
Abstract
End-of-life Goals of Care (GoC) discussions aim to support care that is consistent with patients’ preferences and values. This study uses an exploratory qualitative design drawing upon a social constructivist epistemology to examine family carers’ perspectives on GoC within acute Australian hospital settings. Twenty-five family carers of aging inpatients were recruited from six Australian hospitals to participate in recorded, semi-structured interviews. Data were transcribed and analyzed using reflexive thematic analysis. Three main themes were developed. Theme 1 explored carers’ experiences of GoC discussions—identifying varying levels of preparedness and carers' hopes for open, two-way discussions initiated by empathic Health Care Professionals (HCPs). Theme 2 examined carers’ unmet needs for time, space, consistency, and support to make careful decisions. Theme 3 identified carers advocating for patients' needs when they could not do it themselves. Preparing carers and normalizing GoC discussions relating to end-of-life care maximizes benefits for patients, carers, and HCPs involved.
• Family carers need clarification about the purpose and meaning of GoC discussions and why it is important when caring for aging family members. • Greater death literacy needs to be promoted for older patients and their families so that they can openly discuss their values and preferences.
• Increasingly, it is necessary to normalize GoC discussions as health services institute policies that all patients admitted to the hospital are asked about their goals and preferences as part of treatment planning and preferred options for end-of-life care. • Adopt a flexible, tailored approach to GoC discussions to meet carers' often conflicting and complex needs. • Effective interpersonal communication benefits both carers and their family member and reduces the burden experienced by HCPs.What this paper adds
Practice implications
Introduction
The burden and complexity of physical illness and disability associated with aging populations mean health services globally need to understand better the preferences of the people they care for and the views of their family carers so that the health and social needs of individuals at the end of life can be better met (Bone et al., 2017).
The “Goals of Care” (GoC) framework advocates focused discussions with patients with serious and life-limiting illnesses to participate in shared decision-making in collaboration with Health Care Professionals (HCPs) and their chosen family/support persons to develop a plan of care that is consistent with the patients’ values and preferences (Brimblecombe et al., 2014). Moreover, some Australian hospitals are adopting new policies to undertake GoC discussions for all patients over 65 years, regardless of their diagnoses (O'Connor et al., 2020). GoC discussions aim to ensure that patients who are unlikely to benefit from curative medical treatment will receive care that is consistent with their wishes (Thomas et al., 2014), reduce the risk of non-beneficial and/or futile treatments and hospitalizations (Cardona-Morrell et al., 2016), and increase the use of palliative care or hospice services (Riedl & Schüßler (2017). Conceptually, GoC differs from advance care planning and advance directives because GoC conversations are held in the context of an immediate illness or acute episode of care (Leblanc et al., 2023). The concept of GoC is increasingly used worldwide, but research publications largely focus on the North American health system (Secunda et al., 2020).
Goals of Care has been studied widely in settings such as oncology (Lin et al., 2018) and palliative or hospice care (Boa et al., 2014). In contrast, only a few studies have explored GoC with patients with non-cancer diagnoses (O’Connor et al., 2020). Further, very few studies examine acute general hospital settings, which are challenging settings in which to undertake GoC discussions (Leblanc et al., 2023), particularly when there is a lack of clarity and consensus amongst HCPs about the purpose of these discussions (Hanning et al., 2019) and uncertainty exists regarding how best to involve patients and their families (Secunda et al., 2020). In addition, the need to initiate end-of-life discussions is often poorly recognized within acute hospital settings as the final phase of life is harder to predict in cases of organ failure and advanced chronic diseases, and cessation of life-prolonging treatment cannot always be delineated with poor communication more evident when patients suffer from non-cancer diseases (Bolt et al., 2016). However, patients in acute care settings were reported to be willing to talk about death and dying, but only if these conversations were done well (O'Connor et al., 2020).
Further investigations exploring family carers’ experiences of GoC are required as most studies have been undertaken from the perspective of clinicians or patients (Vermunt et al., 2017) and the literature on how HCPs can best support family carers is sparse. The involvement of family members in GoC is often viewed negatively by HCPs, where families are perceived as resistant to addressing end-of-life issues, having unrealistic expectations, and fail to understand the limitations and complexity of life-sustaining interventions (Aleksova et al., 2016; You et al., 2015). Oncologists have identified many challenges in time-consuming discussions with multiple family members and difficulties managing family distress and conflicting family dynamics. (Lin et al., 2018).
Carers’ views about end-of-life care have been examined in residential aged care (Gonella et al., 2019), hospice or palliative care (Hughes et al., 2019), and dementia care settings (Ma et al., 2021; Cresp et al., 2020). Survey findings on end-of-life care reported that most patients were comfortable with family members being surrogate decision-makers. However, they often hold contradictory views about end-of-life options, appropriate care and stopping treatment (Ang et al., 2016; Bolt et al., 2016). Current North American evidence practice updates for GoC (Leblanc et al., 2023) only consider the carers’ role concerning patients who are minors. However, studies examining advance care planning from non-western perspectives (Miyashita et al., 2021; Wang et al., 2022) have advocated more family-inclusive practice concerning GoC. In conclusion, no studies have specifically examined carers’ experiences of GoC discussions in Western acute hospital settings.
This study aimed to explore in-depth carers’ experiences of GoC discussions. The findings will identify areas for improvement and inform the development of an educational intervention for hospital-based clinicians tailored to carers’ needs.
Methods
Design
Our research used an exploratory qualitative research design drawing upon a social constructivist epistemology. Meaning is viewed as socially constructed by people’s interpretation of their experiences (Creswell, 2013). Ethics approval was obtained from the relevant Australian Human Research Ethics Committees at Curtin University, Western Australia (EC00270) and Monash University (HRE2018-0404).
Study Setting and Participants
A convenience sample of 25 adult carers was recruited from six metropolitan hospitals in two Australian states implementing the GoC framework for all patients aged over 65 years old regardless of diagnosis. The GoC framework aims to help patients (and their nominated family members) understand their condition and make appropriate treatment decisions (including the level of resuscitation) aligned with the patients' preferences. Policies for the hospital sites studied recommend that experienced doctors who have received GoC training lead the discussions (Waldron et al., 2016).
Carers were eligible if they had provided care to a seriously ill older patient and been involved in GoC discussions with HCPs during the patients' current (except for one) hospital admission. Carers of patients receiving palliative care or with cancer diagnoses were not recruited for the study. Initial approaches to participate in the research were made by senior nurses/managers (18 participants) and doctors (seven participants), and consent was obtained for their contact details to be given to the researchers. Informed, written consent was gained from participants prior to conducting interviews. As participants were potentially vulnerable, the research team did not participate in GoC discussions and was independent of the clinical settings studied.
Characteristics of Participating Carers (N = 25).
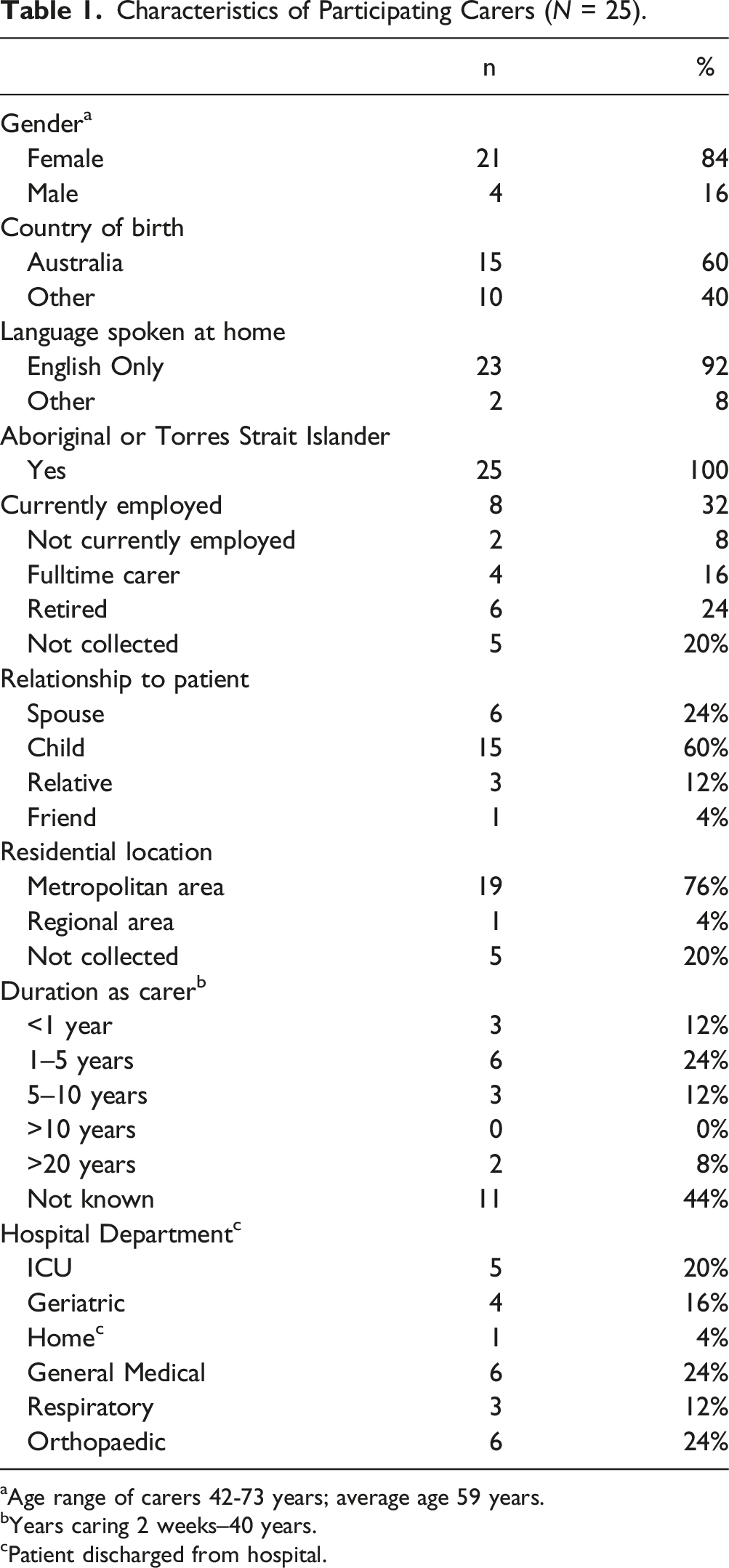
aAge range of carers 42-73 years; average age 59 years.
bYears caring 2 weeks–40 years.
cPatient discharged from hospital.
Interview Data Collection
Semi-structured interviews to explore carers’ experiences were conducted using an interview schedule developed by the research team with reference to the available literature (see Appendix A). Audio-recorded interviews were conducted face-to-face or via telephone, lasting between 13 and 55 minutes (mean of 22 minutes). Interviews were conducted between October 2018 and July 2019 by KW, JS, and JJ. All interviewers were experienced in conducting sensitive interviews, so issues of trust and professional power were explored to elicit participants’ experiences and reflections.
Data Analysis
Interviews were transcribed verbatim, and data were analyzed using Braun and Clarke’s (2006) reflexive thematic analysis, following their six phases (familiarization, initial codes, search for and reviewing themes, defining and naming themes, and writing the final report). Authors KV and JJ randomly selected four transcripts and coded these independently for initial concepts. KV, MO, and CJ met to ensure consistency on the identified coding categories before JJ coded the remaining transcripts. Information power was used to decide when to cease recruitment and to examine the data’s richness, depth, and relevance to the study aims (Malterud et al., 2015).
Reflexive thematic analysis was adopted (Braun & Clarke, 2021) by the interdisciplinary research team (comprised of psychology, nursing, and medical specialties) that brought diverse viewpoints to the final construction of themes and examples; any disagreements were resolved by consensus discussion (Bradbury-Jones, 2007). A component of reflexive thematic analysis is an ongoing reflexive practice, which includes questioning and reflecting on all decisions and assumptions throughout the analysis (Braun & Clarke, 2021). In addition, an audit trail was maintained, and reflexive journaling was used.
Reflexive thematic analysis was enriched by our shared interests as a research team in improving communication about end-of-life care and influenced by our diverse personal histories of death and losses, including many who were also involved in the care of aging relatives. Our positions as carers and HCPs helped us appreciate multiple perspectives and reflexive analysis enabled us to make these different perspectives transparent and explicit when analyzing and interpreting the data. We acknowledged poor experiences of GoC conversations and identified carers’ unmet needs while recognizing the workload burdens on HCPs. The Consolidated Criteria for Reporting Qualitative research checklist (Tong et al., 2007) was used to guide the development of the research team, the study design, analysis, and reporting of findings ensuring the quality and trustworthiness of the qualitative research design.
Results
Three major themes were developed from the data regarding carers’ perspectives on GoC discussions. Theme 1 explored carers’ experiences of GoC discussions—identifying varying levels of preparedness, though recognizing that knowing patients’ wishes and preferences affected how these conversations unfolded. This theme identified carers' hopes for open, two-way discussions initiated by empathic HCPs. Theme 2 examined carers’ unmet needs for time, space, consistency and support to undertake challenging GoC discussions for making careful decisions. Theme 3 identified carers wanting to advocate for patients, especially if they had cognitive decline or were from a non-English speaking background.
Theme 1. Carers’ Experiences of Goals of Care Discussions
This theme explored carers’ varying levels of preparedness when GoC discussions were initiated with them and carers had different understandings of the need for GoC discussions. Participants reported being caught off-guard, feeling confused, and finding these discussions distressing. Whether or not carers know the patients' wishes beforehand is very influential in how GoC conversations unfold. Participants described the variations in the depth of discussions with the patient and knowing their preferences for treatment.
Some carers experienced shock, finding the discussion confronting: [HCP]goes, ‘That’s a do not resuscitate.’ And I'm like, 'Why? What's happening?' You're just so confused…And he said, 'No, … if something did happen, if the worst happens, we need to know what you want us to do.' That was the first conversation we had and it's just like bam! In your face! They're used to dealing with death every day. As someone's wife you're not. (C4)
Others commented on the absence of prior conversations with their family member about their end-of-life preferences and wishes, as C5 explained: “She’s never really been that unwell so we’ve never ever had to really bring that conversation up… about life support.” This impacted the burden experienced by carers: “You can’t expect me to answer what he wants when things go wrong. Yes, we have been married for 42 years but what he really wants or thinks may not be what I think he wants. It’s distressing.”
Participants had difficulty having end-of-life discussions when family members appeared unwilling or unable to think about or discuss life-prolonging measures. These discussions were particularly challenging when patients had cognitive deterioration, as C15 explained: “I can’t rely on mum… her mind’s starting to go. So that’s why I discussed it with…every immediate family…”
Other participants, while not having had direct conversations with the patient, were comfortable making informed guesses about their preferences: When the doctor asked me…what did I think that [Patient] felt?… And I said, ‘Well, he's really upset about his sister who's bedridden… And I know he does not want to be like that…all of the important parts of those discussions come and gel into one. (C3)
Many acknowledged that there was no ideal or right time to have GoC discussions but preferred having such discussions early. C5 explained, “… if the patient is quite seriously ill…. that decision needs to be made.” In contrast, other participants expressed confusion about the need for proactive discussions: “it was through family members who spoke to me and said ‘no, this is normal. They have to explain this to you. We’ve all had that. Don’t worry.’ So, it was actually from outside that I then understood” (C5). Another participant expressed uncertainty about the need for GoC conversation: “…maybe if the person goes in [hospital] for something that’s not life-threatening and they don’t think there’s any chance of it [deterioration] happening, maybe they don’t need to ask these questions.” (C10) In contrast, other participants reported that the timing was appropriate and well-informed. They were given sufficient time to consider these decisions, especially when they reflected on previous discussions between the patients, carer and/or clinician. As C1 reported, “I wasn’t making a decision that hadn’t already been discussed…”
Theme 2. Carers’ Needs for Time, Privacy, and Empathy
The second theme identified carers’ unmet needs during GoC discussions that contributed to their poor quality experiences. Participants reported needing adequate time to digest and think things through, needing physical privacy for holding sensitive conversations, and needing consistent information and processes from the clinical team.
Participants reported needing sufficient time for HCPs to explain, answer questions, and support their decision-making. The availability of HCPs and allocation of time to answer questions from the family was viewed as an important aspect of GoC discussions, with some participants recalling inadequate time—one being given “5 minutes, tops” (C2). This resulted in participants such as C4 reporting HCPs were “so pushy” when they were “too upset” to “take everything in” and they needed “time to think it through” and to consult with other family members and to consider the options. C5 too, reported confusion and feeling overwhelmed: “I felt like I had to make that decision there. and they’re standing there… you just feel, ‘oh my gosh, I’ve got to do this quickly and I don’t really understand, but perhaps this is the right way to go” (C5).
The location of the GoC discussion varied widely, but the need for privacy was a recurring requirement. Some carers reported that discussions occurred in public spaces and were upset by the lack of privacy: Firstly, have struggled to find a place for us to have the conversation with the doctor, so we ended up having it in the waiting room amongst other people… It was a bit uncomfortable…because the door was sliding open and people were walking in and out, sitting next to us … my sister and I couldn’t just sort of turn into blubbering messes …(C8)
Other participants were afforded appropriate privacy in designated offices, the relative’s room, or a bookable space. C12 recounted appreciating her current experience where “four doctors took us to a separate room” which contributed to it being the “best experience I’ve had”. Having GoC discussions within the patient’s room allowed the patient to be present even if they could not actively participate. The shared decision-making reduced the burden for some caregivers: She [mother] was not being left out of any discussions, decisions, even though she couldn't make them. It was right in front of her like sometimes the eyes were open, sometimes they weren't. Sometimes she could nod her head or shake her head. (C1)
In contrast, other participants expressed discomfort when discussions occurred near a patient’s bedside, worrying this might cause distress: “I don’t know whether Mum overheard the conversation but at that point, that might have been a bit worrying for Mum.” (C10)
These open and honest conversations gave participants a sense of clarity and relief. “It … empowered us with the knowledge of what the likely outcomes were and what to expect, and just set your mind at ease…although the news wasn’t good.” (C20). The discussions led carers to consider the impact of life-prolonging measures on the patient and their quality of life: "…I can understand why they would ask that question [about resuscitation]… I didn’t realize but if it’s starting to cause so much damage, that the majority of people don’t survive all that long afterwards anyway, is there any real point?” (C10)
Carers described their views on communicating for quality and valuing “open”, “empathic and calm” approach by HCPs: “It means a lot when the consultant is calm himself or herself and understanding our emotions … and the time that he took with us, which was really, really important” (C2).
Similarly, a style that invited two-way dialogue was appreciated, “It was friendly, an open and two-way conversation [sic]; they didn’t tell me what to do… so the communication was clear but also not stuffy or formal” (C9). Some participants found supportive communication by HCPs made the decision-making less burdensome. C5 reported feeling reassured: ‘“[I said] Is this right?’ And she [HCP] said, ‘I feel that’s a good decision for you and for your mum.’”
Additionally, the opportunity to ask follow-up questions was greatly appreciated, “…before they [doctors] leave, they always go ‘right, are you alright now?’ …' if you need to talk anymore, just let one of the nurses know'" (C1). C14 appreciated the opportunity to address follow-up questions: “…I interrupted him [Consultant]and said, ‘… could you repeat what you said to me?’ And he did it without a problem, to [answer] … a million questions again from the rest of the family.” Carers voiced their appreciation for the use of simple language by HCPs. However, they reported some instances of confusing medical jargon and unfamiliar acronyms such as DNR and CPR. “Well, that terminology. ‘Goals of Care’ again. I think when I heard it the second time, I still wasn’t that clear….” (C5).
All participants reported that GoC discussions were led by doctors and expected this as “the only person that could really answer that [the questions] is the doctor who is treating the patient.” (C6) and having the perceived medical authority. “…[I]t’s how we view hierarchy, isn’t it? You know, if it’s coming from a doctor…” (C3). However, some participants expressed concern that some doctors were unsuited to lead such important and deeply sensitive discussions. A seeming lack of empathy or awareness by the HCPs negatively affected the quality of the conversation. Some doctors were considered “cold” (C4), “too matter of fact” (C8) or “dispassionate” (C10), and “abrupt” (C5) when having these discussions. Others described doctors’ communication styles as “straightforward” (C1) and “forthright” (C13) and that the communication “could have handled it differently”(C22).
While all participants acknowledged the doctor’s role, the potential for other HCPs to lead GOC discussions was raised. Nurses were suggested as they were seen to possess both extensive medical knowledge and have a deeper understanding of patients' personal circumstances and a more consistent presence on the ward than doctors. As C1 explained, “I’d be happy with that nurse telling me because she’s probably the person I would see the most out of everybody”. C10 and C12 suggested that chaplains, priests, and social workers may be more appropriate than doctors because they were viewed as more empathic.
Theme 3: Wanting to Advocate for Patients
If carers perceived the patients’ own needs were being overlooked by the clinical team, carers wanted to be the patient’s voice and to advocate for them. The following examples highlights potential misunderstandings of GoC especially when patients and families are from culturally and linguistically diverse backgrounds: I said, 'No, I'm not going to let my mum die like that. I just want to know why did you stop the treatment so quickly this time?' And they said it was because it was her wishes…… I knew my mum can't speak English, cannot understand any English and I knew Mum;… she was looking forward to joining us for these events and she didn't want to die … you know, it’s just because she refused the mask, they think it was her wish to die.” (C11)
C27 concurred on needing to advocate for patients when they could not do so for themselves: “I’m his voice and I’m his eyes, and I’m his ears. He’s 88 and forgetting and he’s not understanding the second language like he used to. And so, I have to make all the decisions about everything for him because he simply cannot.” C22 also reported similar concerns for their parent “…if I missed the doctors there was no one who could advocate for my mother …or tell me as a primary caregiver what they had said.” Sometimes family members felt they had to advocate for the needs of patients with other family members who held conflicting viewpoints: “I think it is only today that it's actually hit him [partner], how serious the situation is and how important it is to value [patient’s] integrity… [W]e need to respect [patient’s] wishes and …her dignity…” (C2)
Discussion and Conclusions
This study aimed to explore carers' perceptions and experiences of GoC discussions during a relative’s hospitalization. GoC discussions occurred in high-pressured, acute hospital environments where the needs of carers can be overlooked or misunderstood. While it is ideal if GoC discussions are undertaken with HCPs who have prior knowledge of the patient and their family, this is only sometimes possible in an acute hospital setting contributing to varying experiences by our participants. Several important findings from this study need to be highlighted: (i) Confusion about the purpose and meaning of GoC discussions, (ii) discomfort, anxiety and concern experienced by carers about what the conversation means for the patient and their illness, (iii) challenges for carers making GoC decisions when they have never openly discussed this with the patient, and (iv) carers' perspectives on the barriers and enablers to having better GoC discussions.
There are key messages to prepare carers and address their needs in GoC discussions. Prior experience with GoC discussions helped to shape carers' comfort and readiness for GoC discussions and decision-making (Shaw et al., 2018). Promoting greater death literacy (Noonan et al., 2016) can enable older patients and their families to openly discuss their values and preferences and advance care planning before individuals are faced with severe illnesses and/or hospitalization. Third, preparing carers and normalizing GoC discussions will maximize the benefit for the patient, carer, and HCPs involved (Vermorgen et al., 2021). Our study highlighted the importance of doctors, patients, family, and carers having a shared understanding of what has been discussed and the subsequent plan of care developed and documented. The amount of information provided by HCPs can be overwhelming, and the use of complex medical jargon leads to confusion and misunderstandings. Participants appreciated honest, open, empathic communication styles and opportunities for further follow-up communication. These findings reflect previous research with patients who found the process confronting but valued having their voices heard (O'Connor et al., 2020).
Given the limited understanding of the GoC process by carers in our study and the potentially distressing nature of some conversations, there is a need to ensure that patients and families are informed of hospital policies to undertake GoC discussions. Increasingly, it is necessary to normalize such discussions as hospitals implement policies that all patients admitted to the hospital are asked about their goals and preferences as part of treatment planning and appropriate end-of-life care. The Australian Commission for Safety and Quality of Care in Hospitals has developed extensive guidance for health professionals to undertake such discussions (Shaw et al., 2018). However, translation of this into practice remains a work in progress at the time of this research.
Time constraints have been identified by doctors as a challenge to undertaking GoC discussions with patients and families (Waldron et al., 2016) and were considered a barrier in our study. Carers in our current study and patients in previous research (O’Connor et al., 2020) have indicated that nurses and allied HCPs were considered a reasonable alternative to conduct GoC discussions. However, team roles and hierarchical structures within acute hospitals remain a barrier to other HCPs leading in the GOC process (Wittenberg et al., 2016). Nevertheless, doctors and nurses agree that it is acceptable for experienced, skilled HCPs working within a multi-disciplinary framework to facilitate GoC discussions (Stephens et al., 2021). Effective interprofessional communication among HCPs when conducting complex GoC conversations benefits carers and reduces the burden experienced by HCPs (Stephens et al., 2021).
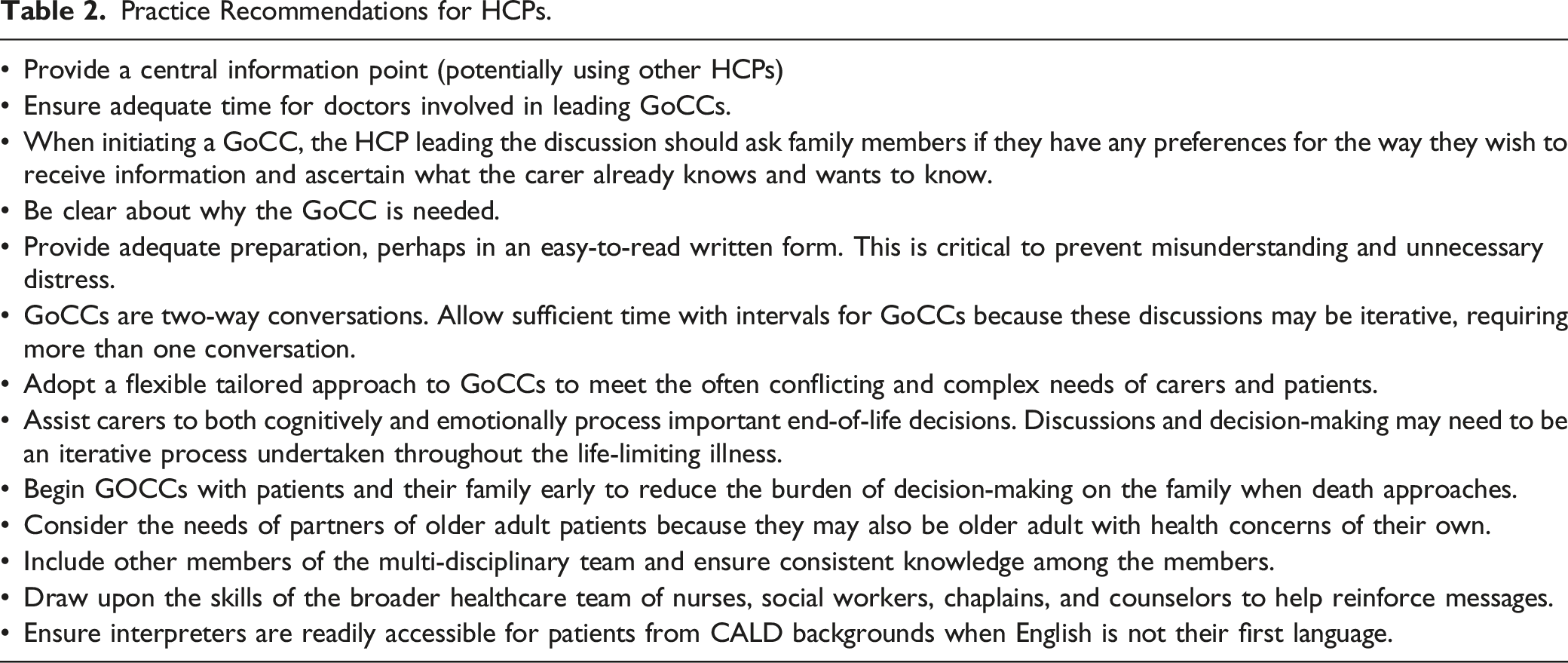
Practice Implications and Recommendations
Limitations
Practice Recommendations for HCPs.
Conclusions
As people age, they often experience physical deterioration, increasing comorbidity, and cognitive decline. Correspondingly, there is increasing reliance on family members to help them understand and negotiate complex healthcare pathways. This process necessitates understanding their illness and its trajectory to make appropriate decisions about treatment. Given that family members are sometimes called upon to negotiate patients' wishes in an acute hospital setting, educating and preparing carers for GoC discussions and providing appropriate support is imperative. Given that GoC has become a core requirement in medical settings, HCPs must build the interpersonal and interprofessional skills needed to communicate effectively in this triadic relationship of HCP–patient–carer.
Supplemental Material
Supplemental Material - Family Carers’ Experiences of Goals of Care Conversations in Acute Hospital Settings
Supplemental Material for Family Carers’ Experiences of Goals of Care Conversations in Acute Hospital Settings by Kitty Vivekananda, Jayamini S. Jayawardene, Moira O’Connor, Kaaren J. Watts, Anton D. Leonard, Sharon Keesing, Georgia Halkett, Josephine Shaw, Valerie Colgan, Kevin Yuen, Renate Jolly, Simon C. Towler, and Anupam in Journal of Applied Gerontology
Footnotes
Acknowledgments
Our gratitude to all the carers who gave their precious time to be interviewed for this study. Shi Hui Lee who undertook some interviews.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Cancer and Palliative Care Network, West Australian Health Department.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.