
Abstract
In this study, we employed a pre-interview survey and conducted interviews with nursing home staff members and residents/family members to understand their perceptions of whether the COVID-19 restrictions fulfilled obligations to nursing home residents under various principles, including autonomy, beneficence, nonmaleficence, justice, and privacy. We conducted 20 semi-structured interviews with staff members from 14 facilities, and 20 with residents and/or family members from 13 facilities. We used a qualitative descriptive study design and thematic analysis methodology to analyze the interviews. Findings from the pre-interview survey indicated that, compared to nursing home staff, residents and their families perceived lower adherence to bioethics principles during the pandemic. Qualitative analysis themes included specific restrictions, challenges, facility notifications, consequences, communication, and relationships between staff and residents/family members. Our study exposes the struggle to balance infection control with respecting bioethical principles in nursing homes, suggesting avenues for improving processes and policies during public health emergencies.
• This qualitative study describes how both nursing home staff and residents and their families perceived and coped with the difficult bioethical trade-offs associated with the COVID-19 restrictions in U.S. nursing homes. • Results from this study contribute to the ongoing discourse surrounding the delicate balance between infection control measures, delivering care ethically, and the broader well-being of nursing home residents, their family members, and staff members.
• Policymakers should identify and address challenges in balancing the need for infection mitigation during periods of crisis with the necessity to respect their ethical obligations to residents. They should develop guidelines that strike the balance between safety measures and principles of respect for persons, dignity, and justice. • To foster better mutual understanding among nursing home staff, residents, and their family members, facilities should develop communication strategies to facilitate clarity regarding facility management decisions and government policies. • Facilities should encourage the active, formal involvement of nursing home residents and their families (e.g., through family councils) in decision-making processes with staff and administrators, to ensure that their perspectives are considered in policy development and implementation.What this paper adds
Applications of study findings
Introduction
Nursing homes have been highly susceptible to the spread of COVID-19 due to the communal living arrangements and the frequent interactions among residents, staff members, and visitors (Markowitz & Paulin, 2022). Older age, chronic conditions, frailty, and biological changes of individuals residing in nursing homes have all increased their mortality risk (Mueller et al., 2020).
In March 2020, responding to the Centers for Medicare and Medicaid Services (CMS)’ guidance, U.S. nursing homes prohibited visits from family and friends and suspended resident group activities (Centers for Medicare and Medicaid Services [CMS], 2020a). While CMS began easing visitation rules from May 2020 (CMS, 2020b), the duration of restrictions varied based on local regulations, COVID-19 risk levels, and facility decisions. Although these restrictions aimed to reduce morbidity and mortality, previous studies noted increased depression and anxiety, alongside reduced physical and cognitive function in residents due to limited interpersonal interactions and activities (EI Haj et al., 2020; Levere et al., 2021). Restrictions also caused significant distress among staff and family members of residents (Conejero et al., 2023; Cornally et al., 2022).
As these studies demonstrate, a central question about the pandemic restrictions is whether they produced reductions in mortality and morbidity that were proportionate to their unintended physical and psychological harms, such as reduced physical and mental well-being in residents, and emotional exhaustion in residents’ families and nursing home employees. Adequately answering this question involves incorporating additional factors into the balance, namely facilities’ ethical duties to these vulnerable individuals. The Belmont Report of 1978 outlined obligations for healthcare professionals, further detailed in subsequent editions of Principles of Biomedical Ethics (Beauchamp & Childress, 2019; National Commissioner, 1978). These principles—beneficence, nonmaleficence, autonomy, and justice—derive from common morality, reflecting widely accepted ethical norms in healthcare relationships. In the long-term care (LTC) setting, beneficence entails prioritizing residents’ well-being to foster positive outcomes for both residents and caregivers. Nonmaleficence requires preventing harm to residents and caregivers, whether by action or inaction. Autonomy mandates healthcare professionals to support residents’ informed decision-making, respecting their autonomy even if they lack capacity, and relying on surrogate decision-makers committed to their welfare and knowledgeable about their preferences. The principle of justice underscores the fair distribution of burdens and benefits across all groups.
In nursing homes, the duties of beneficence and nonmaleficence are met through CMS Conditions of Participation ensuring safe, effective care and minimizing risks to residents’ well-being. These conditions extend to respecting residents’ preferences, including visitation permissions. Upholding the principle of justice requires LTC facilities to ensure decision-makers are free from conflicts of interest.
It’s not always possible to fulfill all these duties simultaneously, so compromises may be necessary (Jonsen et al., 2015). In clinical settings, conflicts often arise between respecting patients’ choices and maximizing their well-being. While medical paternalism contradicts ethical obligations, professionals are not obligated to provide care beyond available resources or that violates standards or laws. In public health settings, obligations based on justice and nonmaleficence require both healthcare professionals and citizens to consider the consequences of their actions and respect necessary orders from public health officials to protect the general welfare. The present study examines the multifaceted impacts of COVID-19 restrictions in U.S. nursing homes in order to understand how both nursing home staff and residents and their families perceived and coped with the difficult trade-offs associated with the COVID-19 restrictions in U.S. nursing homes, as viewed through the lens of ethical principles.
Methods
We conducted a qualitative study with semi-structured interviews with nursing home staff members and residents/family members between May 2023 and August 2023. The study protocol was approved by the University of Southern California Institutional Review Board (IRB Protocol # UP-22-00340).
Recruitment of Study Participants
Nursing Home Staff
We obtained nursing home email lists from MedicoReach (Leander, TX), IQVIA (Durham, NC), and DataCaptive (Santa Clara, CA), covering over 10,000 nursing homes in all U.S. states. In a previous national study, we surveyed individuals in senior administrative and director-level positions in facilities classified as skilled nursing facilities or nursing facilities to collect information about COVID-19 restrictions (Xu et al., 2024). We asked the 402 facility representatives who responded to the survey to forward information about this study to frontline staff, asking those who were willing to volunteer to be interviewed.
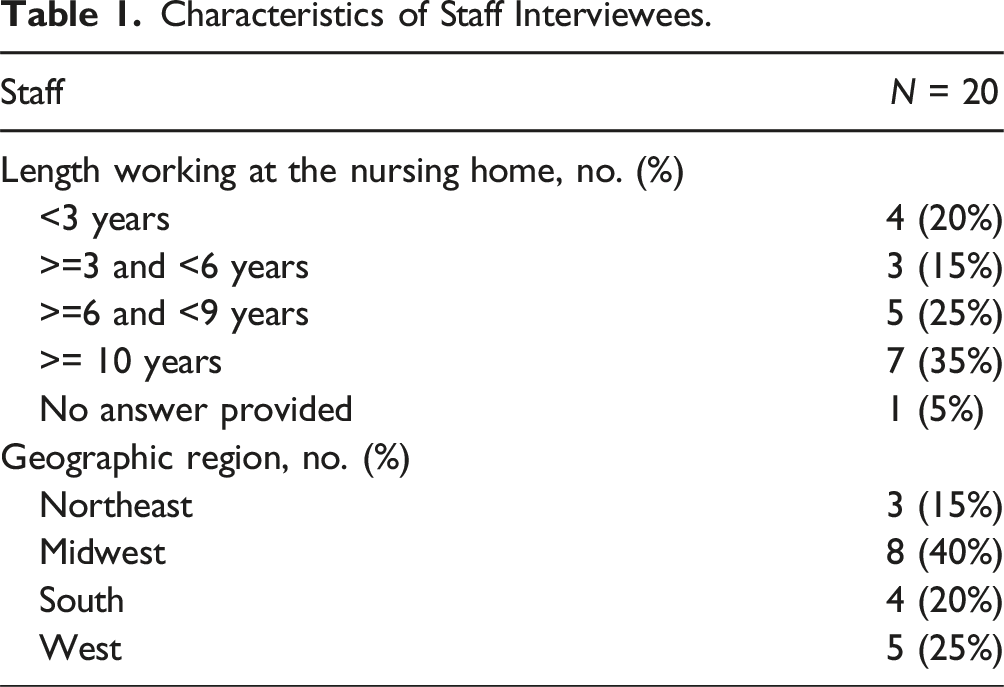
Prior to the interview, we asked screening questions by phone or email to determine whether each volunteer met the study’s eligibility criteria. To be included, staff members needed to be employed in direct care of residents at the same CMS-certified nursing home at the time of the interview as they were in March 2020, when most of the COVID-19 restrictions were first introduced. No more than two staff members from a single facility were included in the study. We screened 44 potential participants to yield the 20 staff members who were interviewed.
Characteristics of Staff Interviewees.
Nursing Home Residents/Family Members
Various recruitment methods were employed to engage nursing home residents and their family members. Initially, survey respondents were asked to facilitate connections with willing interviewees. Additionally, snowball sampling was utilized, with residents/family members encouraged to introduce us to others interested in participating and refer us to relevant community-based organizations. Both residents and families were invited to take part in interviews. In cases where residents faced cognitive or physical challenges hindering their participation, family members had the option to participate on their behalf.
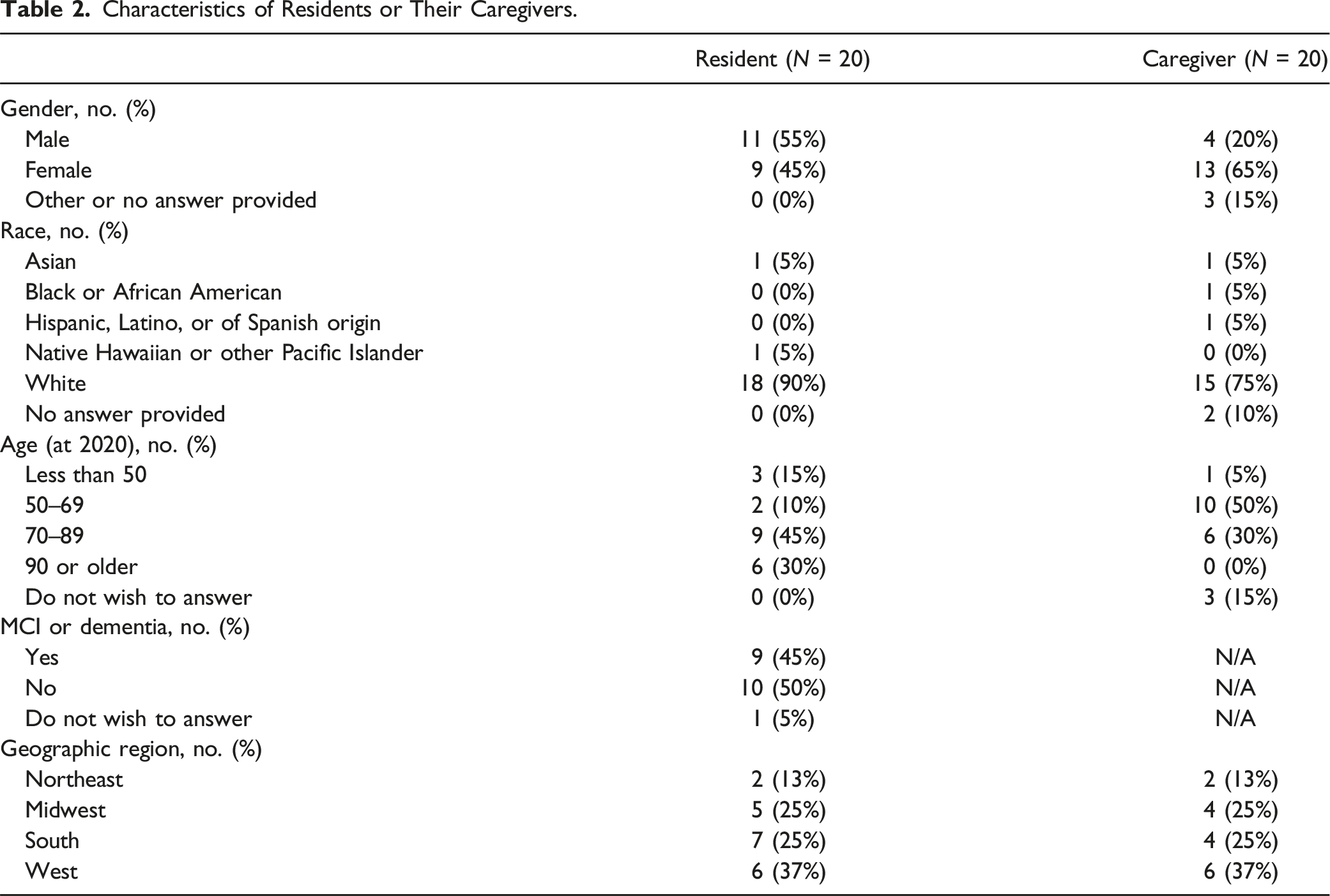
To be eligible for the study, nursing home residents had to be living in a CMS-certified nursing home in March 2020. Family members of residents who had passed away during the pandemic were also eligible. Prior to the interview, we asked screening questions by phone or email to select residents and family members who met the eligibility criteria. No more than two residents/family members from a single facility were included in the study. We screened 35 potential participants to yield the 5 residents and 15 family members who were interviewed.
Characteristics of Residents or Their Caregivers.
Data Collection
We scheduled all of the interviews at least one day after the screening questions were collected and after we obtained oral consent to participate in the study. We informed participants at the beginning of the interview that they were allowed to contact the research team to modify or withdraw their responses within 14 days after the interview; none did. We conducted the interviews on Zoom (or by phone calls if a participant was unable to connect to Zoom). The interviews averaged 40–50 min. All interviews were audio-recorded and transcribed using Rev.com’s automatic transcription tools and were checked for accuracy.
Pre-Interview Questionnaire
We administered pre-interview questionnaires on Qualtrics (Qualtrics™, Provo, UT) to collect demographic information on the respondents (Appendix 1(a) and 1(b)). We asked participants to rate the extent to which ethical principles were respected in the implementation of restrictions. Specifically, we asked both staff members and residents/family members to rate from 0 to 10, the degree to which the principles of autonomy, beneficence, nonmaleficence, and justice were respected when restrictions were in place (where 0 represented “not at all” and 10 represented “extremely”). Participants were given a slider to select the scale, enabling them to choose values to one decimal place instead of whole numbers.
Interview Guides
Separate semi-structured interview guides were used for staff members (Appendix 2(a)) and residents/family members (Appendix 2(b)). The interview guides asked about staff and resident/family member experiences with the restrictions implemented during the COVID-19 pandemic and their perceptions of the restrictions. The guides included questions regarding adjustments of restrictions under special circumstances, how the restrictions were communicated to the respondent, what challenges the respondent experienced due to the restrictions, and the impacts of the restrictions on the physical, mental, cognitive, and spiritual well-being of the respondent.
Data Coding and Analysis
We used a qualitative descriptive analysis approach and Clarke and Braun’s thematic analysis methodology for data coding and analysis (Clarke & Braun, 2017). The transcripts of the interviews were uploaded to Dedoose (Version 9.0.17, Los Angeles, CA: SocioCultural Research Consultants, LLC). Two health policy doctoral students (YG and SX) coded the interviews under the guidance of an experienced qualitative researcher (MSK). We coded the first three interviews using an initial coding approach, that employed some a priori deductive codes (i.e., sensitizing concepts, or starting lines of inquiry) from the interview guides and from bioethical principles (Charmaz, 2006). We developed the majority of the codebook using inductive methods from the data. To increase the rigor of the coding, the two graduate students coded the first three transcripts of each interviewee group together, meeting weekly with the qualitative researcher (MSK) to discuss areas of disagreement and reach a consensus about the coding framework. Through our weekly meetings, we identified higher-level focused codes, which were more conceptual and overarching in nature. We organized the initial codes under the focused codes, and the two doctoral students coded the remaining transcripts. We met weekly for four weeks to review the coding process, discuss the structure of the codebook, and review new codes. After all of the transcripts were coded, we exported all of the coded excerpts into separate documents by focused codes. We met to analyze the transcripts, using the constant comparison method outlined in Corbin and Strauss (2008), comparing both experiences within and across the resident/family interviewee and nursing staff groups. For example, we compared the perceptions of the restrictions in several ways, including within interviewee groups, over time (e.g., during the course of the COVID-19 pandemic), and across the groups. We aimed to identify variation within each theme, for example, instances where an interviewee’s participant differed from the group to account for the full range of experiences. We aimed to develop rich, fully developed themes and stopped the interviews when we felt we had reached theoretical saturation (Charmaz, 2006), that is, when we felt that additional interviews were no longer adding to the concepts identified within each theme and that each theme was fully fleshed out. We also created diagrams to examine how themes related to each other, for example, how perceptions of the restrictions resulted in interviewee’s experiences with the consequences of the restrictions. We did not return the transcripts to participants for correction or comment. We took several steps to reduce bias. First, our semi-structured interview guide included open questions aimed at avoiding leading respondents to answer in any particular manner (e.g., with negative or positive experiences). Second, we used multiple coders on the transcripts and met regularly to develop the codebook, discussing areas where an individual coder’s perspectives and experiences may have shaped a particular code or coding excerpt. Third, our coding scheme and analyses were grounded in the data to reduce the effect of pre-conceived notions. Fourth, we reviewed the literature and identified examples where others had made similar findings (described further in the discussion).
Results
Residents/Family Members Reported Lower Levels of Respect for Ethical Principles Than Staff
The respondents typically did not use bioethics terminology, such as the principles of beneficence, nonmaleficence, autonomy, and justice, when describing their experiences, but both groups of interviewees responded readily to questions about the principles (which had been explained in the materials they received). When asked to rate the degree to which the ethical principles were respected by their nursing home while the pandemic restrictions were in place, the mean scores and score distribution of ratings were substantially lower among resident/family respondents than staff respondents for three of the four principles (see Figure 1). Staff rated respect for the duty of beneficence at a mean of 8.7 and a median of 10.0 (range: 4–10.0, interquartile range [IQR]: 7.9–10.0), while residents/family members’ ratings had a mean of 6.1 and a median of 7.6 (range: 0–10.0, IQR: 1.7–10.0). Respect for the duty nonmaleficence was rated at a mean of 8.4 and a median of 9.8 by the staff (range: 0–10.0, IQR: 8.3–10.0), but much lower—a mean of 6.2 and a median of 7.9 (range: 0–10.0, IQR: 1.2–10.0)—by residents and family members. Staff rated respect for the principle of justice at a mean of 7.4 and a median of 7.8 (range: 0–10.0, IQR: 5.1–10.0), while residents and family members’ ratings on this principle had a mean of 6.0 and a median of 7.2 (range: 0–10.0, IQR: 0.7–10.0). Given that the public health mandates severely restricted the choices available to residents and family members for interacting, it is not surprising that both groups of respondents gave their lowest ratings on the degree to which the principle of autonomy was respected. Staff respondents’ ratings had a mean of 4.4 and a median of 5.0 (range: 0–8.2, IQR: 1.4–6.5), which was similar to those of residents and families which had a mean of 5.0, and a median of 4.5 (range: 0–10.0, IQR: 0.9–9.8). Distributions of staff and residents/families on ratings of ethical principles respected during the restriction period for residents and their families. Notes. x in the boxes represents the mean. Horizontal lines in the boxes represent medians. Upper and lower quartile values are marked by whiskers and outliers are marked by dots.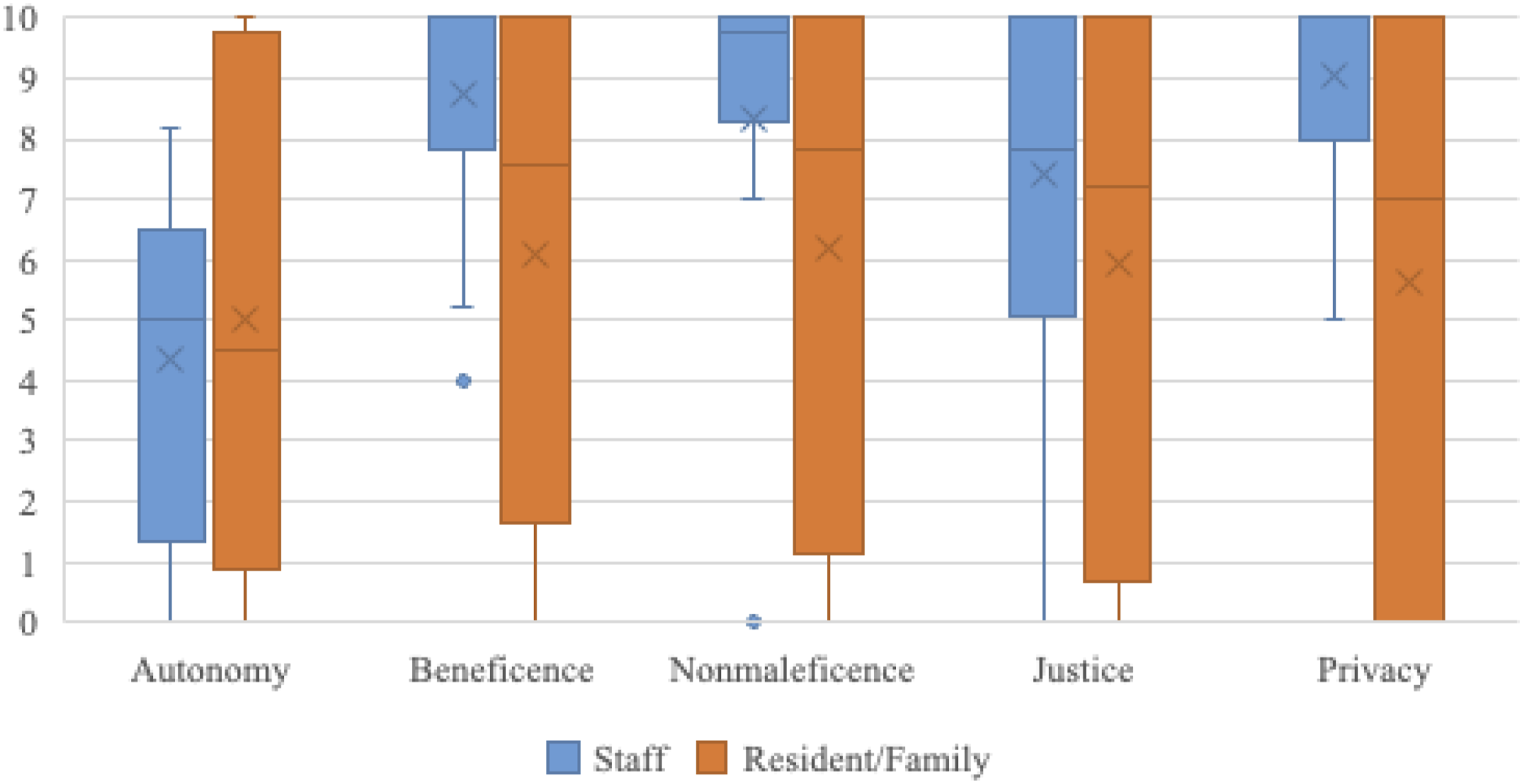
COVID-19 Restrictions Impinged on Autonomy in Nursing Homes
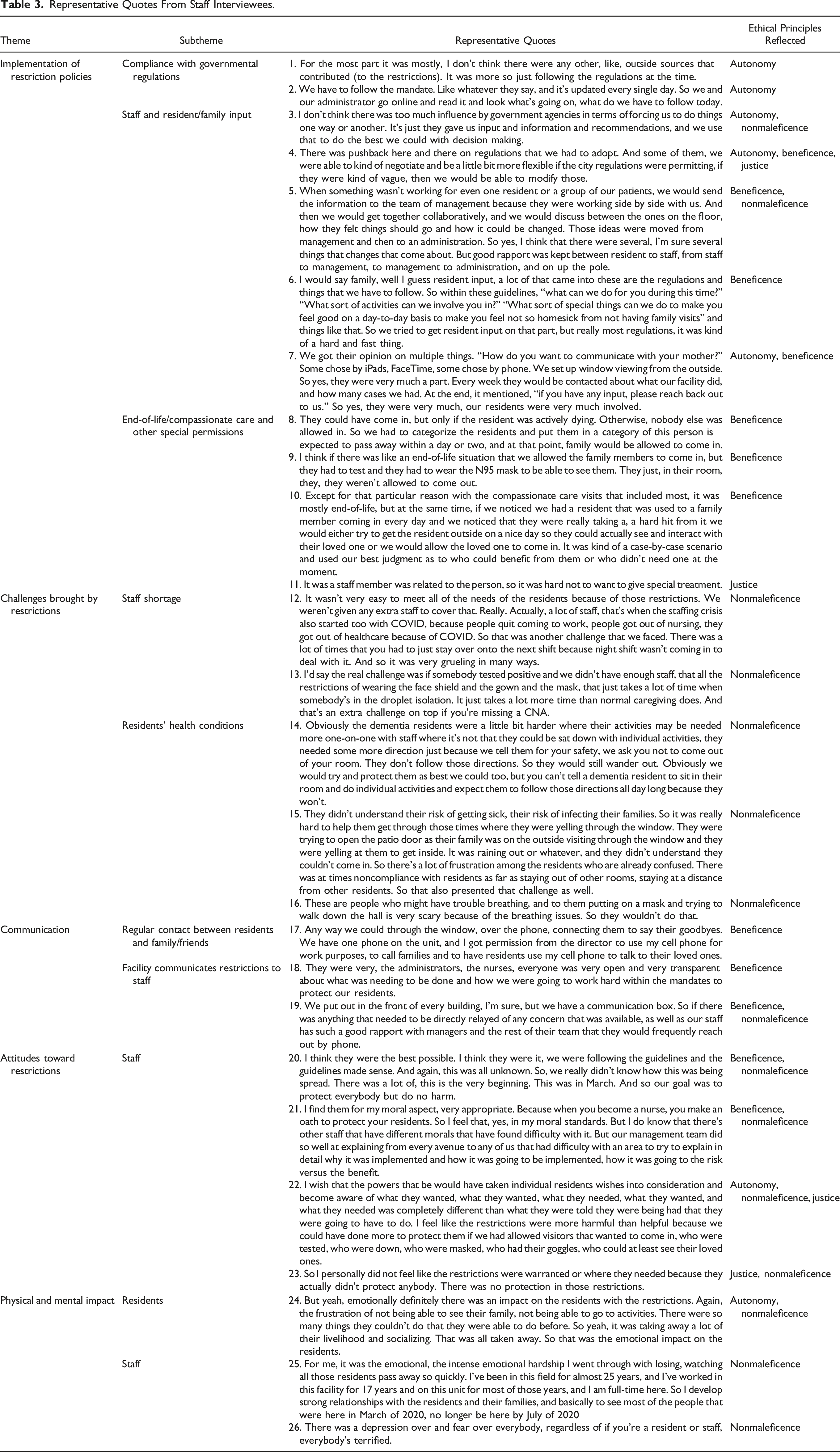
Representative Quotes From Staff Interviewees.
Representative Quotes From Resident/Family Interviewees.
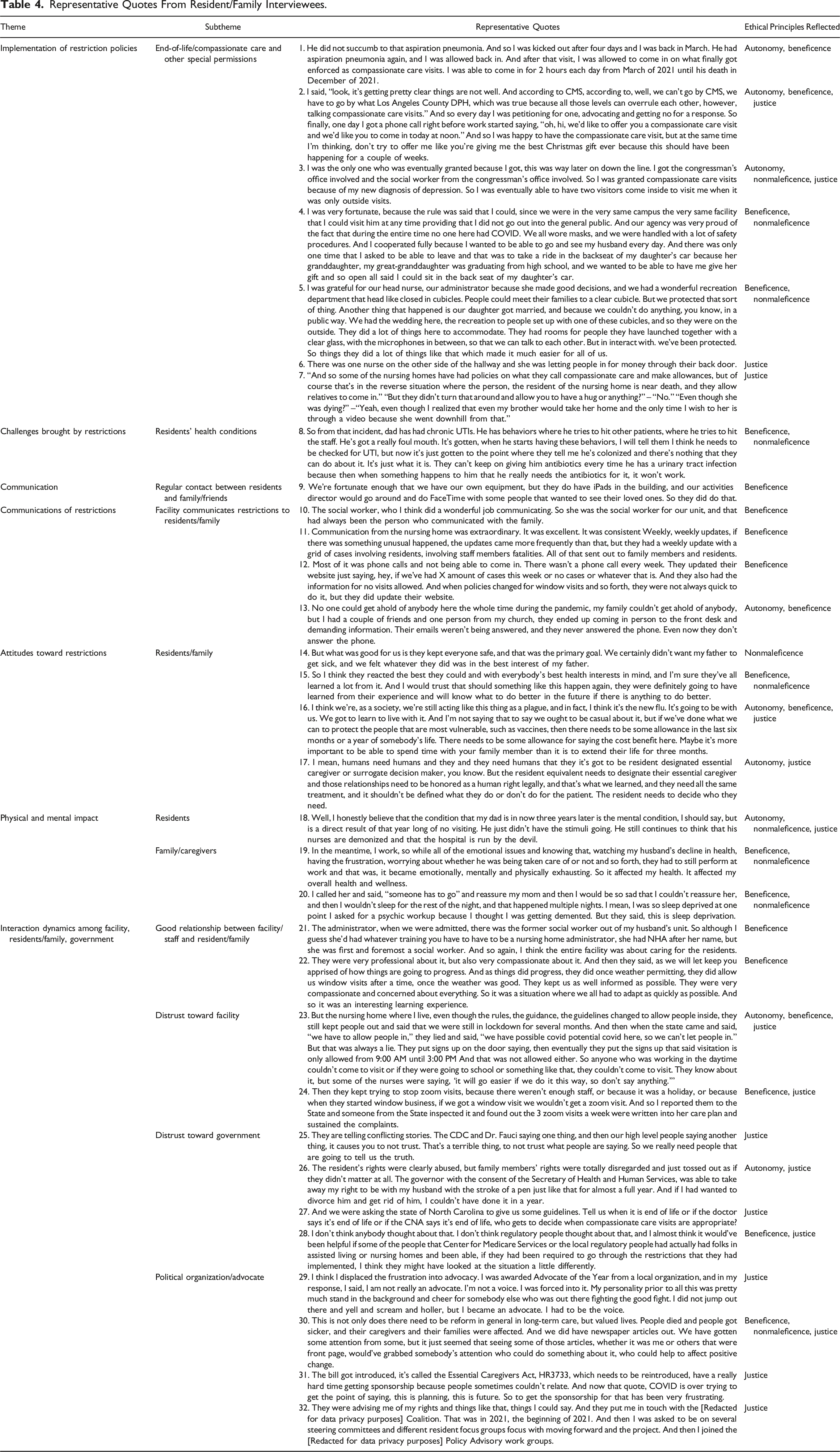
Most of the staff and resident/family member interviewees reported that the facilities allowed end-of-life visits, or compassionate care, though usually the number of visitors, the specific protection procedures, and how to determine the need for compassionate care were subject to facilities’ decisions (Table 3, Quotes 8–9; Table 4, Quote 1). Some nursing home staff reported that facilities occasionally allowed other special exceptions depending on the situation, for example, if a resident was “in absolute need of family support” (Table 3, Quote 10), which could be due to extreme mental distress, if residents or family members fought to allow a compassionate visit or petitioned through government agencies (Table 4, Quotes 2–3), or if the facility had no COVID-19 cases throughout the entire period (Table 4, Quote 4) or had special visitation conditions (Table 4, Quote 5).
However, special accommodations were occasionally made because residents or their family members were acquainted with staff, or they bribed staff members with cash. Sometimes these actions were deemed “injustice.” One staff interviewee said that a staff member in her facility was related to a resident, so “it was hard not to give special treatment” (Table 3, Quote 11). One resident told us that she witnessed a nurse in her facility who “was letting people in for money through their back door” (Table 4, Quote 6).
One special case brought up by a resident was when the facility’s policy did not allow residents to leave to visit their family, an exception was made to permit a resident to be taken to see a family member who was in an end-of-life situation; this was the obverse of the typical end-of-life policy in which family members are allowed to visit a dying resident (Table 4, Quote 7).
Perceptions of the Implementation of COVID-19 Restriction Policies
Residents/family members were about evenly divided in their assessment of the pandemic restrictions; nine out of twenty considered the restrictions appropriate, while the other half considered them inappropriate and overly restrictive. Those in the former group mostly saw the restrictions as according with the principle of beneficence, even though they recognized that autonomy was sacrificed to some extent. Explaining their thinking, residents/family respondents in this group stated that the restrictions “keep their loved ones alive” and were “in the best health interest” of residents, especially during the early stage of the pandemic when little was known about the severity, transmission, or contagiousness of COVID-19 (Table 4, Quotes 14–15).
Among residents/family respondents who considered the policies to be overly restrictive, doubts were expressed about whether the policies respected the nonmaleficence principle: the benefit of protecting people against the virus seemed to be outweighed by the harms created by the restrictions, especially for residents who were already at a late stage of their life, who might feel “it’s more important to be able to spend time with family members than it is to extend their life for three months” (Table 4, Quote 16). A handful of residents/family members who held negative perceptions of the policies said that autonomy was not respected in the restrictions’ implementation. They also believe that most of the restrictions violated the principle of justice: they should have the basic right to make visitation/activity decisions for their loved ones. One family member said that “it’s got to be the resident-designated, essential caregiver or surrogate decision maker” who makes these decisions, and the “need to designate their essential caregiver” should be honored as “a human right legally” (Table 4, Quote 17).
A similar half–half pattern was found among staff members in terms of attitudes toward the restrictive policies. Some felt that the restrictions were “the best possible” means at the beginning of the pandemic to “protect everybody,” weighing “risk versus benefits” (Table 3, Quotes 20–21). Others found the restrictions “were more harmful than helpful” and “actually didn’t protect anybody” because of their perceptions of the actual effects on residents and their families (Table 3, Quotes 22–23). Similar to the views of residents/family members, some staff interviewees also believed it was important for residents/family members to make decisions for themselves, especially for those who were already approaching the end of their lives.
Residents’ Complex Health Conditions Exacerbated the Challenges
Even resident/family and staff respondents who accepted the need for the restrictions reported ways that they exacerbated the challenges of providing residents with the care they needed. Since communal activities and congregate dining were prohibited, the staff had to spend more time attending to residents’ needs individually. The overwhelming burden of work and low morale had the result that “people quit coming to work, people got out of nursing, they got out of healthcare because of COVID,” which made it even more difficult for the remaining staff to provide care (Table 3, Quotes 12–13). Moreover, as most staff (17/20) and residents/family members (16/20) noted, residents’ medical conditions complicated the implementation of the pandemic policies. Many older residents living in nursing homes have cognitive problems such as dementia, which made it difficult to implement restrictions, since “you can’t tell a dementia resident to sit in their room and do individual activities and expect them to follow those directions all day long because they won’t” (Table 3, Quote 14). Another staff member noted: “they didn’t understand their risk of getting sick, and their risk of infecting their families” (Table 3, Quote 15). Other medical conditions, such as chronic obstructive pulmonary diseases, made it challenging for residents to wear protective equipment. As one study participant explained: there were residents “who might have trouble breathing, and to them putting on a mask and trying to walk down the hall is very scary because of the breathing issues” (Table 3, Quote 16). Participants also noted that the COVID-19 restrictions made taking care of patients with conditions such as frailty, hearing problems, vision problems, developmental disabilities, urinary tract infections (Table 4, Quote 8), internal bleeding, stroke, Parkinson’s Disease, and pancreatic cancer increasingly difficult. Beyond the physical challenges that such medical conditions created for the staff and residents, they also complicated the process of weighing potential benefits against potential harms, as the principles of beneficence and nonmaleficence require when making decisions.
Communication and Connection Between Residents and Their Family Members Were Significantly Impeded
During the period that the strictest visitation restrictions were in place (March–May 2020), residents depended on devices such as mobile phones, iPads, and laptops to make calls or Facetime with their family members. Nearly all nursing home staff and resident/family member respondents reported that their facility provided some tools to facilitate communication between residents and their family members, including phone calls, window visits with walkie-talkie equipment, iPad/tablet/monitor for video chats using apps such as Zoom or Facetime, outdoor visits if residents were well enough, exchange of paper messages, and visits using temporary visiting zones or cubes that the facility set up, some with Plexiglass panels (Table 3, Quote 17; Table 4, Quote 9). Ironically, the use of such technologies often created additional challenges. Many residents had a difficult time using these technologies and needed help from staff members. Due to the staff shortages, it was difficult for staff members to help residents maintain frequent Zoom visits with their family members. One resident’s family member reported that “they [staff members] kept trying to stop Zoom visits, because there wasn’t enough staff, or because it was a holiday, or because when they started window visits, if we got a window visit we wouldn’t get a zoom visit” (Table 4, Quote 24).
Of course, the barriers to residents maintaining normal supportive interactions with their families went beyond technological difficulties. Especially, for patients with vision or hearing problems, physical touch was described as being much more important, and the absence of in-person visits was a huge detriment. Staff faced particular problems with dementia patients who found it difficult to understand why physical visits were not possible (Table 3, Quote 15).
Perceptions of the Sufficiency of the Communication Regarding Policies
Perceptions of how the restrictions were communicated were mixed among our study participants. Approximately half of residents/family members (11/20) stated that they were satisfied with the nursing home’s communications about the restrictions (Table 4, Quotes 10–11), but about a third (6/20) expressed negative feelings (Table 4, Quotes 12–13), noting that they were upset that facility was not timely or transparent about policy changes, provided them with updates on the restrictions infrequently, and did not respond well to their requests for information.
Conversely, staff members, in general, did not have strong negative feelings about the way their facility communicated with employees regarding changes in the restrictions and other policies. 13 of the staff respondents explicitly voiced satisfaction with the facility’s communications, saying, for example, “the administrators and the nurses were very open and transparent about what needed to be done and how to work hard within the mandates to protect residents” (Table 3, Quotes 18–19).
Adverse Effects on the Well-Being of Residents, Family Members and Nursing Home Staff
Nursing home staff and residents/family members all reported that the restrictions had significant effects on the quality of life, and the physical, cognitive, and psychological health of residents. All the staff participants reported that the restrictions led to decreased emotional, spiritual, or psychological well-being among residents, and approximately half (11/20) reported functional health decline among residents as a result of their being confined to their rooms and prevented from participating in communal activities. Similarly, nearly all of the residents/family participants (18 out of 20) reported moderate to heavy decline in the emotional, psychological, or spiritual well-being of residents. More than half (13/20) reported functional health decline among residents. One staff member said that “emotionally, definitely, there was an impact on the residents with the restrictions,” caused by “the frustration of not being able to see their family, not being able to go to activities” (Table 3, Quote 24). She thought that the inability to do many of the things that residents had been able to do before “was taking away a lot of their livelihood” (Table 3, Quote 24). One family member noted that she believed that the unstable mental condition of her relative in the nursing home was a direct result of the policy of no visits which the facility kept in place for a year. She reported, “he continues to think that his nurses are demonized and that the hospital [and nursing home] is run by the devil” (Table 4, Quote 18).
Residents/family members also reported that the emotional, spiritual, or psychological well-being of the family members was significantly affected, primarily because of the anxiety or fear brought on by being separated from their loved ones. Most of the nursing home staff (16/20) also noted that they felt that family members were stressed and anxious about the separation and inability to visit their loved ones. One said restrictions affected her overall health and wellness, and “it became emotionally, mentally, and physically exhausting,” to watch her husband’s decline in health, “having the frustration, worrying about whether he was being taken care of or not” (Table 4, Quote 19). Another family member said that she suffered from severe sleep deprivation because she was so distressed that she could only call her mom by phone and could not reassure her mother about anything she needed (Table 4, Quote 20).
Likewise, staff members stated that they experienced declines in their emotional, psychological, or physical health. Almost all (15/20) staff participants reported that they or their colleagues experienced mental health declines due to the intense workload that the restrictions created, depression and fear created by isolation, the emotional difficulty of watching residents suffering or dying, the tensions they had to manage in their relations with family members, and their own concerns about being affected by the virus (Table 3, Quotes 25–26).
Effects on Relationships Between Facility Staff and Residents/Family Members
Among our interviewees, about half of the residents/family members (11 out of 20) maintained good relationships with their facility’s staff members. Among this group, the respondents were generally supportive of the facilities’ restrictions and trusted the protective measures being put in place, noting that “the entire facility was about caring for the residents” (Table 4, Quote 21), and “they were very compassionate and concerned about everything” (Table 4, Quote 22). However, some residents/family members expressed distrust toward the facilities due to the lack of regular communication and perceived misconduct of staff members or administrators. For example, one resident believed that the facility intentionally chose not to disclose changes in visitation rules and perceived that the facility lied about their COVID cases to the government so that they could keep shutting down visitations because “it will go easier if we do it this way” (Table 4, Quote 23). Family and residents also expressed negative feelings about their perceptions of the dereliction of the caring duties by nursing home staff, such as being unable to maintain regular contact between residents and their families (Table 4, Quotes 24), being inattentive to residents’ health changes, and being unresponsive to residents’ needs. Family and residents also expressed that they were unable to voice their needs and have flexibility in the restrictions when needed. Others felt that staff were careless about their own protective measures.
Among those who thought restrictions inappropriate, some residents/family members also expressed explicit distrust (7 out of 20) toward the government in making restriction guidelines and the ability to solve problems or make changes. For example, one family member stated that the public voices were too conflicting (Table 4, Quote 25), saying that “the CDC and Dr. Fauci saying one thing, and then our high-level people saying another thing, it causes you to not trust.” One family member believed that “residents’ rights were abused”, and “family members’ rights were totally disregarded and tossed out” (Table 4, Quote 26). One noted that the ambiguities in government guidelines brought trouble. For example, one stated that it was challenging to determine what constituted an end-of-life situation and whether an end-of-life case was decided by what the doctor said or the certified nursing assistant said (Table 4, Quote 27). Another family member believed that regulators did not really think about the day-to-day situations happening in nursing homes, stating “it would’ve been helpful if some of the people that CMS or the local regulatory people had actually had folks in assisted living or nursing homes and if they had been required to go through the restrictions that they had implemented,” “they might have looked at the situation a little differently”(Table 4, Quote 28).
Some residents/family members responded to the restrictions by participating in advocacy, including writing petitions to the state government, talking to the media, forming coalitions with other long-term care facility residents and family members, and advocating for enacting new laws. For example, some residents advocated for the introduction of a federal bill called the Essential Caregiver Act, HR3733 (Table 4, Quotes 29–32).
Discussion
Our study provides insights into the implementation of restrictive policies in nursing homes during the COVID-19 pandemic and how they were perceived by different stakeholders. Although government guidance, both from CDC and CMS at the federal level and from state and county health departments, shaped the response of nursing homes to the COVID-19 pandemic, some variation existed between facilities regarding the policies and their implementation, and the differences increased over time as more means of treating and preventing infections emerged. The policies implemented by most of the nursing homes in our study sample seemed to our respondents to place very strict restrictions on visits by persons external to the facility and on contacts among residents. More than half of our staff interviewees and half of our resident/family interviewees believed such restrictions were inappropriate, and created numerous challenges to staff and family members in responding to residents’ needs, especially given the residents’ complex health conditions. Visitation restrictions significantly impeded communication and connection between residents and their family members, and many residents and their family members felt that the facilities’ transmission of information about the restrictive policies was slow and insufficient. Restrictions negatively affected the emotional and physical health of residents, their family members, and staff members. Though some residents/family members maintained continued good relationships with facility staff during the period of restriction, many experienced a growing sense of distrust and neglect, leading to heightened tensions between residents/family and facility.
Our interview findings compared perspectives from staff and residents/family members and highlighted the relatively higher dissatisfaction of residents/family members with restrictions and facilities’ actions compared to the perceptions of nursing home staff. This difference appears both in the pre-interview survey’s scoring of the extent to which the facilities met their ethical obligations to residents and their families and in our qualitative data from the interviews themselves. The ratings given by staff respondents on respect for the principles of beneficence, nonmaleficence, and justice in the treatment of residents were generally higher and more uniform (i.e., distributed over smaller ranges) than the ratings given by residents/family members.
Nursing facilities responded not only to governmental requirements but also to the significant risk posed to their resident populations, as evidenced by early deadly outbreaks like the one in a Washington State nursing home. Motivated by obligations to residents, staff, and facility sustainability, nursing home leaders implemented necessary measures to curb the spread of the virus. Our interviews highlighted the deep commitment of many staff members to their ethical duties of prioritizing residents’ interests and preventing harm. The duties of beneficence and nonmaleficence were translated into preventing contact between residents and everyone else. The principle of justice modifies residents’ exercise of their autonomy when the choices they wish to make—to mingle with other residents or to have visitors—could endanger the welfare of other residents and the staff.
Residents/family members expected better care during stressful, isolating times, while staff struggled due to ongoing shortages. Tension arose when residents/family members were dissatisfied, yet staff, feeling defensive, believed they were doing their best. COVID-19 regulations worsened conflicts, leading to verbal aggression toward staff. These conflicts also highlighted a power disparity between family members/residents and facility staff enforcing public health restrictions mandated by federal/state/local governments. Individual voices were often sidelined during the crisis as high-level policies prevailed. The policy advocacy group in which some of our family/resident interviewees participate reveals the potentially significant role of “Family Councils,” which function as independent and self-determining groups of nursing home residents and their families. A well-structured Family Council could play a mediating role in interpreting governmental policies into operational measures for facilities and serve as a conduit for advocating more pragmatic policymaking.
Both staff interviewees and residents/family member interviewees in our study believed that the ethical principle of autonomy of residents/family members was sacrificed to reduce consequences such as mortality and morbidity. Many of them perceived that the harm had far exceeded the benefits. Several participants believed that some universally applied regulations did not take patients with special health conditions or special needs into consideration, thus failing to respect ethical principles. Even though during the implementation process, most facilities and staff members made efforts to balance ethical considerations and follow regulations, it was still widely perceived that those restrictions were inappropriate.
Our study points out the significant deficiencies in policymaking during the COVID-19 pandemic and opportunities for improvement. As reflected by the voices of our study participants, more openness, flexibility, and explicit consideration of harms and benefits are needed during public health emergencies. Future policymakers should continue making efforts to minimize risks but also to maximize autonomy, beneficence, nonmaleficence, and justice when possible. Interviews revealed that currently, no formal mechanism was present or at least not commonly available for the voices of the affected communities to be heard, which prevented important discussions from happening. During public health crises, those who are affected most negatively, including staff, residents, and informal caregivers, especially in the case of nursing homes should be more explicitly involved in policymaking.
Limitations
Our study has several limitations. First, we recruited our nursing home staff and resident/family member participants from the 402 facilities that responded to our previous survey on COVID-19 restrictions (Xu et al., 2024). These facilities may be biased toward those that are willing to disclose information and may not be representative of all the nursing homes across the nation. Second, while we strove for diverse perspectives by restricting our interviews to no more than two interview participants from the same facility, participants were not selected randomly, so our results may not be generalizable to all residents, family members, and staff or U.S. nursing homes. However, the findings may still be transferable since they rely on perceptions of conditions and experiences across many different nursing homes in all regions of the country. Future work might study the perspectives of affected groups using a large-scale survey based on the findings reported here. Interviewing family members instead of residents who have passed away or suffer from cognitive impairment doesn’t directly capture the experience of living through the pandemic in a nursing facility under such conditions. However, we observed that family respondents often relayed residents’ statements and maintained close contact with their relatives in the nursing home both before and during the pandemic, within the constraints of the restrictions. Not interviewing family members would have restricted our resident respondents to a biased subgroup—those who were still alive three years into the pandemic without impairments hindering their ability to be interviewed. Third, the use of snowball sampling to recruit some of the participants may have resulted in identifying like-minded individuals regarding the COVID-19 restrictions. Finally, although we provided explanations of bioethics terminology in our pre-interview survey, we cannot be sure that every respondent understood the terms in the same way.
Conclusions
During the COVID-19 pandemic, balancing infectious disease control policies restricting visitation and social activities in nursing homes with the well-being of residents, families, and staff was challenging due to uncertainties and risks. In future emergencies, policymakers should prioritize a more holistic understanding of affected groups’ well-being and enhance transparency and flexibility when imposing restrictions to minimize harm. Research may explore policymakers’ roles and attitudes, aiding the development of better practices for nationwide adoption by nursing homes and other facilities.
Supplemental Material
Supplemental Material—Exploring the Impact of COVID-19 Restrictions on Nursing Home Residents’, Families’, and Staff’s Perceptions of Bioethical Principles: A Qualitative Study
Supplemental Material for Exploring the Impact of COVID-19 Restrictions on Nursing Home Residents’, Families’, and Staff’s Perceptions of Bioethical Principles: A Qualitative Study by Yimin Ge, Shengjia Xu, Alexander Capron, Michelle S. Keller, and Jakub P. Hlávka in Journal of Applied Gerontology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Greenwall Foundation, New York, NY, USA.
Ethical Statement
Data Availability Statement
Data in this study is not openly available. All interviews are confidential, and access to raw data is limited to our research team members in accordance with our agreement with interview participants.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.