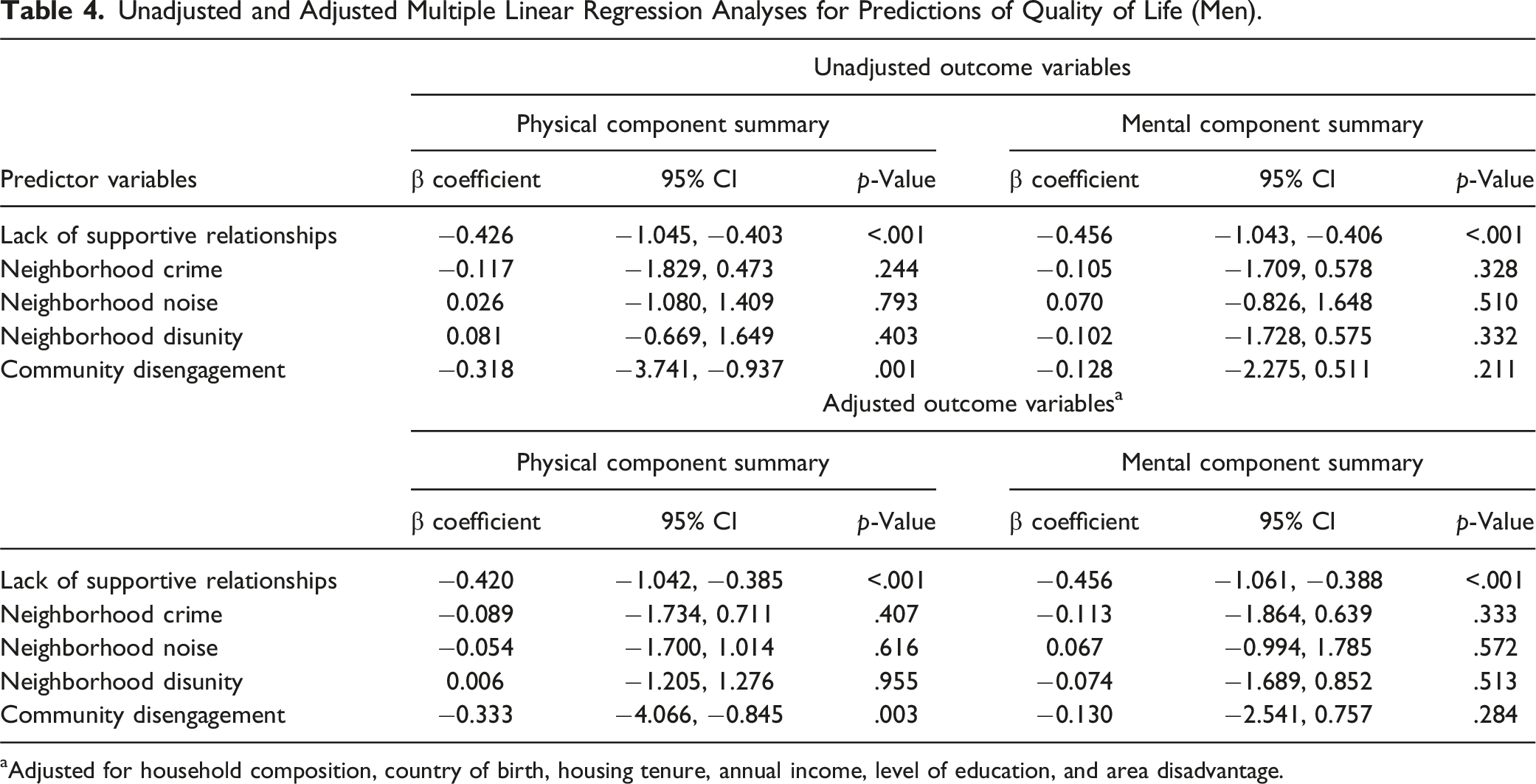
aAdjusted for household composition, country of birth, housing tenure, annual income, level of education, and area disadvantage.
Unadjusted and Adjusted Multiple Linear Regression Analyses for Predictions of Quality of Life (Women).
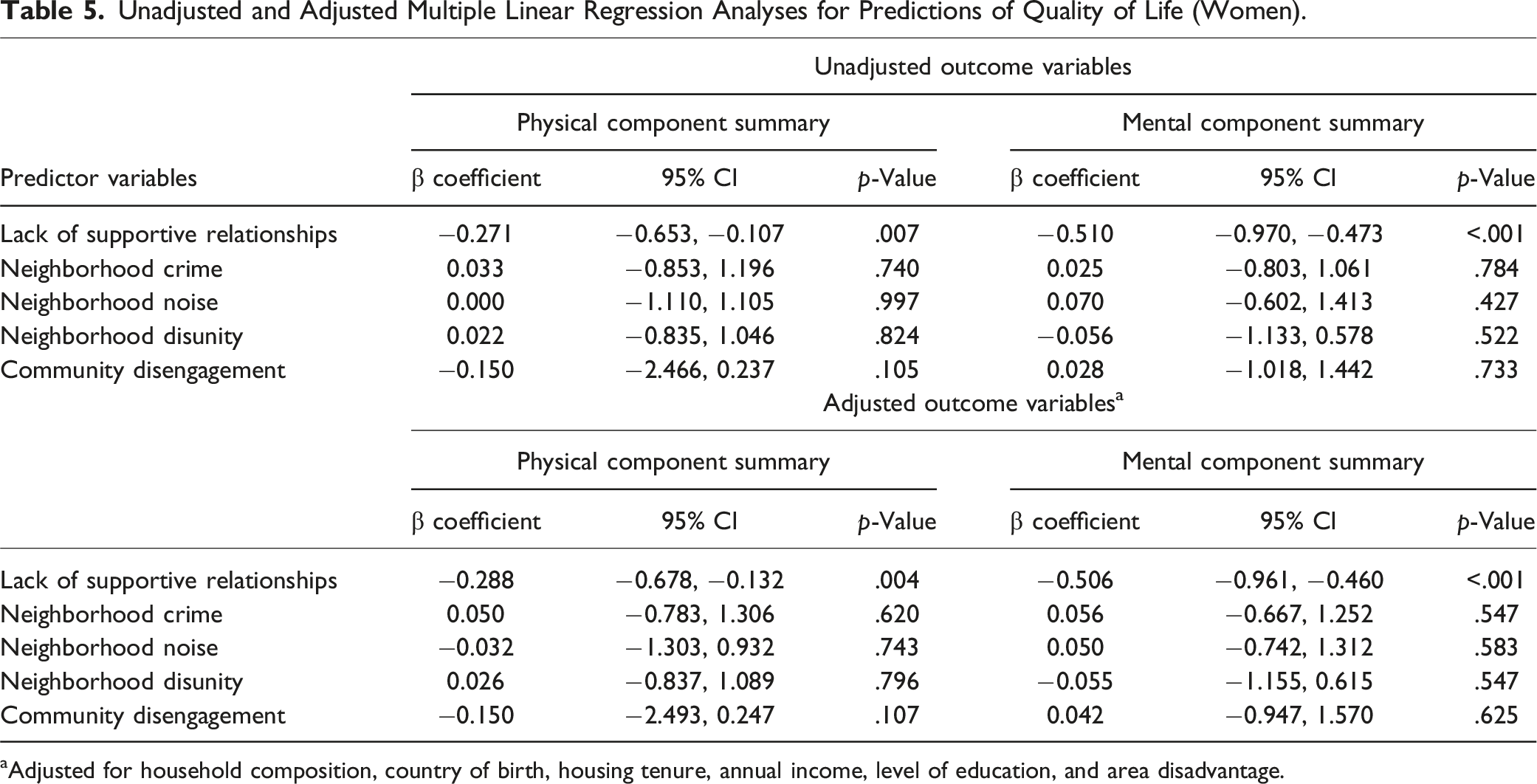
aAdjusted for household composition, country of birth, housing tenure, annual income, level of education, and area disadvantage.
Objective 2: Differences Between Men and Women Regarding Social Exclusion Effects on Quality of Life
Among men, community disengagement was negatively associated with PCS scores (β = −0.333; 95% CI −4.066, −0.845; p = .003) (Table 4). However, no associations were shown among women between community disengagement and PCS scores (β = −0.150; 95% CI −2.493, 0.247; p = .11) (Table 5). Disadvantaged neighborhood social climates, including neighborhood crime, noise, and disunity, did not show a statistically significant association with PCS and MCS scores in men and women (Tables 4 and 5).
Discussion
This study examined associations between three levels of social exclusion and quality of life in the oldest old (aged ≥85) in Australia. We found that social exclusion assessed by lack of supportive relationships was negatively associated with the physical and mental component quality of life in all participants. We also found differences between men and women regarding the effects of social exclusion assessed by community disengagement on quality of life. Our findings highlight the importance of improving supportive relationships.
Among people aged 85–99, we found that lack of supportive relationships was associated with low physical quality of life. This is consistent with a UK study that reported people aged 65 years and older living in their homes perceived negative quality of life when they had reduced social contacts following the deaths of their family and friends as they aged (Netuveli & Blane, 2008). Our finding adds to this as we used the oldest old population. Our data emphasizes the importance of improving lack of supportive relationships between older people in private dwellings and their family members, friends, and other contacts. The implication is that more investment is needed to increase support for carers of older people to allow them to increase the frequency of their visits and improve their quality (Temple et al., 2021). It also suggests that investment in befriending programs, in which volunteers visit older people, is warranted (Department of Health, 2017). One such volunteer program is the Aged Care Volunteer Visitors Scheme (ACVVS), formerly known as the Community Visitors Scheme (CVS) (Department of Health and Aged Care, 2023). This Australian government-funded program aims to provide friendship and companionship to older people who feel isolated through regular volunteer visits (Department of Health and Aged Care, 2023). Further research is required to examine the effectiveness of the ACVVS in improving supportive relationships.
We found that in all participants, lack of supportive relationships was also associated with a decline in mental quality of life. This result is consistent with a US study that demonstrated social exclusion negatively affected mental health in older people (Santini et al., 2020). The US study was a longitudinal mediation analysis that found that disconnectedness from society predicted higher depression and anxiety symptoms in older people aged 57–85 years (Santini et al., 2020). Our results complement this data as they suggest this is also the case in the oldest old. Although MCS scores do not diagnose depression or anxiety, they reflect mental health status. Mental health status is most likely affected by social exclusion at an individual level, while social exclusion at neighborhood and community levels did not affect mental quality of life in men and women. Our findings suggest that social exclusion on an individual level, as assessed by lack of supportive relationships, needs to be focused on improving older people’s quality of life. For example, there is emerging evidence that online social networking may have the potential to improve lack of supportive relationships and develop friendships in this age group (Chen et al., 2022; Gil-Clavel et al., 2022). Although it may be hard to find a new friend in person, there are opportunities to meet new friends virtually through online social networking (Chen et al., 2022). The benefits may also extend to existing friendships by having more frequent meetings and conversations online. This is particularly relevant when there are geographical barriers, such as children living away from their old age parents (Chen et al., 2022). Further research is needed to explore whether online friendships may be a potential aid for older people to reduce social exclusion by examining cost, access, and online training needs in older people.
Among men, we found that social exclusion at the community level, as assessed by community disengagement, was associated with low physical quality of life. This result is consistent with the previous study demonstrating that participating in social activities is an important factor for good quality of life in people aged 65 years and older (Netuveli & Blane, 2008). Conversely, for women, community disengagement was not associated with a low physical quality of life. It may be explained by women being the primary carers of their partners in this age group and tending to do household chores (Swinkels et al., 2019), leading to more physical activity in daily life than men. The implication is that when health policy and interventions are revised and developed, sex differences need to be considered. For example, when an intervention is designed to improve the physical aspect of quality of life in older people, it may be strategic to focus on men. Some such initiatives already exist. For example, the Australian Men’s Shed Association is designed to allow men to socialize, engage in activities, and share common interests (Australian Men’s Shed Association, 2024). The Men’s Shed initiative has been found to improve well-being in older men, and 95% of participants are satisfied with the program (Waling & Fildes, 2017).
The key strength of this study is using the data from the HILDA survey, which is a nationally representative study. This study is the first research with nationally representative data to examine the association between three levels of social exclusion and two domains of quality of life. The results can be generalized to the population aged 85–99 years living in private dwellings. The study is limited because it is a cross-sectional study; thus, causal inferences cannot be made. A longitudinal analysis would be required to determine causality for future research. The data used in this study is based on the self-reported questionnaire, which can be subject to social desirability bias (Demetriou et al., 2015). Also, social exclusion was measured by a Likert scale and the scores were generated. A Likert scale may not show the precise score of social exclusion in the way that continuous measures do. In addition, there are considerations of COVID-19 since wave 20 was collected between 4 August 2020 and 7 February 2021. In the data collection process, although face-to-face interviews were replaced with telephone interviews due to the circumstances, there were no significant missing data and rates compared to the previous waves (Watson et al., 2021). The quality of the wave 20 data was reported to be similar to the previous waves despite unexpected challenges during the COVID-19 pandemic (Watson et al., 2021).
Findings from this study will inform the design of effective interventions and policies for promoting healthy aging. For example, in the Australian National Preventive Health Strategy 2021–2030 (Department of Health and Aged Care, 2021), social exclusion is identified as adversely affecting social support and participation (social determinants of health). Given that social exclusion exists at various levels, policymakers should consider changing the Strategy in light of the current study’s findings. Our study suggests that greater emphasis should be given to the lack of supportive relationships at the individual level of social exclusion, as this may be the most effective way to improve social exclusion in the oldest old. Also, while the Strategy aims to achieve good health and well-being as long as possible for all Australians, there tends to be a focus on younger generations, particularly in the area of mental health. Our research underlines how older people, especially very advanced age groups of people, can also benefit. As a preventative matter, older people should also be highlighted. With the focus on reducing the individual level of social exclusion, assessed by lack of supportive relationships, investments are required to increase support for older people’s carers and promotion of volunteering programs. For example, promoting befriending programs where people regularly visit the oldest old at their home for companionship could be a promising intervention strategy to facilitate better quality of life outcomes, including the ACVVS (Department of Health, 2017). Regarding community-level interventions and health policies, sex differences need to be considered with the impact of community disengagement on the physical quality of life. Future research should examine the effectiveness of befriending programs and online friendships and explore their enablers and barriers to improve lack of supportive relationships in the oldest old.
Conclusion
This study has found evidence for the association of social exclusion and quality of life in the oldest old in Australia. This differed by sex and social exclusion levels. The individual level of social exclusion, assessed by lack of supportive relationships, had associations with low quality of life in physical and mental domains. Community disengagement was associated with physical quality of life in only men. Our findings support public health responses that include the prevention of social exclusion in later life and interventions to improve supportive relationships. Further research is needed to examine the effectiveness of interventions, such as befriending programs and online friendships for the oldest old.
Footnotes
Acknowledgments
I wish to thank Dr. Jennifer Marks and Dr. Michael Steele for providing valuable feedback and suggestions for this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics statement
Approval to use deidentified secondary data of the Household, Income and Labour Dynamics in Australia was obtained from the Australian Catholic University Human Research Ethics Committee (register number: 2023–3249N).
Data Availability Statement
The data that support the findings of this study are available from the Australian Government Department of Social Services. Restrictions apply to the availability of these data, which were used under license for this study. Data are available ![]() with the permission of the Australian Government Department of Social Services.
with the permission of the Australian Government Department of Social Services.