
Abstract
Frailty is a common condition that leads to multiple adverse outcomes. Frailty should be identified and managed in a holistic, evidence-based and patient-centered way. We aimed to understand how UK healthcare professionals (HCPs) identify and manage frailty in comparison with UK Fit for Frailty guidelines, their frailty training, their confidence in providing support and organizational pathways for this. An online mixed-methods survey was distributed to UK HCPs supporting older people through professional bodies, special interest groups, key contacts, and social media. From 137 responses, HCPs valued frailty assessment but used a mixture of tools that varied by profession. HCPs felt confident managing frailty and referred older people to a wide range of supportive services, but acknowledged a lack of formalized training opportunities, systems, and pathways for frailty management. Clearer pathways, more training, and stronger interprofessional communication, appropriate to each setting, may further support HCPs in frailty management.
• HCPs felt frailty identification was useful and used a wide range of tools for this. • HCPs feel confident managing frailty and use multiple comprehensive assessments to develop frailty care plans. • Less than half of healthcare professionals report receiving frailty-specific training.
• Clearer pathways and recommended frailty tools are needed for each setting. • Frailty-related information sharing across professionals needs further support. • Further formal frailty training opportunities need to be offered.What this paper adds
Applications of study findings
Introduction
Frailty is present in 12% of those aged ≥50 years worldwide (O’Caoimh et al., 2021). It is a syndrome encompassing increased vulnerability after a stressor event, with a multitude of deficiencies in various organ systems leading people to struggle to recover to previous functional levels after an episode such as a fall or infection (Clegg et al., 2013). Frailty has multiple adverse consequences, including increased risk of mortality, hospitalization, falls, and moves to long-term care (Kojima, 2018; Ofori-Asenso et al., 2020; Rockwood, 2005). Frailty is also associated with poorer quality of life, increased risk of depression, and increased health care utilization and costs when compared to robust older adults (Bock et al., 2016; Crocker et al., 2019; Ilinca & Calciolari, 2015; Soysal et al., 2017).
It is important to identify those with different stages of frailty to appropriately target interventions and services. “Fit for Frailty” recommendations from the British Geriatrics Society (BGS) (2014) state that older people should be assessed for frailty during all healthcare professional (HCP) encounters, using either gait speed (CGA Toolkit Plus, n.d.a), the Timed Up and Go (Physiopedia, 2023) or PRISMA-7 (CGA Toolkit Plus, n.d.b), with training for all staff. For frailty management, comprehensive reviews are advised, with further referrals if applicable (e.g., to geriatric medicine or old age psychiatry, and medication reviews). A shared care and support plan should be developed and communicated between different care providers, using adequate electronic systems to share this information. Local protocols and pathways should also be developed for frailty (British Geriatrics Society, 2014). There are effective ways to manage frailty, most notably care plans and multicomponent physical activity programmes (Dent et al., 2019).
Studies on HCPs’ understanding of frailty shows that there is still lack of clarity over what frailty is, and how it should be measured across a range of professions (e.g., nursing, physiotherapy, and/or occupational therapy) (Anantapong & Tinker, 2019; Coker et al., 2019; Mulla et al., 2021). Previous surveys of hospital care, medical professionals, and geriatrics show frailty is rarely consistently identified (Jacques et al., 2019; Knight et al., 2022; Taylor et al., 2017). Evidence about effective management has proliferated rapidly over the last five years, and the International Conference of Frailty and Sarcopenia Research (ICFSR) group has developed international guidelines on frailty management for older adults (Dent et al., 2019). However, little is known about how frailty is actually managed in practice, in different settings, and across different HCPs, especially within the UK.
In this study, in addition to understanding frailty identification, we aimed to extend beyond previously conducted surveys (Jacques et al., 2019; Knight et al., 2022; Offord et al., 2019; Taylor et al., 2017) and explore in more detail HCPs’ attitudes, multidisciplinary approaches, frailty management techniques, and the systems and pathways to support these, closely based on the UK Fit for Frailty recommendations (British Geriatrics Society, 2014).
The study therefore aimed to: Understand how and why frailty is identified within acute, community, and primary care settings in the UK and how this compares to established guidelines. Understand how frailty is managed in these settings and how this compares to established guidelines. Identify the training needs and confidence levels of HCPs in identifying and managing frailty. Understand the support structures in place for HCPs regarding frailty.
Method
We conducted an online survey using Jisc online surveys, which the investigators opened between September 2019 and April 2020 in the UK. Recruitment pathways were identified during two mapping meetings between the research team during 2019. We circulated the survey link through professional networks and special interest groups with their agreement, including: the Wessex Academic Health Science Network, the British Geriatrics Society (BGS) “Frailty Special Interest Group”, Malnutrition Task Force, CHAIN, and the Acute Frailty Network. Contact was also made, and the survey link distributed through the following professional bodies: the Royal College of General Practitioners, the Royal College of Nursing, the British Dietetics Association, the Chartered Society of Physiotherapy (CSP) AGILE group, and Royal College of Occupational Therapy. In addition, we made use of social media (Facebook and Twitter) to advertise the study and survey link. Snowball sampling was also utilized, through asking key clinical and academic contacts known to the research team to circulate to relevant colleagues.
Participant eligibility criteria included: membership of a professional group or organization, Allied Health Profession membership, or working for a recognized healthcare provider for at least 5 years. It was not essential to hold a professional qualification (e.g., BSc) for participation, however, holding a recognized professional membership (e.g., British Dietetics Association or Royal College of Occupational Therapy) was required. Before starting the survey, participants were asked to confirm that they met these criteria and consent to participation.
The online survey included twenty open and closed questions, regarding: respondent demographics, frequency of older adult frailty care, practices in identifying and managing frailty, and frailty training. The survey questions were based on the practice recommendations of the BGS “Fit for Frailty” UK guidelines (British Geriatrics Society, 2014). Survey data were collected anonymously unless participants wished to provide contact details in order to receive a copy of the results. In this case, the contact details were separated from the survey data prior to analysis. Ethical approval was obtained from the University of Southampton’s Ethics and Research Governance (ERGO) board for the Faculty of Environmental and Life Sciences (ID: 52195).
For the survey, the raw data from Jisc Online surveys were downloaded as CSV files and saved as Microsoft Excel files. Quantitative data were analyzed descriptively using SPSS v22 (IBM, New York, USA) with responses summarized as N and percentage per category, or mean and standard deviation for continuous data. Open-ended questions containing qualitative data were analyzed in MS Excel. Responses were coded inductively by RF under one or multiple codes, based on content analysis (Weber, 1990). Answers with very brief responses (e.g., types of training courses, other frailty identification tools) were classified into logical (e.g., in-house courses) or named groupings (e.g., Rockwood Clinical Frailty Scale). Those with more data provided were labeled according to their content and the frequency of coded responses provided with supporting quotes.
Results
Survey Respondents
One-hundred and thirty-eight people (n = 138) completed the survey, including 63 physiotherapists, 22 nurses, 20 occupational therapists, 19 medical doctors, three dietitians, two pharmacists, two therapy associate practitioners, and one each of the following: assistant therapist, social worker, care home activities worker, speech and language therapist, pharmacist/geriatrics researcher, researcher (intermediate care), education (primary care). We excluded the latter respondent, as the person reported spending no time in clinical practice or working with older people, leaving a total of 137 completed responses.
Respondents had worked in clinical practice for an average of 17.4 years (SD 10.6 years, range 1–48 years), and had worked with older people for an average of 14.6 years (SD 8.4 years, range 1–35 years). Respondents estimated that 88% (SD 16.5%) of their caseload involved caring for patients aged over 65 years old (range 5%–100%).
Five HCPs were employed in the private sector, the remainder in the public sector (i.e., such as the NHS). Public sector workers spent the majority of their time in an acute hospital (n = 76), intermediate care (n = 30), primary care (n = 26), or did not specify (n = 1). Those employed in the private sector spent the majority of their time in intermediate care (n = 2), an acute hospital (n = 1), primary care (n = 1), or did not specify (n = 1). Respondents self-reported being recruited through professional networks, mainly British Geriatrics Society or CHAIN (n = 31, 23%); a colleague/local lead (n = 31, 23%); email (no other specification) (n = 28, 20%); professional bodies, mainly the CSP AGILE group (n = 26, 19%); and social media, mainly Twitter (n = 18, 13%). Three did not report recruitment source.
Identifying Frailty
Self-Declared Reasons for HCPs to Identify Frailty.
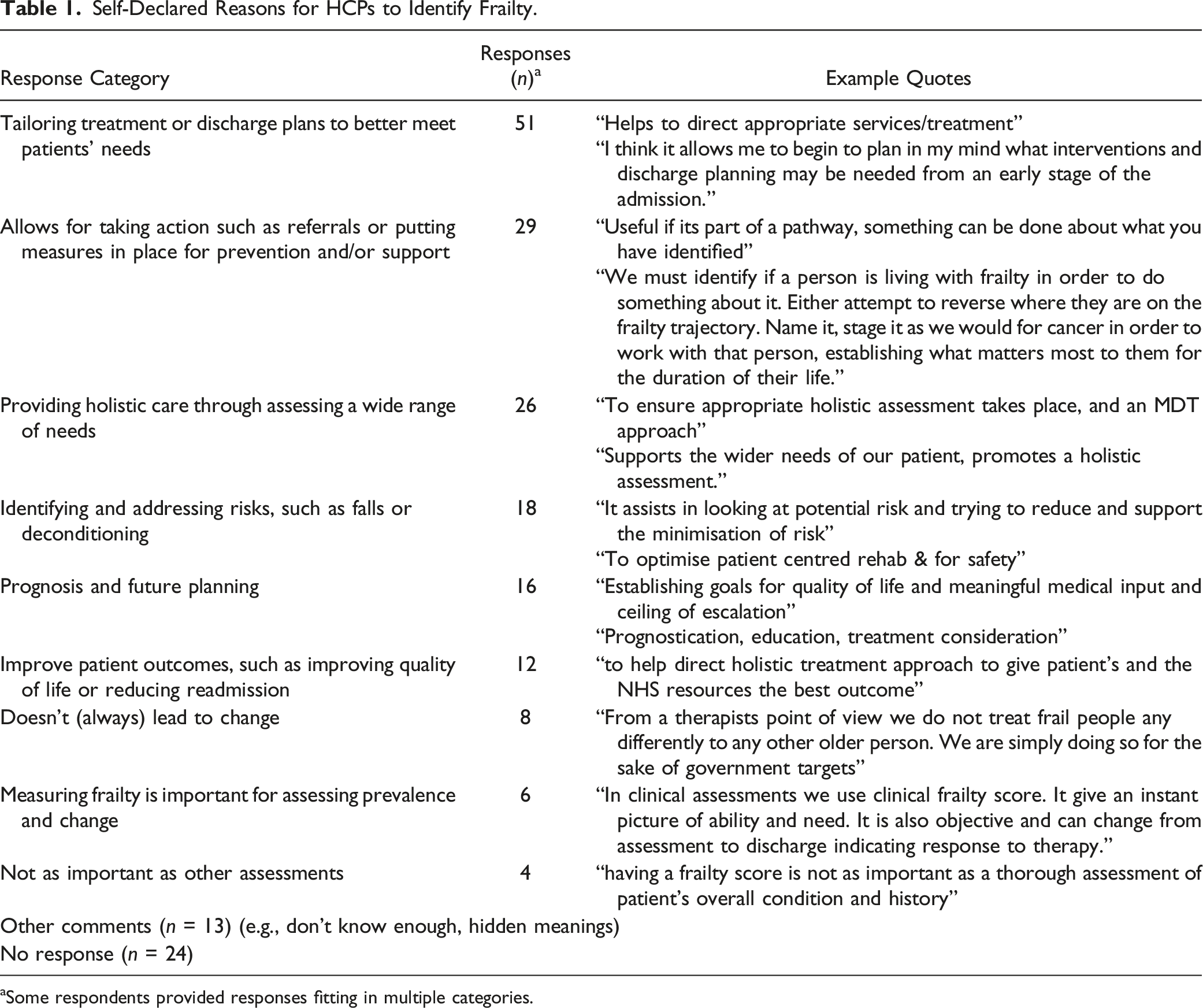
aSome respondents provided responses fitting in multiple categories.
In all, 99 (72%) HCPs indicated that they assessed frailty in older people either routinely or all the time, 26 (15%) when indicated and 12 (9%) never assessed frailty. Those never assessing frailty included five physiotherapists, three occupational therapists, three nurses, and one dietitian, who all worked with older people ≥60% of the time. Reasons given as to why the HCPs did not assess frailty in their role included: other professionals do the assessment (n = 5), not part of practice (n = 3), not enough time (n = 2), and lack of understanding (n = 2).
Reported Tools Used by HCPs to Assess Frailty.
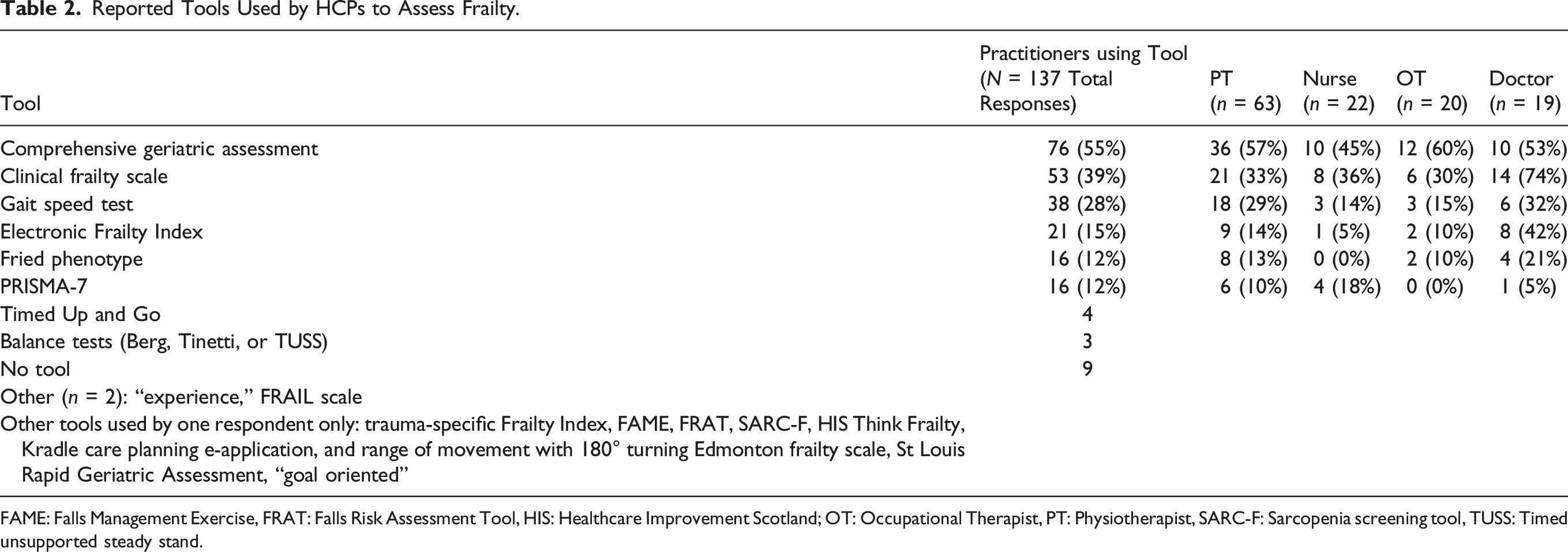
FAME: Falls Management Exercise, FRAT: Falls Risk Assessment Tool, HIS: Healthcare Improvement Scotland; OT: Occupational Therapist, PT: Physiotherapist, SARC-F: Sarcopenia screening tool, TUSS: Timed unsupported steady stand.
Managing Frailty
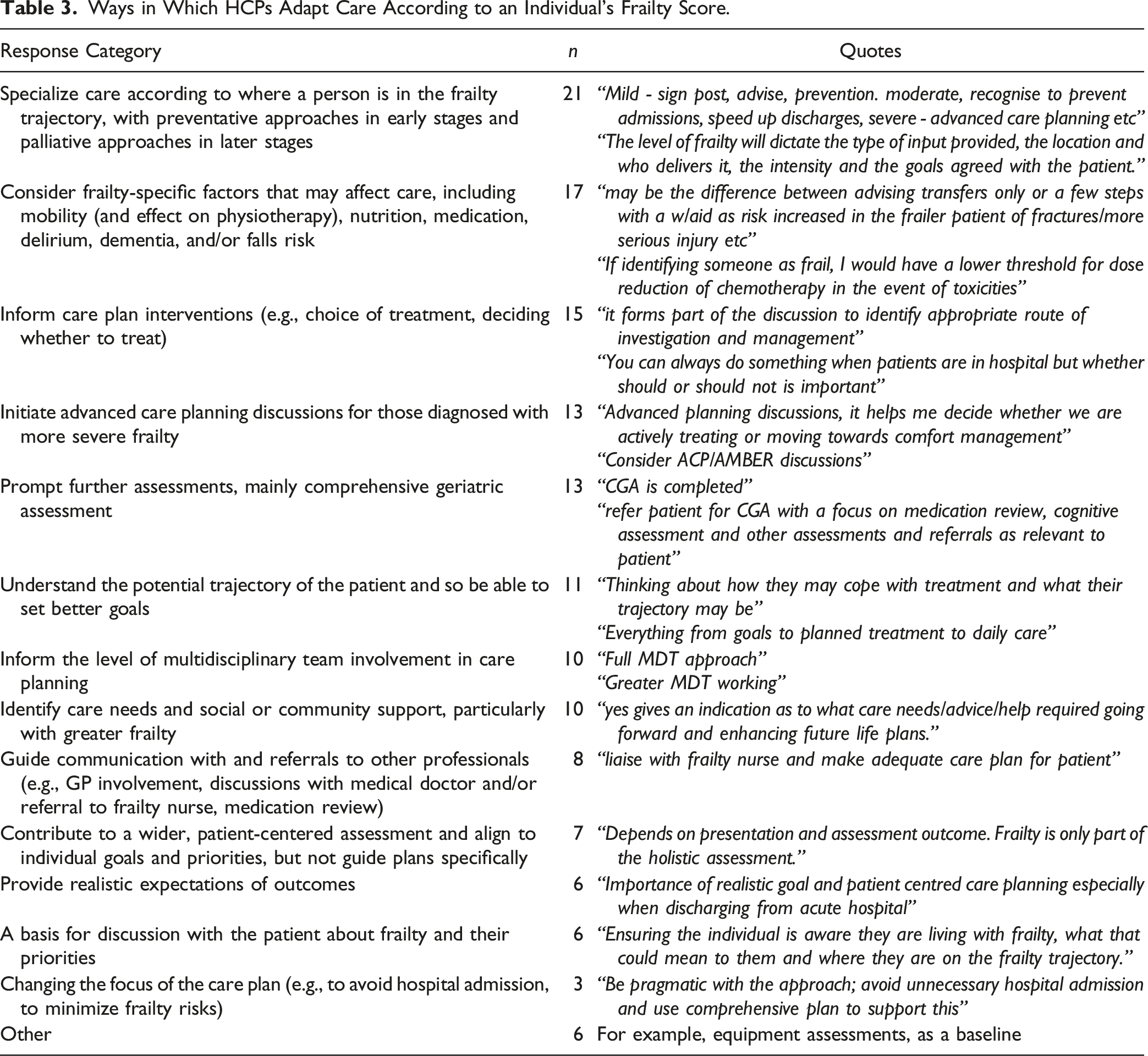
Ways in Which HCPs Adapt Care According to an Individual’s Frailty Score.
In the survey we indicated nine standard further assessment options that could be used after identifying that someone is frail. These were commonly used across all HCPs, with slightly fewer recommending nutritional or psychological assessments (Figure 1). Number of HCPs reporting further assessment types after identifying someone as frail (N = 137).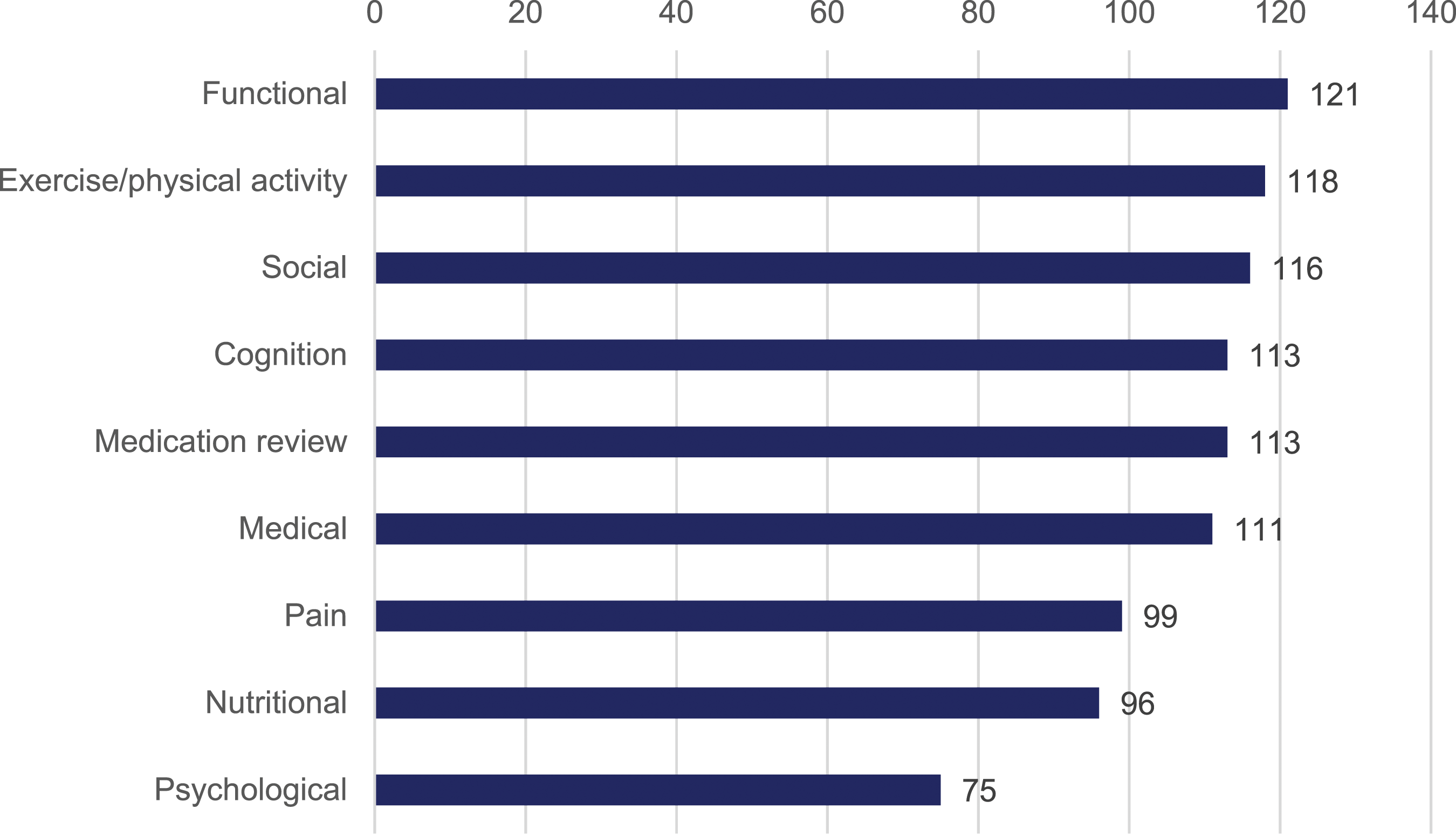
Pathways of Additional Support for the Management of Frailty.
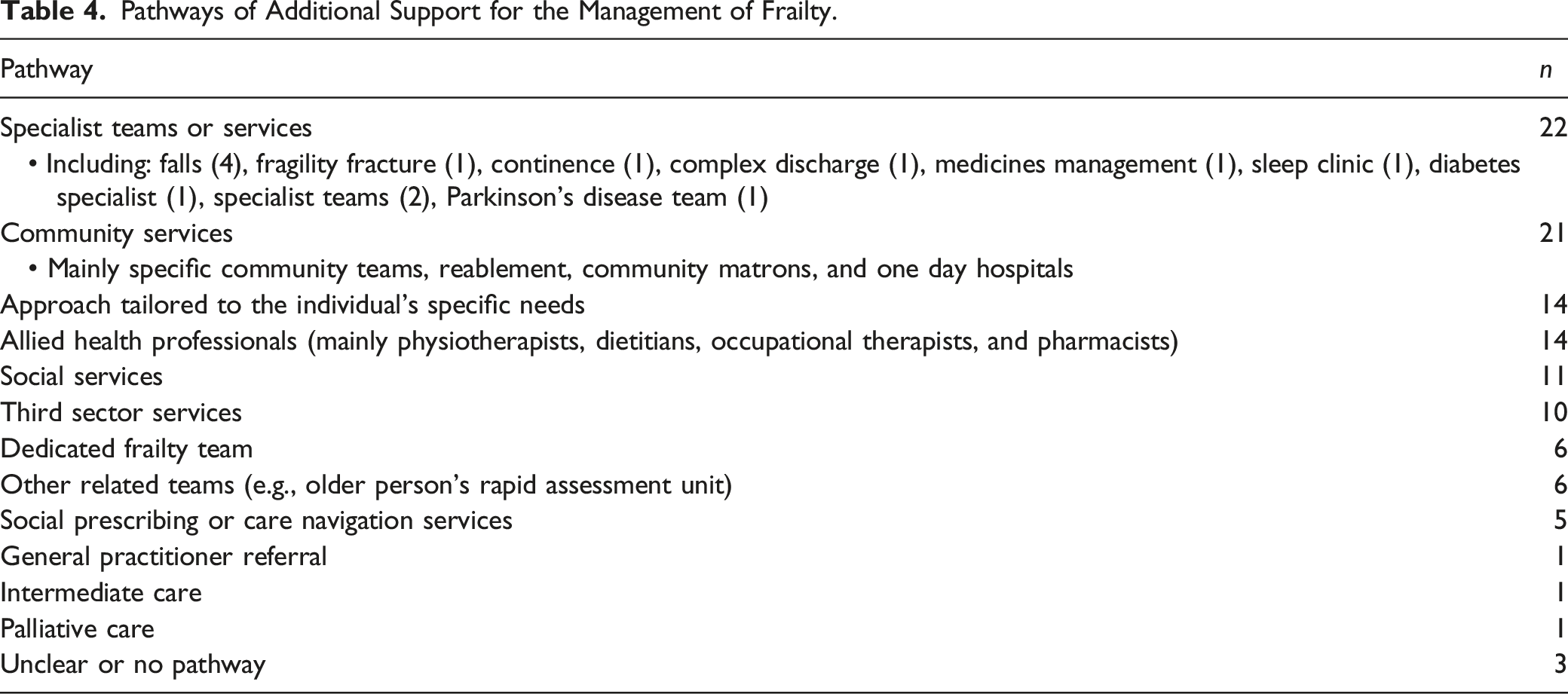
Seventy-four (54%) of respondents regularly developed care plans specific to frailty management. These frailty-specific plans covered: care management (n = 62), treatment (n = 62), end of life care (n = 50), and urgent care (n = 44). Other planning included: social care (n = 2), patient priority-specific planning (n = 2), anticipatory care (n = 1), multidisciplinary team (1), ad hoc urgent care (n = 1), contingency plans for ambulance services (n = 1), advanced clinical practice (n = 1), therapeutic interventions and advice (n = 1), and Comprehensive Geriatric Assessment problem list and agreeing action plans (n = 1).
One hundred and twenty (88%) respondents indicated that they referred their patients or signposted to services to support living at home, a UK pathway to promote independent living arrangements. This was most commonly supported with home care and social care services (n = 55); community therapy teams such as reablement, district nursing, podiatry, or community mental health teams (n = 54); and third sector organizations, such as Red Cross and Age UK (n = 52). Other smaller numbers included listing specific local services we were unable to classify (n = 16), supportive services after discharge from hospital (n = 9), rapid response services (n = 7), social prescribing (n = 6), and befriending services (n = 6). Smaller numbers also reported other services, such as food, falls, intermediate care or telecare.
Training Needs and Confidence Levels
From the responses 78 (57%) stated that they had not received any formal training on how to identify and assess frailty. However, the remaining HCPs (59, 43%) did confirm that they had received some form of training. This included in-house training (n = 26), which could include courses or workshops delivered in an NHS Trust (n = 14), on the job training (n = 3), training run by other team members (n = 3), being a local frailty lead (n = 1), or unclear as to training (n = 5). Twenty-two had attended external training courses (e.g., NHS England training day, as part of an MSc, Acute Frailty Network courses) and eight had learnt during specific geriatrics training. Other routes included self-directed study (n = 6), e-learning (n = 5), at a conference (n = 3), work experience within a community rehabilitation team (n = 1), peer-learning (n = 1), a research fellowship (n = 1), or unclear (n = 4). Fifteen participants reported multiple forms of training (e.g., in-house and external).
When asked “How confident do you feel in managing frailty?”, 113 (82%) felt confident or very confident in managing frailty compared to 24 (18%) who felt less confident. Sixty-three (46%) of the HCPs reported receiving training on frailty management, with 18 reporting multiple sources, five missing responses, and four referring to the previous question on frailty identification training. Over 50% of these respondents declared that they had attended some formal training course, for example, an external course on frailty management (n = 21, 33%) or in-house training (n = 13, 20%). Six or fewer respondents reported other methods such as attending conferences, peer discussions, professional networks, or self-directed study.
Support Structures for Frailty
Only 62 (45%) of HCPs had a system for sharing frailty information between services, mainly electronic records or systems (n = 27), discharge summaries (n = 15) and multidisciplinary teams (n = 6), or multiple methods (n = 13). Other approved methods for sharing (e.g., email) were reported by two or fewer people. Only 33 (24%) respondents reported using an established care pathway for frail older people. This is perhaps due to lack of provision locally, although we did not ask directly the location of the HCP. Seventy-eight (57%) did not know or were not able to identify a local frailty care pathway for their patients. However, 26 did indicate that this type of pathway was in development. This potentially identifies a gap in provision and requires further exploration.
Discussion
Our online survey outlines the experiences of 137 UK HCPs regarding the use and application of frailty tools, management, and pathways. Multiple frailty tools were used, most frequently Comprehensive Geriatric Assessment and the Clinical Frailty Scale, which are the recommended tools for assessment by the BGS (2014). Of concern, less than half our sample reported receiving any formal training in frailty assessment and management. Most HCPs felt confident managing frailty; however, awareness of local frailty pathways was low, and information sharing across professionals was limited.
Our survey results suggest that frailty assessment is valued by individual HCPs and they feel confident in managing frailty. Compared to the BGS “Fit for Frailty” recommendations, further work needs to be done in encouraging HCPs to identify frailty, which our survey found is conducted by the majority (71%) but not by all those responding. This concurs with other literature (Bruyère et al., 2017; Gobbens et al., 2022; Knight et al., 2022; Offord et al., 2019; Roberts et al., 2023). In a broader survey of European services for older people, 52.8% always assessed for frailty and 38.1% sometimes assessed for frailty, with 90.9% assessing it as part of routine practice and higher assessment rates for geriatricians compared to other professionals (Bruyère et al., 2017). A previous large scale survey of acute hospital care in the UK found that out of all hospitals reporting use of a frailty assessment tool, 50% (1026) patients on average were assessed for frailty, with substantial variation across different hospitals (2.2%–100%) (Knight et al., 2022). This variation was also found in a survey by Offord et al. (2019), which found that rates varied between 46% on non-orthopedic surgical wards to 94% in organizations with a dedicated acute medical unit for older people. In the community, 71% teams identified frailty as part of their work in England, and 82% in devolved nations (Offord et al., 2019), whilst community nurses in the Netherlands screened for frailty 61% of the time (Gobbens et al., 2022). A survey of dietitians across acute and community settings in Australia found that 39.4% assessed frailty 75%–99% of the time, with between 8% and 22.3% selecting other categories ranging from none of the time to all of the time (Roberts et al., 2023).
The reasons for inconsistencies in frailty assessment have been explored. Reasons that frailty assessment is valuable align with our survey. Qualitative studies suggest frailty assessment is considered valuable by HCPs to identify and reduce the risk of adverse outcomes, tailor clinical care, and support decision making (Liu et al., 2022; Mulla et al., 2021). However, in a study with Australian orthopedic surgeons, frailty screening was considered positive in principle but unlikely to be helpful or feasible in their everyday practice (Archibald et al., 2020). HCPs from both acute and community settings have suggested that frailty screening is less valuable as they informally assess this anyway without needing a formal tool (Archibald et al., 2020; Canbolat Seyman & Sara, 2023; Mulla et al., 2021; Papadopoulou et al., 2021; Seeley et al., 2023). Previous qualitative work with GPs, psychiatrists, orthopedic nurses, dietitians, and primary and community care staff also suggests frailty is not always well defined or consistently understood by HCPs, particularly across different professions (Anantapong & Tinker, 2019; Canbolat Seyman & Sara, 2023; Coker et al., 2019; Mulla et al., 2021; Roberts et al., 2023; Seeley et al., 2023), with variations in preference of screening tool by discipline (Liu et al., 2022). Lack of support and resources has also been cited as a barrier in both acute and primary care settings (Liu et al., 2022; Mulla et al., 2021; Papadopoulou et al., 2021). Patients often view frailty as an unmalleable, downward trajectory (D’Avanzo et al., 2017), and therefore concerns have been raised around the acceptability of the frailty label to patients (Archibald et al., 2020; Kennedy et al., 2021; Seeley et al., 2023), and in particular understanding of the malnutrition element (Roberts et al., 2023).
The recommended “Fit for Frailty” assessments of gait speed, Timed Up and Go and PRISMA were not used as frequently as Comprehensive Geriatric Assessment and the Clinical Frailty Scale in our survey, which accords with a previous UK survey where the Clinical Frailty Scale was commonly used across all settings, and the Electronic Frailty Index and Timed Up and Go were also used in the community (Offord et al., 2019). Whilst the Clinical Frailty Scale is considered to be a speedier tool to perform it has been reported that HCPs feel it lacks consistency and does not include a useful mental health dimension (Coker et al., 2019).
Regarding frailty management, in our survey HCPs were adherent to the “Fit for Frailty” guidelines (British Geriatrics Society, 2014). They reported taking a holistic and comprehensive approach, such as using a wide range of further assessments (e.g., functional, exercise, medication review), onward referrals (e.g., to geriatricians or GPs), and signposting to community services. The wide range of further assessments used reflects WHO recommendations on Healthy Aging, defined as the process of developing and maintaining the functional ability that enables well-being in older age (World Health Organisation, 2019). It is made up of the intrinsic capacity of the individual, relevant environmental characteristics, and the interactions between the individual and these characteristics. The cited actions include most of the domains of intrinsic capacity, the composite of all mental and physical attributes upon which a person can draw (World Health Organisation, 2015), including vitality (nutrition), locomotor capacity, visual capacity, hearing, cognition, and psychological capacity (World Health Organisation, 2019). Intrinsic capacity is inversely associated with frailty (Tay et al., 2022) and may represent a more positive way of maximizing a person’s assets. Future studies would benefit from exploring if and how HCPs use this approach.
A holistic approach to assessment has also been reported by UK community nurses, general practitioners, and other HCPs in qualitative interview and focus group studies (Coker et al., 2019; Mulla et al., 2021; Papadopoulou et al., 2021) and European surveys (Bruyère et al., 2017). Qualitative studies in the Netherlands have found that proactive monitoring, planning, multidisciplinary collaboration are key parts of primary care frailty management (La Grouw et al., 2020), with nurses feeling that optimizing nutritional status, support from the environment and improving mobility were especially important (Gobbens et al., 2022). The clear changes in care as a result of frailty assessment are encouraging, as qualitative work suggests that making a difference and not being a tick box exercise is important to motivate HCPs to identify frailty (Anantapong & Tinker, 2019; Mulla et al., 2021). However, it should be acknowledged that patients and HCPs often have differing perspectives on frailty management and what can be achieved (D’Avanzo et al., 2017; La Grouw et al., 2020).
With regards to training and confidence, in our survey 82% HCPs felt confident in managing frailty. A previous survey found that only 53% UK hospital doctors were confident in identifying frailty (Taylor et al., 2017), but did not ask about management. Qualitative work with Irish community HCPs found confidence in frailty identification in general, but not in the use of specific tools (Kennedy et al., 2021). The low levels of frailty training in our study are also reflected in other studies. Only 38.1% UK hospital doctors had received frailty identification training, with 67.9% agreeing they would like more teaching on this (Taylor et al., 2017). Particular training needs identified in other studies include the different grades of frailty (Mulla et al., 2021; Seeley et al., 2023), malnutrition assessment and interpretation (Roberts et al., 2023), and guidance on using specific tools with clear instructions as to what the scoring should be used for and how to explain in to other HCPs and patients (Coker et al., 2019). HCPs suggested that frailty training should be incorporated into the curriculum at an early stage (Mulla et al., 2021; Papadopoulou et al., 2021). Further educational courses were recommended to be face-to-face, discussion-based, and interdisciplinary in order to develop a shared understanding (Coker et al., 2019).
Regarding support structures for HCPs, our findings identified a particular lack of clear pathways for patient management and limited ability to share frailty information. This is supported by other studies. One survey of hospitals found that only 62% (80/139) hospitals had a policy of frailty identification (Knight et al., 2022), whilst an Australian survey of dietitians found that only 15% had a policy for screening for malnutrition and frailty, although 63% reported a malnutrition screening policy (Roberts et al., 2023). In addition to screening guidance, a lack of guidance on what to do after frailty identification has been cited as a key barrier to identifying it in practice (Canbolat Seyman & Sara, 2023; Liu et al., 2022), with suggestions from dietitians that pathways and guidance on frailty are less common in the community (Roberts et al., 2023).
Multidisciplinary teams are considered a vital part of frailty management, but challenges have also been identified, particularly in community settings, about information sharing between HCPs (Anantapong & Tinker, 2019; Coker et al., 2019; Kennedy et al., 2021; La Grouw et al., 2020; Roberts et al., 2023). In contrast to the “Fit for Frailty” guidelines, care plans related to frailty were only developed by 54% of our respondents and were not easy to share. Care plans are a key part of the ICOPE approach recommended by the World Health Organisation (2019). Previous work looking at Comprehensive Geriatric Assessment has identified a “know-do gap,” in which failure to implement guidelines depends on many factors, including appropriateness or adaptation to setting, clear definition of roles within the process, good team setup and functioning, knowledge/awareness, patient involvement in service development, adequate resources, organizations supporting complexity, and social and political factors (Gladman et al., 2016). Further involvement of HCPs in service development processes, building on existing networks and communities, and developing clinical academic roles in relation to frailty may help overcome some of these barriers and weak areas (Gladman et al., 2016).
The strengths of our study are our focus on guidelines and a UK national focus compared to more local audits and surveys, including a range of HCPs to ensure findings are widely applicable. Much of the previous literature has focussed on HCPs’ conceptualization and identification of frailty. Our survey provides supporting data on previous findings regarding frailty identification, but extends these by collecting detailed quantitative information on frailty management, information sharing, care pathways, and training programmes attended. We also collected open-ended responses which provided limited qualitative data to contextualize our findings. However, given this is a self-selected survey sample, it is likely to be biased towards those with a particular interest in the topic of frailty and its management. This may mean positive attitudes towards frailty identification and confidence in management may be overestimated compared to those less interested; however, it is likely that the areas identified for improvement (training and pathways) will still be applicable to non-responders. These aspects need to be explored more widely, including in the profession pre-registration training period.
We acknowledge that some responses to some questions were difficult to interpret without further detail (e.g., referring to local service names or use of uncommon acronyms). We did not collect data on the regions covered and so cannot be sure of how generalizable the findings are across other areas within the UK, for example, Scotland and Northern Ireland. We recognize that our survey sample size is fairly small, particularly for some allied health professions, despite a broad and wide circulation list including HCPs’ professional bodies. Other UK and international studies have had response numbers of between 251 and 402 clinicians (Bruyère et al., 2017; Gobbens et al., 2022; Offord et al., 2019; Taylor et al., 2017), suggesting our response rate is lower than other studies. This may have been limited by the onset of the pandemic in the latter half of our data collection period in early 2020. This means that the findings of this survey may not be generalizable; however, they are broadly similar to previous surveys, which gives greater confidence in the results.
Key implications from this work include a need for further formal training to be accessible to HCPs regarding frailty, use of frailty tools, and their application across different clinical settings. There needs to be greater consistency in tools used across different departments and professionals and greater sharing of frailty-related information for improved patient outcomes. Pathways for frailty management need to be made clearer or developed locally. Although it is not the focus of our study, structuring frailty assessment and management comes with the opportunity to include aspects of ICOPE, leading to more complete and holistic care of people living with frailty. It should however be noted that there is good awareness of and value placed on frailty identification, and HCPs feel confident in its management, referring to a wide range of resources and utilizing holistic approaches to care for older frail patients. Further qualitative exploration is needed for UK HCPs under-represented in these studies to date (e.g., dietitians, occupational therapists, physiotherapists, pharmacists) to explore experiences of frailty identification and management in more detail.
Conclusions
Our work suggests that healthcare professionals are aware of frailty and find it a useful concept in practice, prompting further assessment and changing management. Clearer pathways, more training, and stronger interprofessional communication, appropriate to each setting, may help to support HCPs in identifying and managing frailty.
Footnotes
Acknowledgments
We would like to acknowledge funding from the British Council Researcher Links funding programme and FAPESP for funding the workshop “Identifying and addressing shared challenges in conducting health and social care research for older people (OPAL),” where the idea of this paper was born.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: PSA was supported by Coordination for the Improvement of Higher Education Personnel internationalization program (CAPES-PRINT-Unesp) – 001.