
Abstract
Nursing homes were profoundly affected by the COVID-19 pandemic, influencing work outcomes of care aides who provide the most direct care. We compared care aides’ quality of work life by conducting a repeated cross-sectional analysis of data collected in February 2020 and December 2021 from a stratified random sample of urban nursing homes in two Canadian provinces. We used two-level random-intercept repeated-measures regression models, adjusting for demographics and nursing home characteristics. 2348 and 1116 care aides completed the survey in February 2020 and December 2021, respectively. The 2021 sample had higher odds of reporting worked short-staffed daily to weekly in the previous month than the 2020 sample. The 2021 sample also had a small but significant drop in professional efficacy and mental health. Despite the worsening changes, our findings suggest that this workforce may have withstood the pandemic better than might be expected.
Care aides reported lower levels of professional efficacy and mental health in December 2021 (21 months into the pandemic) than in February 2020 (immediately prior to the pandemic).
Ongoing monitoring is essential to ensure small trends observed in our study do not worsen, a situation that could escalate quickly to a workforce crisis of significant proportions.What this paper adds
Applications of study findings
Introduction
Residential long-term care (LTC) including nursing homes has been and continues to be deeply affected by the COVID-19 pandemic. Many studies reveal the nature and extent of traumatic stress experienced by residents, staff, and residents’ families (Cohen-Mansfield & Meschiany, 2022; Reynolds et al., 2022). Care aides (also called personal support workers or nursing assistants) comprise the majority of the workforce in Canadian nursing homes and provide at least 80% or more of direct care (Chamberlain et al., 2019). This workforce is unregulated and often faces high workloads, insufficient baseline staffing resources, and increasingly complex care needs of residents (Reynolds et al., 2022). Canadian care aides are often immigrants who do not speak English as their first language, are often middle-aged women, and frequently work multiple jobs to make ends meet (Chamberlain et al., 2019; Duan et al., 2020; Song et al., 2020a).
Researchers have reported how the COVID-19 pandemic has affected LTC staff quality of work life, such as high caregiver burden (Reynolds et al., 2022), significant anxiety (Riello et al., 2020), and traumatic stress (Blanco-Donoso et al., 2021). Poor LTC preparedness placed direct care staff at unnecessary risk, with many nursing homes lacking an adequate supply of personal protective equipment in the early months of the pandemic (Blanco-Donoso et al., 2021). Care aides experienced frequent symptoms of moral distress as they weighed their own safety against their obligation to perform their vital role in resident care (Arble et al., 2021; Iaboni et al., 2022). Chronic staff shortages in this care sector were heightened by staff sickness which further exacerbated the work stress for remaining workers (Havaei et al., 2022). Burnout is highly prevalent among care aides (Leskovic et al., 2020; Navarro Prados et al., 2022) and is linked to poor staff retention (White et al., 2021) reflected by high turnover early in the pandemic and sustained depleted staff resources as the pandemic continued (Frogner & Dill, 2022).
This knowledge about the healthcare workforce often combines findings for care aides with other staff groups (Arble et al., 2021; Havaei et al., 2022; Reynolds et al., 2022) or focuses solely on licensed clinicians such as registered nurses (Havaei et al., 2022; Leskovic et al., 2020). Our understanding of how COVID-19 has influenced frontline healthcare workers in any setting is lacking given the absence of routinely collected data to assess carer health and work outcomes. Findings specific to LTC care aides is required given this group’s unique care context and responsibilities. The existing knowledge in this area is also largely generated from convenience samples, sometimes from one home (Havaei et al., 2022), and have long intervals between data collection episodes (Leskovic et al., 2020). Here, our aim was to compare care aides’ demographics and quality of work life from immediately preceding the COVID-19 pandemic in February 2020 to December 2021 during the pandemic.
Methods
Study Design
We completed repeated cross-sectional analyses of data from two waves of surveys completed in February 2020 (immediately pre-pandemic; Time 1) and again in December 2021 (21 months into the pandemic; Time 2).
Setting
We sampled care aides in nursing homes in urban areas of Alberta and Manitoba, Canada. Participating nursing homes were registered by the provincial government and randomly selected based on strata defined by (1) health region (Edmonton and Calgary Zones in Alberta and the Winnipeg Regional Health Authority in Manitoba), (2) facility size (small, <80 beds; medium, 80–120 beds; large, > 120 beds), and (3) owner-operator model (public nonprofit, private for-profit, and voluntary nonprofit). The names of all nursing homes in Alberta and Manitoba were publicly available on government websites. For each health region, we generated the list of eligible nursing homes based on the owner-operator model and size of nursing homes. A random number generator was used to create final lists of selected nursing homes. The provincial lead investigators used these lists and followed a standardized procedure for recruitment, and if needed, replacement of nursing homes.
Participants
Care aides were invited to participate if they had worked in a study facility for longer than 3 months, could identify a unit where they worked for at least 50% of their time, and worked on that unit for 6 or more shifts in the past month. Care aides completed structured computer-assisted personal interviews administered by trained interviewers during work hours (Estabrooks et al., 2009). During computer-assisted personal interviews, interviewers read survey questions aloud to care aides and entered their responses directly into a computer survey application predesigned specifically for our research study (Estabrooks et al., 2009). Interviews were in person at Time 1 and were completed virtually using the Zoom platform at Time 2 because of COVID restrictions in the nursing homes.
Ethics
This study was approved by the Research Ethics Board at the Universities of Alberta (Pro00037937) and Manitoba (H2014:164). Participating organizations provided operational approvals. Written informed consent was obtained from care aides prior to data collection.
Measures
Summary of Measures.
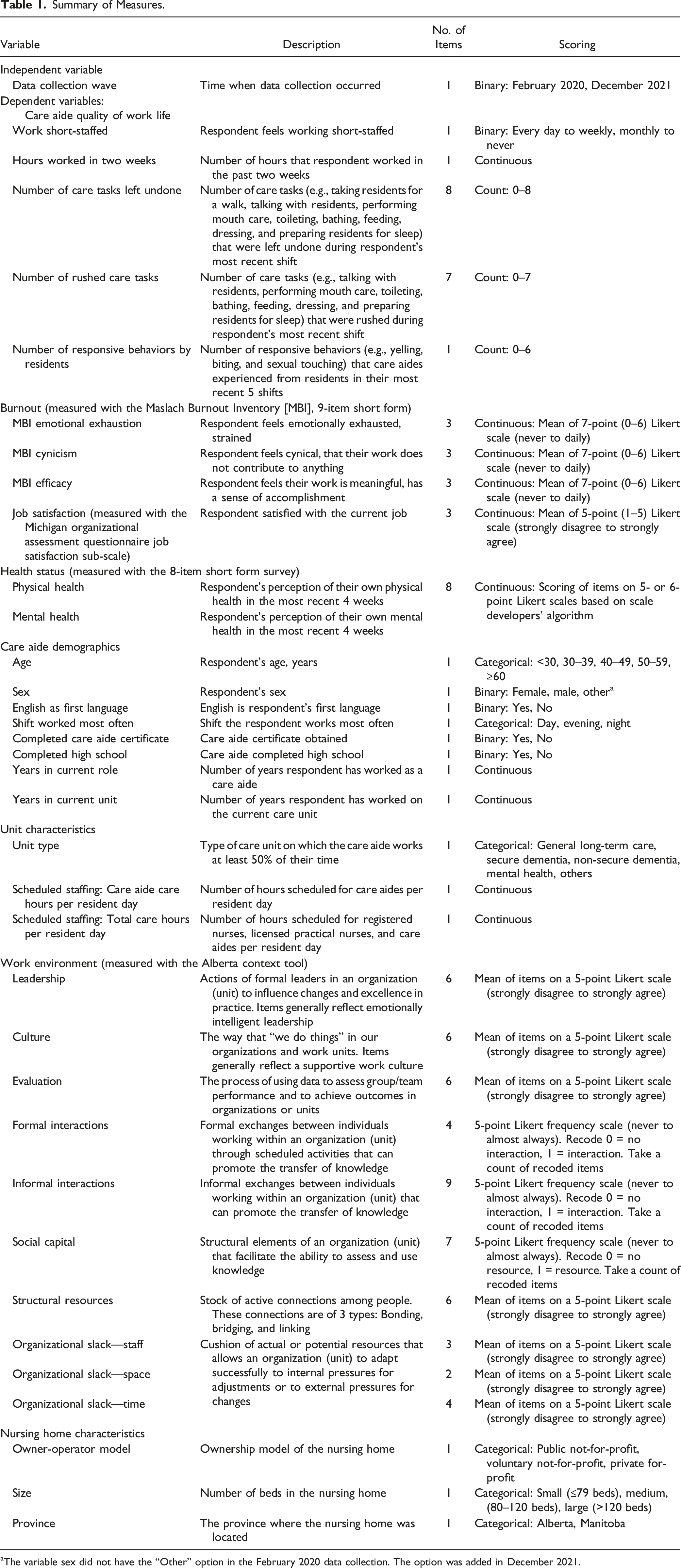
aThe variable sex did not have the “Other” option in the February 2020 data collection. The option was added in December 2021.
Statistical Analyses
We calculated frequency and percentage for categorical variables and mean and standard deviation for continuous variables. To compare care aide demographics and characteristics of resident care units and nursing homes at the two time points, we used repeated-measures regression models to account for certain care aides participating in both waves of data collection. Less than .1% of data were missing for all variables and we used listwise deletion for missing data.
To compare care aides’ quality of work life at the two time points, we used two-level random-intercept repeated-measures regression models to account for repeated measures and care aides nested within same care units (Norton et al., 2014). Outcomes were also adjusted for first language and shift of care aides, and owner-operator model, size, and province of nursing homes (sampling strata). All analyses were performed in SAS, version 9.4.
Results
Comparison of Sample Characteristics at Time 1 and Time 2
Demographics of Care Aides and Characteristics of Care Units and Nursing Homes.
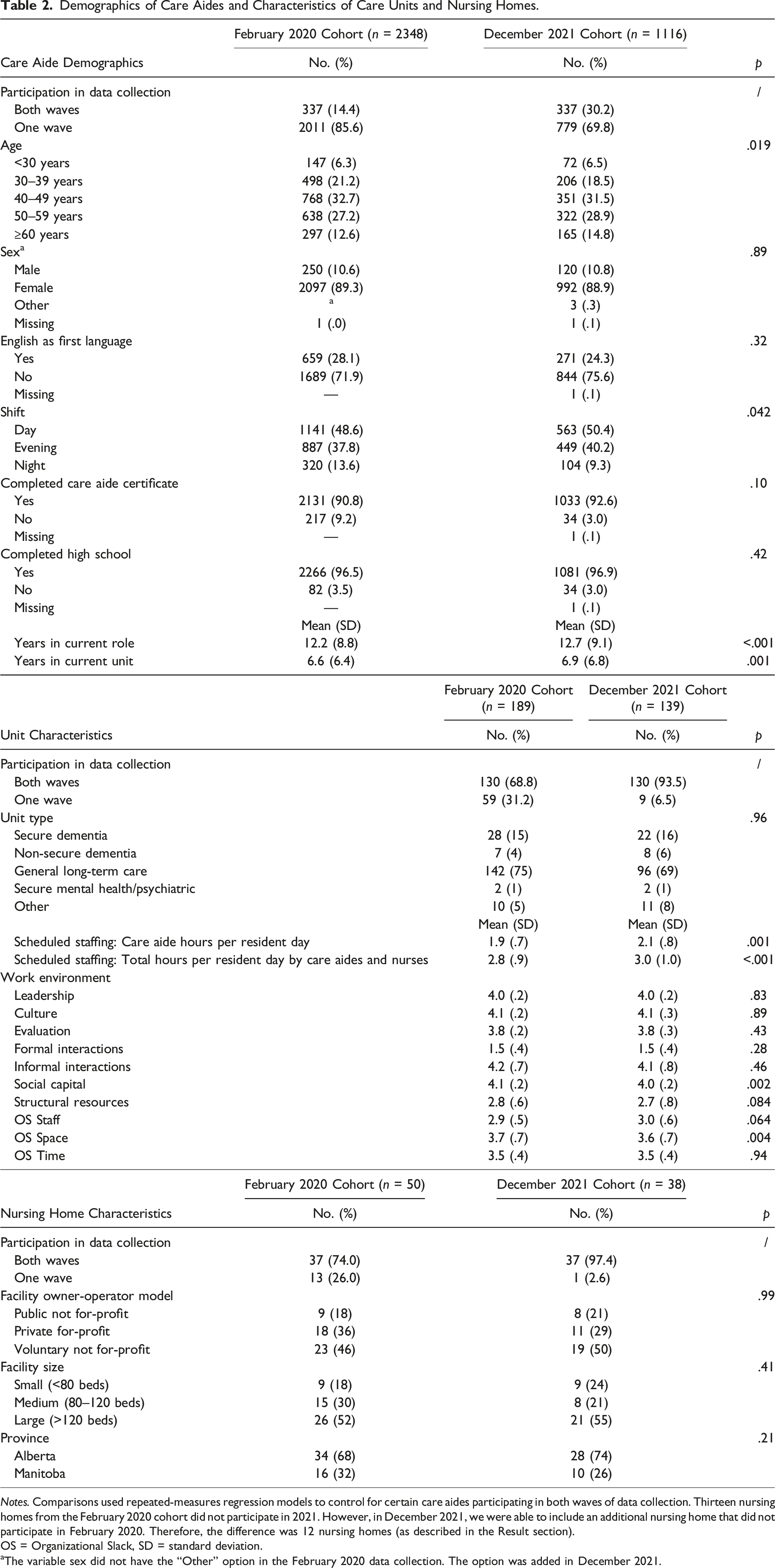
Notes. Comparisons used repeated-measures regression models to control for certain care aides participating in both waves of data collection. Thirteen nursing homes from the February 2020 cohort did not participate in 2021. However, in December 2021, we were able to include an additional nursing home that did not participate in February 2020. Therefore, the difference was 12 nursing homes (as described in the Result section).
OS = Organizational Slack, SD = standard deviation.
aThe variable sex did not have the “Other” option in the February 2020 data collection. The option was added in December 2021.
Comparison of Quality of Work Life at Time 1 and Time 2
Comparison of Quality of Work Life for Care Aides in February 2020 Versus December 2021.
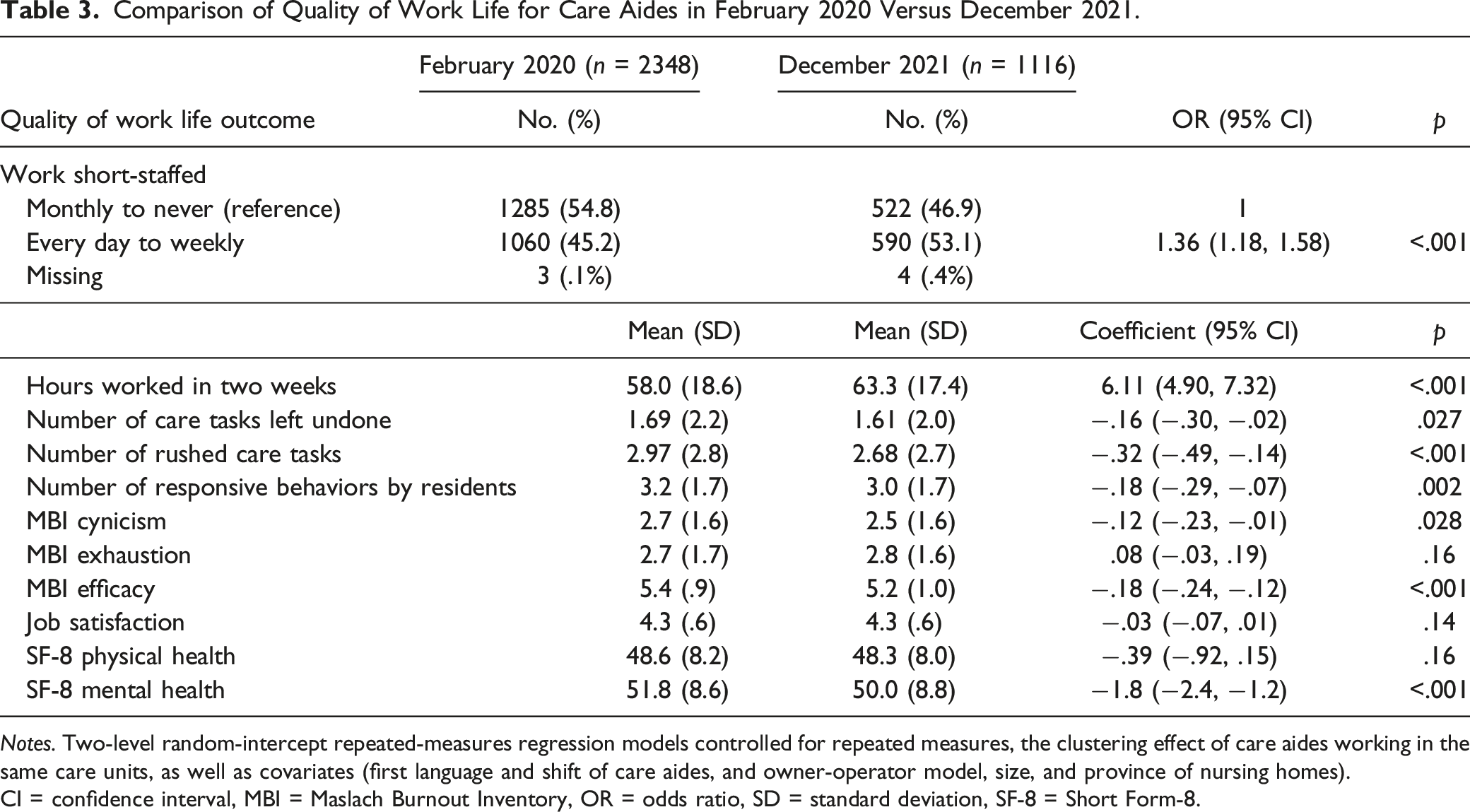
Notes. Two-level random-intercept repeated-measures regression models controlled for repeated measures, the clustering effect of care aides working in the same care units, as well as covariates (first language and shift of care aides, and owner-operator model, size, and province of nursing homes).
CI = confidence interval, MBI = Maslach Burnout Inventory, OR = odds ratio, SD = standard deviation, SF-8 = Short Form-8.
Discussion
In this study, we compared care aides’ reports of work life outcomes from February 2020 to December 2021. Prior reports documented that LTC staff experienced significant burden, anxiety, and traumatic stress during the pandemic (Blanco-Donoso et al., 2021; Reynolds et al., 2022; Riello et al., 2020). While these studies suggest a near crisis among care aides during the pandemic, our findings suggest that care aides may have weathered the first 18 months of the pandemic relatively well—keeping in mind that pre-pandemic scores on a number of measures (i.e., burnout) were high.
A small, but significant drop in professional efficacy (a burnout sub-scale) is worth noting as care aides have historically reported extremely high levels. In previous studies, we suggest that very high efficacy acted as a potential protecting attribute to burnout despite reporting high levels of emotional exhaustion and cynicism (the other sub-scales of burden) (Chamberlain et al., 2019; Song et al., 2020a). The importance of this drop in professional efficacy will not be clear until we have later pandemic assessments. Possibilities for this change may be that the pandemic worsened already concerning levels of working short-staffed, contributed to increased hours worked, and exerted negative effects in mental health and on social capital (which captures important aspects of teamwork). These coupled with personal fears relating to infection of self and family might have exerted important but temporary effects on professional efficacy that will lessen over time. It could also mean that care aides have been under sufficient stressors contributing to longer term effects on their ability to cope and sense that their work has meaning. The latter would be more ominous suggesting that this workforce could be close to or at its limits of coping. Ongoing monitoring is essential to ensure small trends observed in our study do not worsen, a situation that could escalate quickly to a workforce crisis.
Lower numbers of rushed care tasks and responsive behaviors, while seemingly counterintuitive, may reflect pandemic anomalies. For instance, factors, such as visitation restrictions due to the pandemic and fewer resident transfers to acute care settings (Cohen-Mansfield & Meschiany, 2022; Reynolds et al., 2022) might have reduced interruptions to staff’s workflow and protected them from leaving care undone. Historically, we have observed quite high levels of missed care (Song et al., 2020b, 2023).
Social capital, a measure of active connections and teamwork among care staff, was significantly lower in December 2021 compared to February 2020. Having less time to engage with other care aides as supported by self-reports of working short-staffed as well as the requirements to wear masks (Reynolds et al., 2022)) made communication more difficult and may have limited their opportunities to connect with co-workers. Not surprisingly, organizational slack, including perceptions of available space also decreased. Public health directives regarding distancing restrictions affected the space available to care aides to carry out their responsibilities likely contributed to this outcome (Reynolds et al., 2022).
In a different study, this research team assessed changes in health and well-being of the manager group (e.g., unit care managers, nursing home managers) sampled at the same time from the same Albertan nursing homes (Estabrooks et al., 2023; Savage et al., 2022). In the manager study, we observed statistically lower levels of job satisfaction and mental health and higher levels of cynicism and emotional exhaustion in December 2021 than pre-pandemic. Based on findings from the manager group, care aides in the current study have withstood the first 18 months of the pandemic better than the manager group. In an interconnected system such as a nursing home, we need to monitor the health and well-being of all occupational groups. Without stable and resilient managers in nursing homes, other staff groups cannot carry on indefinitely without negative impact.
Our study has a number of limitations. Although the nursing home characteristics were similar in both waves, 13 nursing homes included in Time 1 declined to participate in Time 2 (Table 2), largely due to the still overwhelming demands of COVID-19. The nursing homes dropping from Time 2 data collection might have contributed to the observed differences in care aide outcomes, as supported by the relatively large percent of variance in care aide outcomes explained by nursing home factors (Supplemental Table 1). The care aide response rate for participating nursing homes was much lower at Time 2. A selection bias may have been present. Alternative approaches to analyzing the data are possible, for example, using a linked cohort of care aides who participated in data collection at both time points. We are able to identify this sub-group of care aides (n = 337) with the unique identifier assigned to each participant during data collection. Care aide demographic characteristics were, however, similar at both time points. The study is susceptible to bias from self-report measures. In addition, the demographics of care aides in our study might differ in important ways from those working in other Canadian provinces or nursing homes from non-Canadian contexts. For example, over 85% of our care aide sample were born outside Canada, while in the US, approximately 21% of care aides (more commonly called nursing assistants) in nursing homes were immigrants (Paraprofessional Healthcare Institute, Inc., 2021). The demographics of our participants and the methodological limitations of this study suggest that generalization of our findings to settings and people with characteristics different from ours should be made with caution.
Conclusions
Care aides are an essential and major part of the care system in nursing homes. During highly challenging times such as the COVID-19 pandemic, they were heavily relied upon to get through tough times without much change in support. Prior to the pandemic, we had observed significant stability in measures of physical and mental health and quality of work life (job satisfaction, burnout) over a 15-year period (Chamberlain et al., 2019), making even small changes now more worrisome than they might otherwise be. We may be observing small changes that signal a worsening trend—or, further assessment post-pandemic may reveal a return to pre-pandemic levels. Regardless, our study results show that the relative stability of care aide measures from a pre-pandemic baseline to December 2021 point to a workforce that has withstood the pressures of COVID, at least during the first 18 months, better than might have been expected.
Supplemental Material
Supplemental Material - Changes in Health and Well-Being of Care Aides in Nursing Homes From a Pre-Pandemic Baseline in February 2020 to December 2021
Supplemental Material for Changes in Health and Well-Being of Care Aides in Nursing Homes From a Pre-Pandemic Baseline in February 2020 to December 2021 by Yuting Song, Janice M. Keefe, Janet Squires, Brittany deGraves, Yinfei Duan, Greta Cummings, Malcolm B. Doupe, Matthias Hoben, Amber Duynisveld, Peter Norton, Jeffrey Poss, and Carole A Estabrooks in Journal of Applied Gerontology.
Footnotes
Author Contributions
YS, JMK, PN, JS, and CE made substantial contributions to the conception and design of the study. YS and JMK analyzed data, and the whole team contributed to the interpretation of results. JMK, YS, AD, BG, and YD drafted the manuscript, with all co-authors contributing substantively to multiple versions of the manuscript. All authors approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors acknowledge the Translating Research in Elder Care (TREC) 2.0 team for its contributions to this study. Funding was provided by the Canadian Institutes of Health Research (CIHR) and partners in the Ministries of Health in Alberta and Manitoba.
Ethics Approval
This study was approved by the Research Ethics Board at the Universities of Alberta (Pro00037937) and Manitoba (H2014:164).
Sponsors’ Roles
The sponsors were not involved in the design or implementation of the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.