
Abstract
Infrequent participation in formal social activities among older adults increases the risk of loneliness. We examined whether a higher income level moderates the relationship between infrequent participation and loneliness. Utilizing data from wave #6 of the European Health, Aging, and Retirement Survey, we included participants aged 65+ (i.e., older adults), non-participants in the labor force (N = 24 819). Loneliness was measured by the R-UCLA loneliness questionnaire, formal social activity by participation frequency in volunteer/charity activities, educational course/training, sports/social/other clubs, and political/community organizations. Hierarchical multiple regression models examined relationships between variables, controlled by country. Infrequent participation in formal social activity associated with higher risk of loneliness. However, income moderated the association between participation and loneliness; infrequently participating older adults with low-to-moderate income were more vulnerable to loneliness than higher income older adults, for whom infrequent participation did not increase loneliness. This reinforces the need to encourage formal social activity with subsidy for low-to-moderate income older adults.
• Income moderates the association between participation in formal social activity and loneliness. • Infrequent participation in formal social activity combined with low-to-moderate income increases loneliness in older adults. • Infrequent participation in formal social activity, when combined with higher income, does not increase loneliness in older adults.
• A differential approach must be employed in making formal social activities more accessible. • Subsidies for formal social activities specific to low-to-moderate income older adults may increase participation in formal social activities. • Transport to formal social activities specific to low-to-moderate income older adults may increase participation in these activities.What this paper adds
Applications of study findings
Introduction
By 2050, about 27.1% of the OECD population will be over the age of 65 (OECD, 2019). The aging of the population presents us with a major social challenge: reducing the sense of loneliness that accompanies the aging of adults (Heylen, 2010). Loneliness is a subjective experience that results from low satisfaction with the number and/or quality of social connections, and the gap between what a person wants and what he/she actually has (de Jong Gierveld, 1987, 1998; Peplau & Perlman, 1982; Shiovitz-Ezra & Leitsch, 2010). Loneliness exacts a physical price that can be a decrease in immune system function (Murberg, 2004), an increased risk of heart disease and stroke (Valtorta et al., 2016), deficient sleep patterns, and a poor subjective evaluation of general health (Cacioppo et al., 2002). Loneliness is also linked to mental disorders, anxiety, depression and suicidal thinking (Courtin & Knapp, 2017), cognitive impairment, and distress (Hawkley & Cacioppo, 2010).
Findings on sex-specific and age differences on the experience of loneliness remain unclear and sometimes contradictory. Some studies reported that loneliness among older people increases with age only among the very old (Dykstra, 2009), and others reported that age differences are not significant in gauging loneliness (Chawla et al., 2021), among other things, because predictor variables of loneliness are unevenly distributed across the adult life span (Hawkley et al., 2020). Yet other studies reported that older women feel lonely more often than their male age-peers (Luanaigh & Lawlor, 2008; Victor et al., 2005), possibly caused by women being more disadvantaged regarding risk factors for loneliness especially regard to widowhood (Pinquart & Sorensen, 2001a). Another study reported that the mean level of loneliness did not significantly differ between men and women, except at the oldest old age (≥85 years) when women experience greater loneliness possibly because of the higher tendency to be widowed and therefore likely to live alone (Zebhauser et al., 2014).
Losses and life events such as widowhood, divorce and bereavement (Dykstra et al., 2005; Victor et al., 2005), lack of a social network (Mullins & Dugan, 1990), and poor health (Luanaigh & Lawlor, 2008) are some of the factors that exacerbate loneliness among the elderly. Unmarried individuals indicated feeling lonelier than married individuals (Hawkley & Capitanio, 2015), but in one study marriage was found to have no protective effect at all if the spouse was not identified as the respondent’s confidante (Hawkley et al., 2008). Also living alone was not per se associated with loneliness; instead, a smaller social network was an indicator of loneliness (Zebhauser et al., 2014).
Social participation focuses mainly on the person’s involvement in activities that provide interaction with others in society or the community (Levasseur et al., 2010); participation in such activities contributes to relieving loneliness in later life (Gilmour, 2012; Heaven et al., 2013). Social activity provides adults with meaning and promotes successful aging (McKenna et al., 2007; Menec, 2003). It also contributes to developing a sense of control, meaning, and improved self-image (Kuykendall et al., 2018; Lee et al., 2019; Min et al., 2016), and to better physical and mental health (Driver, 1999; Glass et al., 2006; Hong et al., 2009; Law et al., 1998). Participation in social activity also improves the ability to cope with the losses associated with aging (Kleiber et al., 2002) and with the shrinking social network that accompanies the aging process (Litwin, 1999).
Participation in social activity has limitations that intensify with age (Agahi et al., 2006; Bukov et al., 2002; McGuire & Norman, 2005): Poor health (Agahi et al., 2006), limited mobility (Pinquart & Sorensen, 2001b), an unsupportive environment, lack of available options within one’s residential area (Wen et al., 2003, 2006), lack of partners, and low income (Bukov et al., 2002; Lefrancois et al., 1997), all of which decrease the probability that one would participate in social activity.
Lower income increases the probability of experiencing loneliness both directly and indirectly (Bosma et al., 2015; Savikko et al., 2005; Victor et al., 2005). Lower income limits the adult’s choice of social activity (Bukov et al., 2002; Lefrancois et al., 1997; Wilkie et al., 2007) and increases his/her probability of poor health (Adler et al., 1994). These may result in fewer social connections and harm the ones that do remain (Pinquart & Sorensen, 2001b), thereby increasing the risk of experiencing loneliness. Socioeconomically disadvantaged areas tend to offer individuals a lower level of social services (Barnes et al., 2006) than found in higher socioeconomic areas, as well as limited transportation, a high
In the present study, we examined whether income moderates the link between participation in formal social activity and loneliness.
We emphasize that although various studies contend that informal activity contributes most significantly to relieving loneliness (Lemon et al., 1972; McPherson, 1991), this study focuses on formal social activity because this type of activity can be impacted by the community, local government, and the State. Removal of barriers to participation in formal activities such as cost reduction and solving transportation and other accessibility problems has been defined as an effective way to lead to increased participation (Crawford et al., 1991).
Methods
Data
The present study used SHARE (The Survey of Health, Aging, and Retirement in Europe) data. This survey is the initiative of a multidisciplinary panel launched in 2002 in European countries and constitutes a collection of micro-longitudinal data on health, socio-economic status, and social and emotional status among adults aged 50 and over living in the countries sampled (and their spouses of all ages) and excluding prison inmates and hospitalized people.
The current study used “wave 6” data collected during 2015 from 18 countries. A total of 69 231 interviews were collected in this wave, not including interviews with representatives of deceased individuals (Börsch-Supan, 2019). The data were collected through a face-to-face, computer-guided personal interview. The study population included participants aged 65 and over (i.e., older adults) (N = 28 051), non-participants in the labor force who described themselves as retirees, employed in the household/family care, disabled or handicapped, and who do not live in a nursing home (N = 25 913). Participants with missing values were excluded from the sample so that the final sample included 24 819 participants.
Outcome
The SHARE questionnaire measured loneliness using the abbreviated version of the Revised-University of California at Los Angeles Loneliness scale (R-UCLA) (Hughes et al., 2004). This tool has been well-validated (Russell et al., 1980), and many SHARE researchers have used it (Niedzwiedz et al., 2016; Shiovitz-Ezra, 2015). The questionnaire included three queries: “How often do you feel you lack companionship,” “How often do you feel left out?,” and “How often do you feel isolated from others?” The answers were classified on a Likert scale ranging from 1 to 3: “Almost never/sometimes/often.” Respondents’ scores ranged from 3 to 9, with a higher score indicating greater loneliness.
Independent Variables
Participation in formal social activity was measured by processing participants’ answers to questions about taking part during the previous 12 months in volunteer or charitable activities, attending an educational or training course, attending a sport, social, or other type of club, or participating in a political or community organization. Respondents were asked whether they participated in such activity and if so at what frequency (almost every day, almost every week, almost every month, and less often than “almost every month”). Accordingly, a dichotomous variable was defined: participation in at least one formal social activity almost every day or almost every week deemed frequent participation. Participation in any formal social activity “almost every month” or “less often [than almost every month]” or “non-participation” in any activity was interpreted as infrequent participation.
Range of Household Income by Quintiles Stratified by Country.
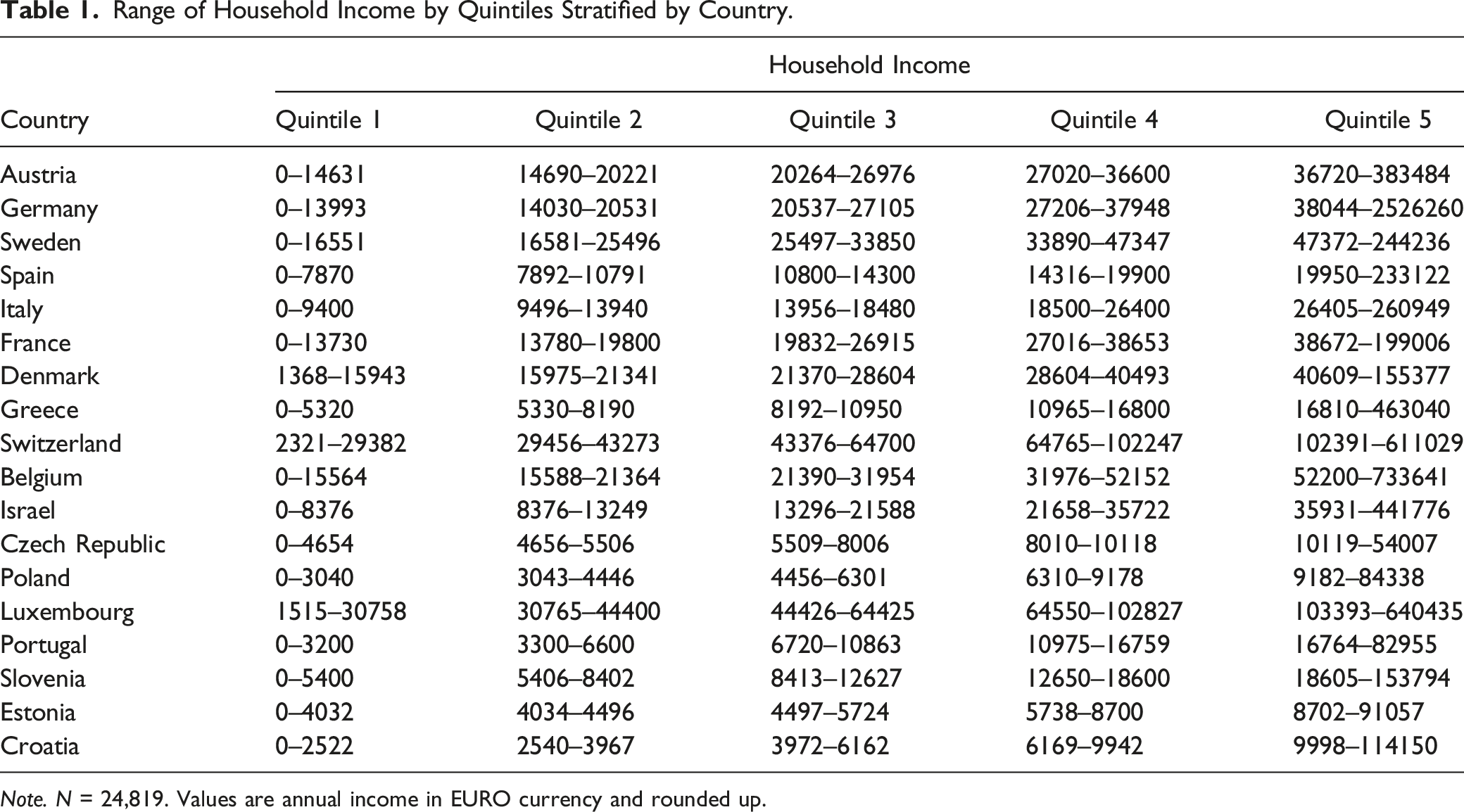
Note. N = 24,819. Values are annual income in EURO currency and rounded up.
In addition, we examined the variables of age (65–74 = 0, 75+ = 1), gender (male = 0, female = 1), whether the adult lives with a partner (yes, no), and the level of education, measured by the International Standard Classification of Education (ISCED). Level of education is standardized across countries through the ISCED and is thus classified into two variable categories: primary (ISCED 0e2) and secondary and tertiary education (ISCED 3e6).
Due to the direct and indirect effect of health on both social participation and income, this study included a number of variables that examine the adult’s health status: The self-rated health variable is measured by asking participants how they rate their own health on a scale of 1–5 (poor, fair, good, very good, and excellent). The Global Activity Limitation Indicator (GALI), which aims to assess health limitations (Van Oyen et al., 2018), was assessed by asking participants how much, in the previous 6 months, they were restricted, due to a health problem, from performing activities that people typically do: (1) unlimited, or somewhat limited; (2) limited but not severely; (3) very limited and translated into a dichotomous variable, limited or unrestricted (Jagger et al., 2010).
Limitations in activities of daily living (ADL) examine a person’s ability to perform six daily activities independently: dressing, walking in a room, bathing, eating, getting into, and out of bed (Katz et al., 1970). Each activity was rated dichotomously (0 = not limited, 1 = limited); the individual’s ADL score was calculated as the sum of all activities and ranged between 0 (no limitations at all) and 6 (limitations in all activities).
Statistical Analyses
First, univariate description of the study variables and their bivariate associations with loneliness were conducted. Associations among continuous, ordinal, and dichotomous variables with loneliness were examined via zero-order correlations, Spearman’s rho, and point-biserial correlations, respectively.
Then, moderation analysis was conducted using a hierarchical multiple regression model. In model 1, participation in formal activity (infrequent = 0 and frequent = 1), household income as well as background and health variables with a loneliness association greater than .10 were entered. Note, that in order to control for the context effect of countries, several dummy variables were entered to the model with Austria as the reference group (e.g., dummy 1: Austria = 0, Germany = 1; dummy 2: Austria = 0, Sweden = 1). In model 2, the interaction terms of participation in formal activity × household income were entered. Loneliness score served as the dependent variable. Probing and visualizing the interaction were carried out using PROCESS macro for SPSS (Model 1) (Hayes, 2018).
Data analysis was conducted using IBM SPSS statistics version 26. An alpha level was set to .05 for all statistical tests.
Results
Descriptive Statistics and Correlations
Descriptive Statistics of the Study Variables and Their Associations With Loneliness.
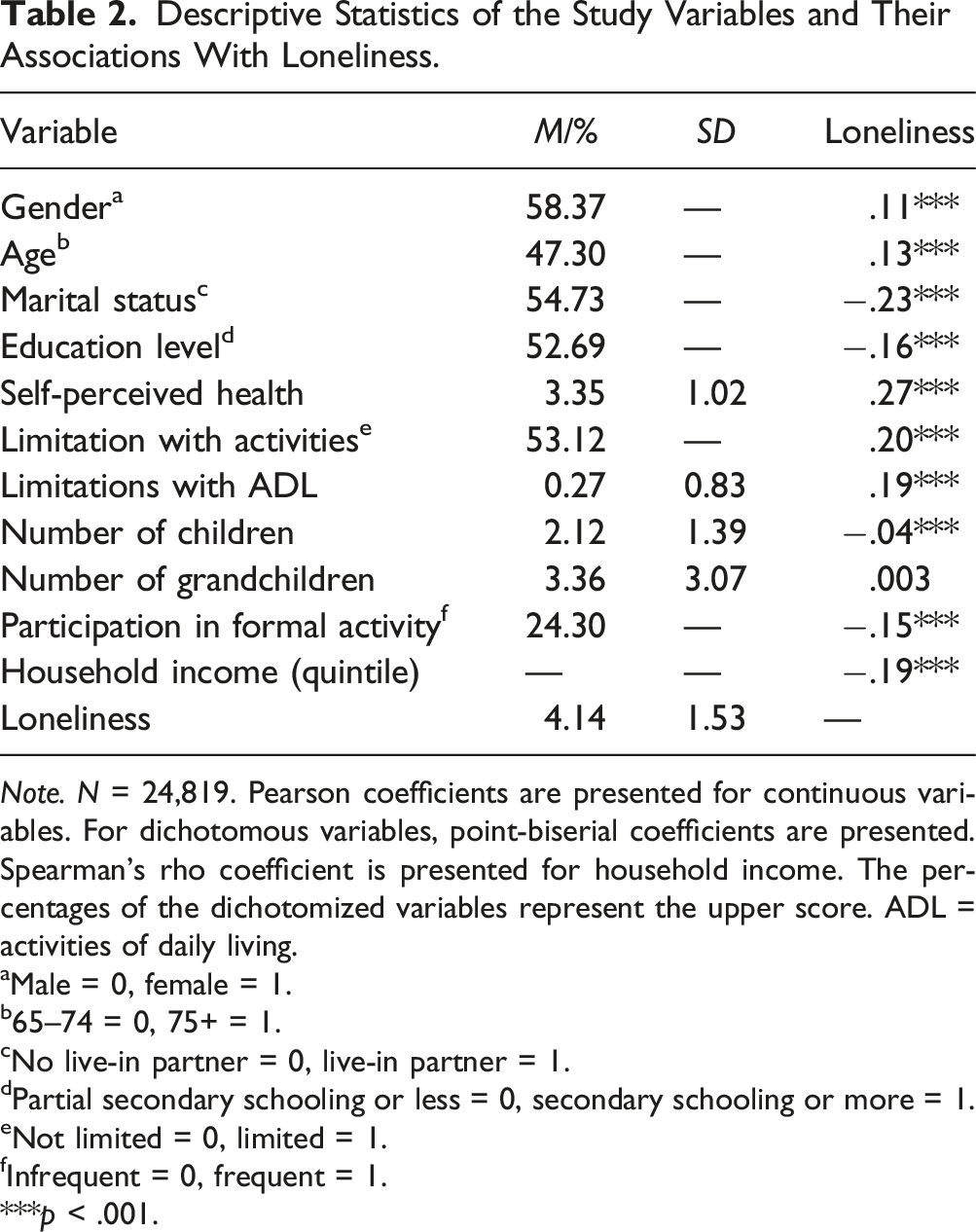
Note. N = 24,819. Pearson coefficients are presented for continuous variables. For dichotomous variables, point-biserial coefficients are presented. Spearman’s rho coefficient is presented for household income. The percentages of the dichotomized variables represent the upper score. ADL = activities of daily living.
aMale = 0, female = 1.
b65–74 = 0, 75+ = 1.
cNo live-in partner = 0, live-in partner = 1.
dPartial secondary schooling or less = 0, secondary schooling or more = 1.
eNot limited = 0, limited = 1.
fInfrequent = 0, frequent = 1.
***p < .001.
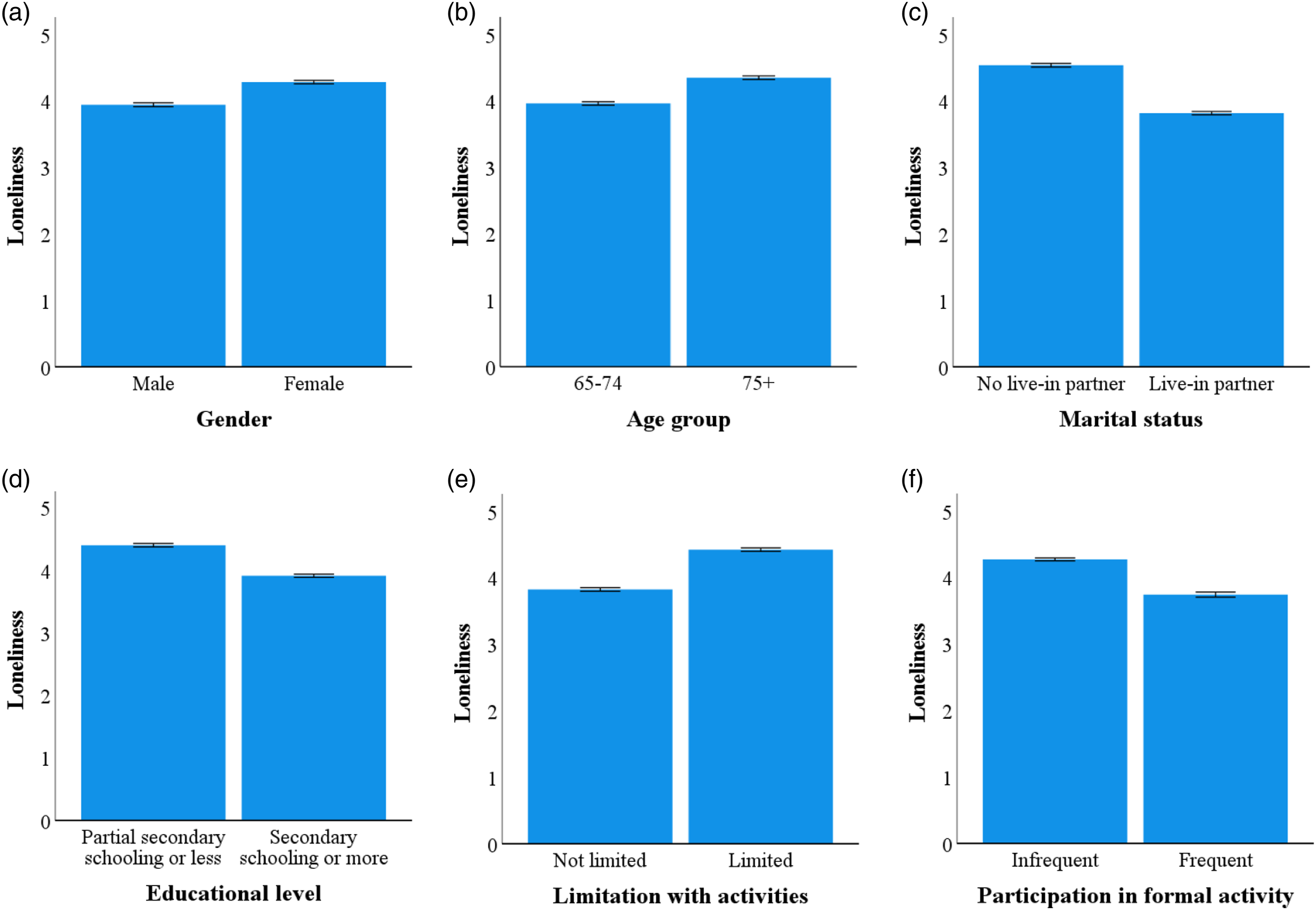
Means and 95% confidence interval of loneliness by: gender (a), age group (b), marital status (c), educational level (d), limitations in activities (e), and participation in formal activity (f). Note. N = 24,819.
Moderation Analysis
Results of Hierarchical Multiple Regression Analysis Predicting Loneliness.
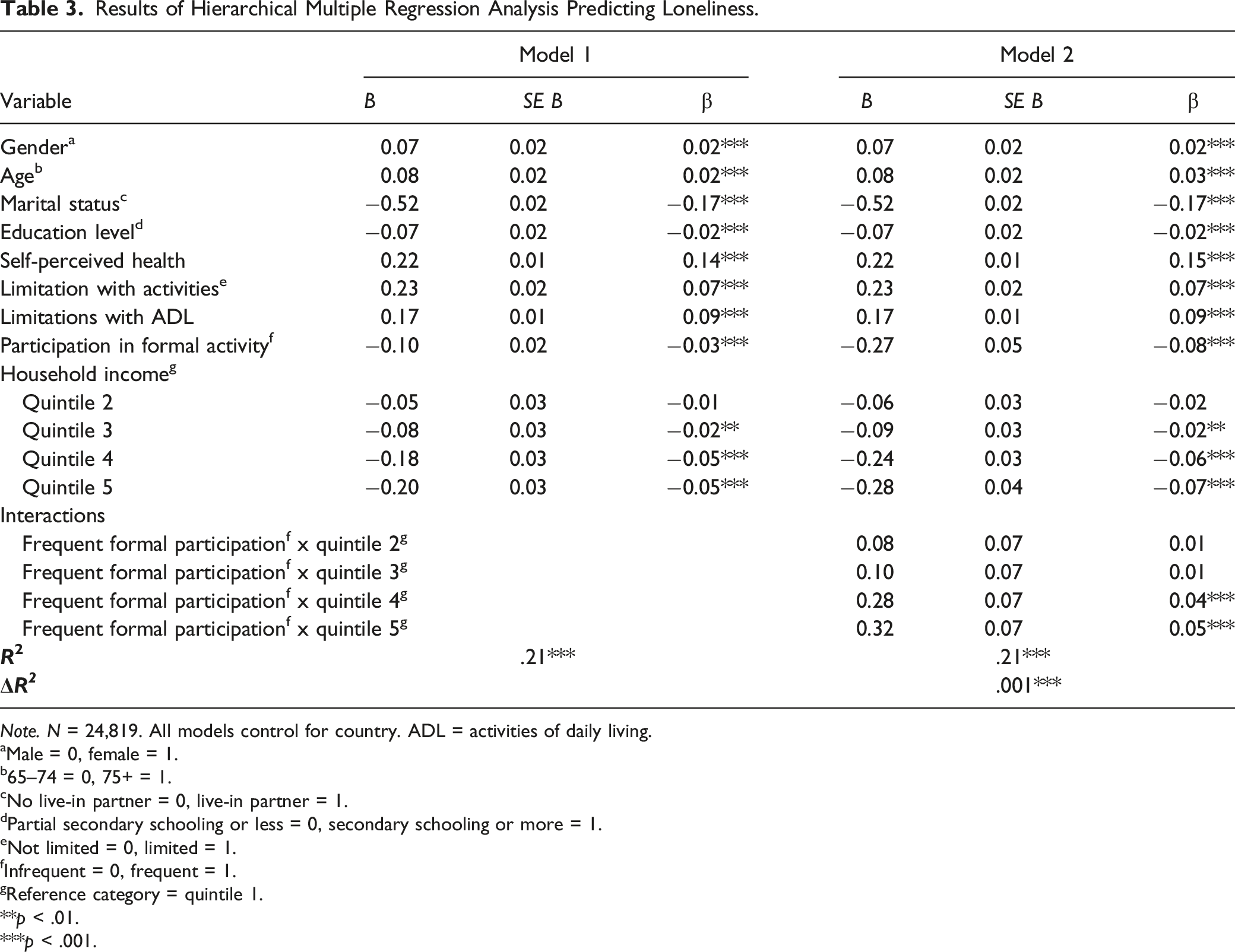
Note. N = 24,819. All models control for country. ADL = activities of daily living.
aMale = 0, female = 1.
b65–74 = 0, 75+ = 1.
cNo live-in partner = 0, live-in partner = 1.
dPartial secondary schooling or less = 0, secondary schooling or more = 1.
eNot limited = 0, limited = 1.
fInfrequent = 0, frequent = 1.
gReference category = quintile 1.
**p < .01.
***p < .001.
Conditional Effects of Participation in Formal Activity on Loneliness.
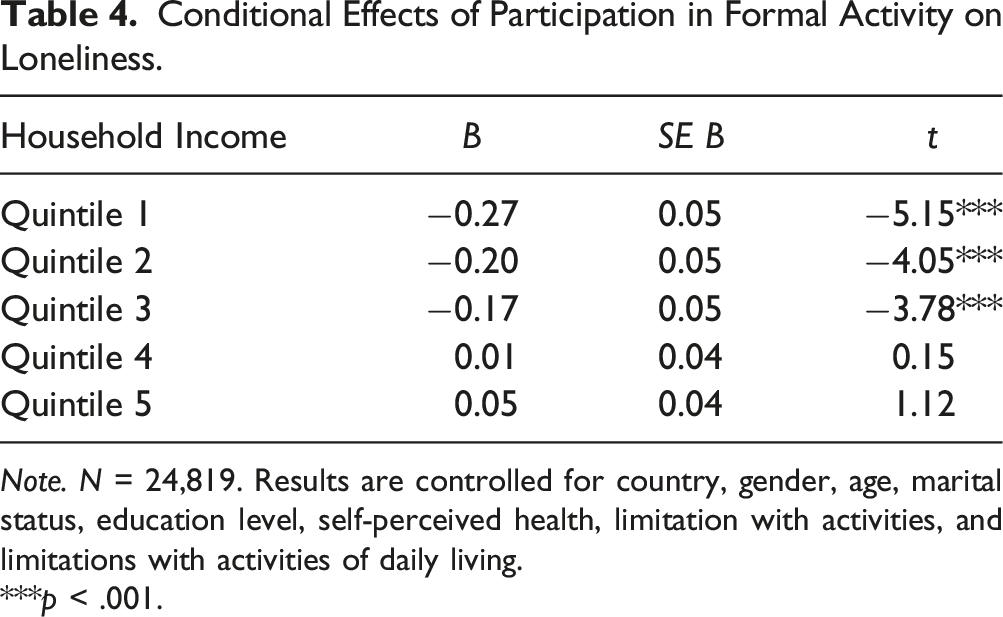
Note. N = 24,819. Results are controlled for country, gender, age, marital status, education level, self-perceived health, limitation with activities, and limitations with activities of daily living.
***p < .001.
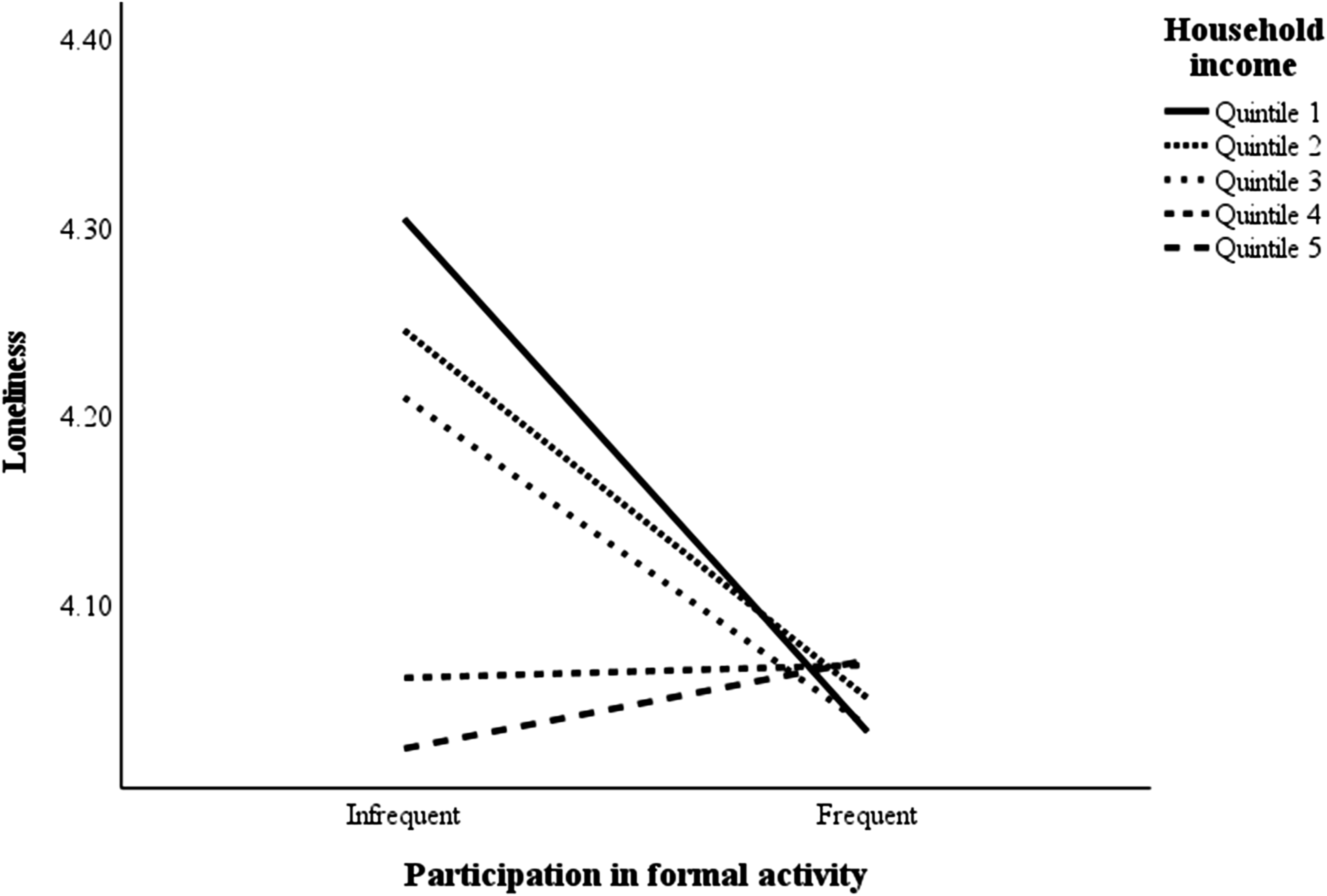
Simple-slope technique for plotting the interaction of participation in formal activity and household income.
Discussion
In order to address one of the greatest social challenges facing humanity, reducing the loneliness that accompanies aging, we must enhance our understanding of the factors that increase loneliness and strive to reduce them. Social participation (such as hobbies, classes, and courses) is considered highly significant for well-being in old age (Mannell & Snelgrove, 2012). After retirement its importance increases (Kelly, 1987; Nimrod, 2007), and is further accentuated in the event of loss, such as the death of a spouse (Nimrod, 2007).
Still, inequalities exist in the aging experience and lead to gaps in the ability of older adults to take advantage of the opportunities that exist in old age, and therefore the weaker groups suffer more from non-participation in social activity and loneliness (Bosma et al., 2015; Hansen & Slagsvold, 2015). The present study adds another layer to the link between participation in social activity and loneliness, showing that income has the potential to moderate this relationship; while infrequent participation in formal social activity of a low-to-moderate income (quintiles 1–3) older adults increases loneliness, higher-income (quintiles 4–5) older adults did not experience loneliness as a result of infrequent participation.
The research findings can be explained by theories from the field of social capital specifically adapted for the older age. Social capital is an umbrella concept that involves individual (i.e., family and friends) and collective social resources (e.g., neighborhoods), and their structural (e.g., social networks, social contacts, and participation) and cognitive aspects (e.g., social support and sense of belonging) (Forsman et al., 2011; Nyqvist et al., 2014). The association between lower income and limited social capital has been proven in previous research (Antonucci et al., 1999; Benner & Wang, 2014; Burke et al., 2010; Hughes et al., 2004; Kearns et al., 2015; Portes, 1998). Lower income increases the probability of residing in an area characterized by partial social services, higher neighbor turnover, and limited transportation service, all of which negatively affect the ability to cultivate social connections (Barnes et al., 2006; Livingston et al., 2010). Lower income also negatively affects an adult’s health status, partly due to poor access to health services and risky health behaviors, and, in turn, negatively affects his/her level of social interaction and social capital (Deaton, 2002). Limited social capital increases the probability of experiencing loneliness (Coll-Planas et al., 2017; Nyqvist et al., 2016).
The gap in social capital may contribute to the fact that lower income adults are fundamentally more vulnerable to infrequent participation in formal social activities, while the social capital accumulated by more affluent adults protects them from being dependent on formal social activities in order to combat loneliness.
Moreover, formal social participation such as a club or community center involves financial expenses and lower income older adults may not be able to afford them (Antonucci et al., 1999; Callan et al., 1993; Scharf et al., 2005), and often precludes adults who do not have the means to join such an activity, thus increasing their chances of experiencing loneliness. This negative impact is not seen among well-to-do adults who do not experience that economic barrier and can afford the expense involved in this type of social participation.
The fact that income is a factor that moderates the link between infrequent participation in formal social activity and loneliness reinforces the importance of reducing the economic constraints on leisure utilization, a point that has also been raised in previous studies (Griffin & McKenna, 1998; McPherson, 1991). We encourage policymakers to tailor interventions to support lower income older adults and this in effect opens the door to implementing a differential approach by encouraging participation in formal social activity and income-dependent subsidy of the activity. These steps may increase the participation of disadvantaged older adults in social activity and thus decrease their loneliness and improve their health and well-being.
Strengths and Limitations
Our study has a number of strengths, including the use of cross-nationally comparable data and the loneliness variable itself which was examined and well-validated and its scale recently harmonized for use in SHARE (Malter & Börsch-Supan, 2013).
At the same time, it is important to also be aware of the limitations of the study. The main limitation is that the independent variables, participation in formal activity and income, rely on participants’ self-report, which may be inaccurate and lead to biased conclusions.
Also, the “income” variable was chosen in our study as representative of the older adults’ socio-economic level, while more and more studies use the “wealth” variable (Demakakos et al., 2016; Niedzwiedz et al., 2016) with the view that wealth (total financial and real assets, minus debts) is a variable that accumulates over the years and therefore, in old age, more accurately reflects the socio-economic situation, especially after retirement.
In addition, we suggest further examination of the effect that the type of formal activity and gender have on the moderating variable—income—in accordance with previous studies that have shown differences in the utilization of leisure activities are gender-dependent, and specifically that older women engage in leisure activities more frequently than do older men (Stanley & Freysinger, 1995).
Footnotes
Acknowledgments
This paper uses data from SHARE Waves 6 (DOIs:10.6103/SHARE.w6.710), see Börsch-Supan et al. (2013) for methodological details. The SHARE data collection has been funded by the European Commission, DG RTD through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812), FP7 (SHARE-PREP: GA N°211909, SHARE-LEAP: GA N°227822, SHARE M4: GA N°261982, DASISH: GA N°283646), and Horizon 2020 (SHARE-DEV3: GA N°676536, SHARE-COHESION: GA N°870628, SERISS: GA N°654221, SSHOC: GA N°823782), and by DG Employment, Social Affairs & Inclusion through VS 2015/0195, VS 2016/0135, VS 2018/0285, VS 2019/0332, and VS 2020/0313. Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071 C, RAG052527 A) and from various national funding sources is gratefully acknowledged (see ![]() ).
).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
Both authors contributed to each phase of this study—data collection, analysis, and writing.
Ethics Approval
The data for this study were taken from the European Health, Aging and Retirement Survey (SHARE).
Consent to Participate
The data used in this study were gleaned from an expansive survey (SHARE) for which the respondents agreed to participate.
Consent to Publish
The data used in this study were gleaned from an expansive survey (SHARE) for which the respondents agreed to participate. Thus, their data are being used with their knowledge and agreement.