
Abstract
Childhood sexual abuse (CSA) is linked to substance use and lower antiretroviral therapy (ART) adherence. However, studies examining the mediational role of substance use between CSA and ART adherence are lacking. Therefore, the aim of this study was to determine the potential mediational role of substance use between CSA and ART adherence among older adults living with HIV (OALH) (n = 91). Mediation analyses assessed the direct and indirect relationships between CSA, substance use, and ART adherence. Statistically significant differences existed in substance use by gender (male vs. female: 12.3 vs. 9.97) and ART adherence by race (Black vs. White: 98.2% vs. 99.6%) and employment. CSA was associated with ART adherence (β = −3.27, p < .001) and substance use (β = 2.14, p = .035), but substance use was not associated with ART adherence, and did not mediate the pathway between CSA and ART adherence in the adjusted model. Trauma-informed interventions may lower substance use among OALH with CSA.
Keywords
• CSA was positively associated with substance use among OALH. • CSA was negatively associated with ART adherence. • Substance use did not mediate the association between CSA and ART adherence among OALH.
• Trauma-informed interventions focusing on CSA may help to lower substance use among OALH. • Screening for CSA among OALH in healthcare settings may identify individuals at risk for substance use. • Future research can determine additional mediators between CSA and ART adherence among OALH (e.g., depression and posttraumatic stress disorder).What this paper adds
Applications of study findings
Introduction
HIV studies on older adults aged 50 and older are becoming increasingly important as the population of people living with HIV (PLWH) in this age group continues to grow due to effective treatment. In 2019, the Centers for Disease Control and Prevention (CDC) estimated that 1.2 million people were living with HIV (PLWH) in the U.S. (CDC, 2022d), and more than half of PLWH in the U.S. are over the age of 50 (National Institute of Aging, 2021). Out of the 36,801 new diagnoses in the same year, people aged 55 and older accounted for 10.5% of new diagnoses, which has been stable since 2015 (CDC, 2022c). In addition, people aged 45 and older accounted for close to one in four new HIV diagnoses (CDC, 2022a). The growing HIV prevalence among older adults living with HIV (OALH) poses specific challenges with treatment and prevention for this population.
OALH are likely to be diagnosed with HIV at a later stage due to HIV symptoms passing off as “older age” and older adults being perceived as outside of the risk group for HIV (Blanco et al., 2010). This late diagnosis may result in OALH having a poorer immunological response to antiretroviral therapy (ART) compared to younger age group populations (Blanco et al., 2010). Other complications, such as comorbid conditions and medications, can also affect the efficacy of ART (Blanco et al., 2010), and the stigma associated with HIV diagnosis often causes OALH to receive less attention from healthcare providers and decreased willingness to accept care (Brown & Adeagbo, 2021). In an ideal situation, PLWH complete the HIV care continuum, reaching 90–95% ART adherence, and achieving viral suppression (Byrd et al., 2019). The HIV care continuum is a series of steps a person living with HIV ideally takes and includes the following: diagnosis, being linked to care, staying engaged in care, receiving and adhering to ART, and attaining viral suppression (US Department of Health and Human Services, 2022). However, the number of PLWH tends to decrease from one step to the next with previous estimates showing that 57% of PLWH were virally suppressed in 2019 (U.S. Department of Health & Human Services, 2022).
Factors such as childhood sexual abuse (CSA) are shown in previous research to be associated with lower ART adherence (Markowitz et al., 2011) and poorer overall quality of life (Draper et al., 2008). CSA is defined as abusive and nonconsensual sexual behavior towards a child (CDC, 2022b). Adverse effects of sexual trauma may include poor psychological and physical health (Harrison et al., 2020) and a higher risk for depression and PTSD (Fergusson et al., 2013). In one study surveying 158 PLWH who were receiving therapy for depression and to improve HIV medication adherence, over 70% of the participants reported a history of CSA before age 16, which is significantly higher than the national estimate of 16%–27% prevalence of CSA (Markowitz et al., 2011). In addition, CSA before age 16 was associated with lower adherence as measured by an electronic pill-cap medication event monitoring system (Markowitz et al., 2011). Among CSA survivors recruited for a 2002–2004 study in New York City, many were not adherent even though they were linked to HIV care (Meade et al., 2009). A qualitative study of eight women in Cape Town found that ART reminded the women of past sexual trauma memories, which may hinder HIV medication engagement and adherence (Watt et al., 2017). For example, taking ART triggered memories of how HIV was acquired for these women (typically through sexual assault), which resulted in self-blame, shame, and impacted their HIV adherence and care. These studies included but did not focus on older adults.
While CSA was found in many studies to be associated with a lower ART adherence rate, research about possible mediating factors between CSA and ART adherence rate is scarce. Potential adverse effects of sexual trauma include drug and alcohol use (Brown et al., 2017; Hines et al., 2023; Shangani et al., 2022). Some research found a high prevalence of substance use among PLWH and people with CSA (Deren et al., 2019; Liu et al., 2006; Lotzin et al., 2019) and as a coping strategy for OALH with a CSA history (Amoatika et al., 2023). Childhood trauma is related to earlier substance use and more severe clinical symptoms such as substance use disorder and posttraumatic stress disorder (Lotzin et al., 2019). Approximately 73% of the women living with HIV and CSA participating in a study reported using hard drugs such as cocaine and heroin, and 45% reported using one type of illicit drug within the past 4 weeks (Liu et al., 2006). OALH have higher rates of substance use than older adults without HIV (Deren et al., 2019), and the additional substance use can interfere with ART pills’ effectiveness because they share several cytochrome enzymes, which reduces enzyme activity (Deren et al., 2019).
The transactional model of stress and coping by Lazarus and Folkman (1984) plays a significant role in helping to understand the impact of trauma on behavioral mediators and outcomes. The first step is primary appraisal (an individual’s perception of a stressor), and this occurs when a person undergoes a specific stressor (e.g., CSA). Secondary appraisal then occurs when the individual makes an evaluation of their abilities (and resources) to deal with the stressor. Coping efforts are then used in response to these stages of appraisal and can be adaptive or maladaptive (e.g., substance use). These coping efforts may be associated with behavioral outcomes (e.g., ART adherence).
Substance use, similarly to CSA, was also shown in studies to be linked to a decrease in ART adherence (Brousseau et al., 2023; Kaswa et al., 2004; Liu et al., 2006; Rosen et al., 2013; Zhang et al., 2018). Marijuana (Zhang et al., 2018), alcohol, cocaine, heroin, and other stimulant use were associated with lower ART adherence (Rosen et al., 2013), but it is unclear if substance use is a mediator between CSA and ART adherence. In addition to examining the prevalence of substance use among PLWH, previous studies focused on the association between CSA, traumatic symptoms, (Lotzin et al., 2019; Watt et al., 2017), and lower medication adherence or higher engagement in risky sexual behaviors. (Markowitz et al., 2011; Meade et al., 2009; Watt et al., 2017). However, these studies analyzed the direct effects between these factors rather than the indirect effect of a mediator variable, such as substance use, between CSA and ART adherence.
Thus, this study aimed to examine the mediating role of substance use between CSA and ART adherence among OALH. We hypothesize that substance use will play a mediating role between CSA and ART adherence. Understanding the relationship between risk factors and ART adherence is crucial for developing intervention programs and improving the overall health of OALH. Specific issues such as substance use relating to ART adherence can be addressed, and healthcare providers can provide better care for OALH.
Methods
Data Source and Study Population
Data were obtained from 91 OALH who were receiving care at an immunology clinic in South Carolina. To be eligible for the study, participants had to be at least 50 years old, living with HIV, and agreed to take part in the survey. Written informed consent was obtained before participating in the study. Data were collected from April to June 2021 via REDCap surveys and paper and pencil questionnaires. Participants were assigned an ID number to ensure confidentiality and compensated with a $40 gift card. The study was approved by the University of South Carolina Institutional Review Board (Pro00104604).
Study Measures
CSA was operationalized using questions from the Early Trauma Inventory-Self Report Form (Bremner et al., 2007). These questions asked whether participants, before age 18, 1) were touched in an intimate/private part of the body; 2) experienced someone rubbing their genitals against them; 3) were forced/coerced to touch another person in an intimate/private part of their body; 4) had genital sex against their will; 5) performed oral sex on someone against their will; and/or 6) were forced/coerced to kiss someone in an affectionate way. Responses were yes versus no. We operationalized CSA as reporting any of these experiences versus not reporting any CSA history. We also examined CSA as the number of multiple forms of CSA experienced.
Substance use was measured using seven substance use-related items from the Substance Abuse and Mental Illness Symptom Screener (SAMISS) (Whetten et al., 2005): 1) frequency of having a drink containing alcohol; 2) number of drinks they have on a typical day when drinking; 3) frequency of having four or more drinks on one occasion; 4) frequency of nonprescription drug use in the past year to get high to change the way they felt; 5) frequency of use of drugs prescribed to them or someone else in the past year to get high or change the way they felt; 6) frequency of drinking or using drugs more than they meant to in the last year; and 7) frequency of feeling that they wanted or needed to cut down on their drinking or drug use in the last year and had not been able to. A Likert-type response scale ranging from 1 or 2 (1) to 10 or more (4) was used for item 2. All other items were scored using a Likert-type response scale ranging from “Never” (1) to “4 or more times a week” (5). For each item, scores were summed to determine an overall substance use sum score. Higher scores reflected greater substance use (Brown et al., 2018).
ART adherence was operationalized using the following phrase and question: Below 0% means you have taken no HIV medications this past month, 50% means you have taken half of your HIV medications this past month, and 100% means you have taken every single dose this past month. What percent of your HIV medications did you take? A visual analog scale was used. This question has been shown to be consistent with viral load data measurements (Walsh et al., 2002).
Potential confounders considered were age, gender, race, employment, and depression. Depression was measured using the Patient Health Questionnaire-9 (PHQ-9) (Kroenke et al., 2001), which has a range from 0 to 27. Previous studies have shown sociodemographic differences in reporting of CSA and ART adherence. For example, there were differences in CSA history reporting by gender, age, employment, and depression status where women, younger individuals, unemployed, and individuals with depression tended to have a higher prevalence of CSA than men, older individuals, employed, and individuals without depression (Brown et al., 2023). In addition, gender, age, and ethnic differences have been found in ART adherence where older, women, and Hispanic individuals reported greater adherence than younger, male, and non-Hispanic individuals (Brown et al., 2019). Previous research has also linked depression to ART adherence, where individuals with depression have lower ART adherence (Brown et al., 2021, 2022; Mireles et al., 2023).
Analytic Approach
Descriptive statistics were used to describe the sociodemographic characteristics of the study population overall, as well as substance use and ART adherence status. Bivariate analysis (linear regression) was conducted to examine the association between CSA and ART adherence. Using bootstrapping confidence intervals, crude and multivariable mediation models adjusting for age (continuous), gender (male vs. female), race (Black vs. White), employment (yes vs. no), and depression (continuous) were used to determine 1) the indirect association between CSA, substance use, and ART adherence; 2) the direct association between CSA and ART adherence; and 3) the direct association between CSA and substance use. The PROC CAUSALMED procedure in SAS was used. Let C denote any included covariate. With using this method, we assume that 1) no unmeasured treatment-outcome confounders given C; 2) no unmeasured mediator-outcome confounders given (C, CSA); 3) no unmeasured treatment-mediator confounders given C; and 4) no mediator-outcome confounder is affected by CSA (directly or indirectly) given C. We also tested the linearity assumption (which was met). We chose this method to determine potential causal mediation effects. Ad hoc analyses were conducted examining the count of multiple forms of CSA in the mediation model. In addition, we also conducted sensitivity tests with individual items of the SAMISS. We also assessed model fit using χ2, Standardized Root Mean Square Residual (SRMR), Comparative Fit Index (CFI), and Goodness of Fit Index (GFI). Guidelines indicate that SRMR< .08, CFI ≥.95, and GFI ≥.95 represent a good fitting model.
Results
Distribution of Sociodemographic Characteristics and Depression Status by Substance Use and ART Adherence.
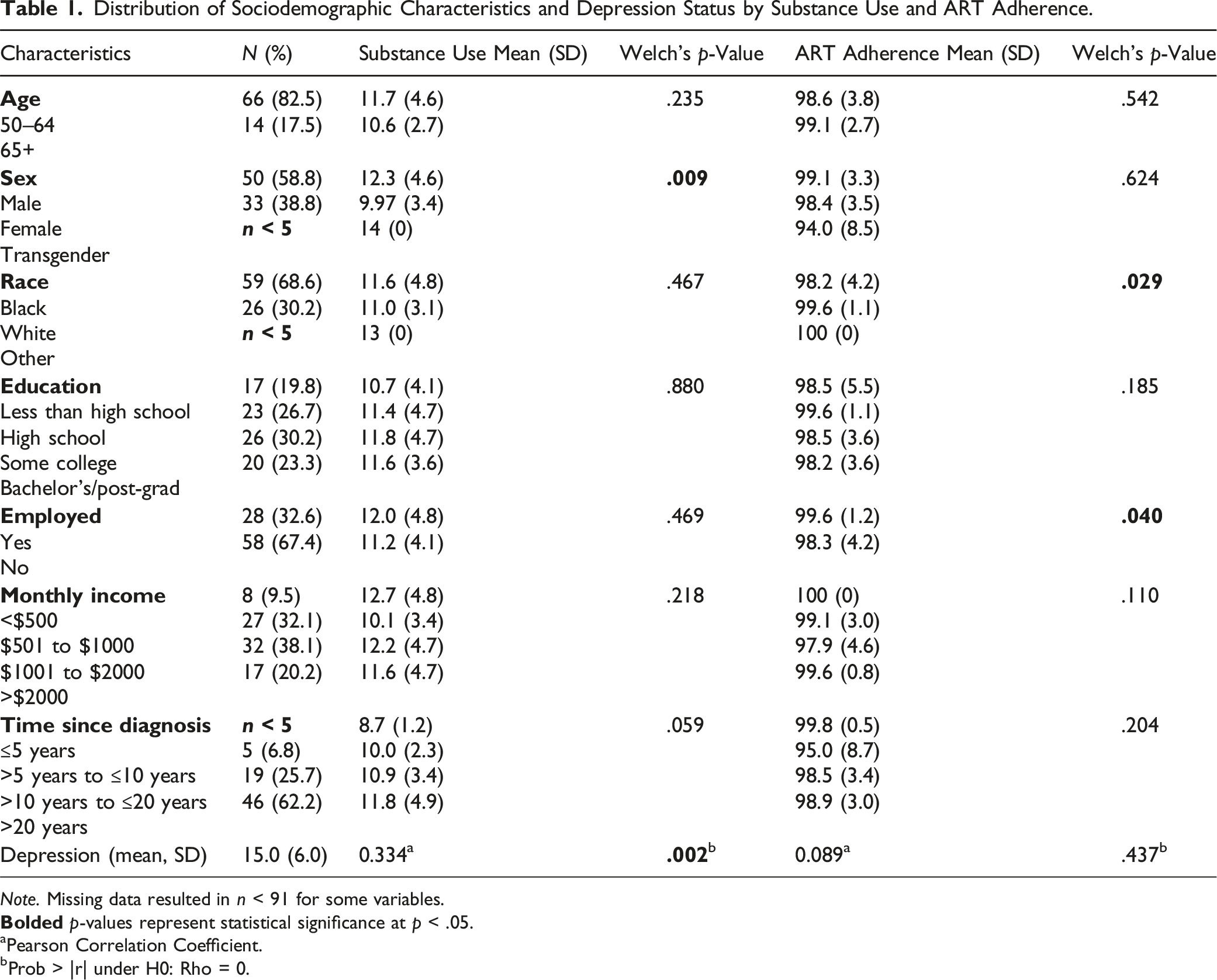
Note. Missing data resulted in n < 91 for some variables.
aPearson Correlation Coefficient.
bProb > |r| under H0: Rho = 0.
Direct and Indirect Associations Between Childhood Sexual Abuse, Substance Use, and ART Adherence.
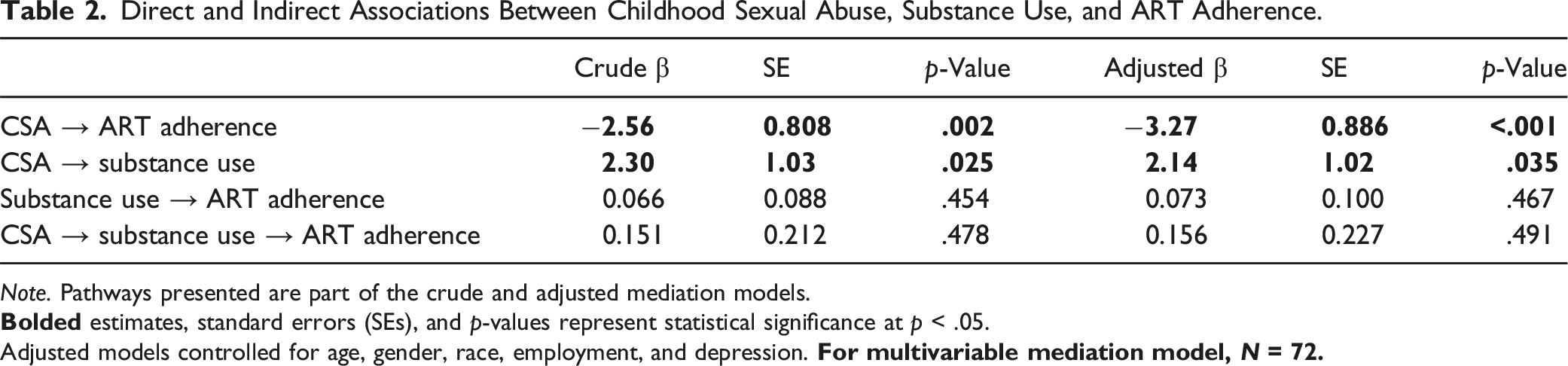
Note. Pathways presented are part of the crude and adjusted mediation models.
Adjusted models controlled for age, gender, race, employment, and depression.
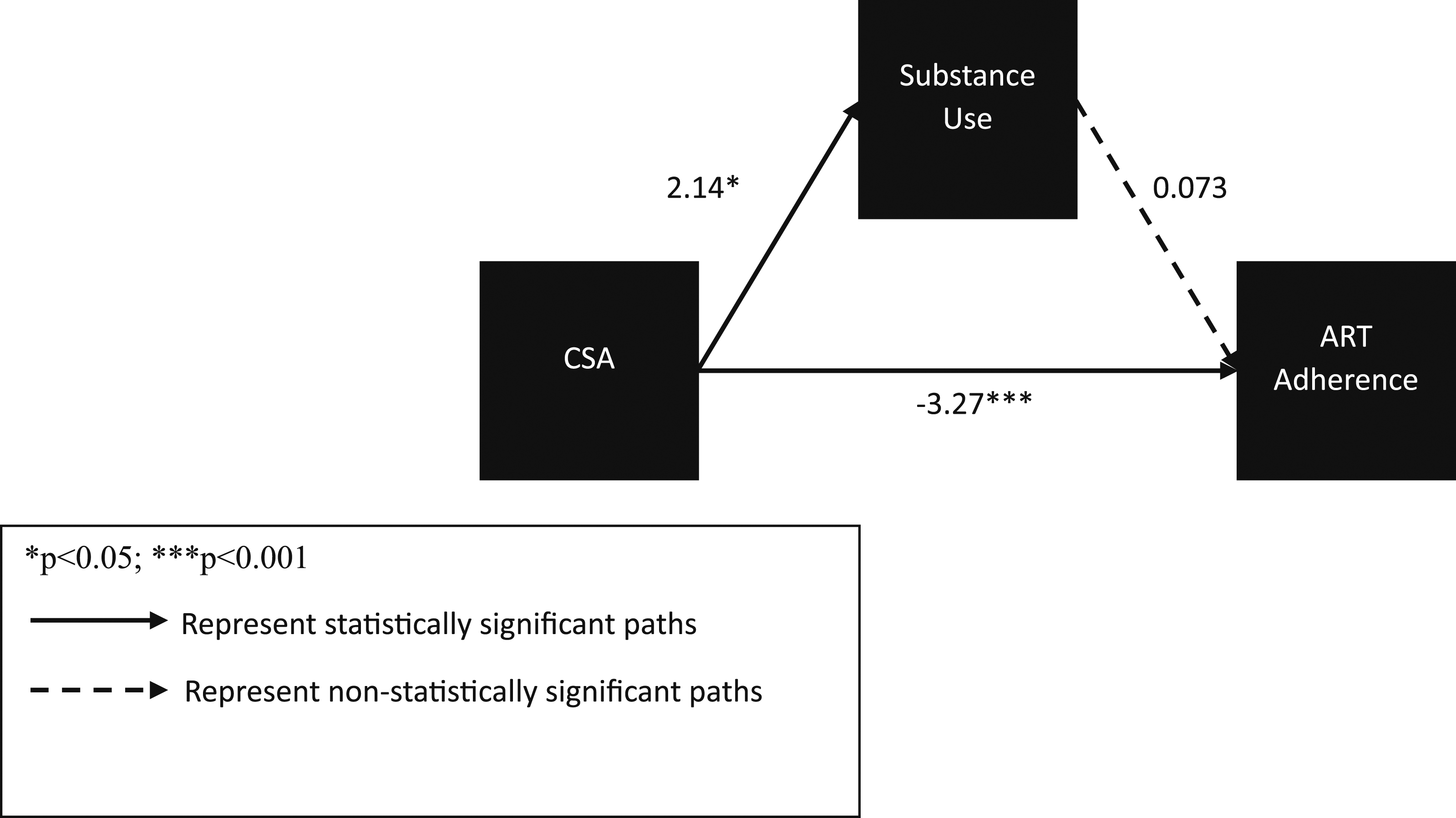
Mediation pathway between childhood sexual abuse, substance use, and ART adherence for adjusted model.
R-squared for the crude model was 0.117. The crude model showed reasonably good model fit according to model fit statistics and indices: χ2(df = 3) = 14.09, p = .003; SRMR = 0.00; CFI = 1.00; GFI = 1.00. R-squared for the adjusted model was 0.221. The adjusted model also showed good model fit: χ2(df = 28) = 69.2, p=<0.001; SRMR = 0.00; CFI = 1.00; GFI = 1.00.
For sensitivity tests for individual SAMISS items for the adjusted models, we did not find any statistically significant indirect effects: frequency of having a drink containing alcohol (β = −0.04, p = .282); 2) number of drinks they have on a typical day when drinking (β = 0.001, p = .960); 3) frequency of having four or more drinks on one occasion (β = 0.030, p = .498); 4) frequency of nonprescription drug use in the past year to get high to change the way they felt (β = 0.083, p = .169); 5) frequency of use of drugs prescribed to them or someone else in the past year to get high or change the way they felt (β = 0.114, p = .103); 6) frequency of drinking or using drugs more than they meant to in the last year (β = −0.010, p = .798); and 7) frequency of feeling that they wanted or needed to cut down on their drinking or drug use in the last year and had not been able to (β = −0.022, p = .643).
Discussion
According to our knowledge, this is the first study to determine the role of substance use as a potential mediator in the association between CSA and ART adherence among OALH in the Southern US. We found that CSA was negatively associated with ART adherence and CSA was positively associated with substance use, and substance use was not associated with ART adherence among this study sample. Therefore, substance use was not a statistically significant mediator between CSA and ART adherence.
Studies have found that CSA is positively associated with substance use as was found in the current study. For example, having a CSA history was associated with early persisting occasional cannabis use in adolescence (Hines et al., 2023). Prior research has found that CSA was also linked to substance use disorders in adulthood (Brown et al., 2017). Research examining the association between CSA and substance use among older adults is lacking. One previous study found that substance use was a coping strategy for OALH who were CSA survivors, before adjustment for confounders (Amoatika et al., 2023).
Previous research has found that substance use is associated with lower ART adherence among varying populations (Brousseau et al., 2023; Kaswa et al., 2004). Brousseau and colleagues found that cannabis use as well as amphetamine/methamphetamine use was associated with lower ART adherence among sexual minority men and transgender women living with HIV in Georgia (Brousseau et al., 2023). In addition, substance use was associated with suboptimal ART adherence among PLWH in the Mthatha region of South Africa (Kaswa et al., 2004). Illicit substance use and nicotine use were associated with lower ART adherence among older sexual minority adults living with HIV in South Florida (Weinstein et al., 2023). Nevertheless, Brousseau et al. (2023) also found that alcohol and cocaine use was not associated with ART adherence.
We did not find a statistically significant association between substance use and ART adherence. The percentage mediated was 6.25%, which suggests that very little of the effect of CSA on ART adherence can be attributed to substance use. The lack of statistical significance between substance use and ART may be due to substance use not affecting ART adherence among this study sample or may be due to the lack of variability in substance use and ART adherence to detect differences. It is possible that substance use disorders (Paschen-Wolff et al., 2020) may impact ART adherence to a greater extent than that measured by the SAMISS. Indeed, our sensitivity analyses did not illustrate statistically significant associations with each SAMISS item. As a result, substance use (as operationalized by the SAMISS) did not mediate the association between CSA and ART adherence in the current study. However, it is possible that cannabis use as well as amphetamine/methamphetamine use may act as mediators between CSA and ART adherence due to their link with lower ART adherence in previous research (Brousseau et al., 2023). These types of specific substance use are not captured by the SAMISS. In addition, while substance use is associated with lower ART adherence in younger populations (Brousseau et al., 2023) and not older populations, it is possible that there is a commitment to taking ART in spite of a traumatic history (Brown et al., 2024) or substance use due to higher levels of resilience among OALH.
The findings suggest important implications for theory, policy, and interventions for OALH. Based on the transactional model of stress and coping by Lazarus and Folkman (1984), interventions addressing primary and secondary appraisals of CSA may impact coping strategies and may reduce substance use. In terms of theory, substance use might not impact ART adherence for OALH and might not be a mechanism through which CSA impacts ART adherence for older adults. Indeed, in the current study, substance use was relatively low and ART adherence levels were high. The findings for this specific study population suggest that while addressing substance use (as operationalized by the SAMISS) might not improve ART adherence, addressing CSA might improve ART adherence. With respect to policy, policymakers should prioritize policies to implement programs addressing a history of CSA for OALH as this approach can reduce substance use and improve adherence to ART. Trauma-informed interventions such as Living in the Face of Trauma (LIFT) (Sikkema et al., 2013) and Improving AIDS Care after Trauma (ImpACT) (Sikkema et al., 2018) are coping interventions and, with their focus on avoidant coping, may help to improve ART adherence among OALH. However, adaptations of these interventions for older adults may need to address additional challenges that these individuals often face such as comorbidities and social isolation. The study results may be applied to trauma-informed intervention programs by addressing a history of CSA, which may then improve ART adherence among OALH. These interventions addressing CSA may also help to reduce substance use among OALH as operationalized by the SAMISS. However, addressing substance use alone may not necessarily impact ART adherence among this study sample.
There are some limitations to be considered in interpreting the results of the study. First, the study participants are in care and therefore findings may not be reflective of OALH who are not in care, who may be more likely to not be adherent to ART. Second, participants in this study also reside in the Southeastern US and findings may also not be reflective of OALH in other geographic regions. Third, the sample size was small. Fourth, the majority of OALH in the current study were aged 50–64 years and findings may not be reflective of adults of older ages. Fifth, we were unable to consider CSA revictimization or frequency, which may also influence substance use and ART adherence to a greater extent.
Nevertheless, there were some strengths. We were able to consider potential confounders in the current study to determine associations controlling for sociodemographic variables and depression status, which may alter the direct and indirect relationships between CSA, substance use, and ART adherence. In addition, we considered a behavioral pathway of ART adherence, which is a crucial step in attaining viral suppression.
Conclusions
Substance use was not found to mediate the association between CSA and ART adherence among OALH living in the Southeastern US. However, CSA was positively associated with substance use and negatively associated with ART adherence among this study population. Future studies should examine the behavioral pathway between CSA, substance use, and ART adherence among older study populations with larger sample sizes. Indeed, the majority of studies focusing on trauma history and ART adherence tend to focus on younger populations. More research needs to focus on factors that can facilitate (or hinder) ART adherence among OALH. Cohort effects may also be present in the associations tested, which we were unable to determine due to the small sample size. Examination of substance use disorders and substance misuse may help to delineate statistically significant pathways among OALH. In addition, examination of the interaction of CSA and substance use may add to the understanding of the potential moderating effect of substance use on CSA. Further exploration of the SAMISS distinguishing between alcohol and drug use as potential mediators can also be assessed in future research. Potential mediators such as cognitive function (Roberts et al., 2022), depression, and posttraumatic stress disorder should also be assessed. Consideration of depression as a potential mediator and accounting for correlations with substance use in multiple mediator models can also be examined. In addition, effect measure modifiers such as social support and medication reminders should also be assessed.
Supplemental Material
Supplemental Material - Childhood Sexual Trauma, Substance Use, and ART Adherence Among Older Adults Living With HIV: A Mediational Analysis
Supplemental Material for Childhood Sexual Trauma, Substance Use, and ART Adherence Among Older Adults Living With HIV: A Mediational Analysis by Monique J. Brown, Josie Zhang, Prince Nii Ossah Addo, Amandeep Kaur, Daniel Amoatika, Elizabeth Crouch, and Steven A. Cohen in Journal of Applied Gerontology.
Footnotes
Acknowledgments
We would like to thank the clinic staff who helped with recruitment and the participants who took part in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute of Mental Health of the National Institutes of Health under Award Number K01MH115794. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.