
Abstract
This qualitative study explored the impact of COVID-19 on older rural-dwelling veterans and their caregivers enrolled in home-based primary care (HBPC) through the Birmingham VA Health Care System (BVAHCS). Phone interviews were conducted with 16 veterans and/or their caregivers and rapid qualitative analysis of interview notes was performed. Average age of veterans was 77 (range = 69–97) and 93.7% were white males. Despite a significant number of co-morbidities, 68.8% reported minimal adverse impacts of COVID-19 on overall physical and mental health. Like many healthcare teams, the inter-disciplinary VA HBPC team incorporated Telehealth during COVID-19. Telehealth utilization varied among the 16 participants, with 50% using telehealth independently, 37.5% needing assistance, and 12% lacking access. Our findings are consistent with prior research that identifies resilient characteristics as potentially protective in this high-risk older veteran population during the COVID-19 pandemic.
• Despite high-risk for adverse impacts of COVID-19, several protective factors (e.g., distancing, masking, vaccinations, and military culture of altruism and optimism) were identified in interviews with rural veterans and their caregivers that may have mitigated risk and/or harmful impacts on physical and mental health. • Frail older veterans were able to successfully access and use formal and informal caregiving and social support resources, home care services, and initiate or continue home-based health care services to sustain aging-in-place despite pandemic-related disruptions and threats to health and well-being. • Our findings confirm challenges implementing telehealth to care for older homebound adults living in rural areas due to limited technology access and internet connectivity.
• Continued support toward HBPC services is crucial for the care of this vulnerable yet resilient veteran population. • The adaptation of telehealth into an HBPC model of care may benefit from tailoring to the unique individual qualities and preferences of the individual based on their ability to successfully navigate telehealth.What this paper adds
Applications of study findings
Introduction
The COVID-19 pandemic significantly impacted healthcare, shifting priorities of organizations, and changing healthcare delivery. Home-bound older adults were particularly vulnerable to the effects of the pandemic, especially around maintaining access to healthcare providers, obtaining medications and supplies, and accessing food and hired caregiver support (Federman et al., 2021). Home-based primary care (HBPC) services were critical to sustaining medically complex older adults in the community, making rapid adaptations at the onset of the pandemic to ensure continuity of care, including the use of telehealth (Franzosa et al., 2021). However, numerous challenges to integrate telehealth in this population have been identified (Ritchie et al., 2021).
The Department of Veterans Affairs (VA) is particularly concerned about the impact of COVID-19 on rural-dwelling veterans’ access to medical care and support services. With older veterans at highest risk for morbidity and mortality from COVID-19, efforts to reduce exposure are crucial, while avoiding disruption in medical services. Video telehealth through VA’s Video Connect (VVC), allows providers and patients to have virtual face-to-face visits while optimizing encounter time, limiting travel, and COVID-19 exposure. Since the beginning of the COVID-19 pandemic in 2020, VA has observed a 1,786% increase in the use of telehealth (VA, 2021). Despite this uptick in utilization, barriers to using VA telehealth include challenges with technology access and use (e.g., limited platform training, technical support, and reliable internet and devices). These challenges may be worse in rural settings and result in disparities in virtual care utilization (Ferguson et al., 2021). Furthermore, challenges to integrate telehealth may be exacerbated by the comorbidity burden of this frail, home-bound population (Lam et al., 2020).
The purpose of this study was to explore the experience and impact of the COVID-19 pandemic on older home-bound rural-dwelling veterans’ health, identify challenges to healthcare access, and explore the use of telehealth to inform future quality improvement and healthcare delivery approaches. Telehealth was defined as the utilization of any technology-based platform, including video (VVC or other video application) and telephone visits.
Methods
Participants were provided informed verbal assent including explanation of the study purpose, duration, voluntary nature of participation, and confidentiality of data collected including basic demographics abstracted from the electronic health record (i.e., age, race, gender, and education). Questions were solicited and answered prior to initiating the telephone interview. The study was designated non-research by the Birmingham VA Healthcare System (BVAHCS) Institutional Review Board. The authors used the consolidated criteria for reporting qualitative research (COREQ) checklist for reporting.
Participants
We recruited veterans and caregivers purposively sampled from a list of older (age 65 or older) rural-dwelling HBPC enrollees receiving services from one of the BVAHCS associated Community Based Outpatient Clinics (CBOCs) in Alabama. Veterans and/or representative caregivers were contacted to assess interest in participating in a telephone interview regarding their health and healthcare experiences during the COVID-19 pandemic. Veterans were encouraged to invite their family caregiver to join the interview or serve as proxy if the veteran was unable to participate. Participants were recruited and interviewed until thematic saturation was confirmed by the team.
Interview Guide
We developed a semi-structured standardized interview guide to capture veteran and/or caregiver experiences specific to the impact of COVID-19 in three a priori domains of interest: health (physical, mental, and social); experience, information, and prevention; access to healthcare and use of telehealth. Telehealth was defined as phone or video visits.
Constructs by Domain: Evaluating the Impact of COVID-19 on Rural-Dwelling Older Veterans Health, Experience, Healthcare Access, and Use of Telehealth.
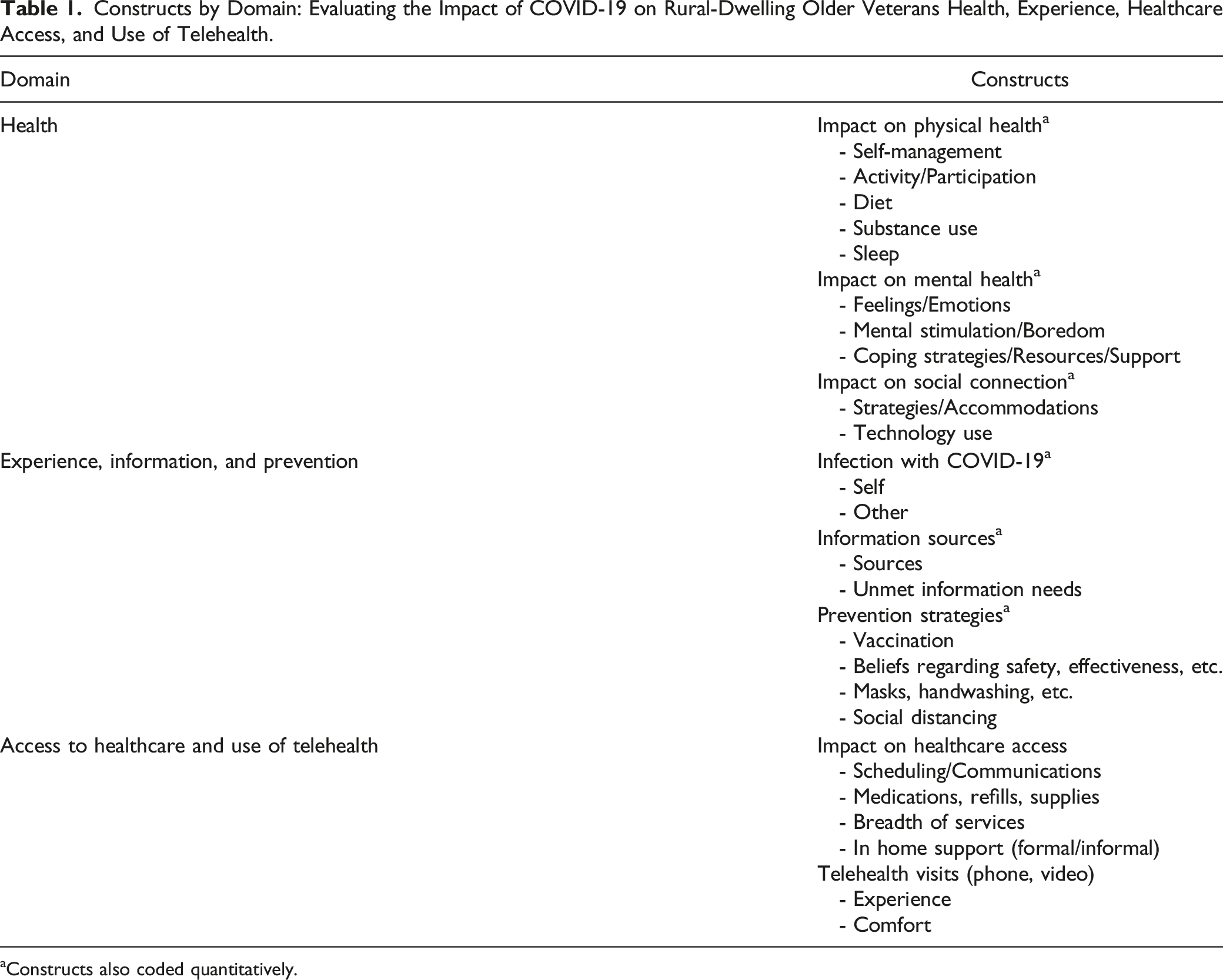
aConstructs also coded quantitatively.
Interview and Notes Process
The interview team consisted of a female advanced fellow in geriatrics interviewer (PY), who contacted the scheduled participant(s), completed telephone assent, and conducted the 30–60-min semi-structured interviews. A female doctorate-level researcher served as a note-taker (KE) to record responses. The interview team was not affiliated with HBPC and had no role in the health care of the participants. At the start of the interview, the interviewer and note-taker introduced themselves by first name and identified their VA affiliation. Interview questions were addressed to both veterans and caregivers, when applicable, with the goal of understanding both perspectives of the veteran experience. Participants were asked to expand or clarify responses, as needed.
The note-taker utilized a structured interview note template to optimize real-time recording of interview responses. Immediately following each interview, the interview team completed a debriefing process to review and verify the noted responses for accuracy and comprehensiveness by comparing with computer-assisted transcriptions. The interview team finalized the notes, highlighted key quotes, and discussed recurrent themes within and between participant responses in preparation for rapid qualitative analysis (Lewinski et al., 2021).
Analysis
We utilized rapid qualitative analysis to expand understanding of the impacts of COVID-19 on health, healthcare access, and use of telehealth. This focused but rigorous approach is applied to obtain targeted qualitative data and inform intervention development and implementation on a shorter timeline than traditional approaches (Gale et al., 2013; Lewinski et al., 2021; Watkins, 2017).
We completed rigorous and accelerated data reduction (Watkins, 2017) by assembling all note data into an all-inclusive table organizing individuals (rows) by our semantic constructs defining each a priori domain (columns), akin to thematic framework. Data were reviewed in depth to verify comprehensive indexing for data in each cell across all applicable constructs. Next, analysis team members independently identified, and rank ordered a subset of key data for each of the thematic constructs. These were jointly discussed in repeated meetings, with differences in selections and rankings examined and adjustments made for consensus, confirming thematic saturation was reached. A summary statement was drafted to characterize the key finding(s), with illustrative quotes for each construct by domain. Remaining analysis sessions engaged the full team and focused on streamlining the key findings to those addressing the overarching study purpose. Quantitative coding was completed for key interview items and descriptive statistics were generated for these and the demographic variables.
Results
Participant Demographics.
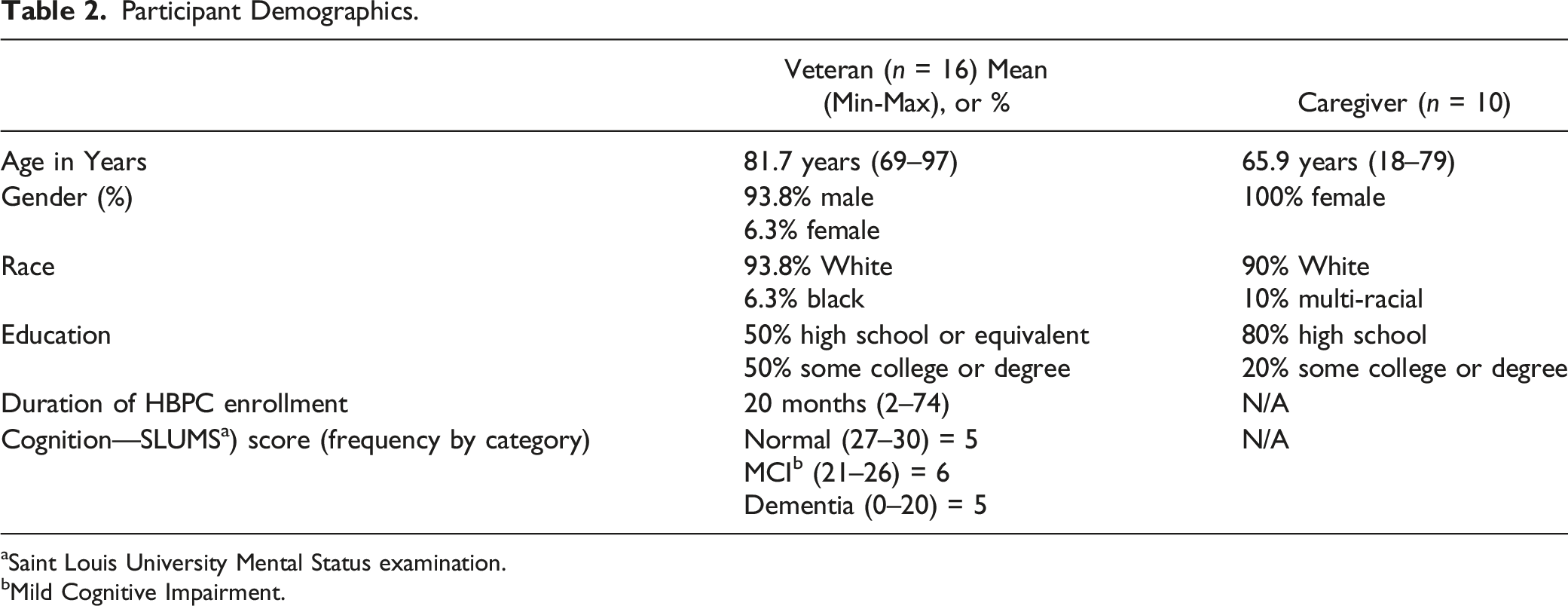
aSaint Louis University Mental Status examination.
bMild Cognitive Impairment.
Impact on Health
The Impact of COVID-19 on Health.
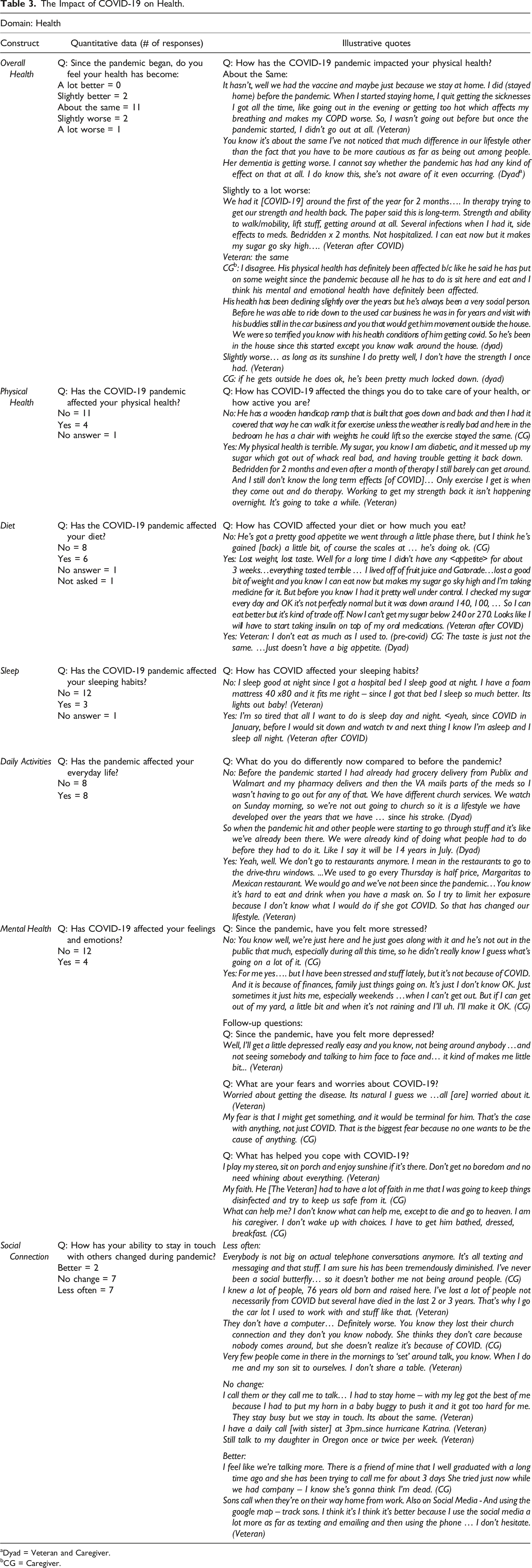
aDyad = Veteran and Caregiver.
bCG = Caregiver.
Mental Health
Overall, many participants approached the pandemic with an attitude of trying not to worry about COVID-19. Some expressed worry about contracting COVID-19 and additional stress due to financial matters and rising costs. Veterans with pre-existing mental health conditions, such as post-traumatic stress disorder (PTSD), isolated themselves prior to the pandemic to avoid triggers. Those who experienced a decline in mental health expressed feelings of loneliness due to isolation.
To cope with the pandemic, many veterans and caregivers turned to their faith, while others turned to hobbies and mindful activities. Illustrative quotes are in Table 3.
Social Connection
Participants were not highly reliant on technology, and some reported a limited capability to use technology to stay connected with others. Responses to changes in the frequency of social connections during COVID-19 were divided between no change (n = 7) and less often (n = 7). The most common strategies to stay connected with others were phone (n = 11) or video chat (n = 3). Respondents who indicated little or no change in social connection during COVID-19 described implementing COVID-related social distancing but preferred in-person interaction. Interestingly, participants who expressed a decrease in social connection reported using video chat to stay connected. See Table 3 for illustrative quotes.
Experience, Information, and Prevention of COVID-19
Experience
Experience, Information, and Prevention of COVID-19.
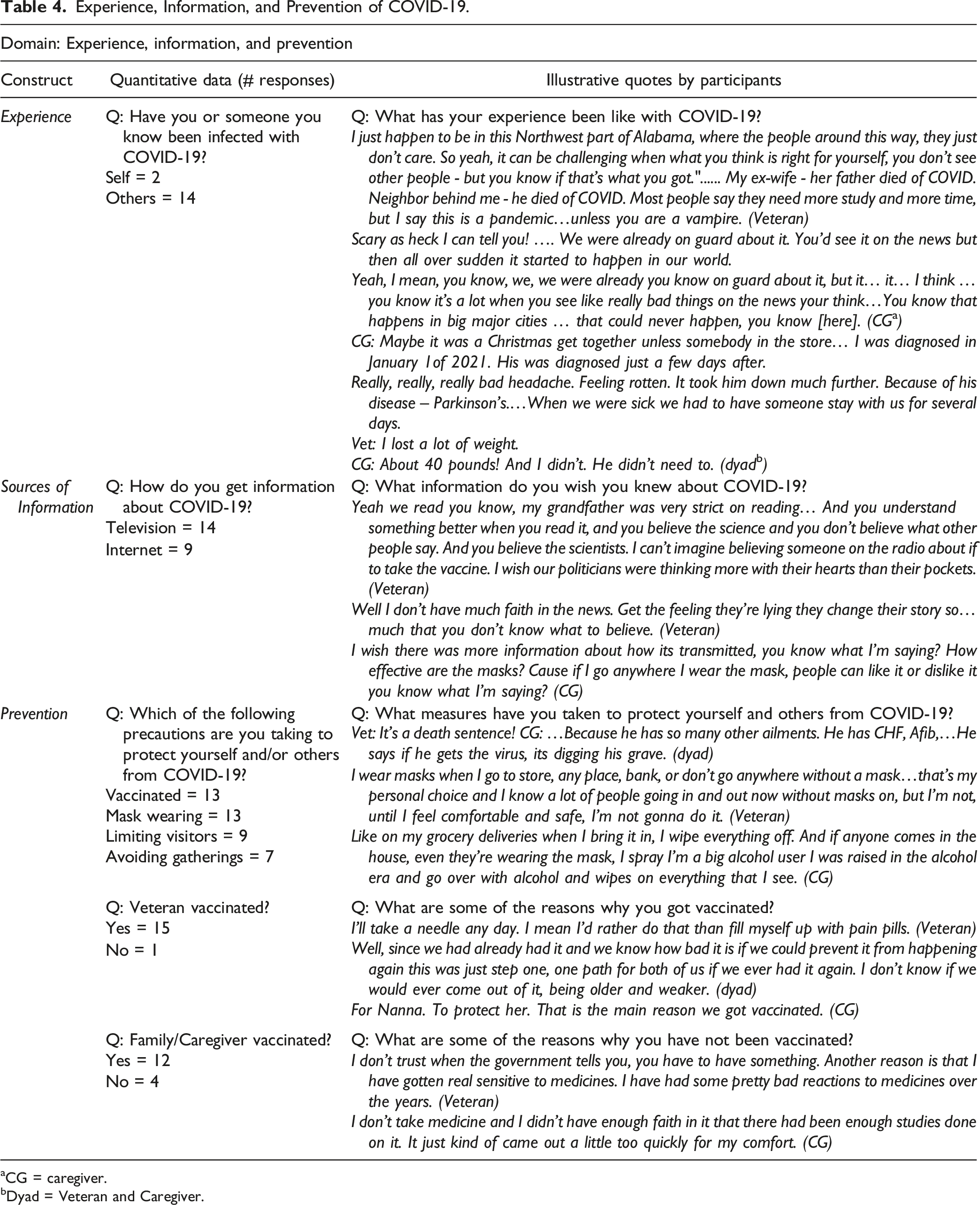
aCG = caregiver.
bDyad = Veteran and Caregiver.
Sources of Information
The primary sources of obtaining information about the pandemic included television and internet. Although participants acknowledged information being available about COVID-19, there were also comments suggesting misinformation, mistrust, and uncertainty. Many expressed doubts about the effectiveness of masks and the integrity or validity of the information provided about COVID-19 (Table 4).
Prevention
Getting vaccinated and wearing a mask were the most common precautions taken to prevent COVID-19. Other approaches included limiting visitors, avoiding large gatherings, hand washing, and sanitizing/disinfecting surfaces (Table 4). Most veterans interviewed (94%) were vaccinated against COVID-19. Reasons for vaccination included avoiding the virus and potential mortality associated with contracting COVID-19. Family members and caregivers were vaccinated (75%) to protect the veteran and avoid spreading the virus. Unvaccinated veterans and caregivers cited reasons of mistrust, medication avoidance or adverse effects, and concerns about side-effects of vaccination (Table 4).
Access to Healthcare
Domains of Access to Healthcare and Use of Telehealth.
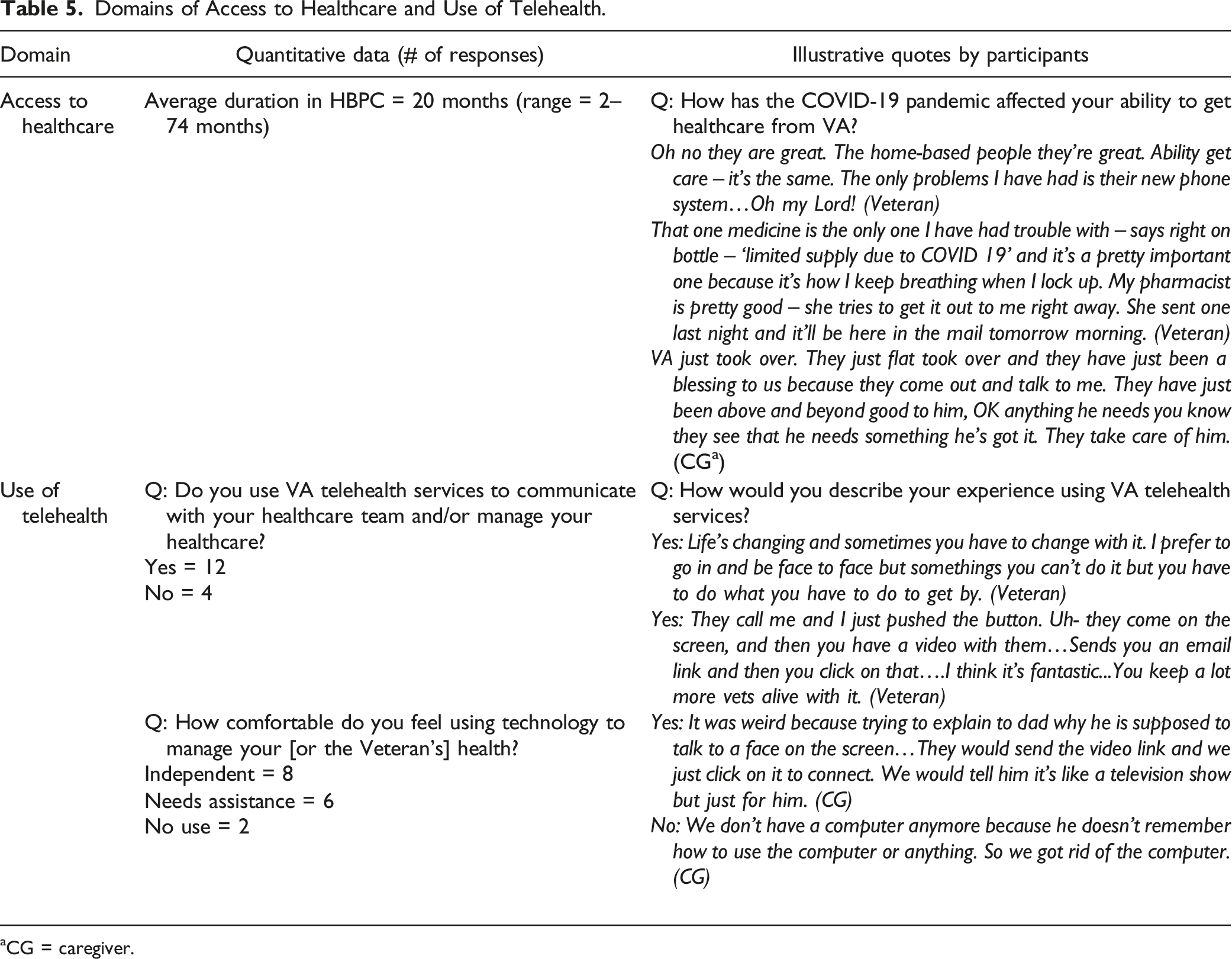
aCG = caregiver.
Telehealth
Half of veterans and caregivers (n = 8) reported a shift during the COVID-19 pandemic from in-person to virtual visits by phone or VVC. They expressed an acceptance by necessity toward using telehealth (i.e., video or phone) and were able to adapt given internet access and capability to navigate the technology. When asked about their comfort levels using telehealth, half of participants expressed independently navigating telehealth visits, some required assistance, and two veterans lacked access to internet and computers. Four participants stated a preference for phone or face-to-face visits citing difficulties connecting during visits or a complete lack of access to the internet and computers. Reasons for lack of access included living in a remote area without reliable internet or cellular reception, no computer or device due to concern for cost, and the inability to use a computer due to sensory deficits, cognitive impairment, or medical illness (Table 5).
Emergent Theme: Resilience
While exploring the above themes among older, rural-dwelling individuals, participants shared about experiences with and perceptions about resilience during COVID-19. Our interviews identified several contributing factors for resilience, including adopting appropriate precautions to reduce risk of contracting COVID-19 and inherent coping strategies through faith or emotional self-regulation. Interestingly, the construct identified both intrinsic and extrinsic factors that likely mitigated the impacts of COVID. Intrinsic factors included activation to take self-protective precautions, social supports (family, religion), military culture (altruism, optimism), managing stress and mental health conditions, and general views on the COVID-19 vaccine. Extrinsic factors included the role of the HBPC and other medical care services, the use of technology and telehealth services, and the behaviors and/or precautions of caregivers to mitigate exposure.
Discussion
Interviews with older rural-dwelling home-bound veterans and their caregivers found that veterans did not perceive a major impact on their overall health due to COVID-19. Interestingly, these veterans demonstrated a high level of resilience, having already adapted to aspects of pandemic life (e.g., social isolation) due to managing multiple medical conditions and frailty. Participants voiced taking additional protective measures during the pandemic such as vaccination, wearing masks, and making changes to daily activities. However, veterans and their caregivers remained uncertain about the information communicated during the COVID-19 pandemic.
Rural home-bound veterans did not perceive any major disruptions in their access to healthcare, and in some cases felt their care had improved due to the efforts of the HBPC team. During the pandemic, HBPC continued to provide multi-disciplinary care for rural-dwelling veterans through telehealth and in-person visits, addressing key barriers of transportation and communication with the healthcare team. Telehealth utilization was higher than anticipated with most veterans able to access telehealth services either independently or with assistance. Those veterans without access to telehealth mostly cited reasons such as a lack of internet or cell-phone reception due to living in rural Alabama.
Veteran participants acknowledged a degree of social isolation, even prior to COVID-19. Many preferred to live in isolation or a rural setting, and therefore did not experience a significant change during COVID-19. Reasons for social isolation included geographic location and lifestyle choices due to underlying PTSD or other medical co-morbidities. Our findings are consistent with Na et al.’s (2022) qualitative study that identified stable levels of loneliness in older veterans during the pandemic compared to pre-pandemic levels and with Grohe et al. (2022) who found home-bound older adults with depression experienced age and health-related impairment-driven isolation both before and during the pandemic (Grohe et al., 2022; Na et al., 2022). However, a similar study on adaptions to care delivery during COVID-19 for veterans living in Medical Foster Homes reported increased social isolation and described successful strategies to mitigate the isolation of veterans and caregivers (Haverhals et al., 2022).
In the face of the COVID-19 pandemic, veterans demonstrated a significant level of resilience, defined in the literature as a “pattern of adaptation in the face of biological, socioeconomic, and psychological risks” (Fontes & Neri, 2015). Although we anticipated impacts to both mental and physical health, we were surprised to learn that no major impacts on health and healthcare were identified because of the COVID-19 pandemic. Participants described successful adaptations such as acceptance and adoption of COVID-19 precautions to mitigate the risk of COVID-19 for themselves and their support systems to ensure successful physical and mental health (e.g., masks, vaccinations, avoiding public spaces, and even online grocery shopping). Some had already implemented these measures prior to the pandemic to manage chronic medical conditions or PTSD. Our findings about resilience are consistent with Pietrzak et al. who conducted a national study in veterans focused on understanding the prevalence and correlates of successful aging using a multidimensional composite measure (Pietrzak et al., 2021). The authors found that physical and mental health difficulties explain 71% of the variance in this composite measure, and protective psychosocial factors (resilience purpose in life, positive expectations regarding emotional aging, and conscientiousness) explained 29% of the variance in successful aging. Our findings suggest that future work might explore tailoring or adapting telehealth to the unique individual qualities and preferences of the individual based on their ability to successfully navigate telehealth. Approximately one-third of our participants reported requiring assistance from others to conduct telehealth visits. To address this problem, it may be useful to develop resources, tools, or even offer ongoing technical assistance for veterans and their caregivers to ensure access to healthcare services.
Our findings add a rural component to similar studies performed in home-bound urban dwelling older adults that identified difficulties in accessing caregiver support, food, and the utilization of telehealth. For example, Ritchie et al. found that care teams were forced to shift their methods of care delivery to offer a combination of in-person visits and telehealth to HBPC patients (Ritchie et al., 2021). Despite previously reported barriers to technology and widening gaps in telehealth use between urban and rural veterans (Ferguson et al., 2021), this study observed a general increase in the use of the telehealth among both rural and urban veterans during the COVID-19 pandemic (Hogan et al., 2022) and among a group older rural-dwelling veterans and caregivers. In fact, veterans in our study did not perceive any disruptions in care and praised their HBPC team for close follow-up and care received throughout the pandemic. However, consistent with prior studies (Muirhead et al., 2022; Padala et al., 2020), barriers to using telehealth beyond phone visits remain, including access to broadband internet, financial concerns, and the ability to navigate these more advanced telehealth modalities independently. Rural-dwelling veterans in this study were largely able to adapt to the use of video telehealth either independently or with the assistance of others, indicating the viability of this HBPC delivery modality and the need for continued efforts to address barriers to access and use in this vulnerable population.
Studies to inform approaches that optimize access to home-based services via telehealth technology are essential, particularly with diverse older patients at-risk for health inequities (Muirhead et al., 2022). Future studies to investigate the potentially protective effect of HBPC services, veteran status, pre-pandemic isolation, and elevated levels of pandemic-related caregiver stress may provide key insights into the observed resilience to adverse impacts of the pandemic on the health and well-being of most of our participants. Our findings suggest that efforts to improve telehealth for older home-bound veterans may want to concurrently identify best ways to support those with telehealth capability (i.e., internet) to use it independently or with their caregiver while also exploring how to expand capability in general.
Limitations
This project was conducted at a single VA Medical Center and the associated outpatient clinics. Our purposive sample was not intended to yield generalizable knowledge about all older veterans living in rural settings. Participants were predominantly white males, unlike prior studies in diverse urban home-bound older adults (Federman et al., 2021). While participants were assured confidentiality of responses, demand characteristics and other response biases cannot be ruled out. Quantitative data on the actual rates of healthcare utilization before and during the COVID pandemic, including frequency and modality of telehealth visits, could further elucidate the qualitative data described herein. Future studies may benefit from additionally gathering data on the extent to which medical conditions impact the ability to use different modalities. Despite limitations, this study provides valuable insights into the impacts of the pandemic on vulnerable rural-dwelling home-bound older adults.
Conclusion
We provide an initial understanding of the impacts of COVID-19 veterans’ health, healthcare access, and the use of telehealth among older veterans living in a rural setting and receiving HBPC. The role of resilience was a common theme across participants as veterans had adopted changes to mitigate the risk of COVID-19 including the use of telehealth for their HBPC services. Importantly, our findings demonstrate that telehealth is a reasonable option for some older rural veterans with the caveat that barriers (unreliable internet, challenges using technology) persist for others.
Footnotes
Acknowledgments
This work was additionally supported by the U.S. Department of Veterans Affairs Office of Academic Affiliations Advanced Fellowship in Geriatrics at the Birmingham/Atlanta Geriatric Research Education and Clinical Center (Dr. Yee), and the Birmingham/Atlanta Geriatric Research Education and Clinical Center (Drs. Echt, Markland, and Zubkoff), Veterans Affairs Healthcare System, Birmingham, AL.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
IRB
The study was designated non-research by the Birmingham VA Healthcare System (BVAHCS) Institutional Review Board.
Disclaimer
The contents of this paper represent the opinions of the authors and do not represent the views of Department of Veterans Affairs (VA) or the United States Government.