
Abstract
This secondary data analysis sought to identify characteristics associated with mistreatment among chronic stroke survivors who transition to dementia. We examined baseline data from a multi-time series survey study (n = 453;
• Stroke family caregiver depression is significantly associated with elder mistreatment. • Stroke caregiving may be more burdensome for those whose care recipients have ADRD.
• Improving caregivers’ mental health may be an important strategy for preventing EAN. • Future work should examine timepoints of heightened EAN risk in stroke recovery.What this paper adds
Applications of study findings
Stroke and Alzheimer’s disease and related dementias (ADRD) are common debilitating chronic conditions presenting significant challenges for patients and their caregivers. Dementia risk is elevated three-fold in the first year after a stroke, decreases to 1.5-fold by 5 years, and remains elevated 20 years afterward (Joundi et al., 2024). As a known precursor to vascular dementia (Rost et al., 2022), stroke is a leading cause of death and disability projected to affect 4% of the U.S. population by 2030 (Virani et al., 2020).
Since stroke is a separate medical condition that requires caregiving and also contributes to dementia, understanding caregiving for stroke survivors in those with ADRD is critical. However, little is known about how stroke may complicate ADRD caregiving. The ADRD caregiving trajectory is defined by increased dependence on caregivers to manage behavioral and psychological symptoms accompanying a care recipient’s gradual cognitive decline, whereas stroke caregiving is needed suddenly. Compared to the general population of caregivers of those with non-stroke-related conditions, caregivers of stroke survivors experience greater social, occupational, and financial disruptions (King & Semik, 2006), which often result in higher levels of burden, depression, and anxiety (Loh et al., 2017). The stroke family caregiving journey, including transition from chronic stroke to ADRD, has not been well characterized including how these caregivers compare to “newer” caregivers on outcomes such as elder abuse and neglect (EAN).
EAN includes neglect, financial, emotional, physical, and sexual abuse (Pillemer et al., 2016). Approximately 10% of U.S. adults experience EAN yearly (Acierno et al., 2010). Known risk factors for EAN include those with impairments in basic and instrumental activities of daily living (ADLs), dependence on others for accessing and receiving healthcare, needs for financial management, and low social support—characteristics which aptly describe stroke survivors, and those with ADRD. Despite this heightened context for EAN, there is a dearth of data on EAN amongst stroke survivors and their caregivers. Identifying context-specific differences in EAN among those with ADRD and stroke history compared to those with ADRD only, may assist health professionals in anticipating and addressing specific caregiver challenges. This study assessed characteristic differences between ADRD family caregivers of care recipients with a previous stroke history and those without.
Methods
This is a secondary data analysis of baseline data from multi-time series study on caregiving experiences examining contextual factors influencing dementia family caregivers’ abusive or neglectful behaviors over time. Participants completed a baseline survey followed by 21-days of daily diary surveys at enrollment, 6-, and 12-months. A third-party honest broker (Choi et al., 2015) was used to administer the data collection software so that the research team was blinded and data remained anonymous. This project was approved as exempt by the Institutional Review Board.
Participants
Participants were recruited across the U.S., through community outreach, print media, and online social media channels. Eligibility criteria were adults over 18 years old, who provided unpaid care and lived with a family member who was at least 60 years old, and with mild cognitive impairment or dementia based on the Eight-item Informant Interview to Differentiate Aging and Dementia (AD8®) (Galvin et al., 2005). Those unable to speak or read English or Spanish, or without internet access were excluded from the study.
Measures
Caregivers reported sociodemographic data and information about the number of hours per week: caring for someone other than the care recipient, working for pay outside the home, and paying others to provide care for the recipient. Physical health ratings and ability to perform ADLS were evaluated with two Patient Reported Outcomes Measurement Information System (PROMIS®) physical function items (Hays et al., 2009). Caregivers’ assistance with ADLs over the previous 6 months was captured using 13-items from the Katz Index of Independence in Activities of Daily Living (Katz, 1983). Finances were assessed through three items pertaining to adequate financial resources, difficulty, and strain (Given et al., 1992). The 4-item short form PROMIS social isolation tool was used (Cella et al., 2010). The Patient Health Questionnaire (PHQ-9) (Kroenke & Spitzer, 2002) and Generalized Anxiety Disorder scale (GAD-7) (Spitzer et al., 2006), respectively, evaluated for depression and anxiety. A single item assessed for stroke history. EAN was measured through nine questions about the frequency of abusive or neglectful behaviors towards the care recipient over the last six months. Items within subscales of the Conflict Tactics Scale-Revised and Conflict-Tactics Scale-Older Adults
Data Analysis
Statistical analyses were performed with R v.4.3.2. (R Core Team, 2018). Descriptive and inferential analysis characterized demographic and clinical characteristics, and tested for group differences between family caregivers of older adults with stroke history and those without. T-tests were conducted to test between-group differences for continuous variables, while between-group differences for categorical outcomes were assessed with Chi-squared analysis.
Results
Sample Comparisons by Stroke History (N = 453).
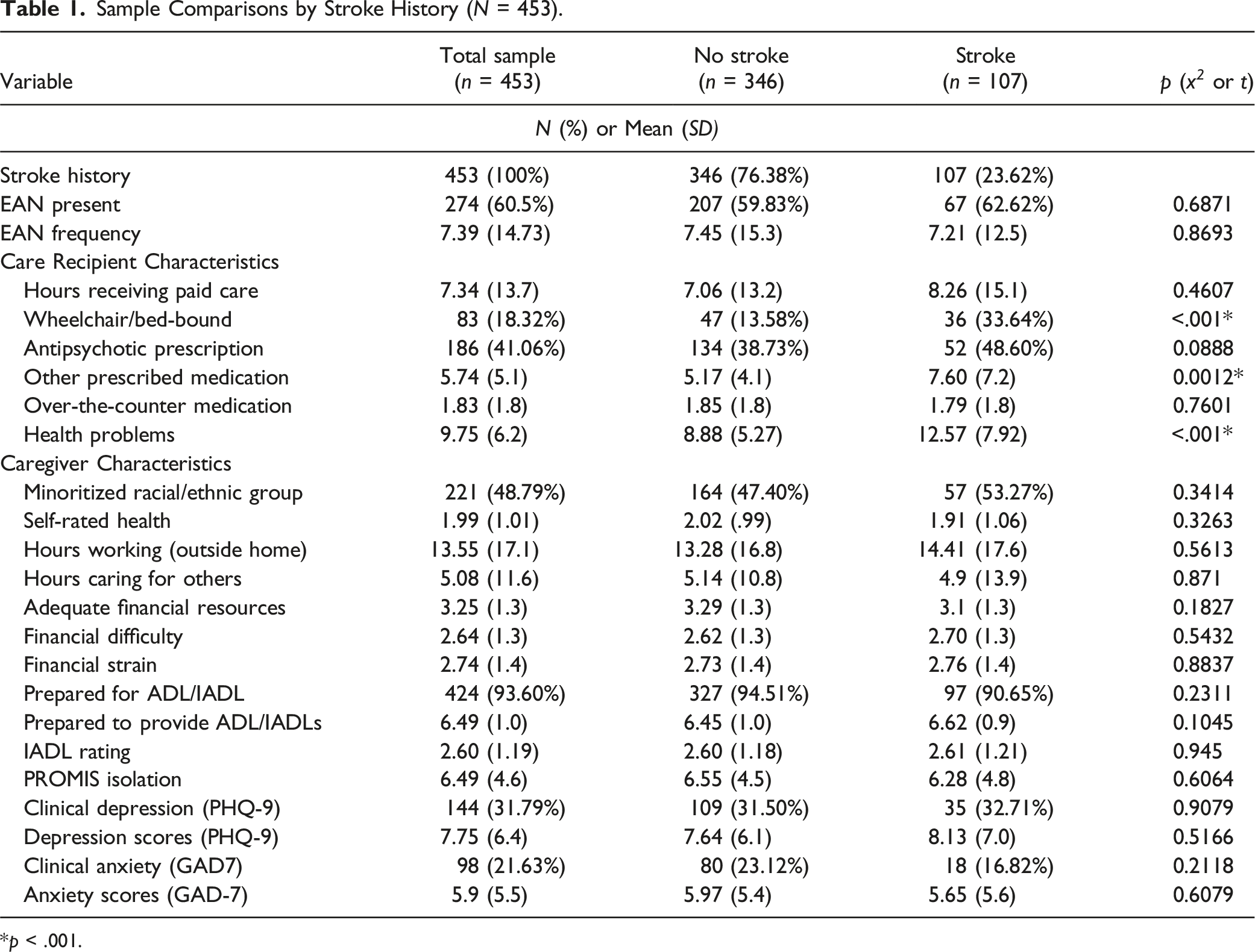
*p < .001.
Associations Between Study Variables and EAN for Stroke Caregivers (N = 107).
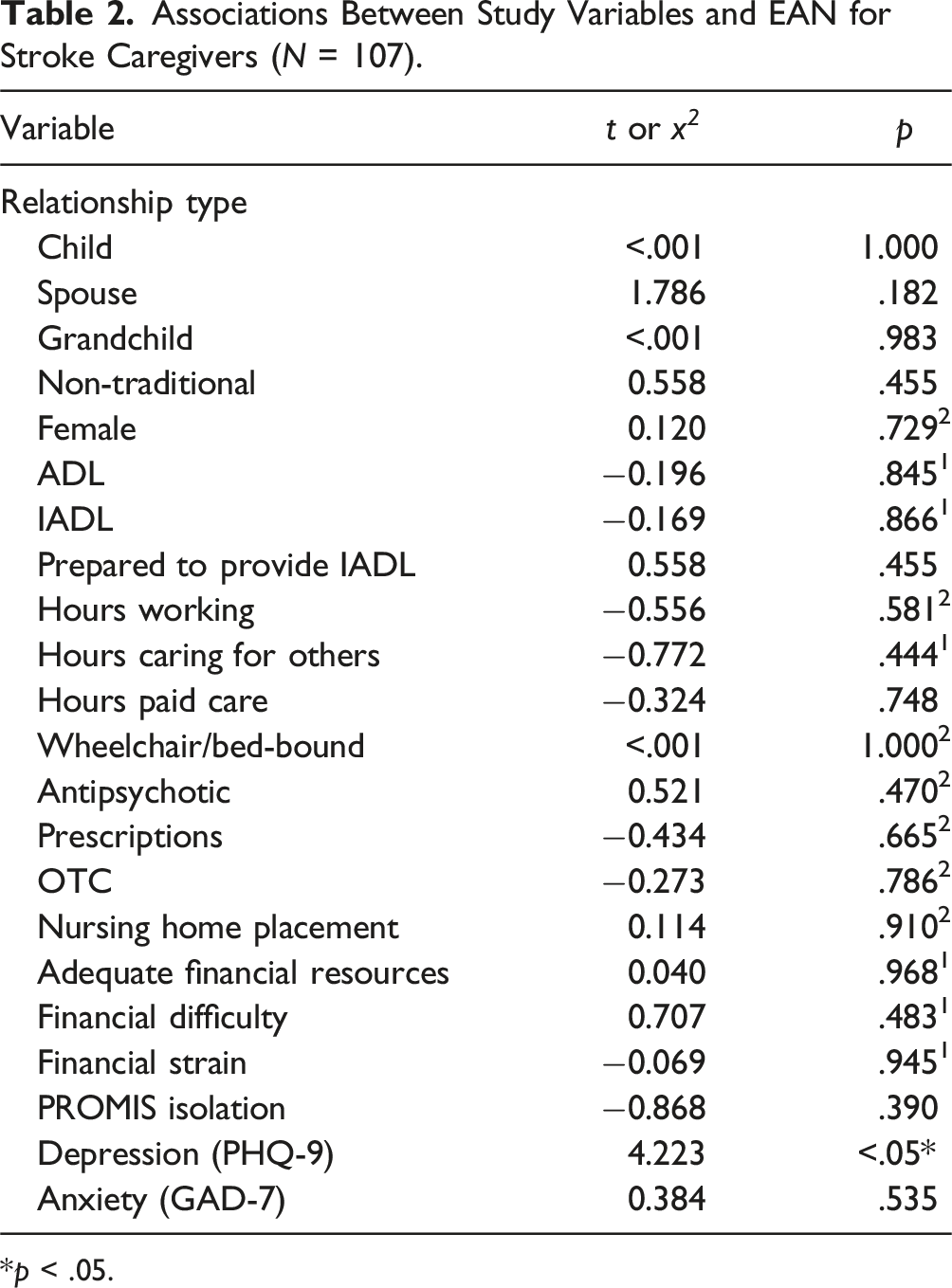
*p < .05.
Discussion
Alzheimer’s disease and related dementia (ADRD) patients are equally affected by EAN, regardless of stroke history. These findings align with a meta-analysis reporting that among those with neurological conditions, stroke was a stronger risk marker for elder mistreatment than dementia or Alzheimer’s disease (Wong et al., 2022). It is possible that drawing our sample from a larger population of ADRD caregivers has a confounding effect. The original study did not collect information about stroke incidence relative to dementia diagnosis; thus, we cannot discern where EAN occurs along the stroke trajectory. Subsequent work examining its prevalence among a general population of stroke survivors without ADRD may elucidate patterns of frequency over the long-term trajectory of stroke management and identify stroke-specific risk profiles for EAN.
Consistent with the established relationship between EAN risk and depression (Beach et al., 2005), we found that stroke caregiver depression was significantly associated with EAN. As many as 20–50% of stroke caregivers experience depression after their loved one’s stroke (Kruithof et al., 2016); while others note that caregivers’ rates of depression exceed that of stroke survivors themselves (Berg et al., 2005). Our analysis could not determine whether caregivers’ depression is due to the effect of stroke, ADRD, or some combination of the two. Supporting stroke caregivers’ mental health is a critical target for mitigating EAN and enhancing caregivers’ abilities to provide long-term care.
Chronic stroke is associated with comorbidities such as heart disease, hypertension, diabetes, chronic obstructive pulmonary disease, and mood disorders (Carriere et al., 2020; Gallacher et al., 2019). That stroke survivors had more multi-morbidities, polypharmacy, and required a greater assistance with ADLs than non-stroke, highlights the additive toll that chronic illness management and treatment burden exert on caregivers. Future work should examine the role of stroke treatment burden upon caregiving outcomes such as caregiver depression and EAN.
Conclusion
EAN is relatively understudied in the context of stroke. This study advances the knowledge on the intersection of stroke care and EAN by providing initial descriptions of EAN prevalence amongst those with stroke, and EAN-related stroke survivor and caregiver characteristics. Identifying critical timepoints in the stroke recovery period where survivors and caregivers are most vulnerable to EAN will assist clinicians in screening and identifying those who are likely to benefit from added support or intervention. Targeted prevention strategies may improve physical and mental health for stroke survivors and their caregivers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the NIH/NIA (R01AG060083).