
Abstract
Using 100% Medicare data files, this study explored whether primary elder mistreatment (EM) diagnosis, EM type, and facility type were associated with 3-year mortality and 1-year unplanned hospital readmission among older patients diagnosed with EM with hospital discharge from 10/01/2015 through 12/31/2018 (n = 11,023). We also examined outcome differences between older patients diagnosed with EM and matched non-EM patient controls. Neglect by others was the most common EM diagnosis. Three-year mortality was 56.7% and one-year readmission rate was 53.8%. Compared to matched non-EM patient controls, older EM patients were at an increased risk of mortality and readmission. Among patients diagnosed with EM, patients with a secondary (vs. primary) diagnosis and those discharged from a skilled nursing facility (vs. acute hospital) were at an increased risk for both mortality and readmission. Compared to other EM types, patients diagnosed with neglect by others had a greater risk for mortality following discharge.
• Contributes to the evidence on the impact of elder mistreatment (EM) and its associated outcomes using a national sample of older Medicare beneficiaries. • Older adults hospitalized for neglect by others are at an increased risk of unplanned hospital readmission and death compared to older adults diagnosed with other EM types. • Some older adults diagnosed with EM are at risk for adverse outcomes following hospital discharge.
• Early intervention and continued monitoring of older adults hospitalized for EM is needed following discharge as their risk of mortality and readmission increases with time. • Future work is needed to further explore the experiences of EM and care utilization of older adults diagnosed with EM who are discharged from skilled nursing facilities.What this paper adds
Applications of study findings
Introduction
Mistreatment of older adults is a public health and safety crisis, with long-term consequences for individuals, families, and communities. Elder mistreatment (EM) has become a growing concern as the U.S. population ages. By 2030, 1 in 5 U.S. residents will be of retirement age, and by 2034, the U.S. population over 65 will be larger than the population under 18 (Vespa et al., 2018). The U.S. population of people 65 and older is majority-female identified and increasingly racially and ethnically diverse (Profile of Older Americans, 2020). As the older adult population grows, so does the risk for mistreatment. EM encompasses physical, sexual, emotional, and financial abuse, neglect, and abandonment (Dong, 2015). An estimated 10%–47% of the North American aging population has experienced EM; prevalence ranges are based on risk factors, including cognitive impairments, the impact of racism, age, gender, and income (Dong, 2015). Given the growing older adult population in the United States, and the subsequent increased risk for mistreatment, it is imperative to understand the health and economic impact of EM and identify prevention and mitigation strategies.
Risks for EM include previous adverse childhood experiences, midlife health challenges such as depression and poor physical health, and reduced cognitive functioning (Easton & Kong, 2021). Lower income and rates of social support and below average physical and mental health were also significantly associated with EM (Naughton et al., 2012). Previous domestic violence is an additional risk factor for EM (Cations et al., 2021). A Swedish study found that older women were more likely to experience mistreatment than older men, with significant associations found for EM with women with violence victimization with post-traumatic stress disorder (PTSD), economic concerns, and social support, and for men, with victimization, poor psychological health, and increased alcohol use (Ahnlund et al., 2020). Longitudinal analysis of the relationship between EM and depression found that depression is both a consequence and cause of EM. Those who experienced EM were 2.28 times more likely to have depressive symptoms three years later, and those with depressive symptoms were 2.23 times more likely to experience abuse three years later (Koga et al., 2022).
Elder mistreatment is associated with significant health impacts. Cisler et al. (2020) found that, among EM types, emotional abuse was uniquely predictive of mental health outcomes. Reports of emotional and financial EM are significantly associated with deceased psychological and physical functioning up to five years later (Wong & Waite, 2017) and with diminished cognitive functioning (Li & Dong, 2021). Longitudinal research illustrates the impact of mistreatment on health. Financial mistreatment significantly increased the likelihood of reporting poor health and symptoms of depression, anxiety, and PTSD (Acierno et al., 2019). Victims of EM were more likely to have poor health, depression, and PTSD symptoms compared to non-victims at 8-year follow-up. However, high levels of social support at follow-up moderated the relationship between mental health and EM (Acierno et al., 2017). There is a strong connection between EM and physical and mental health. Among hospitalized Medicare patients with diagnosed EM, the most common co-morbid conditions were hypertension, depression, fluid and electrolyte disorders, cardiac arrhythmias, and diabetes (Mouton et al., 2019).
A growing body of research suggests that EM may be significantly associated with negative health impacts resulting in hospitalizations and mortality (Dong, 2015). In a study of over 6,000 racially and ethnically diverse older adults in the United States, psychological abuse, financial exploitation, and caregiver neglect were significantly associated with hospitalizations and emergency department visits (Dong & Simon, 2013a, 2013b). In addition, experiencing two or more types of elder abuse was also associated with hospitalizations (Dong & Simon, 2013a). After adjusting for socio-economic status, demographics, and health variables, older adults exposed to EM had two times higher rates of hospitalization (95% confidence interval [CI], 1.45–2.75) compared to those not exposed to EM (Dong & Simon, 2013a). Notably, the hospitalization rates and emergency department visits related to EM did not vary by level of medical comorbidities, physical/cognitive impairments, or additional psychosocial factors (Dong & Simon, 2013a, 2013b). Mistreatment was also significantly associated with admission to skilled nursing facilities (SNFs) and SNF stays of 30 days or longer (Dong & Simon, 2013a). Among EM cases substantiated by Adult Protective Services (APS), those experiencing caregiver neglect had the lowest survival rate at 5-year follow-up (72%), and this type of mistreatment was most significantly associated with all-cause mortality (Burnett et al., 2016). Severe and moderate EM is significantly associated with mortality at 1–4 years post-abuse. Caregiver neglect and psychological mistreatment are associated with higher 3- and 4-year mortality (Li et al., 2019). Data from the Chicago Health and Aging Project showed an association of psychological abuse, financial exploitation, caregiver neglect, and reporting two or more types of elder abuse with increased hospitalization rates, after controlling for confounders (Dong & Simon, 2013a).
Unplanned hospital readmissions, a quality indicator of a health care delivery failure, are associated with poor patient outcomes and higher Medicare costs of care (Jencks et al., 2009). While overall readmission and mortality rates, as well as hospital costs, for older adults have slowly declined over the years (Krumholz et al., 2015; Zuckerman et al., 2016), it remains imperative to identify and monitor specific patient populations who are at risk for experiencing poor outcomes following hospital discharge, such as those who experience EM. EM is linked to poor health outcomes, such as increasing risk for being hospitalized (Dong & Simon, 2013b) or death (Dong et al., 2009; Lachs et al., 1998; Li et al., 2019; Schofield et al., 2013). Most of the previous work exploring the relationship between EM and outcomes has used prospective cohorts residing in an urban U.S. city (Yunus et al., 2019); little is known about the impact of EM and post-hospital outcomes among older adult Medicare beneficiaries using 100% national data.
Therefore, we aimed to address this gap by exploring whether older adult Medicare Fee-for-Service beneficiaries who are hospitalized primarily for EM are at an increased risk of mortality or needing to be hospitalized again, after controlling for medical conditions and sociodemographic factors. We also examined whether certain types of EM and facilities where care was received had an impact on mortality risk and unplanned hospital readmission rates following hospital discharge. We hypothesized that primary diagnosis for EM places hospitalized older adults at greater risk of mortality and readmission following discharge. We also hypothesized that older adults diagnosed with EM would have a greater risk of mortality and readmission compared to matched controls without an EM diagnosis.
Methods
Sample
The Medicare Beneficiary Summary files (MBSFs) and Medicare Provider Analysis and Review (MedPAR) files from 2015 to 2018 were used to obtain demographics, diagnoses, and hospitalizations, which includes 100% of U.S. Medicare Fee-for-Service beneficiaries. Using the MedPAR file, we selected cases whose first discharge had at least one International Classification of Diseases, 10th Revision (ICD-10) diagnosis code for EM during the period from 10/01/2015 through 12/31/2018. We identified various types of EM, including abuse not otherwise specified (NOS; T74.9, T76.9), where a general EM diagnosis is provided without enough information to indicate a specific type of EM, physical abuse (T74.1, T76.1), psychological abuse (T74.3, T76.3), sexual abuse (T74.2, T74.5, T76.2, T76.5), neglect or abandonment by another person (T74.0, T76.0), and psychosocial circumstances (e.g., at risk for loneliness, codependency, interpersonal relationship problem, and emotional deprivation (Z65.8, Z65.9)). We included patients aged 66 years and older at the time of hospital discharge to examine chronic condition history in the previous year prior to hospitalization when patients were at least 65 years of age and Medicare eligible due to age. We excluded patients who did not have insurance coverage for the previous year or who had Health Maintenance Organization (HMO) coverage. In addition, we excluded patients who were discharged after 9/30/2018 or those who had discrepant death data (i.e., multiple death dates), which allowed us to examine mortality and unplanned hospital readmission rates. We used Centers for Medicare and Medicaid Services (CMS) definition for unplanned readmission, which are admissions to short-term care hospitals for any reason. To compare rates of mortality and unplanned readmission to a general population of Medicare beneficiaries, a control cohort was created. This control cohort consisted of beneficiaries who had an inpatient stay for non-EM diagnoses in the same time period as the cases and were individually matched at a 1:2 ratio based on age category, sex, race, original Medicare entitlement, dual Medicaid eligibility, facility type, and Elixhauser comorbidity index category. The Institutional Review Board of the University of Texas Medical Branch at Galveston approved this study (#21-0040). The Centers for Medicare and Medicaid Services (CMS) approved our Data Use Agreement to obtain the Medicare files.
Sample Characteristics
We extracted age, sex, race/ethnicity, original entitlement (i.e., due to age or disability or end stage renal disease [ESRD]), and Medicaid eligibility from the MBSFs. Age was categorized as 66–70, 71–75, 76–80, 81–85, and 86 years and older. Race/ethnicity was categorized as White, Black, Hispanic/Latinx, or Other. For each discharge, we grouped the type of facilities where care was received, such as acute hospitals (non-psychiatric), psychiatric hospitals, SNFs, or other types of hospitals, based on information from the MedPAR files. Using inpatient claims in the 12 months before the index EM admission, we identified the 31 medical conditions used to calculate the Elixhauser comorbidity index for each patient (Elixhauser et al., 1998). The number of medical conditions in the patient’s record was categorized into 0–3, 4–5, 6–7, and 8 or more comorbidities.
Statistical Analyses
Descriptive statistics were obtained for the sociodemographic factors, comorbidities, facility type, and whether hospitalization was for primary or secondary diagnosis of abuse. The entire sample was characterized by the Elixhauser comorbidities at index admission and stratified by EM type. Kaplan–Meier curves were used to estimate mortality and unplanned readmission by EM type (i.e., physical, neglect, NOS, sexual, and other), primary abuse (versus secondary abuse), and facility type. Other abuse includes psychological abuse and psychosocial circumstances.
We developed univariate and multivariate models using Cox proportional hazards to estimate the hazard ratios (HRs) for mortality by EM type, primary abuse (versus secondary abuse), and facility type. Patients were censored at the end of the study period (12/31/2018) for mortality analyses and at loss of coverage or the end of the study period for readmission analyses. Unplanned readmission risk was evaluated using the Fine–Gray competing risk model (Austin & Fine, 2017), which adjusts for death as a competing risk. Proportional hazard assumptions were tested by Kolmogorov-type supremum tests for all models. For models violating proportionality assumptions, time-dependent covariates were generated to demonstrate the HR for the outcomes before and after 50 days from discharge. Assessment of standardized score process plots for all variables and 50 days was chosen based on non-proportional hazards for facility type (specifically acute and psychiatric hospitals), which occurred around 50 days from discharge (see (e)Figure 1 and (e)Figure 2). Additionally, Kaplan–Meier curves were used to estimate mortality and unplanned readmission for controls. HRs for mortality and unplanned readmission were estimated using Cox proportional hazards to compare between cases and controls, controlling for the matching between cases and controls. All analyses accounted for demographic characteristics (i.e., age, sex, race, entitlement, and dual eligibility) and clinical comorbidities at the index admission. Analyses were performed with SAS version 9.4 (SAS Inc, Cary, NC).
Results
When we examined the number of patients discharged with at least one EM primary or secondary diagnosis, we identified 32,471 eligible patients during our study period, 10/1/2015 through 12/31/2018. We excluded any patient who was not at least 66 years old at the time of being hospitalized, those who did not have continuous Medicare coverage in the prior year, or those who had HMO coverage. After excluding those ineligible for the study, our sample included 12,010 older patients with any EM diagnosis during the index or first hospitalization. For the mortality and readmission analyses, we excluded patients who were discharged after 9/30/2018 to allow for at least 90-day follow-up period or had a discrepant death (i.e., multiple death dates), which resulted in a final analytical sample of 11,023 patients (see eTable 1). The matched control demographics were similar to those hospitalized with an EM diagnosis (see eTable 2).
Patient Characteristics by Elder Mistreatment Type
eTable 3 includes the patient characteristics by EM type. Participants with any EM diagnosis code were majority female (64.1%), non-Hispanic White (74.3%), entitled by disability or ESRD (75.3%), and not dual eligible (61.2%). Only 7.7% of participants had one of the EM types as their primary reason for hospitalization. The majority (65.2%) of participants were cared for in an acute care setting. Neglect by others, other psychosocial circumstances (e.g., codependency), and physical abuse were the three most frequently used EM diagnosis codes. Except for other psychosocial circumstances, females represented the greatest proportion of patients in every EM type.
Medical Comorbidities by the Type of EM (e.g., Physical, Sexual, and Neglect)
A number of Elixhauser comorbidities were identified at index admission (eTable 4), and we explored the type of comorbidities that patients had based on the type of EM diagnosed. The most common comorbidities across all EM types were uncomplicated hypertension (50.8%), fluid and electrolyte disorders (e.g., dehydration; 40.9%), depression (29.1%), cardiac arrhythmia (26.0%), and chronic pulmonary disease (25.3%). Hypertension was the most common comorbidity for all types of abuse, with the exception of neglect by others and not specific abuse, where fluid and electrolyte disorders were higher. Notably, depression ranged across EM types from 17.6% (neglect by others) to 41.9% (not specific psychological circumstances).
EM and All-Cause Mortality Rates
Mortality and Unplanned Readmission by Patient Demographics Among Patients Diagnosed With Elder Mistreatment.
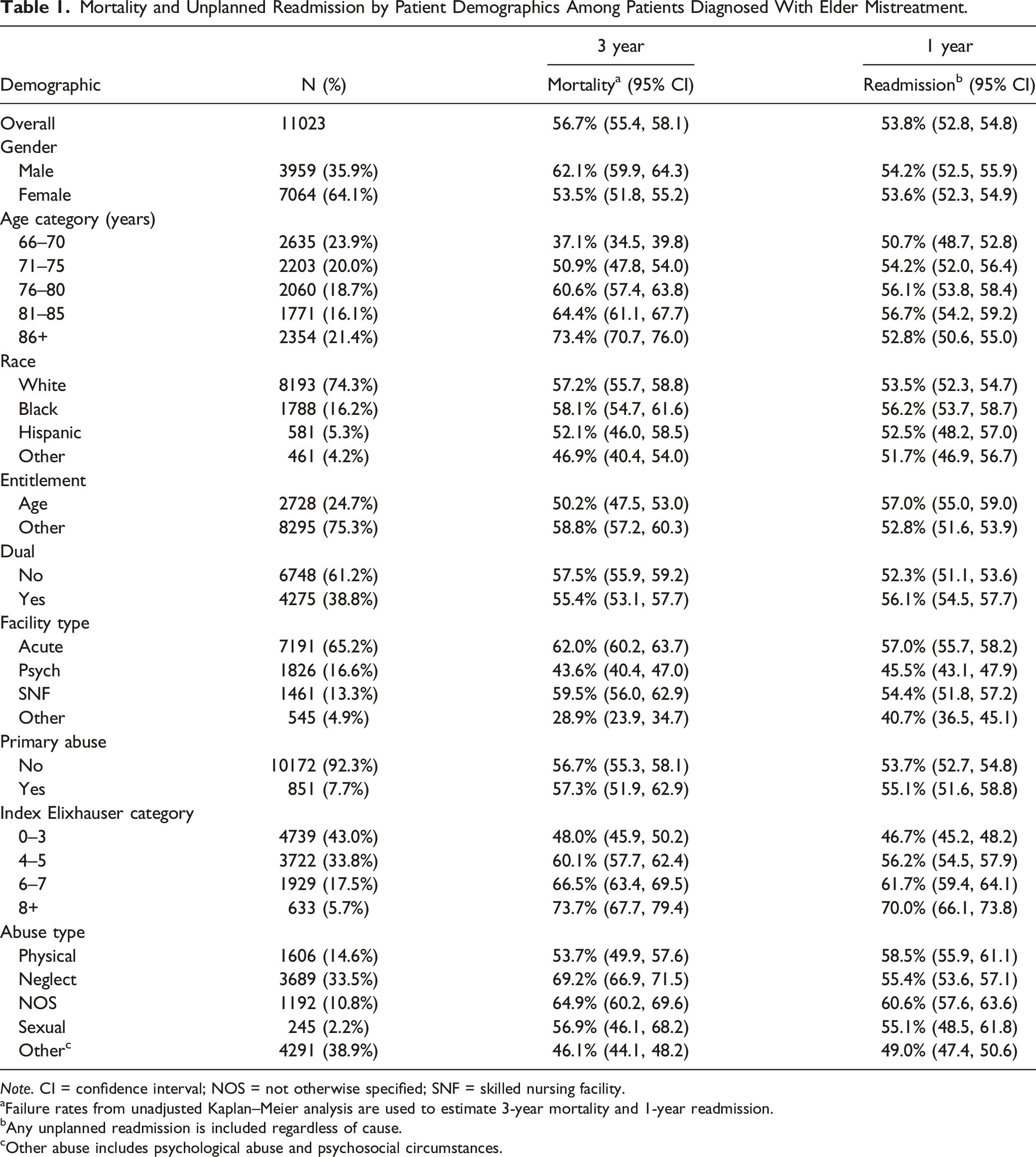
Note. CI = confidence interval; NOS = not otherwise specified; SNF = skilled nursing facility.
aFailure rates from unadjusted Kaplan–Meier analysis are used to estimate 3-year mortality and 1-year readmission.
bAny unplanned readmission is included regardless of cause.
cOther abuse includes psychological abuse and psychosocial circumstances.
Hazard Ratios for Mortality and Readmission Models by Time Among Patients Diagnosed With Elder Mistreatment.
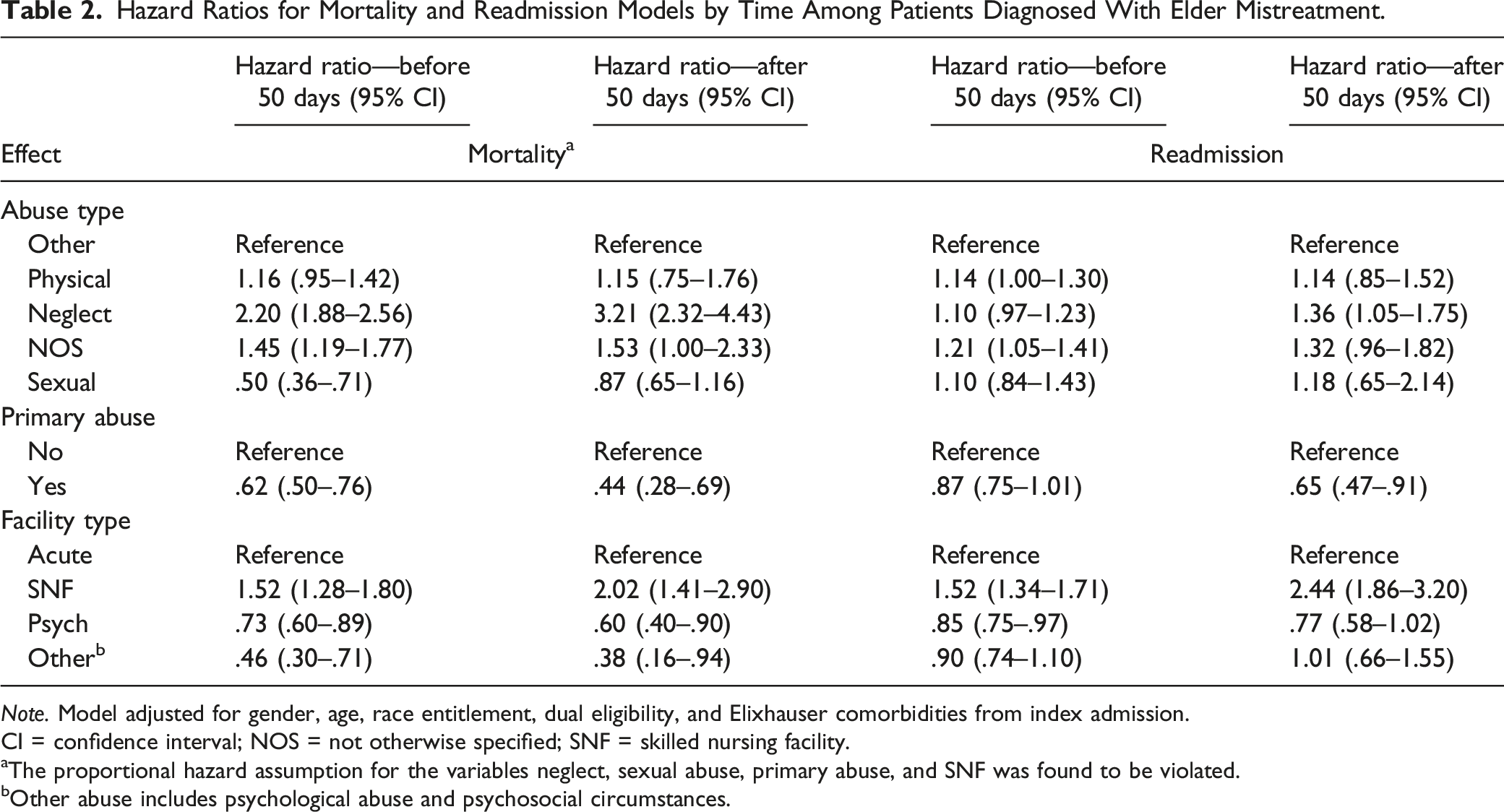
Note. Model adjusted for gender, age, race entitlement, dual eligibility, and Elixhauser comorbidities from index admission.
CI = confidence interval; NOS = not otherwise specified; SNF = skilled nursing facility.
aThe proportional hazard assumption for the variables neglect, sexual abuse, primary abuse, and SNF was found to be violated.
bOther abuse includes psychological abuse and psychosocial circumstances.
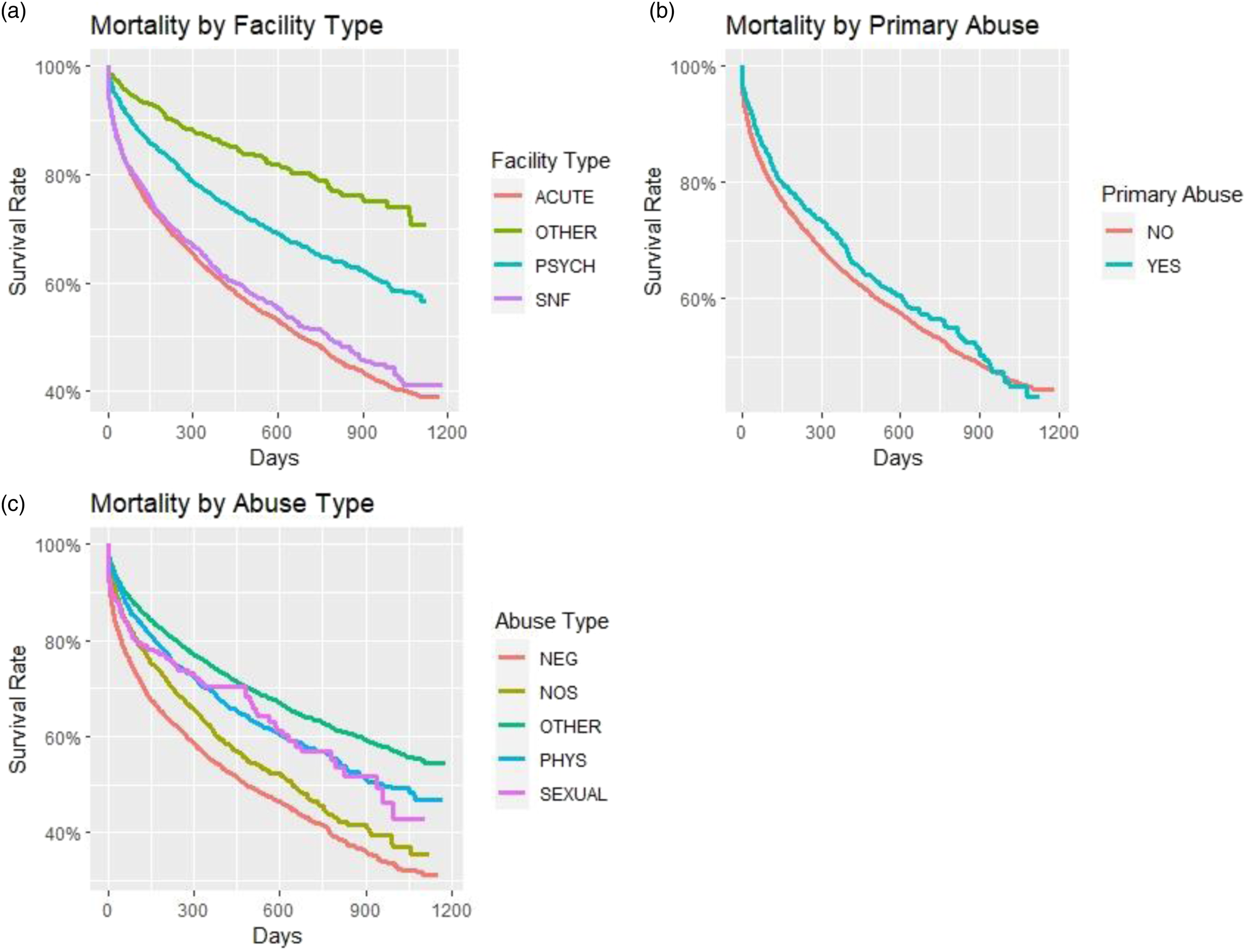
KM curves for mortality by facility, primary abuse, and abuse type: (a) mortality by facility type, (b) mortality by primary abuse, and (c) mortality by abuse type.
EM and Unplanned, All-Cause Hospital Readmission
The overall 1-year unplanned, all-cause hospital readmission rate was 53.8% (Table 1). Patients aged 71–85 years, Black, Medicare entitled by age, dual eligible, or with >3 Elixhauser index comorbidities had higher than average unplanned, all-cause readmission rates. Participants discharged from acute care had the highest unplanned readmission rate (57.0%). Across EM types, unplanned readmission rates were highest for patients who experienced NOS abuse (60.6%) and physical abuse (58.5%). HRs indicate that patients who experienced neglect by others were 1.36 times more likely to be readmitted after 50 days from discharge compared to the reference group (i.e., patients who experienced other EM types) [HR = 1.36, 95% CI = 1.05–1.75] (Table 2). The NOS and physical abuse groups were 1.21 and 1.14 times more likely, respectively, to be readmitted within 50 days from discharge compared to the reference groups of other types of abuse. Before and after 50 days from discharge, patients admitted primarily for EM were at a decreased risk for an unplanned readmission compared to those admitted primarily for other reasons. Compared to patients discharged from an acute hospital, only those discharged from an SNF had an increased risk for unplanned readmission. Kaplan–Meier curves for unplanned readmission by abuse type, primary abuse, and facility type are presented in Figure 2. Readmission risk was then compared between EM patients and non-EM hospitalized patient matched controls. Controls had a 1-year unplanned readmission rate of 48.5% (eTable 2). Those hospitalized for EM had increased risk of unplanned readmission (HR: 1.43, 95% CI = 1.39–1.47) compared to matched controls hospitalized for other causes. KM curves for unplanned readmission by facility, primary abuse, and abuse type: (a) unplanned readmission by facility type, (b) unplanned readmission by primary abuse, and (c) unplanned readmission by abuse type.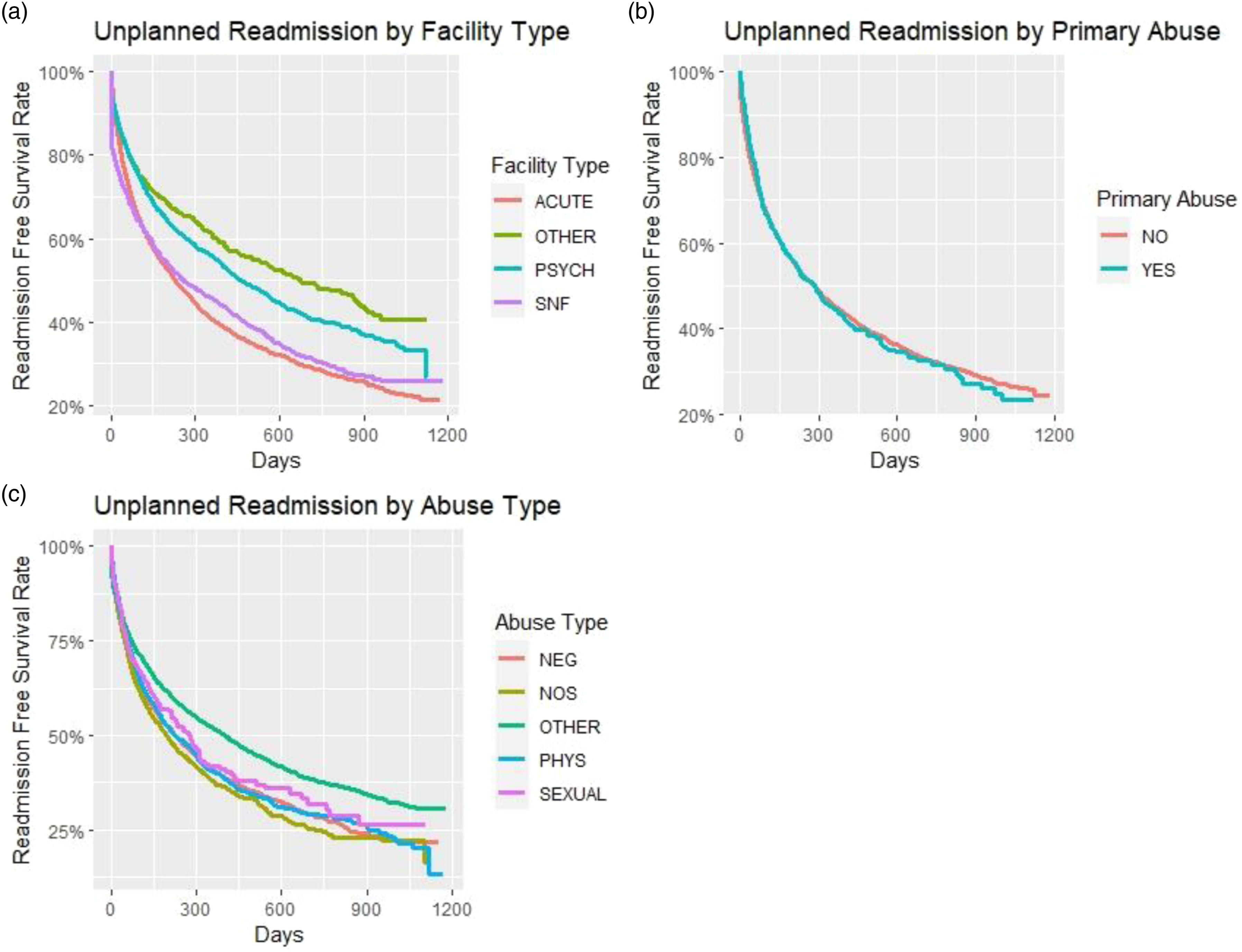
Discussion
Among a nationally representative sample of 100% U.S. Medicare Fee-for-Service patients with an EM diagnosis at hospital discharge, 3-year mortality was 56.7% and 1-year all-cause unplanned readmission rate was 53.8%. We identified several EM types associated with a risk of mortality or unplanned readmission. A primary diagnosis of EM was associated with a decreased risk of mortality and unplanned readmission. SNF patients were at an increased risk for mortality and unplanned readmission compared to those discharged from an acute hospital. We also found that those who were hospitalized for EM were at an increased risk of both mortality and readmission compared to hospitalized matched controls.
Older adults hospitalized for confirmed or suspected neglect by others had the greatest impact on overall mortality. This finding is consistent with previous research. Caregiver neglect had the lowest 5-year survival rate compared to other abuse types among community-based older adults with substantiated cases of elder abuse in Texas (Burnett et al., 2016). Lachs et al. found that community-dwelling survivors of EM (i.e., abuse, neglect by others, and exploitation) in New Haven showed an increased risk for 3-year all-cause mortality (odds ratio [OR] = 5.10; 95% CI = 2.80–9.50) (Lachs et al., 1998). Recently, Li et al. determined that caregiver neglect was associated with greater risk of 1-, 3- and 4-year mortality (Li et al., 2019).
Our study also found that neglect, physical abuse, and non-specified abuse were associated with an increased risk of an unplanned readmission. However, after 50 days from discharge, only those who experienced neglect by others were still at increased risk for an unplanned readmission, which suggests the need for improved transitional care in older adults admitted for EM. Unplanned hospital readmissions among Medicare patients are costly, with annual costs totaling over $17 billion (Jencks et al., 2009). It is possible that those who experience neglect by others, physical abuse, or non-specified abuse are most likely to be the most vulnerable older adults. Those who experience neglect by others may have extreme functional impairments that place them at greater risk for readmission. Based on data from the Health and Retirement Study linked to Medicare claims (Greysen et al., 2015), individuals who were dependent with three or more activities of daily living had 18.2% greater risk of readmission (OR = 1.42; 95% CI = 1.20–1.69).
Sexual abuse was unexpectedly associated with a decreased risk of mortality when compared to other EM types. Only 2.2% of our total EM sample had a suspected or confirmed sexual abuse diagnosis, and among them, 18.4% had a primary diagnosis of sexual abuse. Acierno and colleaguesreported a .6% prevalence of sexual mistreatment in the prior year, of which only 16% were reported to the police (Acierno et al., 2010). Therefore, the actual prevalence of sexual abuse may be much higher. Previous studies that have examined the association of EM and mortality have either combined sexual abuse with other EM types or excluded this category due to low occurrence. Thus, there is limited data available on the prevalence of sexual abuse of older adults. These findings indicate the need for enhanced screening and assessment of sexual abuse among older adult patients.
Patients with a primary EM diagnosis were at a decreased risk for mortality and unplanned readmission. A primary EM diagnosis perhaps prompted early APS or other caregiving intervention that may have mitigated the effect of neglect by others on future mortality or readmission. In addition, a number of factors might be associated with poor care transitions placing patients with comorbidities at risk for readmission, such as not receiving appropriate follow-up care, lack of advanced care planning near the end of life, delay in follow-up visits with primary or specialty care following discharge, and poor medication management of chronic conditions (Ouslander et al., 2020). This finding also underscores the need for comprehensive assessment of EM in patients hospitalized for co-morbid medical causes to assess any additional health risk factors and to plan to mitigate risks for hospital readmission and mortality that occur when EM is present with other medical concerns.
Interestingly, in our study, SNF patients were at an increased risk for both mortality and unplanned readmission compared to those discharged from an acute hospital. Individuals in an SNF might have already experienced EM and other adverse life events, which contributed to their placement in an SNF. Although each state operates APS differently, when cases are confirmed, additional services might be provided, such as placement in a nursing home or long-term care facility. APS referrals for EM (including neglect by others) and self-neglect are among the stronger predictors of SNF placement (Lachs et al., 2002). Recently, caregiver neglect (RR 4.73; 95% CI = 3.03–7.40) had the greatest increased rate of SNF placement compared to other types of elder abuse (e.g., psychological, physical, and financial exploitation) (Dong & Simon, 2013c). In addition, nursing homes are unfortunate settings for abuse or neglect by others among older adults. Although there is scarce data on the prevalence of EM in institutional settings, Yon et al. indicated that the prevalence is high (Yon et al., 2019). Over 64% of staff admitted to elder abuse in the prior year, and the prevalence estimates were highest for psychological abuse (33.4%), followed by physical (14.1%), financial (13.8%), caregiver neglect (11.6%), and sexual abuse (1.9%). Given that nursing home residents are at a greater risk for mortality and readmission compared to those in an acute care setting, improved discharge planning and advance care planning are needed for individuals at risk of mortality or readmission, particularly vulnerable groups such as those with multimorbidity, cognitive impairments, frailty, or disability.
Of note, in this population suspected of EM exposure, having been admitted to a psychiatric hospital decreased mortality by 15%. The impact of psychiatric hospitalization is not clear; however, we postulate that admission to a psychiatric hospital may protect those older adults who are especially vulnerable to abuse: those with cognitive and behavioral disorders. Perhaps psychiatric hospitalization provides respite to caregivers coping with these difficult situations and thus allows for the de-escalation of potentially violent encounters, protecting these older adults from EM.
Limitations
Our analysis has some limitations. Our use of ICD-10 codes for EM relies on the accuracy and subsequent documentation of suspected EM by health professionals, which is often under-detected and under-reported (Beach et al., 2016; Krueger & Patterson, 1997; Phelan, 2012). Even when EM is identified, it might not be coded due to unclear reimbursement and uncertainty of the impact of EM codes on a hospital’s payer mix (Rovi & Johnson, 2003). Safety concerns can also prevent EM disclosure if medical staff have insufficient training and attention to patient needs. We suggest that the EM codes in the claims used in this study likely represents the most obvious, egregious incidents of EM. We only included the ICD-10 codes for neglect or abandonment by others; we did not include EM codes for non-specific self-neglect or self-neglect due to insufficient food or water intake. Furthermore, we combined psychological abuse codes with psychosocial circumstances codes into an “Other” category. The ICD-10 codes for psychosocial circumstances have multiple uses, such as loneliness, codependency, or emotional deprivation, which we believe are closely related to EM, similar to other studies (Evans et al., 2017; Mouton et al., 2019). We excluded individuals with HMOs; therefore, our results may not be generalized to them. Older adults with Medicare Advantage or private insurance are diagnosed with EM much lower than population-based prevalence (Rosen et al., 2021) Similar to most of the elder mistreatment literature, our sample lacked racial/ethnic diversity with majority classified as non-Hispanic White. Race/ethnicity was based on claims data, but methods have been used to improve the estimation of ethnic minority beneficiaries (Eicheldinger & Bonito, 2008). In addition, we did not have the living situation of most of the patients included; therefore, we are unable to determine the role of social isolation or loneliness or low social networks in readmission and mortality risk.
Despite these limitations, our study has several strengths. We were able to use claims data in a 100% Medicare Fee-for-Service sample to provide insight into the prevalence and types of EM and the association of this diagnosis with adverse outcomes following hospitalization compared to matched controls. We also found that EM exposure had an impact on readmission rates, a key quality of care measure. Future work should consider using post-acute and outpatient claims to explore the prevalence of EM in these settings. In addition, future work should longitudinally explore patterns and continuity of care prior to and following EM diagnosis to identify potential time points when healthcare providers could identify patients at risk for EM and those at risk of adverse outcomes following an EM diagnosis. Lastly, the development of a comprehensive identification approach to detect EM would help to identify older adults at risk for EM, and help medical and social work hospital staff promote strategies to improve outcomes for this population.
Conclusion
This study demonstrates that EM is associated with higher rates of mortality and all-cause unplanned readmission among older adult Medicare Fee-for-Service beneficiaries compared to non-EM patients. Elder neglect by others placed older adults at 2–3 times increased risk for mortality and 10%–36% increased risk for unplanned readmission compared to other EM types. Older adults discharged from an SNF were also at an increased risk of both mortality and unplanned readmission compared to other facility types. Greater attention is needed for early intervention of EM or caregiver neglect as well as for those being discharged from an SNF who are at an increased risk of adverse outcomes following EM.
Supplemental Material
Supplemental Material - Risk Factors for Post-Discharge Adverse Outcomes Following Hospitalization Among Older Adults Diagnosed With Elder Mistreatment
Supplemental Material for Risk Factors for Post-Discharge Adverse Outcomes Following Hospitalization Among Older Adults Diagnosed With Elder Mistreatment by Monique R. Pappadis, Leila Wood, Allen Haas, Jordan Westra, Yong-Fang Kuo, and Charles P. Mouton in Journal of Applied Gerontology
Footnotes
Acknowledgments
The authors acknowledge Sarah Toombs Smith, PhD, ELS, for editing this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The contents of this publication were developed under grants from the National Institute on Aging [NIA grant numbers R61AG078519, K01AG065492; P30AG024832; P30AG059301], National Center for Advancing Translational Sciences/National Institutes of Health [NIH grant number UL1TR001439], and the National Institute on Minority Health and Health Disparities [NIMHD contract number L60MD009326L]. The views, opinions, and/or findings contained in this article are those of the authors and should not be construed as an official institutional position or any other federal agency, policy, or decision unless so designated by other official documentation. The contents of this publication do not necessarily represent the policy of the National Institutes of Health, and you should not assume endorsement by the Federal Government.
IRB Protocol/Human Subjects Approval Numbers
The Institutional Review Board at the University of Texas Medical Branch at Galveston approved this study [IRB # 21-0040].
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.