
Abstract
Although allostatic load (AL) is a key concept to reflect physiologic wear and tear from stress, older adults are underrepresented in AL-related research, especially the oldest old (≥80). Further, attenuative factors are often unaccounted for. This longitudinal analysis using data from National Health and Aging Trends Study investigated relationships of AL in 2017 and multi-wave (1) comorbidity accumulation using multilevel Poisson modeling and (2) mortality risk using survival analysis. By year five (2022), each incremental AL increase that older adults (n = 3614) experienced was associated with a 47% increase in comorbidity (p < .001), and a 33% increased mortality risk (p < .001). This research supports a shift to a more proactive, health promotion/risk mitigation paradigm through informing intervention research targeting AL, which is currently scarce. Identifying potentially modifiable and key driving factors influencing the relationship between AL and health among older adults is an important next step to inform intervention design.
• This is the first AL study with updated outcome data spanning COVID-19 years for more relevant, ongoing context of health of older adults. • This study provides a robust analysis of AL and includes contributing health behaviors in response to stress/adversity (e.g., smoking) and potential attenuative factors such as social support. • Findings over the five years indicate that the negative health effects of AL have a linear trajectory, supporting the need for future intervention research inclusive of older adults.
• Older adults should be meaningfully included in AL research. • Developing and implementing evidence-based interventions that lower AL in clinical practice may help mitigate risk of morbidity and mortality. • Efforts targeting AL could help improve longevity and quality of life of older adults.What this paper adds to existing literature
Applications of study findings to gerontological practice, policy, and/or research
Background
The impact of stress and adversity across the lifespan is a growing area of research with foci spanning single disease factors to population level health outcomes (Grummitt et al., 2021; Polick et al., 2023). Lifetime exposure to psychosocial stressors is believed to increase the risk of diseases in later life by disrupting physiological regulatory systems that govern the initiation, inhibition, and maintenance of the stress response (e.g., the sympathetic nervous system and the hypothalamic-pituitary axis) which in turn increases vulnerability to disease (McCrory et al., 2023; Seeman et al., 1997). While some health outcomes are driven, in part, from health risk behaviors (e.g., smoking and alcohol misuse), many negative health outcomes have been attributed to physiological sequelae of immune and inflammatory cascades elicited during stress responses (Guidi et al., 2020; McEwen, 2017). For example, many of the top ten causes of mortality including obesity, diabetes, heart disease, dementia, and lung disease have been linked to inflammatory response (Furman et al., 2019; Kochanek et al., 2019; Slavich, 2020).
Allostatic load (AL) is a multi-system composite index for quantifying physiological dysregulation caused by life stressors (McCrory et al., 2023). While there is no gold standard measurement approach (Li & Rosemberg, 2020), AL typically reflects function across the cardiovascular, neuroendocrine, and immune systems and is measured with a combination of biomarkers and anthropometric measures (Li et al., 2019). Elevated AL is commonly associated with increased risk of cardiovascular disease and mortality across many populations (Parker et al., 2022), and additionally with frailty, disability, and number of chronic conditions in older adults (Freire et al., 2020; Gruenewald et al., 2009; Karlamangla et al., 2006; Seeman et al., 2001, 2004).
The older adult population is rapidly expanding in the United States. Promoting quality of life among older populations is an increasing priority, yet many older adults, especially those in the oldest-old category (i.e., 80 or more) are generally underrepresented in AL research (Guidi et al., 2020). One reason may be that older studies suggest that AL plateaus around age 70 (Crimmins et al., 2003). More recent studies, however, which account for more covariates highlight a persistent linear trajectory of AL with age (Tampubolon & Maharani, 2018). Yet, more focus is needed on whether the effects of AL continue to rise with age in later life. Further, when participants within the oldest-old group are included in AL research, they are often reported in wide age categories (e.g., 65+ and 70+), or only included based on their high functionality (Gruenewald et al., 2009), which lacks nuance that would help inform health promotion strategies for adults as they reach advanced ages.
Previous studies indicate significant associations between stressors (e.g., discrimination stress and neighborhood disadvantage) and AL, highlighting AL as an intermediary to worse health outcomes (Gustafsson et al., 2014; Obaoye et al., 2023; Rosemberg et al., 2022). Much of the literature is limited, however, by failing to examine whether positive influences (e.g., social networks) attenuate the effects of AL on health. Further, health risk behavior covariates (e.g., smoking) are not consistently included (Rosemberg et al., 2020). A further limitation of the literature examining AL is that many studies have relied on older data, not yet evaluating more recent data since the COVID-19 pandemic. The utility of AL as an emerging prognostic tool to detect morbidity and mortality risk remains understudied and may be critical to improving health and longevity among diverse groups of older adults, especially the oldest-old population (>=80 years). The aim of the present study was to investigate relationships and trajectories between AL and morbidity and mortality in a large representative national cohort of older adults (ages 65+) in the United States.
Methods
This study used a retrospective, observational design using longitudinal data to examine the relationship between AL and morbidity, defined as number of chronic conditions or health events, and mortality over five years spanning before the COVID-19 pandemic to 2022. This secondary data analysis was deemed exempt by Duke University IRB.
Participants
The National Health and Aging Trends Study (NHATS) is a national longitudinal sample of community dwelling older adults (ages 65+) in the contiguous United States (US) from the Medicare enrollment file (https://www.nhats.org/). Due to the complex sampling design, weighting is commonly used to make results nationally representative. Initiated in 2011, 8245 participants completed a baseline survey about the health, economic, and social consequences of aging and disability. Follow-up interviews have been, and continue to be, conducted annually. In 2015, additional participants aged 65 and over were added. In 2017, 6312 participants remained in round 7. If over time a participant lost the ability to self-report or had died, information was obtained via a proxy such as a spouse and blood was not obtained. Public and sensitive data files from rounds 1 (2011) and 7 (2017) through 12 (2022) were used in the current study. Baseline demographic information such as sex and race/ethnicity was obtained from upon entry, and blood and anthropometric measures were collected at round seven, along with other relevant covariates (e.g., smoking and social support). Health issues were measured at rounds 7–1
Measures
Primary Predictor: AL Indicators
A total of six AL indicators were available from round seven. These indicators represent the immune (i.e., high sensitivity C-reactive protein (HS-CRP), interleukin-6 (IL-6), endocrine (i.e., hemoglobin A1c (Hgb A1c), and cardiovascular (i.e., diagnosis of elevated blood pressure) systems. Body mass index (BMI) and waist circumference (WC) represent damage to multiple systems. A diagnosis of hypertension (HTN) was used as a proxy for an elevated blood pressure; therefore, BP medication was not accounted for. The AL score was calculated with the common approach of first dichotomizing (e.g., 0 and 1) the 5 biomarker variables using the fourth quartile as a “high-risk” threshold (Li & Rosemberg, 2020). Participants also received a score of 1 if they had a diagnosis of hypertension. Then the number of high-risk markers was summed. Final AL score (0–6) was tabulated as the total number of high-risk markers.
Outcome: Morbidity (Number of Health Issues)
Following other studies with count-based health outcomes (Hirschman et al., 2020; Rosemberg et al., 2022), the primary outcome variable was a count of health issues ranging from 0 to 8 that summed the number of chronic conditions (i.e., diabetes, heart disease, dementia, arthritis, lung disease, and cancer) or health events (i.e., heart attack and stroke) that an individual experienced at each of rounds 7–12. New diagnoses between rounds were captured as being present at the subsequent round. Physical conditions known to be associated with the inflammation process were chosen for the morbidity variable (Furman et al., 2019).
Outcome: Mortality (Rates of Death)
The secondary outcome of mortality was recorded via a dichotomous variable indicating whether a given respondent had died during the previous round. For instance, if a respondent died during round 10, an indicator of such was provided in round 11 in the absence of health outcome data for rounds 11 and 12.
Covariates
Demographic covariates included age (categorized in ordinal increments of five years), race/ethnicity (categorized as White, Black, Hispanic, and other), marital status (e.g., married and divorced), and education. Smoking status (e.g., nonsmoker and smoker) was covaried due to its known detrimental health effects, especially on the cardiovascular system (Ding et al., 2019). Social support was also covaried due to its inverse relation to health problems (Slavich, 2020). This was measured by the count of people the participant listed in their close social network.
Statistical Analysis
Given multiple observations per person corresponding to rounds 7–12 (i.e. multiple years nested within a single participant), we used multilevel modeling (MLM) to assess the association of allostatic load with number of poor health outcomes. Unlike repeated-measures ANOVA, MLM can handle data missing at random via maximum likelihood estimation, thus using all available data. Hence, incomplete data through round 12 did not pose a substantial risk of bias. Given the skewed nature of count data, Poisson and negative binomial parameterization with log link were used to model the morbidity outcome (Elhai et al., 2008). The Poisson model would serve as the default model unless the Bayesian information criterion (BIC) for the negative binomial model was 10 less than that of the Poisson model. The selected model examined count of health outcomes as a function of allostatic load, time (dummy-coded for waves 8–12, with 7 representing the reference value), the interaction of allostatic load with time, and the aforementioned sociodemographic variables (age, sex, race, education, smoking status, and social support). To improve interpretability, social support was centered.
In a second analysis, we additionally assessed risk of mortality as a function of allostatic load. Given an indeterminable date of death, discrete-time survival analysis was used to model risk of mortality. This approach uses latent variable analysis to model proportional hazards, akin to Cox survival models, but accounts for uncertainty in the situations where events are assessed at regular intervals rather than at the time of those events. Specifically, we modeled time until mortality, with time defined as the number of rounds since round 7 in which death was reported. For instance, death at wave 8 was marked as time 1; at wave 9, time 2; and so on. Respondents who were still alive at round 12 were censored. Allostatic load was the primary predictor, with the aforementioned sociodemographic variables entered as covariates.
Results
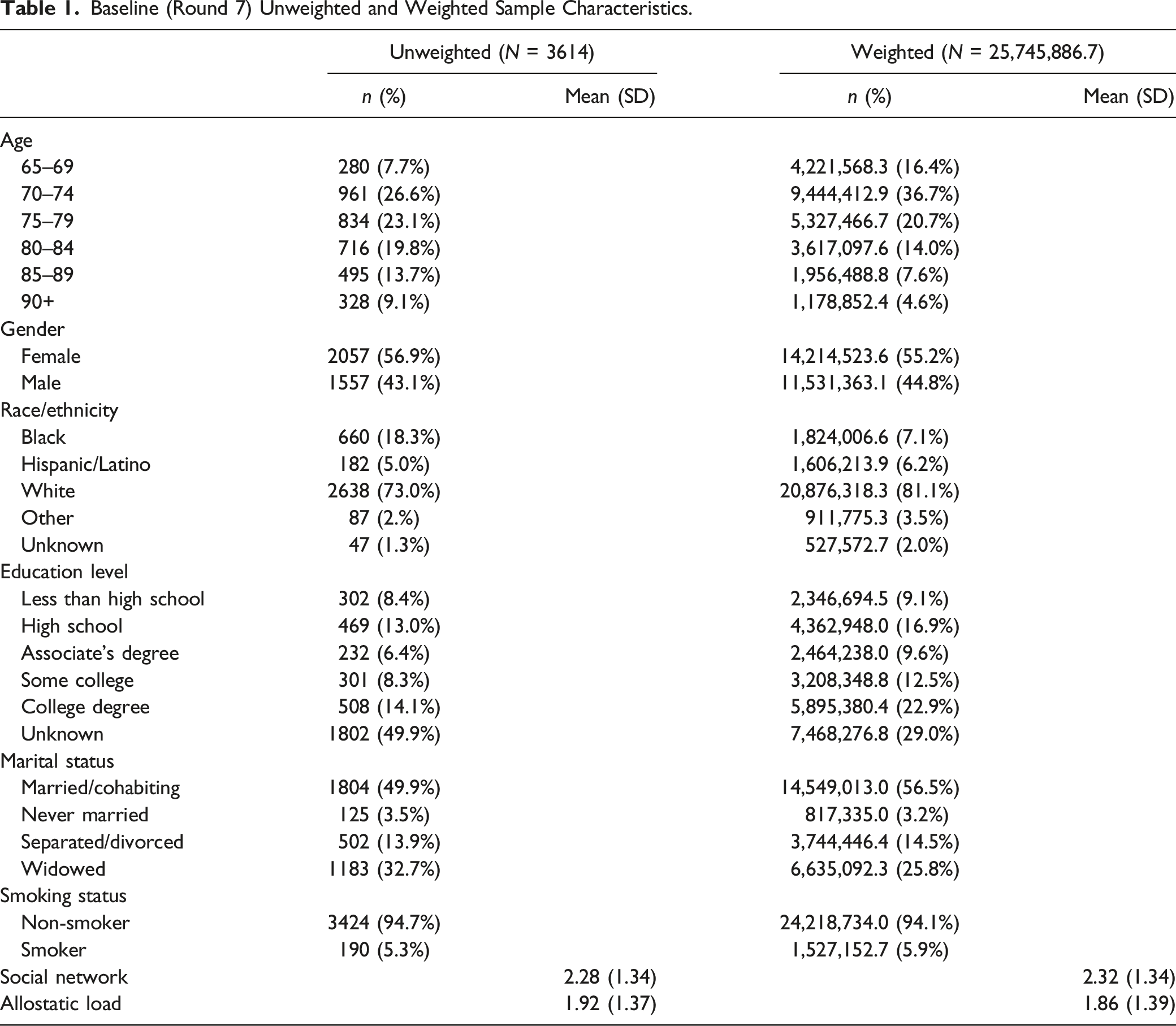
Baseline (Round 7) Unweighted and Weighted Sample Characteristics.
Morbidity
Weighted Negative Binomial Model of Health Outcomes.
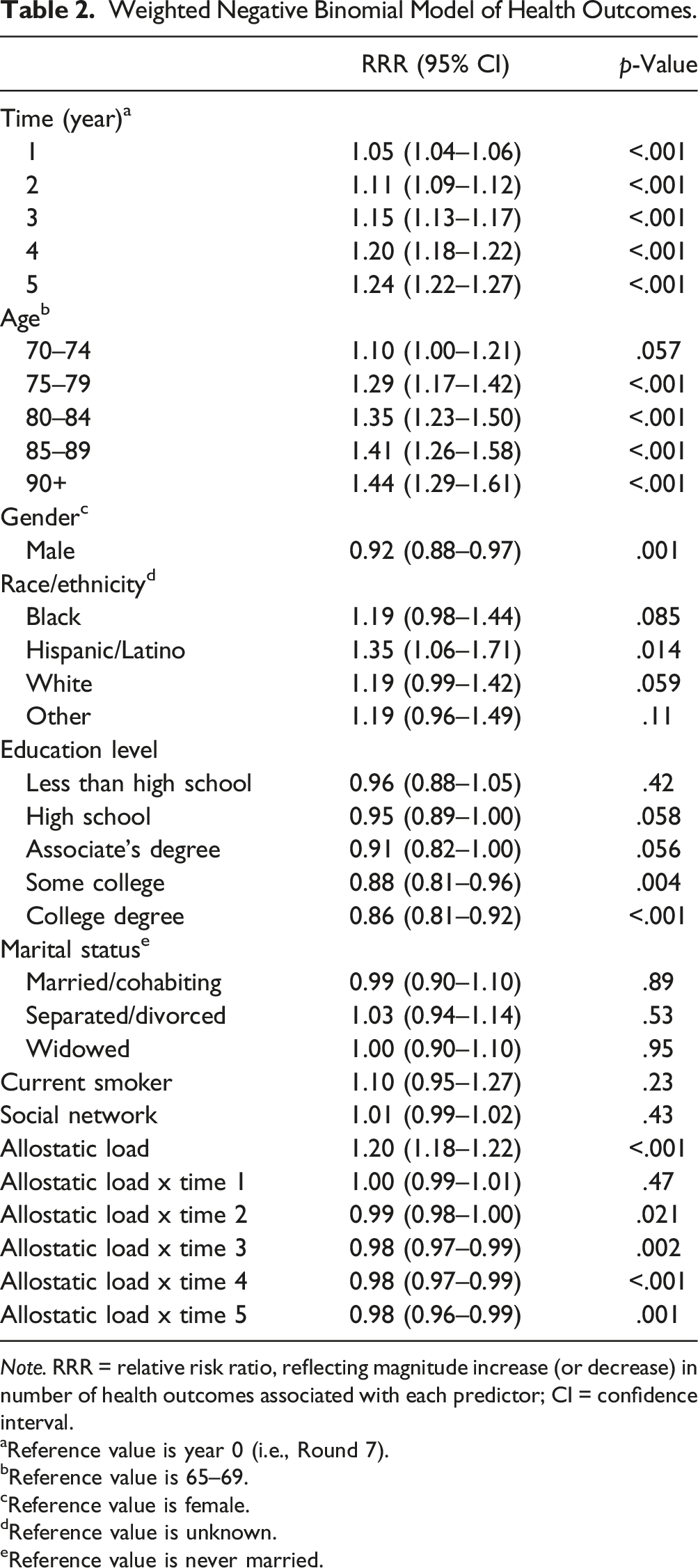
Note. RRR = relative risk ratio, reflecting magnitude increase (or decrease) in number of health outcomes associated with each predictor; CI = confidence interval.
aReference value is year 0 (i.e., Round 7).
bReference value is 65–69.
cReference value is female.
dReference value is unknown.
eReference value is never married.
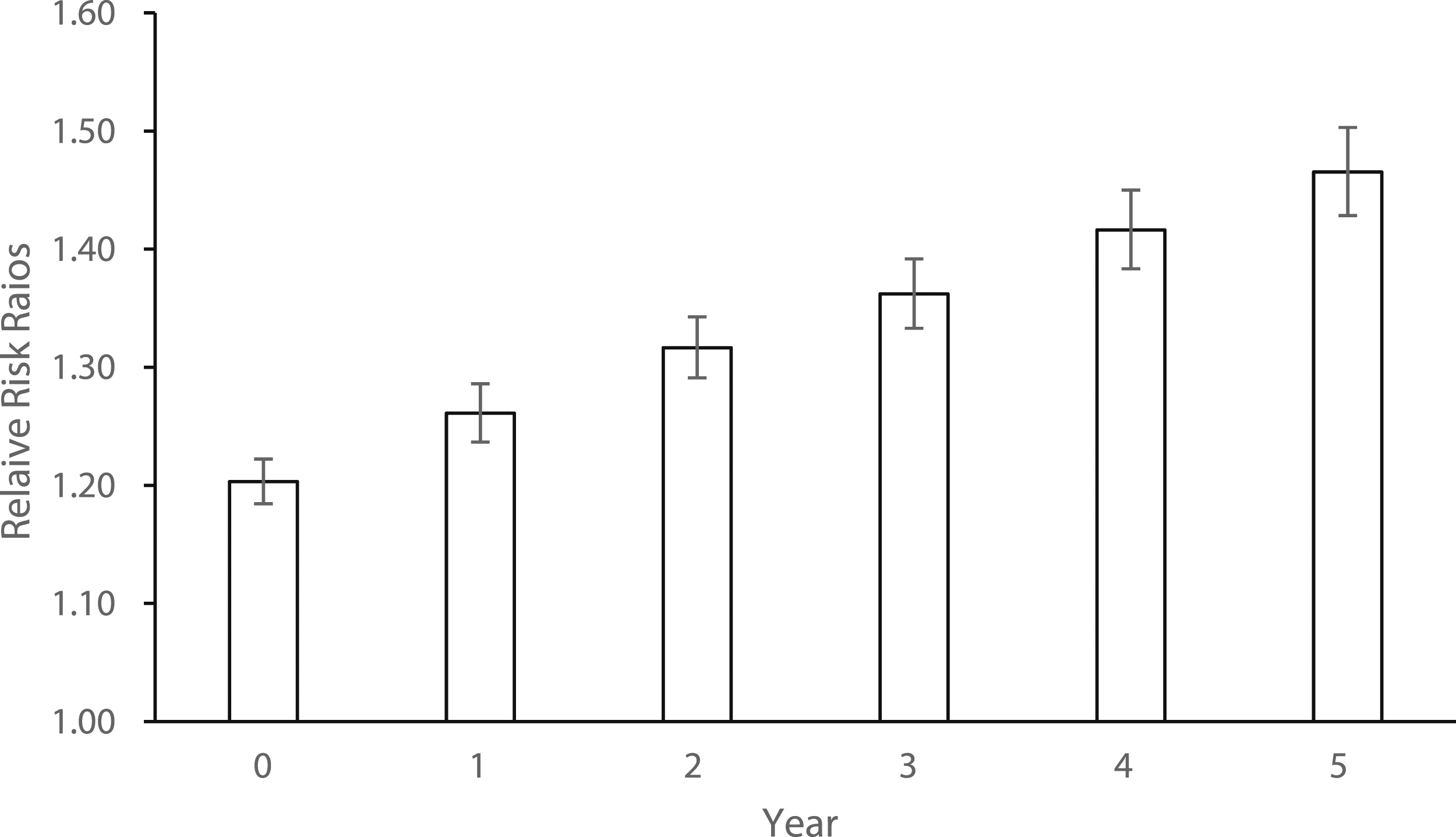
Relative risk ratios associated with 1-point increment in baseline allostatic load by year. Note. Error bars represent 95% confidence intervals.
Mortality
Weighted Discrete-Time Survival Model.
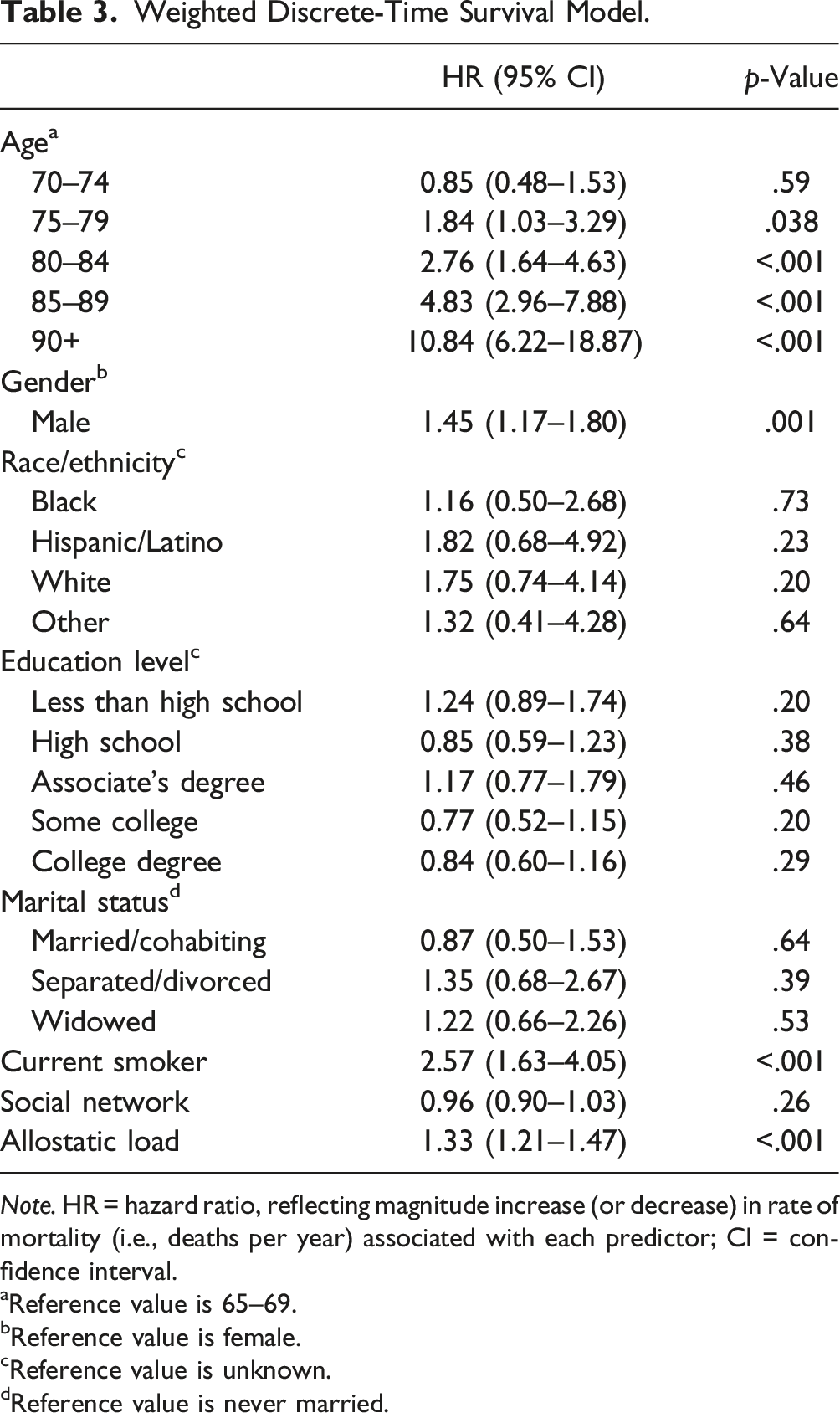
Note. HR = hazard ratio, reflecting magnitude increase (or decrease) in rate of mortality (i.e., deaths per year) associated with each predictor; CI = confidence interval.
aReference value is 65–69.
bReference value is female.
cReference value is unknown.
dReference value is never married.
Discussion
In this nationally representative study among older Americans, increased AL was associated with significantly increased morbidity and mortality each year over five years. The number of comorbid health issues increased over time (nearly 50% by year 5), even when controlling for sociodemographic, health behaviors (i.e., smoking), and positive factors (i.e., social support). Mortality increased by 33% with each one-point increase in AL. Collectively these findings demonstrate a compounding detrimental effect of cumulative wear and tear on the body, which is generalizable to US-based adults aged 64 years and older. This work advocates for more inclusion to help inform interventions to promote healthier trajectories as people age.
Findings from seminal work support that AL is higher among older adults compared to younger adults and that it plateaus around the age of 70, with increases in mortality risk observed with increased AL among older adults (Parker et al., 2022; Seeman et al., 2001). These studies were limited in that they focused on high functioning older adults (not inclusive of those over 80) who were more likely to have fewer health issues at baseline, which could underestimate the compounding effect of AL on mortality overtime. These early findings have been used to justify the exclusion of the oldest-old and the prioritization of younger adults in more recent AL research. In contrast, by including older adults across all ages, using a larger sample, and a longitudinal design this study highlights a critical period in time in which health outcomes are significantly affected by lifetime stress (regardless of whether a plateau in AL exists). Future AL research should include older adults across all ages in order to provide a more comprehensive understanding of this critical period and to inform potential strategies to mitigate the effects of AL in older adulthood.
Implications
This study further demonstrates the utility of examining AL as a predictor of important health outcomes such as morbidity and mortality especially among the oldest of old who have been excluded from prior work. While trending a personalized AL risk assessment aligns with the clinical shift towards precision medicine and a more holistic view of patients, there are significant barriers to implementing AL as a standard clinical practice. Under a more reactive, disease management paradigm, current practice typically involves trending pertinent biomarker lab tests for patients who have already been diagnosed with a disease. Implementing AL would involve additional lab tests and associated costs, which insurance companies may not reimburse without a clear indication (e.g., existing diagnosis) for being ordered. To the best of our knowledge, there are not any studies testing the feasibility, acceptability, and cost of increased workload due to implementing AL as a proactive risk indicator in the clinical setting.
AL can still support a shift to a more proactive, health promotion/risk mitigation, paradigm through informing intervention research. Evidence-based health interventions are more easily adopted by health systems and other health entities to help avoid or delay the accumulation of morbidity. A recent review highlights the paucity of intervention research in this area, with only six studies that specifically target al, most of which have average participant ages of 65 or younger (Rosemberg et al., 2020). Cognitive behavioral therapy and tai chi show promise in lowering AL among older adults and warrant further investigation (Carroll et al., 2015). Although our indicator of social support, the number of people in the participant’s social network, was not significant in this study, a more sensitive measure that captures the quality of social support may yield different results. Interventions that enhance social support or mitigate loneliness are another potential mechanism to explore. Previous studies have shown that social support across the lifespan partially mediates the relationship from childhood adversity to AL in middle adulthood (Horan & Widom, 2015). More recently, the negative effects of social isolation on the health of older adults have been highlighted since COVID-19. Comprehensive multi-modal interventions to address issues spanning the stress response, supporting resilience/coping and decreasing health risk behaviors like smoking may be particularly helpful to older adults.
Limitations of this research should be noted. Since participants needed to have the ability to self-report to consent to blood sampling, the AL scores may be skewed toward a healthier sample. There is potential for a survivor bias, where older adults that survive are typically healthier than those who died, which may underestimate the relationships between AL and morbidity accumulation. However, using five years of data helps capture a wider range of experiences compared to just one outcome time point. Further, exact dates were unavailable so years were used, and thus, lacks some granularity. Strengths of this study include a large sample that is nationally representative of adults aged 65 years and older. Our study is also novel for using updated outcome data spanning from before COVID-19 onset to 2022, which helps inform older adult research in the context of ongoing respiratory threats.
Conclusion
This study highlights the importance of improving the inclusion of older adults in AL research, especially intervention research. As the US population continues to age, supporting holistic, healthy longevity will continue to be at the forefront of aging research and policy (National Academy of Medicine, 2022). The rising emphasis on wellness necessitates interventions to mitigate the impact of AL on morbidity and mortality among older adults.
Supplemental Material
Supplemental Material - Allostatic Load, Morbidity, and Mortality Among Older Adults: A Multi-Wave Analysis From the National Health and Aging Trends Study
Supplemental Material for Allostatic Load, Morbidity, and Mortality Among Older Adults: A Multi-Wave Analysis From the National Health and Aging Trends Study by Carri S. Polick, Melissa L. Harris-Gersten, Paul A. Dennis, Devon Noonan, Susan N. Hastings, Patrick S. Calhoun, Marie Anne Rosemberg, and Sarah A. Stoddard in Journal of Applied Gerontology.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Duke Clinical and Translational Science Institute (CTSI), NIH/NINR (T32NR016914), and the Durham VA. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funders.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.