
Abstract
This study explored differences among older adults in mental health by sexual minority status. Data came from the 2021 U.S. National Health Interview Survey. The study sample included older adults (or those aged ≥50 years, N = 15,559), and of those, two percent (n = 380) self-identified as lesbian, gay, or bisexual (LGB). Older LGB adults had significantly higher odds of reporting a diagnosis of depression and anxiety and experiencing serious psychological distress than older non-LGB adults. Additionally, older LGB adults reported higher odds of experiencing depression and anxiety more frequently than older non-LGB adults. Significant covariates included age, sex, housing, food security, and social support. Increased risk for mental illness may be long-term consequences of stigma and discrimination that this population has experienced over the life course. The combination of structural interventions and affirming mental healthcare that recognizes the cumulative negative experience among older LGB adults is necessary to achieve mental health equity.
Keywords
The U.S. population is aging. In 2020, adults 55 years and over accounted for 29.8% of the U.S. population (Administration on Aging, 2021). The growing older adult population is also reflected among lesbian, gay, bisexual, and transgender (LGBT) adults aged 50 or older. By 2030, more than five million older LGBT adults are expected to live in the United States, an increase from an estimated 2.4 million in 2014 (Fredriksen-Goldsen et al., 2015). Despite the growing number of older adults identifying as a sexual minority and this group’s historical and current experiences of stigma and discrimination, mental health in older lesbian, gay, and bisexual (LGB) adults remains understudied (Flatte et al., 2022; Yarns et al., 2016).
In 2021, approximately 15% of people aged 50 or older experienced mental health problems such as anxiety, depression, severe mood swings, or bipolar disorder (National Institute of Mental Health, 2023). Multiple factors make the aging population vulnerable to mental illness, including a decline in functional ability or physical health, late-life stressors such as bereavement, and downward socioeconomic mobility due to retirement, which may further contribute to loneliness, isolation, and further psychological distress (World Health Organization [WHO], 2017). Current evidence suggests that one in six older adults faces elder abuse, which may increase the risk of mental health disorders such as depression and anxiety (WHO, 2017). Prior research has also identified a possible link between negative attitudes toward aging and the mental health of older adults (Lyons et al., 2017). Ageism, which the WHO defines as the stereotypes and prejudices against people based on age, is a major contributing factor to mental illness because it may lead to the internalization of negative and damaging self-perceptions such as older adults being burdens on society due to their diminished productivity (Allen et al., 2022).
The intersection of age and sexual minority status may differentially affect the mental health of older LGB and non-LGB adults. Older LGB adults must confront various forms of stigma and discrimination related to ageism and heterosexism (Fredriksen-Goldsen, 2017; Lyons et al., 2022). The compounded effect of ageism and heterosexism may heighten the risk of mental illness and other adverse health outcomes among older LGB adults than their non-LGB peers. Compared with their non-LGB counterparts, older LGB adults experience higher rates of mental illness, including depressive symptoms, serious psychological distress, and emotional distress (Dai & Meyer, 2019; King & Richardson, 2017). This pattern has also been observed among older LGB and non-LGB adults outside the United States. In Britain, older LGB adults were more likely to have a history of mental illness and more concerned about their current and future mental health than their non-LGB peers (Guasp, 2011). The same study revealed that gay and bisexual men were twice as likely to be diagnosed with depression and anxiety than heterosexual men (Guasp, 2011). In addition to mental health disparities, research has documented higher rates of sexual, physical, and behavioral health problems in older LGB adults than in older non-LGB adults (Brennan-Ing et al., 2021; Dragon et al., 2017).
Older LGB adults are exposed to multiple stressors over their life course that heighten their risk for mental illness. Many older LGB adults’ experiences of discrimination and violence might have begun in childhood (Clarke et al., 2019). Over the life course, LGB individuals confront family rejection, harassment, isolation, bullying, and other forms of violence (Fredriksen-Goldsen et al., 2017; Operario et al., 2022). Public debates surrounding the legitimization of LGBT identities and their relationships and families contribute to psychological distress among LGBT adults (Kealy-Bateman & Pryor, 2015). High-profile public votes and legislative decisions regarding the rights of LGBT people, such as same-sex marriage, are associated with significant increases in mental distress, anxiety, and substance use disorders among LGB adults (Casey et al., 2020; Hatzenbuehler et al., 2010). Furthermore, stigma and discrimination perpetuated by healthcare providers influence older LGBT adults to conceal their sexual orientation or delay or avoid health care altogether (Choi & Meyer, 2016). In turn, older sexual minority adults utilize health information technology more than their heterosexual counterparts as a resource to receive less stigmatized health care safely and comfortably (Lee et al., 2017).
The cumulative experience of stigma and discrimination confronted by older LGB adults underscores the significance of investigating differences in mental health outcomes among older adults by sexual minority status. Although prior studies examined similar research questions, many studies are not based on a nationally representative sample (Brennan-Ing et al., 2021; Guasp, 2011; Rowan et al., 2022). To our knowledge, the study by Dai and Meyer (2019) is the most recent published research that examined mental health status among older sexual minority adults using 2014–2016 survey data collected from a probability sample of older adults in select U.S. regions. Our current study expands the Dai and Meyer (2019) study using data from the 2021 National Health Interview Survey (NHIS), a nationally representative household survey of the U.S. civilian non-institutionalized population residing within the 50 states and the District of Columbia. Thus, our primary aim was to explore mental health differences among older adults by sexual minority status. We examined multiple mental health indicators, including depression, anxiety, serious psychological distress, and frequency of experiencing depression and anxiety.
Methods
Survey Design
We used data from the 2021 National Health Interview Survey (NHIS) to examine the mental health characteristics of older adults in the United States and the differences between older LGB and non-LGB adults. NHIS is a series of annual cross-sectional, nationally representative household surveys of the U.S. civilian non-institutionalized population. The survey uses a multistage probability sampling design, creating a nationally representative sample of individuals or households underrepresented in large-scale survey research. Data are collected using survey questionnaires on demographics, socioeconomic status, health conditions, healthcare access, and health-related behaviors. Detailed information about the 2021 NHIS survey methods, including its sample design, response rates, interviewing procedures during the COVID-19 pandemic, data collection, and questionnaires, is described elsewhere (National Center for Health Statistics [NCHS], 2022).
Our study, which involved secondary analyses of publicly available, de-identified data, did not require human subjects review. We conducted our analysis following relevant guidelines and regulations. The data supporting this study’s findings are available through National Center for Health Statistics, Centers for Disease Control and Prevention at https://www.cdc.gov/nchs/nhis/2021nhis.htm.
Sample
Our study sample was restricted to older adult (≥50 years old) participants (N = 15,878). This age cut-off was selected to account for cultural differences in what “older” is considered among the various groups in the sample. For example, some gay men may perceive themselves as older adults earlier than non-gay adults due to the prioritization of youthfulness and masculinity in the gay community (Schope, 2005). Our age cut-off is consistent with prior research with older sexual minority adults (e.g., Brennan-Ing et al., 2021; Dai & Meyer, 2019; Travers et al., 2022). We excluded older adult participants who identified their sexual orientation as something else, missing, or refused to answer (n = 319). Our final analytical sample size was 15,559.
Variables and Measures
Mental Health
We used three indicators of mental health: depression, anxiety, and serious psychological distress. Depression was measured with two questions. The first question (yes or no) asked whether participants had ever been told by a doctor or other health professional that they had any type of depression, including major depressive disorder, bipolar depression, post-partum depression, and seasonal affective disorder. The second question asked how often they felt depressed (never, a few times a year, monthly, weekly, or daily). Anxiety was also measured with two questions. The first question (yes or no) asked whether participants had ever been told by a doctor or other health professional that they had any type of anxiety disorder, including generalized anxiety disorder, social anxiety disorder, panic disorder, post-traumatic stress disorder, and obsessive-compulsive disorder. The second question asked how often participants felt worried, nervous, or anxious (never, a few times a year, monthly, weekly, or daily). Serious psychological distress (SPD) was measured using the Kessler 6 (K6) nonspecific distress scale (Kessler et al., 2003). K6 items asked respondents to assess the frequency of feeling sad, nervous, restless, hopeless, that everything was an effort, and worthless in the past 30 days. Each item used a five-point Likert scale, with higher scores indicating more frequent experiences of sadness, nervousness, restlessness, hopelessness, and worthlessness. We summed the responses for each question and created a dichotomous variable using the pre-determined cut-off value to assess the presence of serious psychological distress (Kessler et al., 2003). Older adults who scored 13 points or higher were coded as experiencing SPD, whereas older adults who scored between 0 and 12 were coded as not experiencing SPD.
Sexual Orientation
Sexual orientation was measured using a single item that asked participants whether they think of themselves as gay or lesbian, bisexual, straight (i.e., not gay or lesbian), or something else. Older adults who responded that they did not know the answer, refused to answer, or did not ascertain were excluded.
Covariates
Consistent with the literature, the following social and economic variables were included in our multivariable models: age (in years), assigned sex at birth (male or female), race/ethnicity (White, Hispanic or Latinx, Black or African American, or other racialized groups, including American Indian, Alaskan Native, Asian, and biracial/multiracial persons), education (high school graduate or lower, some college without a degree or associate degree, bachelor’s degree, or graduate, professional or doctoral degree), marital status (married, living with a partner together as an unmarried couple, neither), housing (owned/being bought or rented/other arrangements), health insurance (yes or no), income-to-poverty ratio, food insecurity, and social support (Murniati et al., 2022; Petrova & Khvostikova, 2021; Pourmotabbed et al., 2020). The income-to-poverty ratio refers to the family income ratio to the poverty threshold for the sample adult’s family. Based on its frequency distribution, we recoded the income-to-poverty ratio using five categories: below poverty, 100%–174% of the poverty threshold (PT), 175%–299% of PT, 300%–499% of PT, and ≥500% of PT.
Food security was measured using the 10-item U.S. Adult Food Security Survey Module (AFSSM). The AFSSM assesses the extent to which individuals can access enough food for an active, healthy life in the past 30 days. AFSSM scores are calculated by summing the affirmative responses to the ten questions, with higher scores reflecting inadequate access to enough food. After summing their scores, participants are grouped into four categories: older adults with a score of 0 were categorized as high food security, scores of 1–2 as marginal food security, 3–5 as low food security, and 6–10 as very low food security (Coleman-Jensen & Nord, 2012). We recoded food insecurity into two categories: food secure (high and marginal food security) and food insecure (low and very low food security), taking into account the distribution of responses. Socioemotional support was a single item that asked participants how often they received the social and emotional support they needed (never, rarely, sometimes, usually, or always). Due to their low frequency, we recoded the support variable and combined never and rarely as one category. The final social and emotional support item was measured using a four-point Likert scale (never/rarely, sometimes, usually, or always).
Analysis
Our analysis comprised three steps, each using Stata’s survey features to account for the complex survey data outlined in the 2021 NHIS survey description (NCHS, 2022). First, we described target population characteristics using univariate frequency distributions with weighted percentages for categorical variables and weighted mean and standard error for age. Second, we conducted bivariable tests with correction for complex survey design to compare characteristics by sexual minority status. We used weighted Pearson χ2 for categorical variables and weighted simple linear regression for age. Third, we conducted multivariable generalized linear regressions to examine whether older LGB adults were more likely to experience mental illness than older non-LGB adults. We estimated three multivariable logistic regression models to examine whether older LGB adults were more likely to be diagnosed with (model 1) depression, (model 2) anxiety, and (model 3) serious psychological distress. The third model included the bias correction method that King and Zeng (2001) suggested to correct biased estimates of rare events, that is, reported diagnoses of serious psychological distress. We also estimated two multivariable ordinal logistic regression models to examine whether older LGB adults experienced depression (model 4) and anxiety (model 5) more frequently than older non-LGB adults. Adjusted p values for multiple comparisons were obtained to evaluate significance while considering the multiplicity of tests.
Before estimating multivariable models, we tested whether to include the NHIS sampling weights in the analyses (Bollen et al., 2016). When weights do not substantially influence the parameter estimates, unweighted estimates are preferable because they are more efficient than weighted estimates (Winship & Radbill, 1994). We used Stata’s wgttest to evaluate the significance of the impact of sampling weights on estimation results (Jann, 2004). We included the sampling weights in the regression analyses if the results of the test were significant (p < .05), meaning that the addition of weight and the interaction of weight with each independent variable in the model significantly explained the model’s variance (Bollen et al., 2016). The models with nonsignificant results did not use sampling weights, as the weighted and unweighted estimates were not significantly different (Winship & Radbill, 1994). Three multivariable models, depression (F12,15304 = 2.05, p < .05), anxiety (F12,15311 = 2.13, p < .05), and frequency of depression (F12,15262 = 1.92, p < .05), included the 2021 NHIS adult sampling weights, whereas the models that examined the association of sexual orientation with reported diagnoses of serious psychological distress (F12,15240 = 1.47, p = .13) and frequency of experiencing anxiety (F12,15272 = 1.61, p = .08) did not include sampling weights. We compared the results of models with nonsignificant wgttest results (models 3 and 5). Parameter estimates using weighted and unweighted estimators were similar. All analyses were conducted using Stata 17. Statistical significance was set at p ≤ .05 with a two-tailed test.
Results
Descriptive Statistics and Bivariable Results
Descriptive Statistics and Bivariable Results by Sexual Minority Status: NHIS 2021 (n = 15,559).
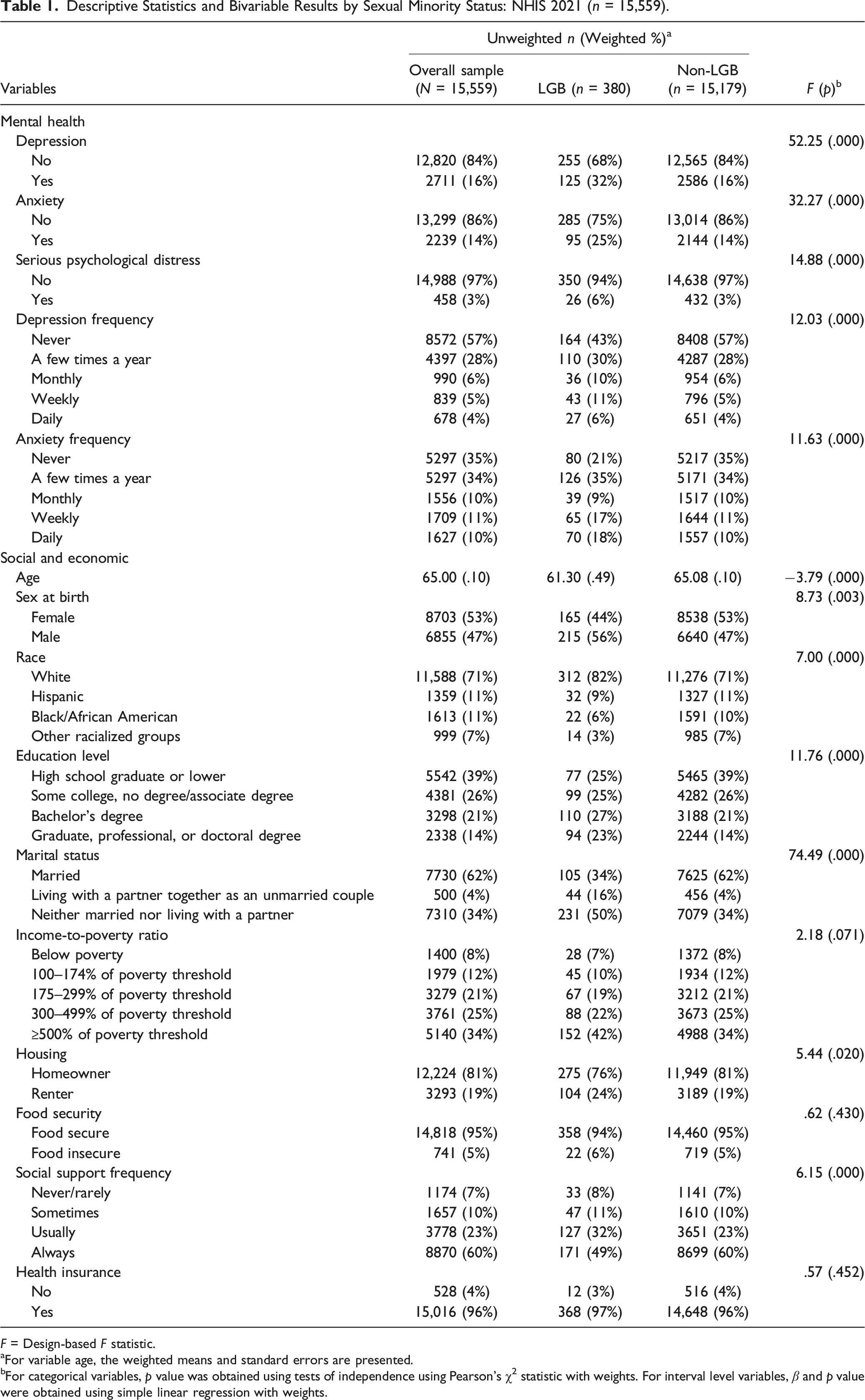
F = Design-based F statistic.
aFor variable age, the weighted means and standard errors are presented.
bFor categorical variables, p value was obtained using tests of independence using Pearson’s χ2 statistic with weights. For interval level variables, β and p value were obtained using simple linear regression with weights.
Mental Illness in Older LGB and non-LGB Adults
Multivariable Results of the Association Between Sexual Minority Status and Mental Health in Older Adults Aged ≥50.
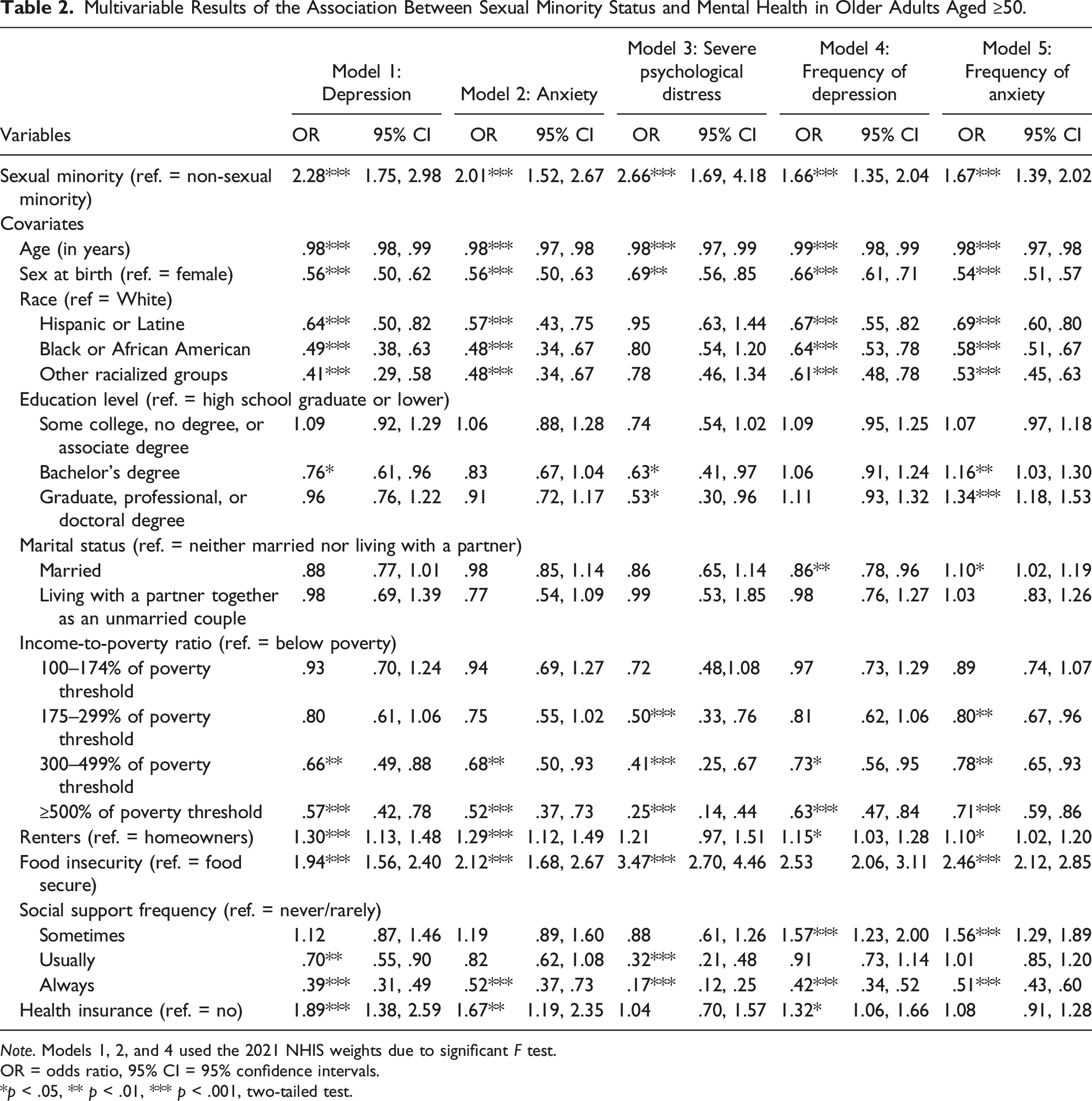
Note. Models 1, 2, and 4 used the 2021 NHIS weights due to significant F test.
OR = odds ratio, 95% CI = 95% confidence intervals.
*p < .05, ** p < .01, *** p < .001, two-tailed test.
Discussion
Our results identified a higher risk of mental illness in older LGB adults than in their non-LGB counterparts. These results are consistent with prior research that found higher levels of mental illness, including depression, loneliness, and suicide, among older LGB adults than their non-LGB peers (Cochran & Mays, 2000; Dai & Meyer, 2019; DeVries, 2014; Guasp, 2011). The cumulative experience of stigma and discrimination due to ageism and heterosexism and the chronic exposure to rejection, bullying, and violence at the individual, community, and societal levels may explain the heightened risk for mental illness among older LGB adults (King & Richardson, 2017; Yarns et al., 2016). Mental illness among older LGB adults might also indicate possible long-term effects of the cumulative and institutionalized stigmatization and discrimination against sexual minorities in the United States. The study sample, whose mean age was 65, has witnessed and experienced first-hand the discrimination and stigmatization of sexual minorities in the United States as established through governmental policies within the last 30–40 years. These policies, including the 1986 Supreme Court’s decision on Bowers v. Hardwick upholding the legality of Georgia’s sodomy law criminalizing oral and anal sex in private between consent adults, the military’s “Don’t Ask Don’t Tell” policy (1993 DADT), and the Defense of Marriage Act (1996 DOMA), which prohibited federal recognition of same-sex marriage, deepened the exclusion and discrimination experienced by LGB adults during those periods.
Enactment of discriminatory policies targeting sexual minorities has been linked to mental illness and increased substance use among LGB adults (Hatzenbuehler et al., 2010; Hylton et al., 2017). Furthermore, the deliberation and debate surrounding the legislation of LGB rights have been shown to affect mental health in LGB populations negatively (Casey et al., 2020; Kealy-Bateman & Pryor, 2015). Although legal protections exist for LGB populations, such as the right to marriage, and discriminatory legislations have been overridden (e.g., DADT and DOMA), LGB adults in the United States continue to confront repeated condemnations and delegitimation of laws supporting their rights. In recent years, LGBT populations have confronted a surge in anti-LGBT legislation, particularly at the state level. In 2022, 13 states signed anti-LGBT bills into law, whereas another 23 states introduced anti-LGBT + bills (Human Rights Commission, n.d.). A recent decision by the Supreme Court of the United States ruled that the constitutional right to free speech allows certain businesses to refuse to provide services for same-sex marriages, a decision that the dissenting justices called “a license to discriminate” against LGB people (Creative, 2023, p. 35). For many older LGB adults, the current and persistent anti-LGBT environment in the United States may intensify worries that progress achieved to date is incrementally being overturned. These concerns may heighten mental illness among LGB older adults. Unlike their LGB peers, older non-LGB adults are not subjected to frequent delegitimization of their rights and the repeal of LGBT-affirming laws. It is also important to note that participants in this study lived their early adulthood during the initial stages of the AIDS epidemic, which resulted in concentrated illness, societal blame, stigma, and loss in the LGB community (King & Richardson, 2017). This experience of survivorship and loss is likely to reflect in the mental health of older LGB adults.
The historical and persistent inequitable distribution of social, economic, and political resources may erode socioeconomic protective factors that may buffer against frequent experiences of anxiety, depression, and serious psychological distress among older LGB older adults. In turn, this inequitable distribution of resources could be attributed to the unequal treatment and discrimination of LGB populations (Hatzenbuehler et al., 2013; Mogul et al., 2011). The inequitable distribution of resources due to unequal treatment and discrimination of LGB populations might affect their ability to earn income, gain employment, and build wealth. A Federal Reserve Bank of St. Louis report identified that LGBT adults have lower household income and assets than their non-LGBT counterparts (Kent & Scott, 2022). Our study identified a significant difference in housing status between older LGB and non-LGB adults, with more LGB adults renting than non-LGB adults. Given the role of economic resources in mental health outcomes (Darin-Mattsson et al., 2017), it is plausible that the risk of mental illness among older LGB adults is heightened by the impact of unequal treatment and discrimination on their economic status.
Unlike their non-LGB counterparts, older LGB adults may not have the same level of emotional support that older non-LGB adults nurtured over their life course. Homophobia contributes to the rejection of LGB family members and the dissolution of emotional and social support from their families and friends (Anil & Raveendran, 2022). The current sample of older LGB adults grew up when same-sex relationships were unlawful and unrecognized. Many same-sex couples hid their relationship to avoid stigma and discrimination. As older heterosexual adults strengthened their connections with their romantic and life partners, older LGB adults likely struggled to maintain their romantic relationships and to provide the emotional support their partners expected (Hsieh & Wong, 2020).
Additionally, internalized homophobia might have led some LGB adults into mixed-orientation marriages. For older LGB adults in mixed-orientation marriages, coming-out might have additional stressors, including deterioration of family and social ties (Higgins, 2002). Older LGB adults who come out later in life may fear rejection as a consequence of coming out to family and friends and feel isolated as they begin to connect with other LGBT individuals (Higgins et al., 2016). In our study, older LGB adults were significantly less likely to report that they frequently received social and emotional support than their non-LGB peers (see Table 1). Although economic insecurity and inadequate social and emotional support heighten the experience of mental illness among older adults, older LGB adults may be at a higher risk of adverse mental health outcomes due to the consequences of sexual stigma and discriminatory policies on their economic standing and social support system.
Implications
Further research is needed to investigate the pathways and life course experiences contributing to the high risk for mental illness health among LGB older adults. The mental illness consequences of social exclusion and stigmatization have been noted in previous research as a persistent concern affecting marginalized or stigmatized groups, including sexual minorities (Fredriksen-Goldsen et al., 2015). Structural interventions, which address the environmental, social, and economic factors that influence individual risk and protective behaviors, are needed to improve mental health equity in older adulthood (Marshall & Cahill, 2022). These structural interventions tackle underlying determinants of mental distress among LGB populations and their impact on their well-being. These structural interventions may include enacting policies that provide a framework for legitimizing and affirming same-sex relationships and promoting their full participation in society (Operario et al., 2022). In addition, mental illness in older LGB adults must be combatted with affirming and trauma-informed care that recognizes the cumulative experience of stigma and discrimination and harnesses individual and community assets (Levenson et al., 2021). Many older LGB adults have thrived despite daily and cumulative experiences of stigmatization due to their sexual identities. Mental health programs may benefit from determining, discovering, and adapting these protective factors for use with other older LGB adults who are experiencing mental illness. The combination of structural interventions and affirming mental healthcare may achieve mental health equity.
In addition to structural interventions, access to affirming mental healthcare is critical for older LGB adults, as our study suggests older LGB adults are at a higher risk of mental illness than older non-LGB adults. It is imperative that mental healthcare for LGB adults is competent of the distinctive barriers that sexual minorities face, such as stigmatization and discrimination (Dickson et al., 2022; Fredriksen-Goldsen et al., 2018). Therefore, treatment efforts must consider the duality of being a sexual minority and an older adult.
Limitations
Although this study contributed to knowledge by examining the mental health outcomes among older LGB adults compared with non-LGB counterparts using a nationally representative household survey, a few limitations of the study should be noted. First, because of its cross-sectional design, the study could not assess if and how changes in the social and economic variables influence older LGB adults’ mental health status over time. Second, due to the use of a secondary dataset, some potentially influential variables on their mental health status were not available for the analysis, such as older LGB adults’ negative experiences they encountered due to their sexuality, including discrimination (Clarke et al., 2019). Third, we were unable to examine anxiety and depression with standardized clinical measures due to the lack of such measures in the NHIS data. Lastly, our study sample consisted of the non-institutionalized population and did not include individuals in long-term care facilities. Future research should explore the mental health of older LGB adults who reside in institutional settings. Previous research has shown that mental illness is common among older adults in institutional settings (Seitz et al., 2010) and that stigma remains a major barrier to care among older LGB adults in long-term care facilities (Dickson et al., 2022; Smith et al., 2018).
Conclusions
Our results add to the growing evidence of health disparities in mental health outcomes among older lesbian, gay, and bisexual (LGB) individuals. The observed relationship between sexual orientation and mental health in older adults may suggest long-term consequences of sexual stigma, compounded by experiences of discrimination over the life course of older LGB adults. In addition, the cumulative experiences of stigma and discrimination among older LGB adults might have adversely affected their ability to maintain and nurture supportive relationships and achieve economic security through gainful employment and income security. Although older adults with low economic standing and inadequate social and emotional support may experience a heightened risk of mental illness, unequal treatment and discrimination of LGB populations at the individual, community, and structural levels might have deprived them of opportunities to build and utilize protective factors, such as economic security and social support, that buffer against the risk of mental illness, including anxiety, depression, and serious psychological distress.
Supplemental Material
Supplemental Material - Mental Health of Older Adults by Sexual Minority Status: Evidence From the 2021 National Health Interview Survey
Supplemental Material for Mental Health of Older Adults by Sexual Minority Status: Evidence From the 2021 National Health Interview Survey by Rainier Masa, Megumi Inoue, Lucas Prieto, Dicky Baruah, Sarah Nosrat, Samreen Mehak, and Don Operario in Journal of Applied Gerontology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.