
Abstract
Many individuals who reside in permanent residential aged care (RAC) have a diagnosis of dementia, with the majority experiencing a communication disorder. Existing literature has placed an emphasis on the need for staff to undertake communication partner training. This study aimed to investigate the preferences of RAC staff, and their perceived barriers and facilitators to workplace training. Through an exploratory cross-sectional online survey, a sample of RAC workers in Australia were recruited (n = 104). Descriptive statistics revealed that the majority of participants preferred training to be delivered face to face and being paid for participation. Through content analysis of open-ended questions, seven categories were identified regarding perceived barriers and facilitators for communication partner training in the workplace. These included staff shortages, time pressures, remuneration and training delivery method, and quality of the educators. Additionally, management attitudes were pertinent. These findings may inform the development and outcomes of future communication partner training in RAC.
• RAC staff and managers see the need for communication partner training to assist people with dementia but time restraints are the main barrier. • Staff-informed data regarding preferences for, and barriers and facilitators to communication partner training, concerning method of delivery, timing and remuneration.
• Consideration of end-user (RAC staff) perspectives may contribute to more successful implementation and outcomes of dementia communication partner training in RAC. • Communication partner training that considers barriers and facilitators may promote and enhance the quality of communication between residents and staff, quality of care provided, and the quality of life for residents with dementia.What this paper adds
Applications of the study findings
Introduction
The prevalence of dementia is rising, with an estimated total of 55 million people currently living with this condition and a further 10 million cases identified annually, worldwide (World Health Organisation, 2022). This global trend is reflected in the prevalence of dementia in permanent residential aged care (RAC). RAC refers to any facility different from a person’s traditional home that is a person’s main residence and provides support for activities of daily living (McCabe et al., 2020). In Australia, there were 183,000 people residing in RAC in 2019 and 53% had been diagnosed with dementia (Australian Government Department of Health, 2021). Many people with dementia have difficulty communicating, which affects their capacity to express needs, wants, and engage in social interactions. RAC staff must have a thorough understanding of the communication needs of residents with dementia, with residents reporting that staff are their primary communication partners (Bennett et al., 2016). Existing research has shown a positive link between the type, quality, and quantity of resident-staff communication/interactions and the quality of life (QoL) for residents with dementia in RAC (Beerens et al., 2016; Kolanowski et al., 2020; Lee et al., 2017; Zimmerman et al., 2005).
The quality of care provided by aged care staff to people with dementia has been flagged by the Royal Commission into Aged Care Quality and Safety (an Australia-wide Government funded enquiry, referred to henceforth “Royal Commission”) as an area of concern. Communication has been specifically highlighted as requiring significant improvement (Royal Commission into Aged Care Quality and Safety, 2021). Consequently, the Royal Commission has emphasized the need for improving the skills of people who work in aged care to better communicate with people with dementia. (Royal Commission into Aged Care Quality and Safety, 2021). Interventions which focus on improving the communication skills of people who communicate with people with dementia (or other communication disorders) is often referred to as “communication partner training” (O’Rouke et al., 2018) and this nomenclature will be adopted in this research for any such intervention. By increasing carer’s knowledge of cognitive linguistic changes associated with dementia and teaching strategies to facilitate communication, communication partner training aims to enhance the quality of life and wellbeing of people with dementia (Smith et al., 2011). Consistent with the Royal Commission recommendations, the need for quality dementia communication partner training for RAC staff is a reoccurring key concern within the literature (Bennett et al., 2016; Bryan et al., 2002; Smythe et al., 2017; Stanyon et al., 2016). Bennett et al. (2016) found that there was a lack of evidence-based individualized communication management for people with dementia in RAC, and recommended using experts that specialize in this area, such as speech pathologists, to facilitate evidence-based practice in communication partner training. Evidence-based communication partner training could support improved communication management in RAC (Bennett et al., 2016).
The outcomes of communication partner training on both residents with dementia and RAC staff have been explored. Various approaches to communication partner training led to improved knowledge and use of communication skills amongst staff over a short-term period (up to three months) (Bourgeois et al., 2004; Broughton et al., 2011; Kuske et al., 2009; McCallion et al., 1999; McGilton et al., 2017; Ripich et al., 1995; Sprangers et al., 2015). However, training requires consistent follow-up and, potentially, organizational changes within the aged care setting to be effective long-term (Eggenberger et al., 2013). Exploring staff perspectives on ways to support sustainable implementation may enable outcomes to be maintained. With improved knowledge and use of quality communication skills by staff, overall communication between staff and residents with dementia may be more effective. There is evidence that improved communication between staff and residents with dementia improves QoL of residents with dementia (McCallion et al., 1999; McGilton et al., 2017), improves staff mood, and reduces burden and strain on staff (McGilton et al., 2017). This highlights the benefit of effective communication partner training in RAC.
Despite the potential benefits of communication partner training for the improvement of QoL for residents with dementia and worker satisfaction, how to provide this training to best suit the needs of RAC workers requires further exploration. In a review of the literature of staff training in aged care, Beeber et al. (2010) evaluated the attributes of staff training that may impact on its effectiveness. Amongst their findings, the authors concluded that training should be planned with the age care community (residents, workers administrators, etc) to maximize success. In accord with this recommendation, this research aims to inform the development and implementation
The specific research questions to be answered are: 1. What are preferences of RAC staff and managers for method/delivery of training in communication partner training with residents with dementia? 2. What barriers and facilitators do RAC staff and management see for successful implementation of professional development in communication partner training with residents with dementia?
Methods
Study and Survey Design
An exploratory cross-sectional online mixed-methods survey design was employed in this study to investigate the preferences, barriers, and facilitators of dementia communication partner training for RAC staff and management in Australia. The online survey approach was chosen to allow participation from a geographically widespread population (Sarantakos, 2005), to support generalization of the findings (Liamputtong, 2017). Ethical approval was granted by the Human Research Ethics Committee of Australian Catholic University (project approval number 2021-298EAP).
Participant Sample and Recruitment
This study aimed to recruit RAC staff and management within Australia. Staff included registered nurses (RN), enrolled nurses (EN), or personal care assistants (PCA), nurse unit managers, nurse practitioners, diversional therapists/activities coordinators, support workers and hospitality/catering. Participants required internet access, the ability to read and write English at a functional proficiency level (as defined by Australian Government Department of Home Affairs, 2021), current employment in RAC within Australia (at least one shift per week), and to be working directly with people who have dementia within RAC. Management staff were included if they performed any duties in the supervision of care staff or the financial management of a RAC facility.
Both purposive and snowball sampling techniques were utilized for participant recruitment. Purposive sampling involved the research team contacting organizations via email that employ or represent RAC workers and requesting for distribution of the online survey to their employees or members. Snowball sampling involved a request within the survey for participants to share the survey link with relevant people. Additionally, targeted paid advertisement through Facebook was developed for further participant recruitment.
Data Collection Procedures
The survey was presented using the online platform REDCap. Data collection commenced in mid- May 2022 and ceased at the end of July 2022. There was only a requirement for compulsory responses for three questions within the survey; (i) to provide or withhold consent, (ii) whether the participant worked in RAC, and (iii) other aged care settings they work in addition to RAC. Those who withheld consent or responded that they do not work in RAC were directed away from the survey.
The survey followed a level 2 reading criteria (Australian Government Style Manual, 2021) so comprehension of questions was ensured for all RAC workers. Time restraints of RAC workers were considered in the development of the survey, with a goal to keep the survey between 10 and 15 minutes to complete. The survey questions were developed by the research team and then pilot tested by members of the research team and speech pathology associates working in aged care. The feedback received related to the specific wording of questions, that is, to remove ambiguity or use clearer terminology. The structure of the survey followed an inverted funnel format; specific closed-ended questions such as multiple choice, yes/no and Likert scales, followed by two open-ended questions (Appendix A).
Data Analysis
All incomplete surveys without final consent were deleted from REDCap prior to exporting the data for further analysis (90 surveys were deleted).
Descriptive statistics (frequency and percentage) were conducted on the quantitative data using IBM SPSS statistics (Version 28) (IBM Corp, 2021). Additionally, Chi-Square tests were used to analyze the relationship between nominal variables and all assumptions (i.e., categorical variables and independent observations) were met (McHugh, 2013).
An inductive content analysis following the methodology of Elo and Kyngäs (2008) was undertaken to analyze the qualitative data. The process of open coding, creating categories and abstraction was completed for participant responses from the two open-ended survey questions. To uphold trustworthiness and rigor, the inductive content analysis was undertaken by two members of the research team and the findings were discussed and reviewed in collaboration. Exemplar quotations from each identified category have been reproduced verbatim, with applied standard punctuation to enhance readability and used to show support for each of the categories. Quotations are identified by participant number. Intercoder reliability (percentage agreement) was conducted by the third author coding responses from 20% of randomly selected responses. 90% agreement was found between coders.
Results
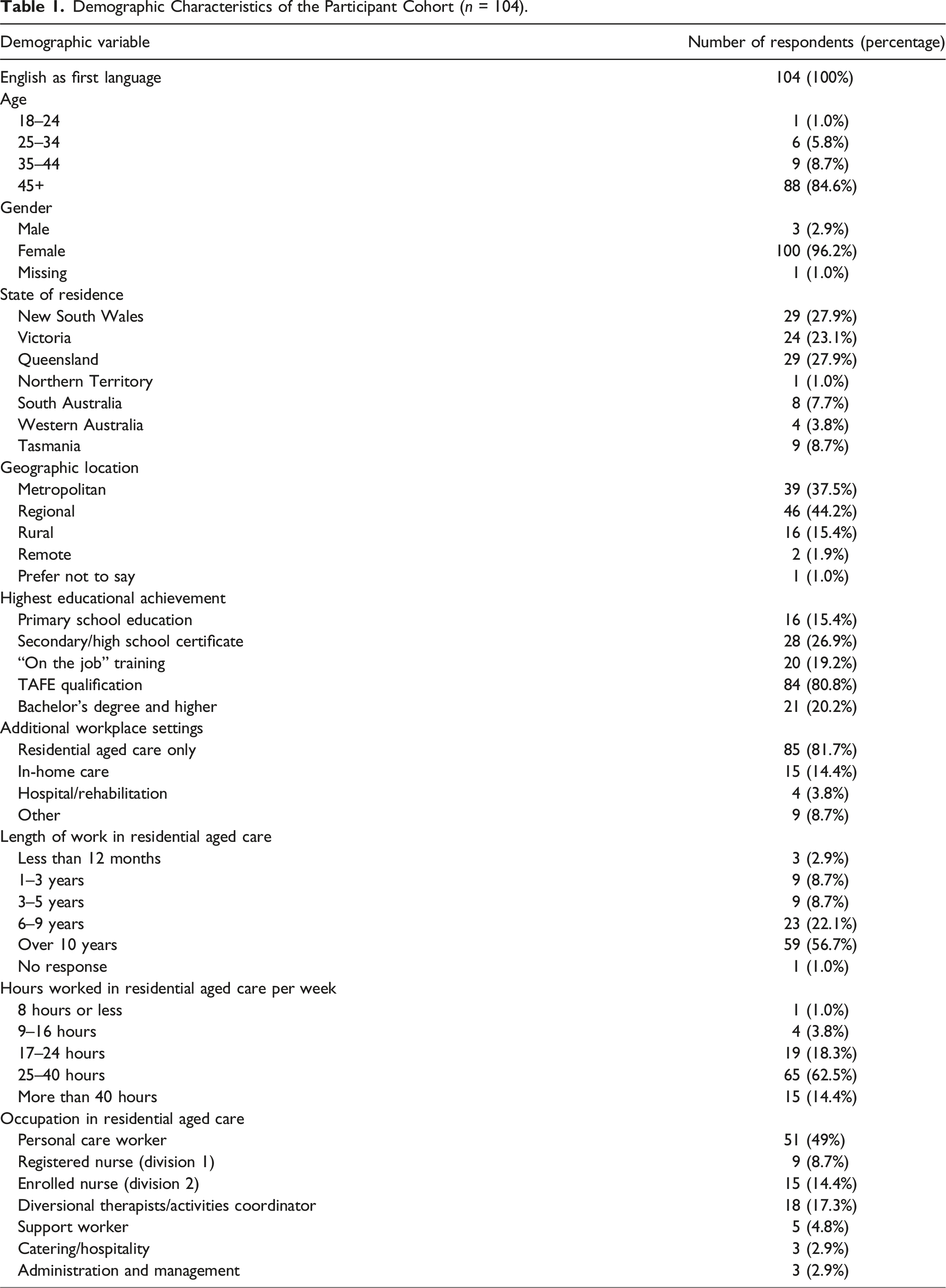
Responses and Demographic Characteristics of the Participants
Demographic Characteristics of the Participant Cohort (n = 104).
Staff Participation and Methods of Previous Dementia Communication Partner Training
Staff Participation and Methods of Previous Dementia Communication Training.
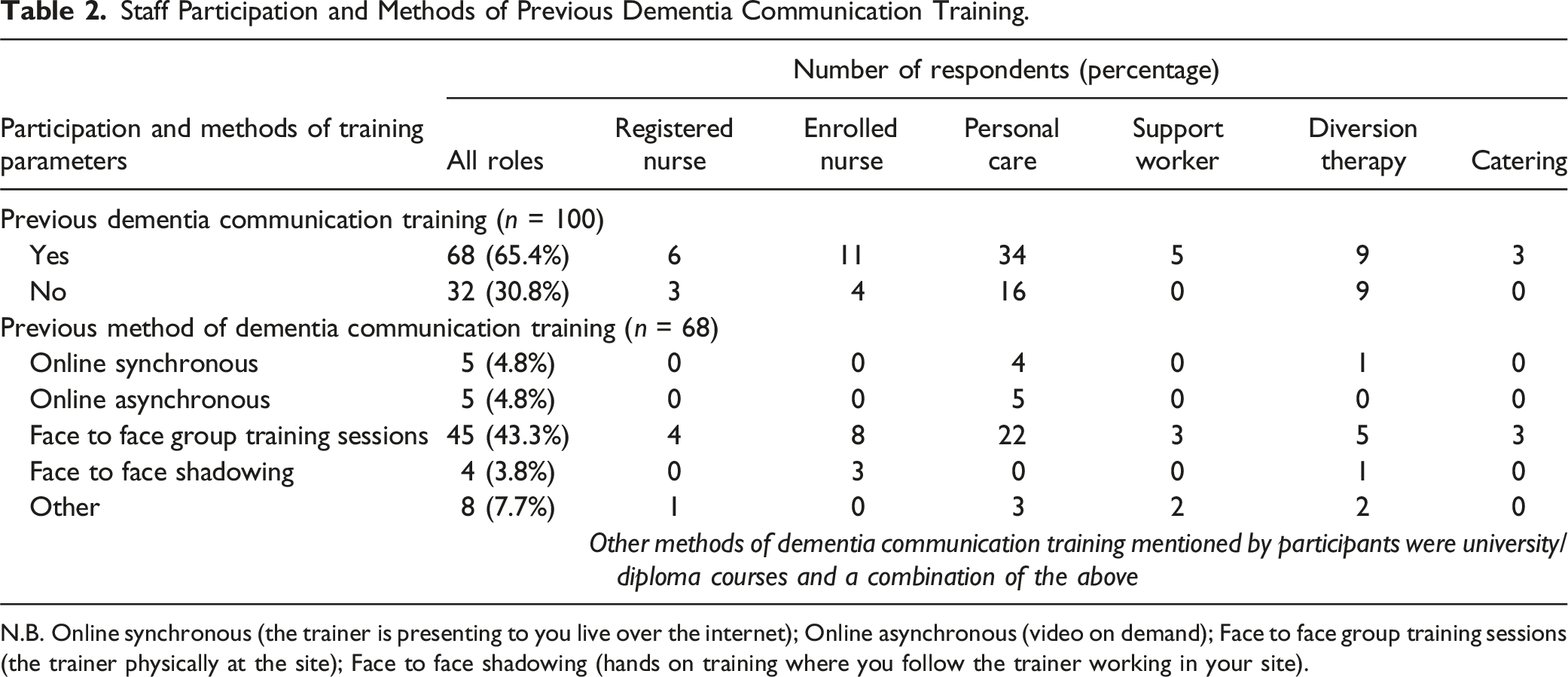
N.B. Online synchronous (the trainer is presenting to you live over the internet); Online asynchronous (video on demand); Face to face group training sessions (the trainer physically at the site); Face to face shadowing (hands on training where you follow the trainer working in your site).
Dementia Communication Training Preferences of Staff and Managers
Three participants were in an administration/managerial role within RAC. All managerial participants reported dementia communication partner training as “very important.” Majority (2/3) of these participants preferred training to be within paid work hours and would be prepared to pay staff $0-$500 for training.
Dementia Communication Training Preferences of Staff.
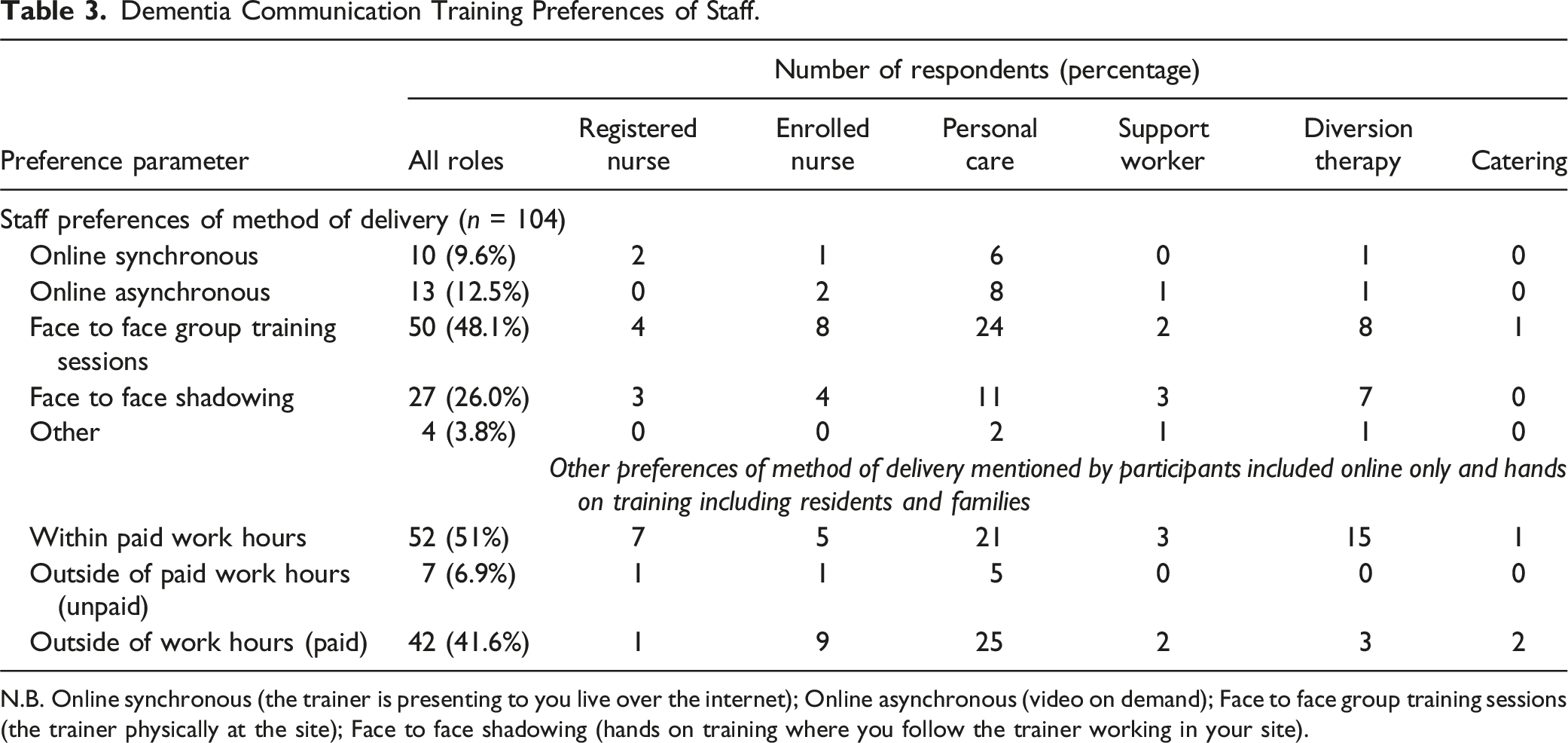
N.B. Online synchronous (the trainer is presenting to you live over the internet); Online asynchronous (video on demand); Face to face group training sessions (the trainer physically at the site); Face to face shadowing (hands on training where you follow the trainer working in your site).
Relationships Between Variables
Chi-Square tests were used to determine if demographic factors influenced future preference of method of delivery of training. These factors included age, state, geographical location type within a state, role in RAC, and past methods of dementia communication training. Additionally cross tabulation was conducted to determine if education level or role in RAC influenced whether staff had participated in dementia communication training before. Overall, there was no significant relationship detected between any of these variables.
Barriers and Facilitators to Workplace Training
The two open-ended questions were “What do you think are challenges to training in your workplace and why?” and “What factors/elements do you believe are necessary to create more opportunity for more communication training in the workplace?” In total, 86 and 84 responses were analyzed for the first and second open-ended questions, respectively. Responses were excluded if irrelevant to the topic. Overall, seven categories were identified regarding barriers and facilitators to workplace training.
Category 1: Number of Staff
Participants described various challenges related to the staff numbers. Participants (n = 41) highlighted staff shortages and availability as a barrier to participation in training. Additionally, participants (n = 11) specifically noted that due to staff shortage, there was a “lack of staff” to replace other staff if they choose to participate in training during work hours. Some participants (n = 3) expressed concern regarding the impact on residents when training takes them “away from residents without being replaced” (#46).
Consequently, numerous participants (n = 21) highlighted the need for “more staff” in their workplace to facilitate workplace training. Some participants (n = 7) explicitly stated that by increasing the number of staff working, this will “allow staff to attend” (#21), and more staff to “cover training sessions” (#41).
Category 2: Time
Numerous participants (n = 30) indicated that “lack of time” was a barrier to participation in training, with some (n = 12c) that explicitly linked this back to staff shortage, expressing concern to “…not leave other staff short on the floor” (#12). One participant also stressed external competing demands as a barrier to participation, stating “staff have second jobs or children they need to care for” (#18). Participants (n = 11) emphasized the importance of “more time” to facilitate more opportunity for communication partner training. One participant noted that there needs to be “time to do training…time to spend with new staff to teach them properly” (#71). Another participant expressed the need for “time allocated to training people without having an impact on the workday” (#92). Furthermore, some (n = 6) participants linked time restraints to staff’s heavy workload, where staff are “still expected to complete all on the job tasks as well as training, never enough time … to complete it on shift” (#22).
Category 3: Remuneration
Some (n = 7) participants noted that “not getting paid” (#10) for training is a barrier to participation, with two participants that further described the difficulty for staff to “attend outside paid working hours” (#17). One participant highlighted that “usually workplace training is unpaid” and that aged care is a “low paid workplace as it is” (#35). Thus, many participants (n = 12) reported that being “paid” to attend training was a facilitator to participation in training. One participant stated that management should be “willing to provide paid training during working hours” (#86).
Category 4: Training Elements
The method of delivery of training was one of the key elements that was noted by participants (n = 20) in both open-ended questions. Participants (n = 4) expressed the challenge of training being completed online. One participant reported they “can’t access” online training “from home” (#71), and other participants expressed their concern that online training is not suitable for dementia education. Most participants (n = 13) expressed that face to face training was their desired method of delivery. Types of face to face training participants mentioned included “on the job” and “hands on” training, for example, learning at the same time as working with dementia residents, and on-site training, however, not working at the same time. In contrast, two participants indicated that “online” training was their desired method of delivery. The remaining participant suggested a combination of both “online and onsite opportunities” (#22) for training.
Some participants (n = 8) revealed that the quality of the facilitator/educator of the training was an important factor to facilitate workplace communication training. For example, participants stated the need for “passionate qualified trainers … who care about the level of care given to our residents” (#70) and “trainers with actual real-life skills, not just a cert 4 in training” (#20).
Many features of the training itself were described by participants (n = 12). For example, one participant mentioned factoring into the training programs the staffs’ experience regarding the needs of the resident with dementia. Others (n = 3) highlighted that training needs to be “individualized” to both the staffs’ current skills and the dementia resident’s needs. Two participants suggested that training should focus on “how to apply the staffs’ understanding” (#15) of dementia to the resident with dementia.
The frequency and standards of communication partner training for dementia was highlighted by many participants (n = 13). Some participants (n = 5) stated that training needs to be more frequent. Some participants (n = 4) explicitly indicated the time frame; every two to three months, every six months, or yearly. Participants (n = 5) also expressed that the training “should be mandatory” (#81) for staff. In contrast, one participant noted that staff should “do it because you want to NOT because you have to” (#14), regarding participation in training. Another participant proposed that staff should receive a type of “certificate” after completing training and that it should be a “minimum standard” (#46).
Lastly, the timing of training was discussed by some participants (n = 8). They reported that “varied times” (#19) to complete training would be beneficial due to “different staff rosters” (#19) and “short staffing issues” (#68). Two participants suggested having designated days for training, with one participant that further explained this would be more beneficial “instead of pulling staff off the floor or adding more hours to staffs week” (#55).
Category 5: Management Factors
The “cost” of training for RAC management was emphasized as a barrier by participants (n = 8). One manager participant noted that “training is not budgeted for” (#14). Other participants (n = 3) stated that management will simply “not pay for it.” Another participant expressed that management do not “pay for training to be done correctly or on the right topics” (#46). One participant noted the challenge for “the company paying for Dementia Australia to come and provide at the facility” (#56). Participants (n = 11) identified that increased “funding” for training from the government, or organizations increasing their financial “budget” for training would provide benefit and facilitate workplace training. A few participants (n = 3) stated that management having “easily available resources for staff to access whilst on the job to assist” (#82) such as “reliable in-house services”, “finding space to train” (#4), “computers” (#59) and “evidence-based training programs” (#46), would facilitate communication training in the workplace.
Additionally, staff participants (n = 6) mentioned that there is “no value placed on training” (#27) by management. One participant noted that management lack the understanding of the importance and impact the training could have on the RWD, staff and families (#79) whilst another stated management opposition and not “being allowed to go to training” (#6). One participant described management perceiving training as a “‘tick box’ to appease assessors and achieve accreditation.” One participant also noted that management uses “time and money restraints” (#79) as an excuse for not offering training. Participants expressed that management need to understand the importance of training/education for dementia communication (n = 8), and the impact this will have on the RWD. For example, one participant stated, “management need to realize staff training in dementia would help behaviors” (#49). One participant suggested for “human resources to spend time working on the floor as opposed to having a walk through or visit” to gain an understanding of “what dementia behaviors look like” (#96).
Category 6: Staff Attitudes and Knowledge
Various participants (n = 14) noted staff attitudes as a barrier to participation in training. Staff exhibiting a lack of interest or motivation “not wanting to participate” (#83) or “getting those that need training to turn up” (#5) was a point raised by some participants (n = 8). Additionally, others attributed the lack of participation in training to staff having “old ideas or beliefs” (#77); with long held personal beliefs involving dementia communication, leaving them closed to new ideas, and resistant to change. A participant highlighted the challenge for staff to “follow through what they have learnt” (#68) in training, with another participant that stated training results in an “information overload” (#74) for staff. One participant highlighted how too many staff “have zero understanding of dementia as a disease” (#92), therefore do not understand the “impact it has on the client to communication needs/wants” (#92).
Category 7: Culturally and Linguistically Diverse Background
A few participants (n = 3) mentioned that a barrier to participation in training is many staff having a “non-English speaking background” (#8). One participant stated that some staff “are very hard to understand when talking English and some do not understand what you are saying” (#48).
Taken together, seven key factors accounted for the participants views on barriers and facilitators to participation in communication training. These factors are the number of staff available, available time, the make-up of the training, remuneration, attitudes of management, staff attitudes and the impact of culture and linguistic diversity. The availability of staff to cover care duties, whilst training occurs and time to participate in training were the most frequently reported factors.
Discussion
This study aimed to investigate the preferences and perspectives of Australian RAC staff and managers for workplace-based communication partner training with residents with dementia. Overall, staff perceived value in communication partner training and were eager to support communication between themselves and residents with dementia. Staff reported that they would prefer communication training to be delivered face to face, that training acknowledges the current skills of staff, and that implementation of training could by facilitated by supporting staff availability and paying staff for training time. There were also many perceived barriers identified to the effective implementation of communication partner training; these barriers are both systemic and reflective of challenges faced in aged care settings (e.g., staff shortages, funding, and resources), and individual (e.g., staff attitude). This study supports the recommendation by Beeber et al. (2010) that dementia care staff training design should be collaborative, including the voice of aged care workers. The following discussion will consider the views of the participants with respect to the existing literature and offer recommendations for future implementation of communication partner training in residential aged based on the views of the workers.
Many participants identified the importance that dementia communication partner training has on the quality of care they provide, expressing that training should be both more frequent and a mandatory requirement as a RAC worker. This finding highlights that the staff perception of the need for the provision of dementia communication partner training is consistent with the literature and findings of the Royal Commission (Bennett et al., 2016; Bryan et al., 2002; Hamiduzzaman et al., 2020; Royal Commission into Aged Care Quality and Safety, 2021; Smythe et al., 2017; Stanyon et al., 2016; Talbot & Brewer, 2016). This finding suggests that staff willingness to engage in training is not a barrier to quality communication in RAC.
Another important element of training discussed by participants was the need for high-quality and experienced educators to deliver the training. Previous research has reported that staff perception of training usefulness and quality contributes to the quality of care post training (Anderson & Blair, 2021). One aspect that may facilitate educator quality is educator content expertise. With respect to communication, the use of Speech-Language Pathologists with experience in communication in aged care as educators should be considered. Speech-language pathologists are allied health professionals that have specialist knowledge in management of communication difficulties (Speech Pathology Australia, 2019). To date there have only been a few communication partner training programs that are designed or facilitated by SLPs (e.g., MESSAGE; Smith et al., 2011). This is an area of potential improvement; Speech Pathology Australia (2019) strongly supports the increased utilization of allied health professionals in RAC training, particularly around the use of speech pathology evidence-based strategies (Speech Pathology Australia, 2019) particularly in communication partner training (Bennett et al., 2019).
A key finding gained from this study related to staff perspectives on training implementation was that most participants prefer dementia communication training to be delivered face to face. Some participants went on to express that online training was ineffective for dementia-related education. In their review of dementia care training programs, Beeber et al. (2010) found that successful training programs were usually delivered face to face. The current findings also suggested that training should support staff to apply the information learnt directly to the residents with dementia in their care. These preferences are consistent with behavioral rehearsal, feedback, and modeling documented as behavioral change techniques considered in the implementation science literature (Michie et al., 2008). In past research, RAC staff reported difficulties with the implementation of some of the recommendations from communication partner training in practice (Bennett et al., 2014, 2016; Smythe et al., 2017). The MESSAGE communication partner training program, however, reported that staff knowledge was maintained at three months post training (Conway et al., 2016). This program included the trainers providing feedback of video recorded conversations between the staff member and a resident at one, two and six weeks post initial training. Integrating the findings from this study on worker preference and the existing literature, it is therefore recommended that staff training be both (i) face to face/in person as much as possible and (ii) that training is work integrated such that a component of the training involves working with people with dementia in practice contexts and observations with feedback are provided on the staff’s work.
While staff have identified ways to improve the implementation of training, it appears that they face additional barriers to their actual participation in workplace training. A recurring theme from participants was that they have an inadequate amount of time to participate in workplace training, which seems to be a consequence of staff shortages and a heavy workload. Additionally, there is concern regarding the impact on residents with dementia if staff choose to attend training; as staff report that they need to make an untenable choice between upskilling or caring for their residents. These findings align with the 2019 National Aged Care Survey (Australian Nursing and Midwifery Federation, 2019), where inadequate staffing levels and the consequent impacts on both staff and residents was one of the main concerns raised by staff in RAC. Furthermore, the impact of staff shortages and high workload is the main contributor for nurses leaving aged care (Australian Nursing and Midwifery Federation, 2019), with high staff turnover being a barrier to successful communication amongst staff and residents with dementia (Bennett et al., 2014). Participants have also expressed the personal conflict that exists between training outside of work hours and other competing demands, such as working a second job or their children/family. Staff are inadequately paid for their work, as evidenced by the Royal Commission recommendations (Royal Commission into Aged Care Quality and Safety, 2021). Most staff are not in the position to voluntarily use their personal time without payment. These barriers highlight the demand placed on staff, and the choices they need to make to undertake professional development.
The attitudes of staff towards workplace training were described by many participants. For example, it was reported that some staff lack the interest and motivation to upskill and participate in workplace training. However, this was not the main issue. It was evident that factors around insufficient time due to staff shortages, a heavy workload, and other competing demands, as well as inadequate pay are having a greater impact. Given these barriers, it is understandable why staff may be disinterested in undertaking training; it is simply too challenging. If staff choose to participate in training when offered within work hours, staff shortages and the implications of this become problematic. With evidence of staff reported hierarchal bullying/harassment from management to meet work demands (Australian Nursing and Midwifery Federation, 2019), staff may also be fearful of the repercussions they face from management if they choose to participate in training and leave residents unattended, that is, not fulfilling their work duties. Although staff in the survey did not report that they had hierarchal bullying experiences, in a broader context we must consider the pressures on workers to meet work demands plus participate in training.
The role that management play in the implementation of communication training was a key category that emerged from participant survey responses. Staff participants perceived that management placed no value on communication partner training, and did not understand the impact it can have on the residents with dementia, staff and families. However, this was in contrast to the three managerial participants who reported dementia communication training as “very important.” Furthermore, the cost of training is a primary concern for management; consequently, there may be conflict between what training is the highest priority to fund. These findings were not unexpected, as the Royal Commission into Aged Care Quality and Safety (2021) highlighted the insufficiencies of funding for aged care by the Australian government. These inadequacies in funding may explain reports in the present study of lack of financial budget for workplace training. With the improvements in funding for education and training implemented by the Australian government (Australian Government Department of Health, 2022), and the Royal Commission recommendations to improve the communication skills and capacity aged care staff have (Royal Commission into Aged Care Quality and Safety, 2021), management may be more likely to direct funding towards communication training in the future.
Recommendations and Future Directions
It is recommended that communication partner training in RAC be delivered face to face in the practice context with residents with dementia, be provided more frequently, and should accommodate for as many RAC staff to participate as possible. Future research is needed to better understand the effectiveness of communication partner training that incorporates these worker preferences and the resultant worker experience. Future research should also explore the reasoning behind worker preferences for mandatory communication partner training and how this might be made possible in the industry. Such research could be considered in the context of the behavioral change theory literature given the finding that staff identified preferences consistent with behavioral change techniques. Lastly, the perspectives of culturally and linguistically diverse RAC staff on communication training require further exploration.
Limitations
There were existing limitations to this study that should be considered when interpreting the current findings. Only three managers participated in the survey; therefore, caution should be taken when interpreting the responses of managerial staff. Second, this study was not successful in recruiting participants who speak English as a second language. With approximately 35% of the RAC workforce from a culturally and linguistically diverse background (Australian Government Department of Health, 2020), the opinions expressed in the study findings were not representative of all those who work in RAC. Finally, as many participants were recruited through targeted Facebook advertising, a potential bias exists as individuals with an interest in the subject were more likely to respond to the survey. Therefore, findings may not reflect all RAC worker perspectives. Future investigations with a larger and more diverse representative sample would improve the power of statistical analysis and generalizability of findings. 194 people commenced the survey, but only 104 surveys were completed and included in the analysis. Decreasing the length of the surveys may assist increasing participation and sample size.
Conclusion
This study explored the perceived barriers and facilitators of RAC staff and managers for communication partner training in Australian RAC. Additionally, their preferences for the method/delivery of communication training were investigated. Given the existing barriers for staff to participate in workplace training, considering staff preferences and facilitators in the development of future communication training is significant. Staff may be more motivated to undertake communication training if better suited to their needs and preferences, more likely to maintain the knowledge and skills learnt, and subsequently, in alignment with the Royal Commission’s recommendations, offer residents with dementia a higher quality communication environment.
Supplemental Material
Supplemental Material - “Time is a Big Factor”: Aged-Care Workforce Perspectives on Communication Partner Training for Working With Residents With Dementia
Supplemental Material for “Time is a Big Factor”: Aged-Care Workforce Perspectives on Communication Partner Training for Working With Residents With Dementia by Charlotte McKenzie, Michelle Smith-Tamaray, Erin Conway, and Kieran Flanagan in Journal of Applied Gerontology.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.