
Abstract
Current research on technophobia and readiness to adopt new technology in the aging population is often limited to the context of specific technologies and treat
• Unlike previous research, our study explores technophobia as a multidimensional construct and in the general context. • Technophobia is explored as a mediating mechanism between stable demographic characteristics and readiness to adopt new technologies among aging adults.
• Older and less educated individuals are particularly hesitant to adopt new technologies supporting their well-being and should be prioritized in the efforts to increase technology adoption. • Efforts to increase new technology adoption should involve setting realistic expectations and presenting new technology as something that facilitates access and complements human services instead of replacing them.What this paper adds
Applications of study findings
Introduction
Population aging is one of the key global issues faced by today’s society; according to World Health Organization (2022), the share of the population aged 60 years or more will increase from 1 billion in 2020 to 1.4 billion in 2030 and more than 2 billion in 2050, resulting in complex socio-cultural, psychological, economic, and public health challenges (Sander et al., 2015). Previous research suggests some of the adverse effects of this demographic shift could be mitigated by promoting “ageing well,” which is often characterized by prolonged independent living in the community, good self-assessed health, and psychological well-being (Fornara et al., 2019; Kendig et al., 2014). Due to recent technological advances (e.g., developments related to ambient assisted living and availability of various internet-based solutions), these endeavors can now be supported by new technology (Barbosa Neves et al., 2019; Blackman et al., 2016; Forsman & Nordmyr, 2017; Zager Kocjan et al., 2022). However, according to the meta-analysis by Hauk et al. (2018), the adoption of technologies designed to support aging adults is relatively low and negatively correlated with age.
While low adoption can partly be attributed to technology-related factors (e.g., not involving aging adults in the design process; Sayago, 2019), individual-related variables from models such as the extended unified theory of acceptance and use of technology (Venkatesh et al., 2012) and the model of technology adoption by older adults (Wang et al., 2017) are also at play. One such variable is technophobia (also known as technology anxiety), generally defined as “aversion or anxiety toward technologies and technology-related products” (Sinkovics et al., 2002, pp. 478) or “irrational fear and/or anxiety that individuals form as a response to a new stimulus that comes in the form of a technology” (Khasawneh, 2018b, pp. 48). It has been found to be negatively associated with readiness to adopt new technology or adoption of new technology in both general samples (Khasawneh, 2018a; Tsai et al., 2019) and samples consisting of aging adults (Hoque & Sorwar, 2017; Pal, Funilkul, Charoenkitkarn, & Kanthamanon, 2018). Moreover, studies show that aging adults tend to exhibit higher levels of technophobia than younger age groups (Powell, 2013; Xi et al., 2022), although it is worth noting that both technophobia and technology adoption also vary within this target group, with certain demographic cohorts being particularly hesitant to use new technology (e.g., Nimrod, 2018).
In the present study, we investigate the role of gender, age, education, and various aspects of technophobia in determining Slovenian aging adults’ readiness to adopt new technology in general and, in particular, in the health domain, which has previously been identified as the most important life domain for Slovenian aging adults (Musil et al., in press; Smrke et al., 2022). We also aim to explore whether aspects of technophobia mediate the relationship between demographic variables and readiness to adopt new technology.
By doing this, we will advance the existing literature and address several important gaps. First, while some studies focusing on technophobia among aging adults exist, they are scarce and primarily limited to Western, English-speaking samples. Our study will add to the body of knowledge by exploring these concepts within the country that is aging faster than the European Union average and is already experiencing the effects of aging on healthcare capacities, economic competitiveness, and several related issues (INAK, 2020). Second, as noted by Khasawneh (2018a), technophobia is still often explored in the context of specific technology, mainly computers, whereas much less is known about general technophobia. Our study takes that into consideration and studies technophobia independently of specific products, thus providing a more holistic understanding and findings that can be easily transferred across different technologies. Third, while technophobia was found not to be a one-dimensional concept, but is rather comprised of several different factors (e.g., Khasawneh, 2018b), and several authors have pointed out that technophobia needs to be treated as a multidimensional concept (e.g., Khasawneh, 2018b; Martínez-Córcoles et al., 2017), studies often neglect this complexity and instead employ unidimensional (self-construed) scales. In the present study, we employ a more nuanced approach to understanding technophobia and aim to pinpoint specific technology-related fears and concerns. Lastly, to our knowledge, no study has investigated technophobia (i.e., a malleable variable that can be addressed with interventions; Brosnan & Thorpe, 2006) as a mediator between stable demographic characteristics and readiness to adopt new technology among aging adults. This is one of the key aims of our study, oriented towards unraveling mechanisms through which stable demographic characteristics influence readiness to adopt new technology. Altogether, our study’s findings could provide a novel insight into variables associated with aging adults’ readiness to adopt new technology and inform future interventions designed to improve the adoption of technology capable of enhancing aging adults’ quality of life.
Theoretical Background and Hypotheses
Even though technology use among aging adults has increased substantially in the last decade, reflected in the increased share of those owning a smartphone and using the internet (Faverio, 2022), there is a major digital divide present in this population (Kim et al., 2023). Technophobia has been proposed as one of the main factors explaining this divide (e.g., Czaja et al., 2006; Dogruel et al., 2015; Soja & Soja, 2015), while also being disproportionally pronounced in this age group compared to younger cohorts, resulting in generally the lowest adoption of various technologies in the population of aging adults (Hauk et al., 2018). Predictors of technophobia have already been studied, often exploring the roles of gender, age, education, and socioeconomic status (Hill et al., 2015), while the link to the actual readiness to adopt new technologies has been neglected.
Some studies (e.g., Xie, 2008) suggest that women in the aging adult population exhibit higher levels of technophobia compared to men. This could be at least partially explained by socialization and traditional gender roles that discourage women’s involvement in technology-related activities (Czaja & Lee, 2007). Moreover, aging men are, in general, more exposed to technology through work, increasing their familiarity with technology (Chiu & Liu, 2018). While some studies conducted among aging adults did not find any significant differences between men and women in technology adoption (e.g., Czaja et al., 2006), other studies suggest that women might perceive themselves as less capable of using technology due to societal norms or stereotypes, potentially decreasing their readiness to adopt new technology (Nayak et al., 2010; Xie, 2008). Therefore, we propose that women will exhibit higher levels of technophobia compared to men (Hypothesis (H) 1a) and lower readiness to adopt new technology (H1b).
While the population of aging adults generally demonstrates higher levels of technophobia and lower adoption of new technologies than younger generations (Hauk et al., 2018), age-related differences have also been found within this age group, indicating that the oldest age groups might exhibit even higher levels of technophobia (Czaja et al., 2006). Generational differences may play an important role since older generations have not been exposed to technology for most of their lives, contributing to their lower familiarity with it and greater technophobia (Xie, 2008). Another important factor can be found in age-related cognitive declines, posing additional challenges in learning and using new technologies (Mitzner et al., 2008). In line with these findings, the oldest age groups might also exhibit higher levels of reluctance to adopt new technologies (Czaja et al., 2006). We propose that age will be positively related to greater levels of technophobia (H2a) and lower readiness to adopt new technology (H2b).
Previous studies exploring the relationship between educational level and the central constructs of this study have consistently found that higher levels of education often lead to greater familiarity with technology and greater digital literacy (Czaja et al., 2006). Higher educational attainment is also linked with greater specific cognitive skills (Ritchie et al., 2015) and lifelong learning, fostering a more adaptive, open, and favorable attitude towards the adoption of technology on the one hand and decreasing the presence of technophobia on the other hand (see also Gatto & Tak, 2008; Hill et al., 2015). In the present study, we propose that higher educational levels will be linked to lower levels of technophobia (H3a) and higher readiness to adopt new technology (H3b).
Another variable important in explaining the attitudes toward new technology is socioeconomic status (SES). As it influences access to technology (i.e., individuals with higher SES have more opportunities to obtain and maintain technological devices), it can impact the levels of technophobia experienced and the likeliness to adopt new technologies (Gatto & Tak, 2008; Mitzner et al., 2008). Therefore, we expect that higher SES will be related to lower levels of technophobia (H4a) and higher readiness to adopt new technology (H4b).
In the present study, we will also explore the link between technophobia and readiness to adopt new technologies. Existing research states that technophobia can hinder both readiness and actual adoption of new technologies in the aging adult population (Czaja & Lee, 2007; Hoque & Sorwar, 2017; Pal, Funilkul, Vanijja, & Papasratorn, 2018). Therefore, we expect that higher levels of technophobia will be negatively related to the readiness to adopt new technology (H5).
Methods
Participants
Whereas 279 home-dwelling aging adults at least partly filled out our questionnaire, we excluded participants who did not respond to the demographic questions and those with more than 20% of missing values within any of the key questionnaires. Follow-up analyses showed that the included and excluded participants with available demographic data did not differ in gender (χ2(1) = 4.16, p = .057), age (t(256) = 1.07, p = .287), education (t(261) = −1.13, p = .258) nor socioeconomic status (t(249) = −1.77, p = .078).
Our final sample comprised 198 home-dwelling aging adults, the majority of whom were female (f = 147; 74.2%). Their age ranged from 65 to 95 years, with an average of 73.18 (SD = 5.81). The participants exhibited a relatively high level of education, with 92 individuals having completed some form of tertiary education (46.5%), 85 participants having completed some form of secondary education (42.9%), 19 participants having completed primary education (9.6%), while only two participants did not complete primary education (1.0%). Most participants reported being able to cover all necessary expenses with some surplus for other expenses (f = 174; 87.9%).
Approximately half of the participants (f = 97; 49.7%) resided in urban areas, while the remaining participants lived either in rural areas (f = 67; 34.4%) or in suburban areas (f = 31; 15.9%). Most of them lived with others, such as a partner, children, or other relatives (f = 114; 57.6%), whereas the rest lived alone (f = 84; 42.4%). Most participants did not receive any formal or informal assistance at the time of the study (f = 139; 71.3%).
Measures
During the survey, we obtained various demographic data, such as gender, age, education level, and socioeconomic status, and data about the living situation of participants, such as the type of dwelling environment (urban, suburban, rural area), whether they lived alone or with others, and whether they were receiving any assistance in their daily life.
Technophobia was measured with the Technophobia scale (Dogruel et al., 2015; Sinkovics et al., 2002), initially developed to assess the fear of using ATMs but later adapted for other contexts. For the present study, items were reformulated to refer more generally to the new technology. Participants responded to the 13 items via a five-point scale from 1 (»I do not agree at all«) to 5 (»Strongly agree«). The scale consists of three dimensions, that is, »personal failure«, referring to the fear of not being able to deal with technology (e.g., »I feel some anxiety when I approach new technology.«, six items), »human-machine ambiguity « referring to the preference of human versus ICT-based contact (e.g., »I prefer to have people providing me help rather than using new technology.«, four items), and »convenience« referring to the convenience of technology use (e.g., »New technology makes life easier.«, three items). All three dimensions were scored so that higher values reflect more negative attitudes towards technology.
Readiness to adopt new technology was measured with one subscale of a questionnaire developed for a broader study on the needs and preferences of aging adults regarding the use of supportive technology in their daily life (Musil et al., in press). The questionnaire entails seven areas of instrumental activities of daily living (i.e., finances, social and leisure activities, communication, health, mobility, home care, and nutrition), for which participants indicate how important each area is for them, to what extent they need help, and how willing they are to use new technology in each area (Musil et al., in press). Only the items on readiness to adopt new technology were used in the present study, that is, participants indicated how willing they are to use new technology in each of the seven aforementioned areas (e.g., “I would be willing to use new technology in the area of health”) on a five-point scale from 1 (“Completely disagree”) to 5 (“Completely agree”). The average score on these items represents readiness to use new technology in general, and the answer to the health domain items represents readiness to use new health technology.
Procedure
Data were collected between April and December 2022 among home-dwelling aging adults in Slovenia. In order to obtain a diverse sample, participants were approached via three channels: (1) an invitation with a link to the online questionnaire was distributed by one of the Slovenian mobile companies (n = 41, 20.7% of the final sample), (2) similar invitation was shared by various organizations and societies for aging individuals among the users of their services (n = 42, 21.2%), and (3) paper-pencil format of questionnaires was distributed to participants in group meetings of organizations and societies for aging adults, and with the help of institutions providing in-home care (n = 115, 58.1%). Additional analyses revealed that the three subsamples differed in their demographic variables and the studied outcomes, with the last, paper-pencil group, generally being the oldest, least educated, most technophobic, and most hesitant to use new technology (for detailed results, see Table S1 in Supplementary materials).
Before filling out the questionnaire battery, participants were informed about the study and their rights as participants. Those who agreed to participate signed an informed consent (or indicated their agreement in the online version). Participants required 15–20 minutes to fill out the questionnaires. After completion, as an incentive to participate, they were offered an option to participate in a raffle to win one of the three smartphones. The research procedure was approved by the Institutional Research Ethics Committee of Faculty of Arts, University of Maribor (approval no. 038-26-116/2022/5/FFUM).
Statistical Analysis
We initially cleaned the data and conducted the missing value analysis. Participants with missing data that cannot be imputed (i.e., demographic information) and those with too many missing points within a given questionnaire (i.e., more than 20.0% of empty cells) were excluded from further analyses. The remaining missing data were imputed using the expectation-maximization algorithm. We then calculated descriptive statistics and bivariate associations between the variables.
We employed partial least squares structural equation modeling (PLS-SEM) for our main analyses. PLS-SEM is a non-parametric alternative to covariance-based structural equation modeling (CB-SEM) that is less focused on goodness-of-fit and uses bootstrapping to determine statistical significance. While both methods are equally effective for analyzing the structural relationships (Dash & Paul, 2021), the use of PLS-SEM is advised for prediction-oriented research that includes complex models with multiple constructs, indicator variables, and structural paths, which is the case in our study. Moreover, compared to CB-SEM, PLS-SEM is more suitable for situations when a small population restricts the sample size, as is the case in our study, in which the number of participants is below the minimum sample size for CB-SEM (Hair et al., 2019; Willaby et al., 2015).
Following the recommended procedure for PLS-SEM outlined by Hair and colleagues (2019), we first examined the measurement models. Specifically, we investigated the indicator loadings (loadings above .50 were considered acceptable; Chin, 1998), internal consistency reliability (composite reliability (CR) between .70 and .95 indicated good reliability; Hair et al., 2019), convergent validity of each construct measure (average variance extracted (AVE) above .50 was considered acceptable; Hair et al., 2019), and discriminant validity (heterotrait-monotrait ratio (HTMT) below .90 was considered acceptable; Hair et al., 2019; Henseler et al., 2015). As no major issues were identified, we proceeded with the assessment of the structural models using standard criteria, such as the coefficient of determination (R2) and the statistical significance of the path coefficients (using bootstrapping). Throughout the result section, we report standardized coefficients. Since we conducted two separate analyses (i.e., predictors of readiness to adopt new technology in general and in a specific sub-domain, namely, health), the significance level was adjusted from conventional .050 to .025. The analyses were conducted using the SmartPLS 4 software (Hair et al., 2019; Ringle et al., 2022).
Results
Preliminary Analyses
Descriptive Statistics and Reliability and Validity Analysis.
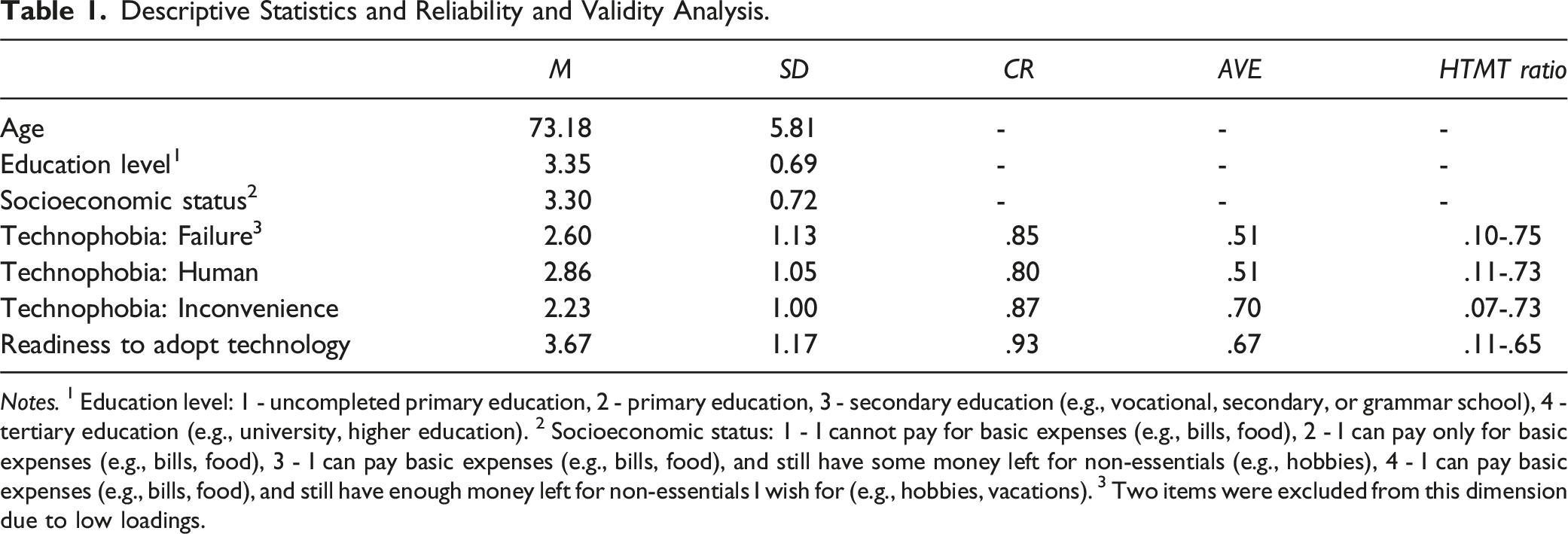
Notes. 1 Education level: 1 - uncompleted primary education, 2 - primary education, 3 - secondary education (e.g., vocational, secondary, or grammar school), 4 - tertiary education (e.g., university, higher education). 2 Socioeconomic status: 1 - I cannot pay for basic expenses (e.g., bills, food), 2 - I can pay only for basic expenses (e.g., bills, food), 3 - I can pay basic expenses (e.g., bills, food), and still have some money left for non-essentials (e.g., hobbies), 4 - I can pay basic expenses (e.g., bills, food), and still have enough money left for non-essentials I wish for (e.g., hobbies, vacations). 3 Two items were excluded from this dimension due to low loadings.
The latent variables were additionally analyzed in terms of their reflective measurement models. First, we examined the indicator loadings and identified two personal failure (technophobia) items with loadings below .50, which were subsequently excluded from analyses (see Table S3 in Supplementary materials). Next, we assessed internal consistency using composite reliability, with results suggesting good to great internal consistency. Furthermore, we evaluated the convergent validity of each latent variable by calculating the average variance extracted, with results demonstrating acceptable convergent validity. Lastly, discriminant validity was assessed using the heterotrait-monotrait ratio, with all the calculated values being below the critical threshold.
Correlations Between the Variables.
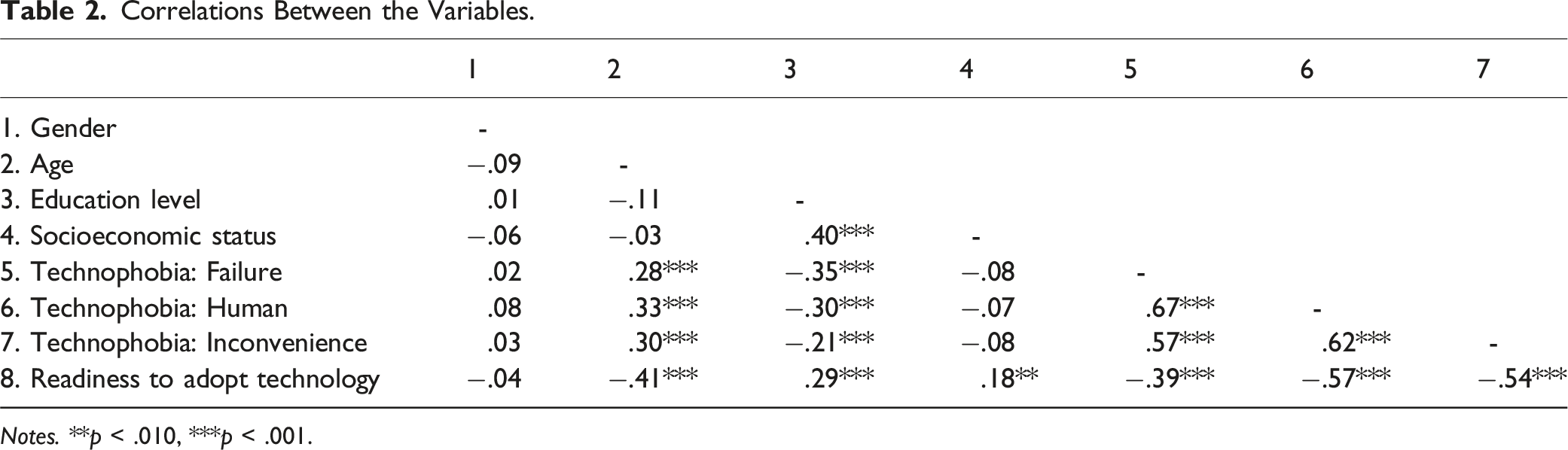
Notes. **p < .010, ***p < .001.
Assessing the Structural Model
In the next step, we examined our hypotheses with a structural model incorporating gender, age, education level, and socioeconomic status as predictors of technophobia and readiness to adopt new technology. Additionally, technophobia was included as a predictor of readiness to adopt new technology. The main findings are depicted in Figure 1, while detailed results for all paths can be found in the Supplementary materials (Table S5). Structural model results.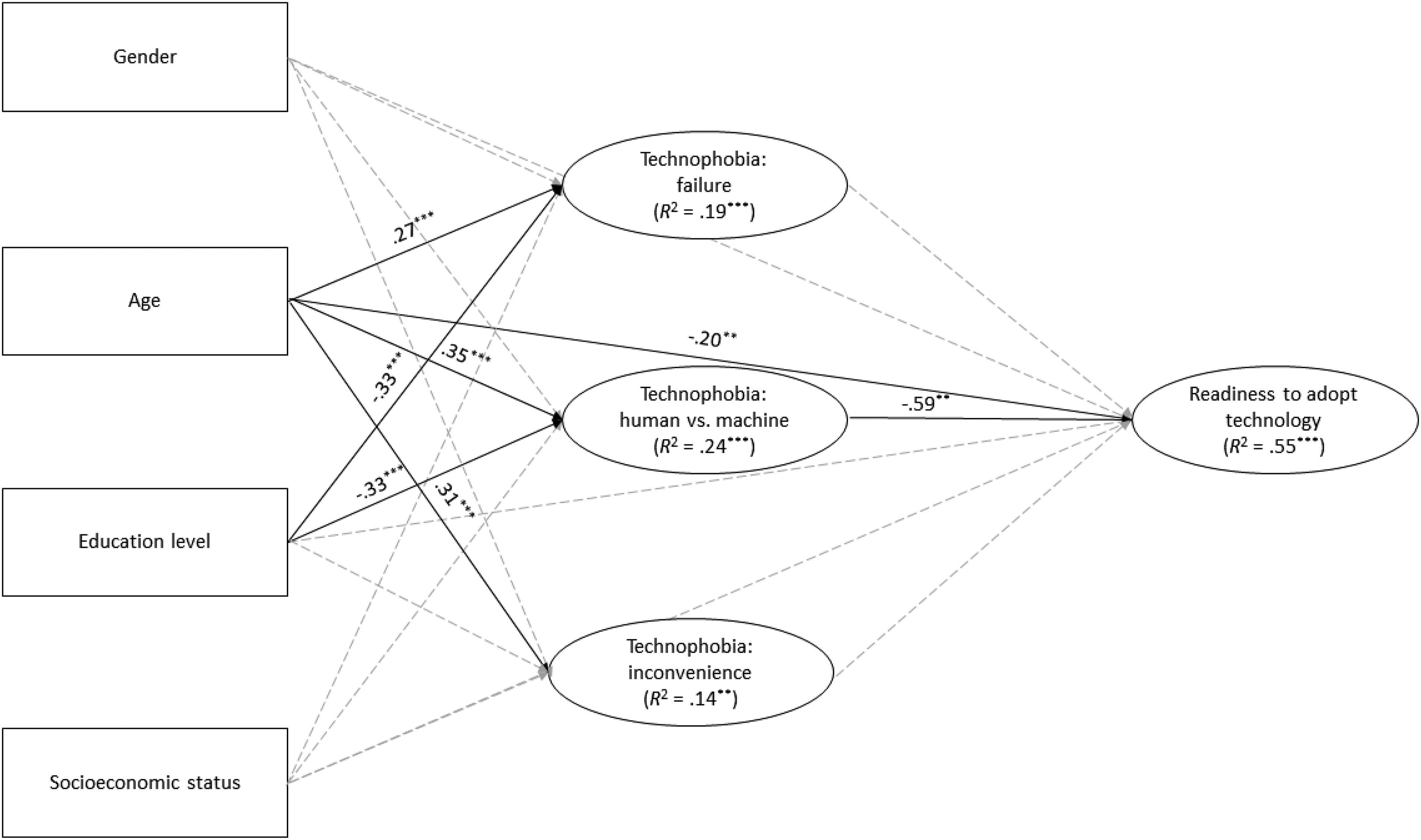
As shown in Figure 1, age exhibited a significant and positive association with all three aspects of technophobia while being significantly and negatively associated with readiness to adopt new technology. Education level significantly and negatively predicted the failure and human versus machine dimensions of technophobia, but it did not predict the inconvenience dimension of technophobia nor exert a direct effect on readiness to adopt new technology. Gender and socioeconomic status, on the other hand, did not display significant associations with the other variables in the structural model.
Furthermore, human versus machine ambiguity, but not personal failure and inconvenience, significantly predicted readiness to adopt new technology. Interestingly, human versus machine ambiguity and inconvenience exhibited a negative association, whereas personal failure exhibited a moderate, albeit non-significant, positive association with readiness to adopt new technology (the latter is likely a statistical artefact, which is explained in more detail in the discussion section).
The selected variables explained 14.0%–24.0% of the variance in different aspects of technophobia and approximately 55.0% of the variance in readiness to adopt new technology. Similar results were obtained when treating technophobia as a unidimensional construct; age (β = .34, p < .001) and education level (β = −.32, p < .001) significantly predicted technophobia. Additionally, age (β = −.24, p < .001) and technophobia (β = −.50, p < .001) significantly predicted readiness to adopt new technology.
Similar results were obtained when predicting specifically readiness to adopt new technology in the health domain. Age was found to have a significant and positive association with all aspects of technophobia (failure: β = .27, p < .001; human versus machine ambiguity: β = .35, p < .001; inconvenience: β = .31, p < .001). Education level demonstrated a significant and negative association with failure and human versus machine dimensions of technophobia, but not inconvenience (failure: β = −.34, p < .001; human versus machine ambiguity: β = −.33, p < .001; inconvenience: β = −.19, p = .033). Lastly, personal failure (β = .40, p = .020) and human versus machine ambiguity (β = −.66, p = .005) predicted readiness to adopt new technology. In this structural model, we did not observe any direct effects of demographic variables on readiness to adopt new technology. A comprehensive overview of the results regarding the structural model for predicting readiness to adopt new health technology can be found in the Supplementary materials (Table S6).
Indirect Effects
Indirect effects: Age, Education Level, Technophobia, and Readiness to Adopt New Technology.
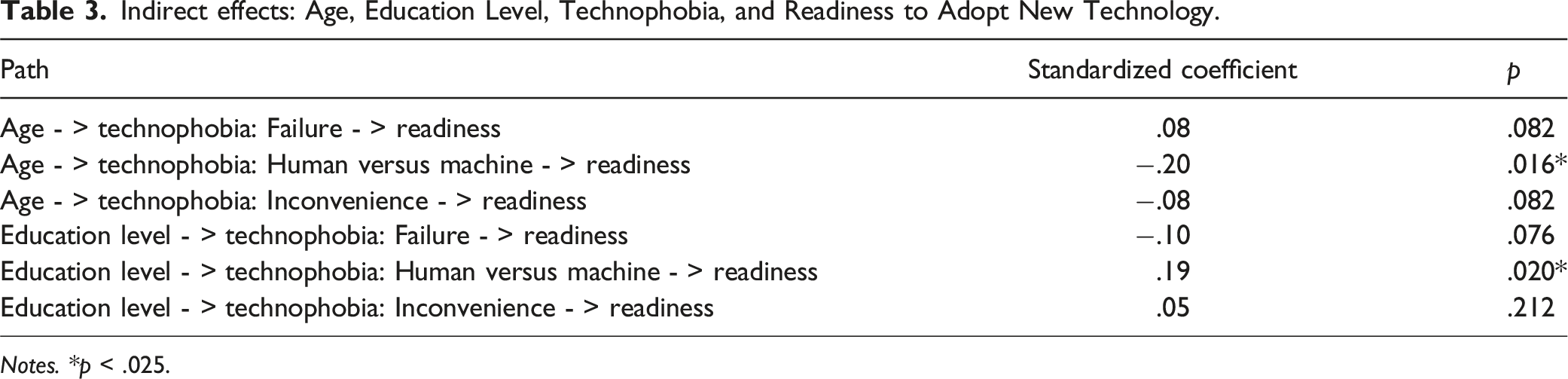
Notes. *p < .025.
Discussion and Conclusions
In the present study, we aimed to investigate the role of various demographic variables and aspects of technophobia in predicting readiness to adopt new technology in general and in the health domain, and to investigate the potential role of technophobia as a linking mechanism among the central variables in the sample of Slovenian aging adults. As such, our study adds to the body of knowledge aimed at exploring the relationship between aging adults’ perception and adoption of technologies that could potentially support their well-being. Specifically, our study contributes to existing research by investigating general technophobia (i.e., not tied to a specific technology; Khasawneh, 2018a), exploring technophobia as a multidimensional construct (Khasawneh, 2018b; Martínez-Córcoles et al., 2017), collecting data outside of Western, English-speaking environments, and, most importantly, exploring technophobia as a mediating mechanism between demographic characteristics and readiness to adopt new technologies among aging adults.
In our study, age and educational level were significant predictors of technophobia, apart from the association between education level and inconvenience. Moreover, both variables exhibited significant indirect effects on readiness to adopt new technology via the human versus machine ambiguity dimension of technophobia. Lastly, age and the human versus machine ambiguity dimension of technophobia were direct negative predictors of readiness to adopt new technology. Both general and health context models exhibited similar relations among central variables, with only minor discrepancies.
Age-related differences in technophobia among aging adults, already reported in previous research (Czaja et al., 2006), also emerged in our models; age positively predicted all aspects of technophobia, while it negatively predicted readiness to adopt new technology in the general context model, but not in the health context model. This discrepancy between the models could be explained by the fact that our sample of Slovenian aging adults expressed the lowest quality of life in the health domain and, at the same time, evaluated health as the most important domain among those assessed (Musil et al., in press). Inferring that these results point to a high perceived health risk, our results can be explained in the context of the Health belief model (Champion & Skinner, 2008; Rosenstock, 1974). Specifically, higher perceived health risk is linked to a greater motivation to engage in health-promoting behavior (e.g., Ahadzadeh et al., 2015), in our case, to potentially overcoming the effects of technophobia and adopting new technology in the health domain.
In line with our hypotheses and previous studies (Czaja et al., 2006; Gatto & Tak, 2008; Hill et al., 2015), educational level was significantly negatively associated with two out of the three aspects of technophobia in the general and health context model, but no direct effects were found on readiness to adopt new technology. However, we found an indirect positive effect of education level on general readiness to adopt new technology via the human versus machine ambiguity aspect of technophobia. The relationship also held true if technophobia was treated as a unidimensional construct. However, no such association was found specifically in the health sub-domain. This may be due to individual characteristics, such as demographic variables, being a less important factor of technology adoption in contexts where aging adults’ perceived need for support is more pronounced.
While age and education exhibited a significant indirect effect on readiness to adopt new technology via human versus machine ambiguity, this was not true for failure and inconvenience dimensions. Human versus machine ambiguity was the most pronounced and had the strongest negative relationship with readiness to adopt new technology among all three aspects of technophobia. As it encompasses an emotional and probably irrational aspect of technophobia, it could signify that aging adults place a high importance on human contact, especially since loneliness is highly prevalent in this age group (e.g., Bolton & &Dacombe, 2020). On the other hand, more cognitive aspects of technophobia (i.e., failure and convenience) might be less pronounced, especially if aging adults can secure support in these areas, such as informal carers, that might help them mitigate their negative feelings regarding new technology (e.g., Yow et al., 2022).
Lastly, we were interested in the relationship between technophobia and readiness to adopt new technology. Human versus machine ambiguity (i.e., preferring human contact over technology) significantly negatively predicted readiness to adopt new technology in general and health context models as expected, where inconvenience exhibited no significant relationship. Contrary to our expectations, both models showed a positive relationship between the personal failure dimension and readiness to adopt new technology, indicating that a higher fear of being unable to deal with technology is linked to higher readiness to adopt new technology. This association was significant in the health domain, whereas it only approached the significance threshold in the general context. Since previous studies provide convincing support for the opposite relationship (e.g., Czaja & Lee, 2007; Hoque & Sorwar, 2017; Pal, Funilkul, Vanijja, & Papasratorn, 2018), and the association between technophobia as a unidimensional construct and readiness to adopt new technology was negative, the observed positive association might indicate a statistical artefact, such as suppression effect or unobserved heterogeneity in the data obtained (Becker et al., 2013), that would need to be further explored in the future studies.
The main limitation of the present study is a relatively small and homogeneous sample of aging adults, which differs from the general population in aspects such as gender, socioeconomic status, and, most notably, education; while national-level data suggest that about 37% of aging adults finished primary school or less, 50% finished secondary education and 13% tertiary education (Statistični urad Republike Slovenije, 2020), our study contains a much larger share of individuals with tertiary education and lower share of individuals with primary education or less. Due to this sample bias, the results of our study may only partially reflect the state regarding technophobia and readiness to adopt new technology in the broader population. Another thing that makes our findings less generalizable is the possibility that some participants provided socially desirable answers; as experiencing technology-related fears could be seen as irrational or a sign of weakness, some participants may have presented themselves as less technophobic than they are. Lastly, while measuring the general level of readiness to adopt new technology is one of the key contributions of our study, it also has a downside, as it is possible that participants did not have an accurate idea of what new technology in areas such as health actually is. To address these limitations, future research should investigate similar research questions in more diverse (ideally, representative) samples and try to incorporate brief descriptions or demonstrations of recent technological developments in their study design. Additionally, another fruitful area for further work is investigating a broader array of technophobia predictors among aging adults, such as cognitive variables, as well as testing the observed associations using a longitudinal approach.
Despite these limitations, our study has important implications for addressing the low adoption of new technology among aging adults. In particular, our study’s findings illuminate to whom efforts to increase technology adoption should be targeted and what these efforts should entail. First, while various target groups may benefit from interventions promoting the use of new technology, older individuals and, to a lesser degree, less educated individuals within our sample of aging adults are the ones who seem to be most hesitant and should hence be prioritized. Second, as human versus machine ambiguity is the aspect of technophobia that is the strongest predictor of readiness to adopt new technology as well as the aspect that significantly mediates the association between age and education on the one hand and willingness to adopt new technology on the other, efforts to increase adoption of new technology should involve promoting realistic expectations (that might differ from general perceptions) regarding the role of new technology as something that facilitates access and compliments human services instead of replacing them. Such an approach might yield more beneficial outcomes compared to an approach focusing on other dimensions of technophobia (i.e., convenience and personal failure) that were not significant mediators of the association between age and education and readiness to adopt new technology. We argue that fostering good practices related to technology development (e.g., participatory design) and positive attitudes towards technology could pave the way for technology to become a valuable tool supporting aging in place and enhancing the overall quality of life of aging adults.
Supplemental Material
Supplemental Material - Technophobia Mediates the Associations Between Age, Education Level, and Readiness to Adopt New (Health) Technology Among Ageing Adults
Supplemental Material for Technophobia Mediates the Associations Between Age, Education Level, and Readiness to Adopt New (Health) Technology Among Ageing Adults by Urška Smrke, Tanja Špes, Izidor Mlakar, Bojan Musil, and Nejc Plohl in Journal of Applied Gerontology.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Public agency for scientific research and innovation activity of the Republic of Slovenia (Javna agencija za znanstvenoraziskovalno in inovacijsko dejavnost Republike Slovenije), grant number J5-3120.
Institutional Review Board Statement
The research procedure was approved by the Institutional Research Ethics Committee of Faculty of Arts, University of Maribor (approval no. 038-26-116/2022/5/FFUM).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.