
Abstract
Patient perspectives are essential to understand healthcare disparities such as low rates of advance care planning (ACP) among adults with limited income. We completed twenty semi-structured interviews using purposive and snowball sampling. Initial and final themes emerged from inductive inclusion of recurring codes and deductive application of the cumulative disadvantage theory. Four themes emerged: (1) structural, (2) life-stage, (3) social stressors and resources, and (4) individual stress responses and ACP readiness. ACP resources among participants included positive structural and social support and previous familial death experiences that were mitigated by stress avoidance and competing priorities. Structural resources and healthcare stressors should be addressed with policy and research to improve continuous healthcare participation and support early, comprehensive ACP.
• We used the cumulative disadvantage theory to provide a dynamic description of healthcare and advance care planning stressors and resources for a socioeconomically deprived community. • Specifically, ACP may be limited by lifetime healthcare coverage gaps, public benefit denials and delays, and personal and social stressors. • While policy-level solutions will be essential, we found that individual and familial resilience may facilitate ACP.
• Clinician awareness of existing stressors such as lack of care coordination should motivate ACP initiation by taking a personalized and compassionate approach. • Future research should explore the intersection of coping strategies for overlapping stressors with ACP stress to develop tailored intervention and implementation approaches. • Future policies should simplify ACP procedures to reduce wait times in accordance with expanding and simplifying access to Medicaid, Medicare, Social Security Disability Income, and Housing, among other essential social services.What this paper adds
Applications of study findings
Introduction
Compared to those with high income, older adults with low income are 26–33% less likely to do any advance care planning (ACP) (Inoue, 2016; Nouri et al., 2020). Compared to those with high income, these adults are more likely to experience healthcare and health challenges that underscore the importance of early ACP but also challenge the development and sustainment of preventative health behaviors, that is, ACP. Members of this community are more likely than those with high income to be uninsured or underinsured during middle adulthood, contributing to preventative healthcare avoidance apart from emergency care (Testa et al., 2022). Additionally, this population is at increased risk for early disease onset, multiple co-morbidity development, and premature mortality from mechanisms of chronic stress (Myers, 2009), necessitating the exploration of ACP barriers and facilitators that may be addressed by early intervention.
Optimal ACP consists of the continuous process of learning, communication, and preparation of close social ties that begins in early adulthood and requires sufficient social support to ensure adequate preparation for times of cognitive incapacity, but structural and individual-level barriers limit optimal ACP (Fried et al., 2009; Malhotra et al., 2022). The ideal ACP process includes opportunities to communicate and document life-sustaining measure preferences, define care goals and quality of life values, and prepare healthcare decision-makers for the difficult in-the-moment decision-making during a health crisis. Older adults with limited income and overlapping marginalized identities faced barriers to optimal ACP such as unmet basic needs, conflicting religious beliefs, lack of knowledge, limited social support, medical mistrust, prognostic uncertainty, and healthcare staff with insufficient training and/or self-efficacy (Coogan et al., 2022; Hong et al., 2018; Kaplan et al., 2020). Facilitators included previous death-related experiences, trust, adequate social support, and ACP facilitator communication skills (Brean et al., 2023; Hong et al., 2018). However, little is known about how ACP factors may evolve over the lifespan. We aimed to address this knowledge gap by exploring the experiences of community-dwelling older adults with low income to understand what early, mid-life, and later-life barriers and facilitators may lead to low ACP participation in this population.
Methods
Design
We chose a qualitative descriptive design (Sandelowski, 2000). Our research followed the standardized qualitative reporting guidelines (Consolidated Criteria for Reporting Qualitative Studies) (Booth et al., 2014). Vanderbilt University’s Institutional Review Board approved all study protocols and practices (IRB 210905).
Theoretical Framework
The cumulative disadvantage theory holds that socioeconomic inequities among older adults result from the compounding exclusion from financial, material, healthcare, and social resources over time (O'Rand, 1996). The core constructs that guided our final thematic development included the structural context, the historical domain, and the individual. The purpose of this theoretical application was to identify potential factors for future study but did not extend to a complex analysis of the underlying mechanisms of ACP inequities. The use of theory supported the research aim to explore experiences by life-stage, interview guide (prompts to discuss life-stage patterns (e.g., childhood)), and qualitative analysis (situating final themes within the core theoretical constructs).
Sample and Recruitment
We purposively and snowball sampled from six community sites in Nashville, Tennessee, to ensure that most participants identified as Black or African American, but also varied by gender and age. Inclusion criteria included (1) an annual, individual income of less than US$20,000/year, (2) age of ≥50 years, (3) independent living status, and (4) no severe hearing, visual, or language barriers to study tasks. Among 22 individuals we approached, twenty completed a qualitative interview and two declined due to a lack of interest.
Recruitment locations were selected based on geographic position and use by the population of interest. These non-healthcare sites included three affordable housing complexes, a food pantry, a resource center, and a senior program at a community center. The primary investigator (PI) (CCK) visited recruitment locations for face-to-face recruitment and flyer distribution. Interested individuals were contacted in person or by phone to screen for eligibility, describe the study, and schedule interviews (November 11, 2021–June 9, 2022). Recruitment continued until we achieved data saturation—no novel data emerged from the interviews.
Data Collection
Interview Guide.
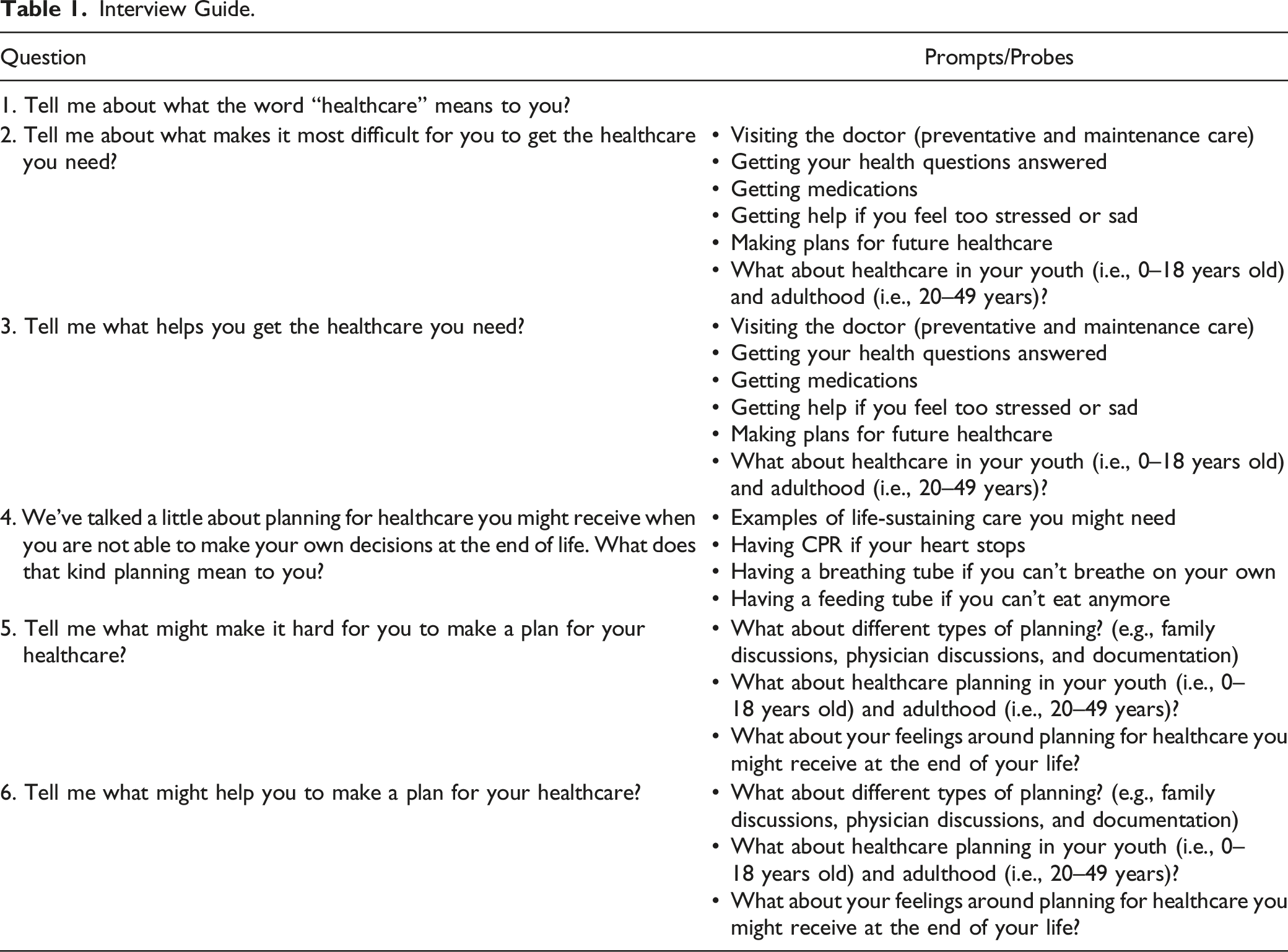
Most interviews were one-on-one. One participant’s wife consented and contributed per his preference, but her data were excluded. After each interview, each participant received a US$25 gift card incentive and the PI recorded field notes about the interview context. Audio recordings were professionally transcribed by Rev.com. Interviews lasted between 21.0 to 82.5 minutes (median = 47.5).
Data Analysis
We reviewed transcripts (N = 20) using thematic analysis to develop a hierarchical coding system, ensuring a close relationship between the data and emerging themes and a thorough understanding of each theme’s meaning (Maguire & Delahunt, 2017). Two trained, independent coders (CCK and ACR) coded individual lines of data and then divided codes into groups according to the interview guide questions. Any coding discrepancies were resolved following an iterative process, strengthening coding consistency. Initial inductive phases of open, line-by-line coding of data were followed by grouping of codes using the interview guide questions to form a single codebook (e.g., ACP barriers). During the initial and subsequent phases of analysis, initial themes became evident upon re-review and collapse of the code groups using a combination of inductive grouping of the data (e.g., social stressors) and the deductive application of the theoretical framework (e.g., structural stressors). Major themes emerged from a final review and reiteration of the initial themes and consideration of the theoretical framework (themes: life-stage, structural, and individual factors). Quotes were then selected that supported and corroborated each theme. Excel and SPSS 28 were used to analyze and manage data.
Results
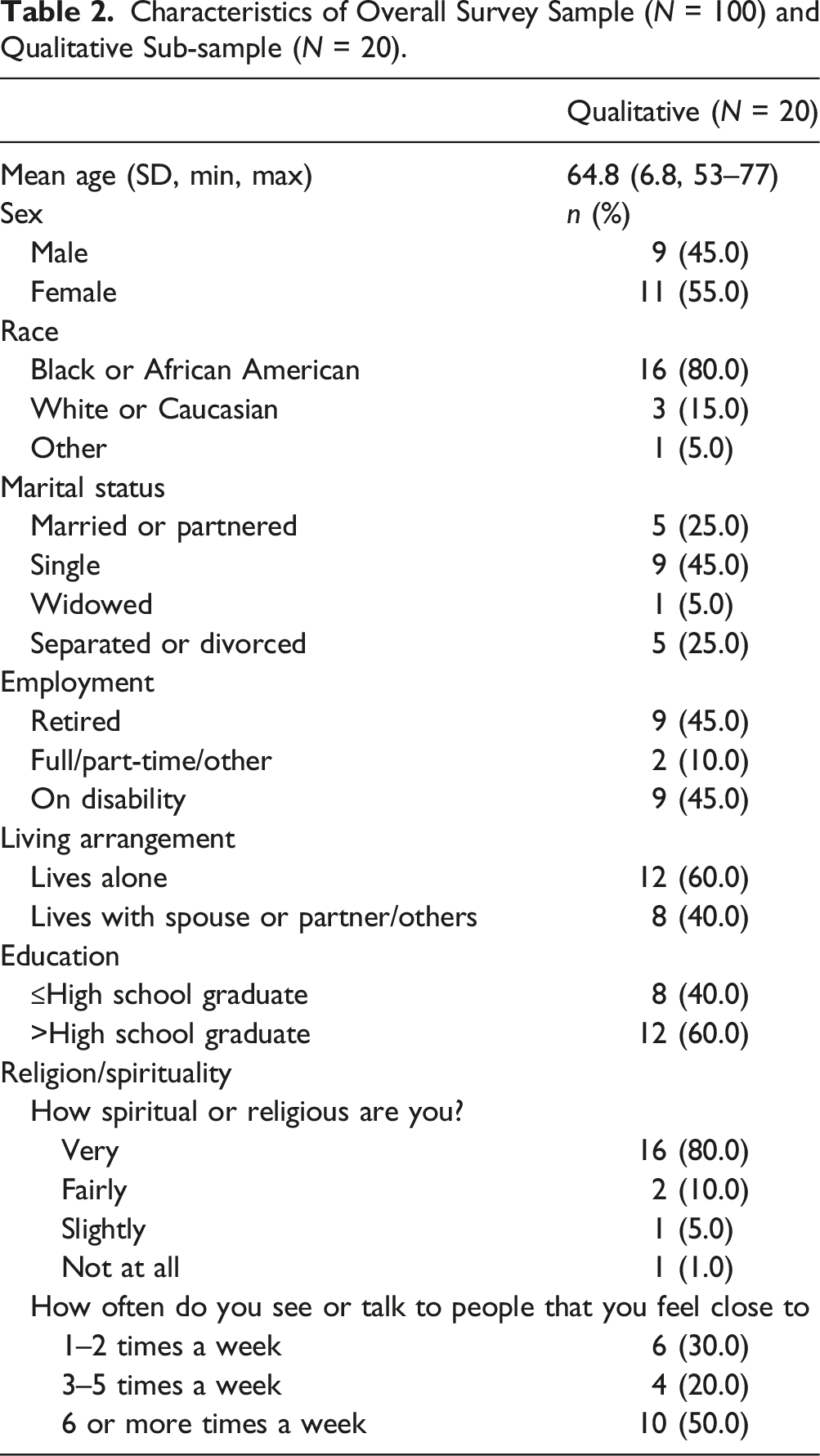
Characteristics of Overall Survey Sample (N = 100) and Qualitative Sub-sample (N = 20).
Thematic Analysis of Participant Interviews
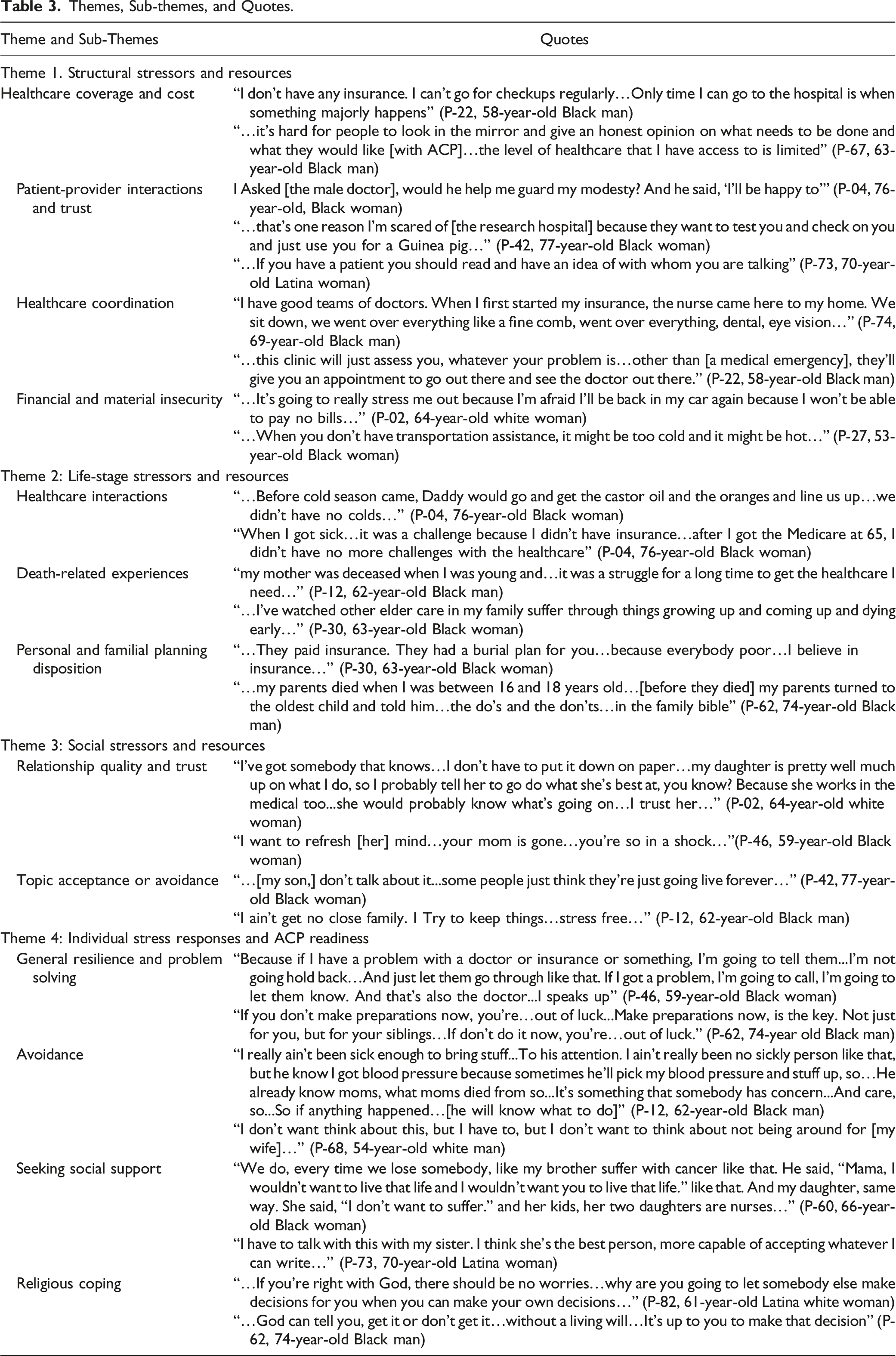
Four themes captured a complex picture of stress and ACP readiness among older adults with low income (Figure 1, Table 3). The first three themes consisted of domains of stress and resources: (1) structural; (2) life-stage, and (3) social. The final theme included: (4) individual stress responses and ACP readiness. Initial analysis phases included the ACP process as a theme, finding that although most participants informally identified a healthcare decision-maker, all varied in the depth and extent of ACP communication and documentation. Such participation included universal life insurance planning, some level of family discussion, some informal documentation (letter-writing), and very minimal formal documentation (advance directive completion) or discussion (physician). Rather than develop a separate theme, further analysis promoted the inclusion of ACP behavior types within each of the four final themes. Each theme on the left-hand side of the figure represents stressors and/or resources that affect coping with ACP (on the right). The social domain affects life-stage stressors and resources, and vice versa, by contributing to familial planning dynamics, communication, and contributing to ongoing life experiences. Structural stressors and resources also have a bidirectional relationship with the life-stage domain, particularly the healthcare interaction sub-theme, such that the healthcare quality and insecurity are age-dependent. Each coping type on the right is affected by these different thematic domains: 1. General resilience and problem-solving include the individual ability to adapt to stressors combined with robust resources across domains, 2. Avoidance was typically a gendered coping strategy and was influenced by a variety of stressors such as the lack of social support, lack of healthcare support, and competing financial concerns, 3. Those who sought social support were also supported by family and, sometimes, healthcare providers, and 4. Religious coping was influenced primarily by individual beliefs based on the life-stage domain (death-related experiences and familial planning practices). The dashed lines indicate possible relationships for future study but do not indicate confirmed mechanisms. Themes, Sub-themes, and Quotes.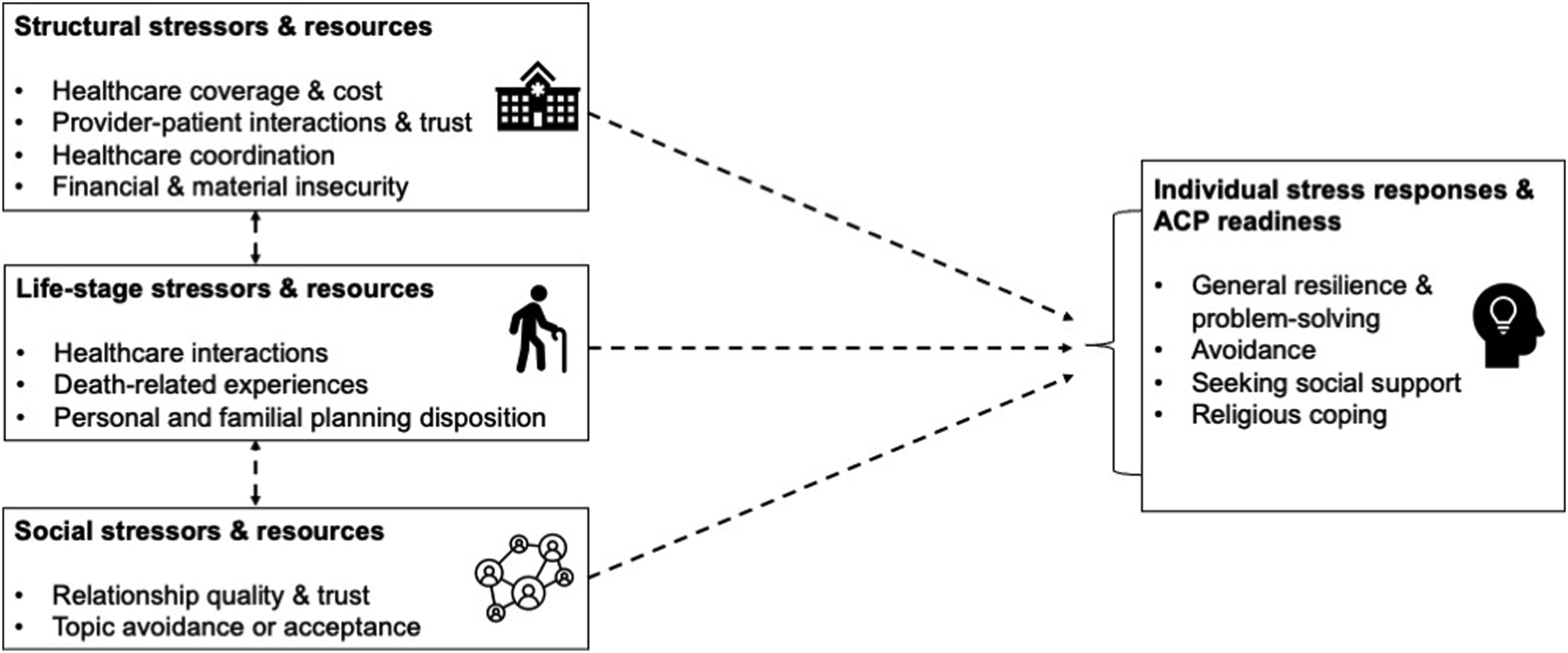
Theme 1. Structural Stressors and Resources
This theme referred to institutional stressors and protective factors that complicated or simplified preventative healthcare participation such as advance care planning. Participants who were uninsured or underinsured experienced the stress from high healthcare costs and less healthcare access, resulting in fewer ACP opportunities. Stressors included navigating healthcare without financial means, the reality of care refusal that delayed care, and balancing healthcare costs against other essential needs. Participants also dealt with numerous categories of out-of-pocket costs, such as copays, co-insurance, and medications, which resulted in delaying, limiting, or avoiding care altogether. These stressors followed a cumulative pattern of disadvantage, resulting in isolation and no one to turn to for health and healthcare decision-making needs: Some people self-medicate…Don't have the money to go see the doctor…when something do go wrong, it's way wrong before they get some help. It's out of control…they suffer in silence… (P-22, 58-year-old Black man).
Generally, insufficient health insurance coverage and a lack of primary care reduced preventative checkups and proactive planning. These issues contributed to fewer opportunities to formally discuss and document ACP with an established provider: “I don’t have a primary doctor, so there’s no one to consult” (P-22, 58-year-old Black man). Additionally, participants internalized the stress of chronic underinsurance, which resulted in a lack of confidence that they would receive the care they wanted during times of cognitive incapacity because it surpassed the care they could afford.
Alternatively, trusted provider and provider continuity was a resource that created a safe environment for ACP. Participants emphasized the importance of provider compassion, empathy, and respect, “She is a very good listener…If you explaining something, they in tune” (P-74, 69 year-old Black man). Conversely, stressful experiences included careless and disrespectful providers who did not adequately prepare for appointments. Harmful healthcare experiences promoted feelings of dehumanization and fear as some participants felt out of control or worried about being treated like a “guinea pig.” However, trusted, established providers that prioritized ACP served as an essential resource to create ACP opportunities, “The doctor asked me, did I have a living will…he gave me the necessary forms. I filled them out…and gave it back to him” (P-62, 74 year-old Black man).
Efficient and reliable healthcare coordination provided participants with stable resources, but a lack of coordination contributed to stress and uncertainty. Participants characterized the advantages of comprehensive care coordination via insurance, which included 24 h telephonic support for health concerns and logistical support for transportation to appointments. Participants also identified community health resources that triaged complex social and health needs, adjusted costs to income, and made appropriate referrals and follow-ups. Participants communicated that the system of ACP documentation did not reflect effective and efficient care coordination, follow-up, and document retention: “they give you a lot of papers and different stuff…[the advance directive] just get lost in the papers…” (P-04, 76-year-old Black woman).
Financial and material insecurity was a structural stressor that limited healthcare and ACP opportunities and prioritization, but also motivated participants to plan with life insurance to prevent financial burdens for family members. Public benefits such as social security, food stamps, and Medicare provided a resource to participants, but constantly shifting policies left participants in fear of benefit loss. Lack of transportation was the most discussed stressor regarding healthcare appointments. Public transportation resources varied with age and disability. Participants experienced the stressors of long walks to bus stops, walking in extreme weather conditions and temperatures, and allocating additional travel time to get to appointments. Housing insecurity was a major stressor that superseded the concerns of proactive planning, “…thing that worries me the most is to wake up and not knowing where I’m going to be able to lay my head…” (P-66, 58-year-old Black man). However, the stressor of financial insecurity motivated most participants to proactively plan with life insurance to prevent financial strain for family members, “…if you don’t have insurance, you make your family suffer…” (P-60, 66-year-old Black woman).
Theme 2. Life-Stage Stressors and Resources
This theme referred to the recollection of personal exposures to healthcare, death-related experiences, and familial planning over three life stages that either overwhelmed people with stress or protected them by enhancing their ability to cope and plan for times of cognitive incapacity.
Healthcare interactions across life stages shaped personal conceptions of healthcare participation underpinning later-life healthcare and ACP participation. Most participants had reliable health insurance resources in childhood and older adulthood but they identified stressful gaps in healthcare access during adulthood. In childhood, some participants recounted memories of addressing health concerns outside of healthcare institutions by relying on the wisdom of older generations and the use of folk remedies (e.g., castor oil and oranges). Childhood was also marked by fewer health problems but, when needed, participants recounted access to affordable options such as community hospitals and sliding-scale payment plans. In adulthood, participants reported healthcare coverage from resources such as public health insurance programs for adults with low income, employer-based insurance, and disability benefits.
Conversely, participants experienced stressful periods with no or insufficient insurance due to working without benefits, living in states that heavily restricted access to Medicaid, and not meeting age requirements for Medicare: “…if you’re over 20 and under 50, there’s no healthcare for you…,” (P-82, 61-year-old Latina white woman). In older adulthood (age 65), participants expressed the newfound security of reliable coverage amid growing health concerns. Still, those with complex health conditions without Medicare continued to experience stress, “the doctor prescribes you something and then you get a letter from TennCare [Medicaid] saying that they don’t pay for that…” (P-66, 58-year-old Black man).”
Death-related experiences across life stages introduced unique stressors that shaped individuals' perceptions of and relationships with death-related decision-making. These experiences influenced the acceptability and motivation for proactive planning. In childhood, participants recounted the stressful, “haunting” experiences of losing beloved caregivers and loved ones. In adulthood, participants witnessed the suffering of dying family members or the premature death of family members. Specifically, these experiences, while stressful, served as a resource to motivate reflection about ACP preferences for quality of life (cognitive status, blindness, independence), life-sustaining measure preferences (do not resuscitate, pull the plug), and motivation to prevent family members from experiencing similar distress from lack of preparation. Notably, women tended to report more experiences of being healthcare decision-makers for family members than men, which may contribute to more acceptance in women and more avoidance in men. In older age, participants with families that had high mortality rates were motivated to actively discuss their wishes with their families and ensure that they were prepared to make decisions during sudden health crises.
Personal and familial planning disposition varied across life stages and determined ACP participation. Throughout stages of life, planning traditions were intertwined with religious beliefs and practices (writing the will in the family bible). Early and mid-life experiences of seeing family leaders prepare for death served as a resource and important life lesson to promote proactive planning such as purchasing life insurance to allay financial burdens on family, “…They had a burial plan for you…because everybody poor…” (P-30, 63-year-old Black woman). However, some participants communicated a lack of open communication or questioning about death-related planning, which reduced family-based coping and learning. During adulthood, participants recalled feeling “invincible” and not seeing the need for proactive planning (retirement, healthcare, long-term care, or ACP). During this time of life, participants rarely sought healthcare save for sudden injuries or illness or new-onset chronic illnesses that developed in their 40s and 50s. However, participants who witnessed active ACP among other family members advocated for ACP earlier in life. Older age brought a readiness for ACP due to achieving milestones (seeing descendants reach adulthood), experiencing more health problems, and acceptance of mortality, “…I know I didn’t come here to stay…” (P-42, 77-year-old Black woman).
Theme 3. Social Stressors and Resources
This theme referred to the quality of one’s social network that either added to the stress of ACP or provided the social resources to participate in ACP. Several participants identified available family members that could advocate for their preferences including children, siblings, and spouses. Beyond available family members, participants described the quality of their relationships in terms of special bonds and respect, denoting the view that the potential healthcare decision-maker was responsible for carrying out ACP preferences during times of stress. Participants with capable healthcare decision-makers expressed trust, confidence, and peace of mind, “I feel comfortable let [my son] make the decision…I trust his judgment…” (P-74, 69-year-old Black man).
Alternatively, participants noted that death was a stressful and undesirable discussion topic for some without adequate social support. Some participants described family members that avoided the topic of death and ACP, because of family members that were emotionally immature or felt “invincible” as if they would never die. Other reasons for topic avoidance included past familial trauma that made discussing loss more difficult, “…We separated [when he was young], now we are together…I understand that for [my son], [the thought of] losing me…would be terrible” (P-73, 70 year-old Latina woman).” Conversely, participants with family members who accepted the topic and embraced proactive planning felt empowered to maintain meaningful and ongoing discussions.
Theme 4. Individual Stress Responses and ACP Readiness
This theme referred to the psychosocial coping strategies developed in response to different types of stressors and resources and the impact on ACP participation. General resilience was evident as participants described adapting to obstacles with problem-solving and determination, “I’ve been homeless…don’t give up that easy...my survival skill…” (P-12, 62-year-old Black man). Regarding ACP, resilient participants described turning toward robust resources such as talking with trusted healthcare providers, counting on previous death-related and planning experiences for insight, and taking steps at the individual level to overcome a lack of social resources (writing letters) and knowledge stressors (searching online or asking healthcare insurance providers for advice for how to complete documentation). Conversely, in some cases, some participants exhibited general resilience and problem-solving to survive in the context of limited resources (healthcare, financial, and material insecurity), but not to discuss ACP. This general resilience focused on the here and now rather than future-oriented decision-making.
Resilience and individual problem-solving enabled the fortitude to adapt to stressful circumstances, but some participants, particularly those who identified as male, still avoided ACP generally or specific ACP types (documentation). One participant named his healthcare decision-maker but avoided discussing care preferences because he viewed it as too stressful and that he was not sick or old enough, “I really ain’t been sick enough to bring stuff...to his attention…if anything happened…[he will know what to do]…” (P-12, 62-year-old Black man). Additional reasons for avoidance consisted of the desire to “keep things stress-free” with family or because of a lack of social resources (no family or estrangement). Other reasons for avoidance included the desire to focus on the bright side of life or because they could not bear thinking about leaving family behind in financially desperate situations. These worries and fears affected the depth and extent of ACP such that some participants wholly avoided ACP of any type while some engaged in certain behaviors (family discussion) and not others (documentation).
Religious beliefs and traditions around planning emerged from life-stage experiences with family and community, and religious beliefs were either a resource to ACP acceptance (free will) or contributed to decisional avoidance (God’s sovereignty over death). In cases where religious beliefs brought comfort with death (being right with God), participants accepted ACP as their God-given responsibility and right. Additionally, the belief in free will enabled ACP acceptance as a recognition that God instills individuals with the power and the ability to be self-sufficient. Alternatively, the belief that making decisions about death was God’s domain precluded ACP, “...if you do something to discontinue life while you’re still breathing…you’re actually taking life because if your time is up…life is going to leave you” (P-93, 70-year-old Black man).
Participants who were motivated to complete ACP expressed the importance of seeking social support from family and, sometimes, healthcare professionals to address ACP challenges. Participants talked about seeking support from healthcare decision-makers through discussion, but also making alternative arrangements with other family members. For instance, participants reached out to more accepting, older family members (siblings, aunts, and uncles) for support with decision-making and to create a secure plan. Other participants conveyed a strong motivation for familial ACP discussions due to continuous familial death experiences. Participants with such death and disease-related experiences had a desire to prepare family members for health crises to prevent additional emotional and decisional distress care preferences are unknown. Some participants described reaching out to healthcare professionals for ACP support when they believed that their family was too emotionally invested to make a rational decision and respect their wishes.
Discussion
We found three domains of stressors and resources that influenced individual stress responses and ACP readiness. Consistent with the literature, our findings highlighted inconsistent healthcare access, the importance of death-related experiences for ACP motivation, and the connection of familial planning disposition with personal ACP behaviors (Hong et al., 2018). To the best of our knowledge, this is the first study to explore ACP stressors and resources for this population within a structural and life-stage context, which will be essential to develop effective policy-driven and patient-centered interventions to correct these disparities. While we found that resources across domains served as protective factors for ACP, multi-level stressors and lack of resources likely exacerbated ACP avoidance and indifference.
Our findings correspond with prior literature that highlights that positive healthcare interactions and trust are an ACP resource (Hong et al., 2018) and the urgent unmet needs of older adults with low income often outweigh future-oriented planning (Coogan et al., 2022; Kimpel et al., 2022; Kaplan et al., 2020). Our work builds on this work by illuminating the pre-retirement stressors and vulnerability created by public health underinsurance and Social Security Disability Income (SSDI) denial, which are far too common. SSDI beneficiaries are also entitled to additional health coverage (Medicaid, Medicare, or both) (Aggarwal, et al., 2022; Donahue et al., 2022). However, restrictive SSDI policies reduce eligibility and correspond with worse mental health outcomes, poverty levels, health inequities, feelings of dehumanization and fear, and arduous wait times (Lee et al., 2020; Simpson et al., 2021; Weaver, 2021). While we did not explore the direct effects of this stress on ACP, a preventative and proactive health behavior, future research should explore how streamlined public benefits procedures may relieve stress, improve healthcare participation, and bolster ACP in this population.
Recent research has highlighted the stress of ACP for patients and healthcare decision-makers across socioeconomic levels (Jimenez et al., 2018; Lipnick et al., 2020) and coping strategies associated with ACP (Miyashita et al., 2023). Our study adds to this literature by focusing on stress, resources, and coping with ACP in this specific population. We found that stressors emerged from structural (lack of consistent providers, financial toxicity, and unmet needs), age-related events (death and gaps in healthcare coverage), and social sources (topic avoidance and lack of reliable social support). Alternatively, we found that robust resources across thematic domains supported personal and familial coping. While recent interventions have introduced mindfulness-based training approaches to ACP (Cottingham et al., 2019), community-level solutions are needed for this population to address multiple stressors and resource insecurity.
Community-based interventions may promote formal ACP in communities that have been marginalized by the healthcare system and experience chronic and complex stressors that require more intensive ACP. Recent community-based research has reported successful lay navigator training with the Respecting Choices program—a comprehensive, systematic ACP training and completion program that promotes systemic, sustained equity (IOM, 2015). This program improved navigator confidence to hold ACP conversations, improved patient self-efficacy, and fewer hospitalizations among those with completed ACP (Fahner et al., 2019). Future research should include early community-based intervention within a comprehensive approach to address multi-insecurity, reduce healthcare gaps, and promote timely ACP among adults with low income.
Additionally, future research should characterize patient and familial coping styles to tailor interventions to address individual (e.g., gendered coping styles) and interpersonal ACP barriers (e.g., relationship trauma). Furthermore, ACP patient education and provider training programs should incorporate trauma-informed, family-centered approaches (e.g., mindfulness training) that advance coping skills to plan for and navigate health crises (Cottingham et al., 2019). Lastly, adverse and positive childhood experiences should be considered to identify previous trauma, understand current coping strategies, and customize ACP interventions and implementation.
Practice and Policy Implications
While there has been recent criticism of ACP effectiveness (Morrison et al., 2021), our findings suggest that ACP empowers patients to prepare for and relieve the burden of familial and provider decision-making during times of cognitive incapacity. ACP should become a regular part of preventative healthcare screenings early in life and earlier in the disease process. This approach ensures that patients have ample time to make informed decisions and update plans as life events and disease status change. Institutional policies should support this practice by allotting time, training, incentives, and resources to promote ACP among healthcare providers. Such changes may include simplified and inclusive forms of formal ACP (e.g., audiovisual) and specialized ACP coaches to reduce provider burden. ACP can also be emotionally charged, particularly for patients and families that have experienced multi-insecurity and traumatic loss. It is crucial to blend coping style assessment with ACP patient education to identify ACP conversations' appropriate timing, intensity, and duration.
Implementing ACP in healthcare settings will require careful consideration of various factors, including the appropriate implementation process, healthcare providers' experience and skill mix, and the needs and experiences of patients and families. One approach is to embed ACP in the context of a secure social safety net, such as a Respecting Choices program based in a Permanent Supportive Housing context (Aubry et al., 2020). This approach ensures that patients have access to the support and resources they need to engage in ACP conversations while also addressing the cumulative disadvantage and trauma experienced by many residents. Successful ACP implementation will ultimately require a collaborative and patient-centered approach that considers each patient and family’s unique needs and preferences.
Government policies at the state and federal levels are needed to reduce financial barriers and incentivize ACP activities, particularly for older adults who do not yet meet the Medicare and Social Security age or work requirements. State governments should review restrictive public benefit regulations (e.g., work requirements). These restrictive policy barriers create competing ACP priorities by the added work that patients need to do secure income, housing, food, and healthcare in a way that makes proactive planning seem unobtainable and superfluous. Medicare reimbursement for one 30-min ACP conversation has reduced ACP inequities, but provider and patient education is necessary to incentivize use (Palmer et al., 2021). Additionally, the current Medicare reimbursement structure should be modified to support ongoing discussions given the changing nature of ACP preferences throughout the life trajectory. This updated reimbursement structure should be replicated with Medicaid. Furthermore, states that declined Medicaid expansion should re-examine this decision to promote population health and patient autonomy (Graves et al., 2020).
Strengths and Limitations
Our study rigor provides a robust picture of ACP factors considering its strengths and limitations (Morse et al., 2002). We did not conduct member checking; however, trustworthiness was supported by a professional transcription service, iterative data review, and transcript authentication with the audio files (credibility). Study findings are limited to similar populations and settings, but transferability was promoted using six recruitment sites, allowing for a diverse breadth of sites and participant demographics. Our findings may not transfer to states that expanded Medicaid, unlike Tennessee. The dependability of the six themes was supported by reaching data saturation across twenty interviews. Confirmability was supported by using an audit trail, independent coding, final theme agreement across a six-author team, and mitigating personal biases using a tested interview guide. Additional strength was achieved by having all the interviews completed by the PI, which strengthened data collection consistency. Personal nursing biases may have been introduced as participants exhibited various health concerns but were reduced by adhering to the formal interview guide structure.
While the cumulative disadvantage theory allowed us to situate our findings within the broad theoretical constructs, we used the original version of this theory. Our data did not allow us to delve deeply into underlying mechanisms. Future work should apply newer versions of this theory and focus on the causal pathways of disadvantage.
Conclusion
Addressing ACP inequities requires structural and historical context to unpack the contributing factors and identify workable solutions. This study illuminated the importance of comprehensive planning among adults with low income, hindered by the competing need to survive multi-level stress and supported by positive coping strategies.
We plan to use community-engaged research to explore and build on existing coping strategies to design intervention bundles to provide social resources and promote ACP among older adults with socioeconomic disadvantage.
Supplemental Material
Supplemental Material - Life-Stage and Contextual Factors of Advance Care Planning Among Older Adults With Limited Income
Supplemental Material for Life-Stage and Contextual Factors of Advance Care Planning Among Older Adults With Limited Income by Christine C. Kimpel, Jana Lauderdale, David G. Schlundt, Mary S. Dietrich, Amy C. Ratcliff, and Cathy A. Maxwell in Journal of Applied Gerontology
Supplemental Material
Supplemental Material - Life-Stage and Contextual Factors of Advance Care Planning Among Older Adults With Limited Income
Supplemental Material for Life-Stage and Contextual Factors of Advance Care Planning Among Older Adults With Limited Income by Christine C. Kimpel, Jana Lauderdale, David G. Schlundt, Mary S. Dietrich, Amy C. Ratcliff, and Cathy A. Maxwell in Journal of Applied Gerontology
Footnotes
Acknowledgments
We thank all our participants and community leaders that supported this work at the different recruitment locations.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Office of Academic Affiliations, Department of Veterans Affairs. VA National Quality Scholars Program and with use of facilities at VA Tennessee Valley Healthcare System, Nashville Tennessee. The VAQS Program in Nashville, Tennessee is supported by and operated within the Veterans Affairs Quality Scholars, Tennessee Valley Healthcare System, Geriatric Research Education and Clinical Center (GRECC). This work was also supported by the National Center for Advancing Translational Sciences (NCATS) Clinical Translational Science Award (CTSA) Program [5UL1TR002243-03]. This project was supported by the Agency for Healthcare Research and Quality (T32 HS026122). The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality.
Ethical Statement
Data Availability Statement
The codebook for this study will be provided, but the data will not be made accessible to protect the anonymity of our participants. This study was not pre-registered.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.