
Abstract
This study explored the experiences of Australian family members having conversations about driving with older adults. An exploratory cross-sectional design using an online survey was carried out with Australian family members of current or retired (former) older drivers. One hundred and fifty-six intergenerational family members across Australia completed the survey. Qualitative content analysis of free-text responses identified that the outcomes of conversations were impacted by a range of environmental and individual factors. The essence of conversations centered around two opposing (positive and negative) discourses. The findings highlighted that an individualized approach to the content of conversations is required due to; driver attributes and actions, variations in the level of support experienced by family members, differences in physical and cognitive declines with age, negative perceptions on the impact of driving retirement, and absence of acceptable alternatives to driving. We recommend using positive discourse and reappraisal techniques when initiating driving conversations with older adults.
Keywords
• New understandings of the nuanced approaches employed by family members when initiating conversations with older adults about the sensitive topic of driving. • Offers intergenerational family member perspectives into the content of conversations between family members and older adults on decisions that are complex and emotionally charged. • Provides insight into environmental and individual factors impacting the outcome of conversations about driving between family members and older adults.
• This study has practice implications for family members and primary care professionals in how and when to approach conversations about driving. • Using positive discourse and reappraisal techniques should be considered by family members when initiating conversations about driving. • Driving conversations with older adults should occur well before a critical event, to facilitate the continuance of safe driving or prepare for driving retirement.What this paper adds
Applications of study findings
Introduction
Driving a car is highly valued and the preferred mode of transport by older adults in western societies (Cui et al., 2017). Driving affords convenience and embodies independence, freedom, and social participation (Buys et al., 2012; Ang et al., 2019; Pristavec, 2018) and therefore necessitates avoidance of premature driving retirement. Nonetheless, many older adults will become reliant on alternatives to driving for up to ten years post driving retirement (Foley et al., 2002). Greater attention is required to understand how best to support older adults to either continue driving for as long as safe to do so or transition to driving retirement.
To ensure older drivers are prepared and adjust for life after driving, conversations and planning are advised to start well before driving skills decline or driving retirement is forced (Betz et al., 2016; Pomidor, 2019). Conversations are crucial as driving retirement is linked to health and social declines including depression (Chihuri et al., 2016). A considered approach to the discourse or language used when initiating conversations is needed, as driving retirement is perceived as an end-of-life event for some older drivers (Veerhuis et al., 2022). Deficit discourse focuses on the deficiencies or failures of an individual or group of people, while positive discourse emphasizes agency and capabilities (Birt et al., 2017).
Involvement in driving decisions is critical for most older adults due to the importance placed on driving (Betz et al., 2016). However, older adults’ decisions about driving are also guided by the advice of trusted confidants, such as family members, friends, or health care professionals (D’Ambrosio et al., 2007; Johnson, 1998; Betz et al., 2016). Spouses, adult children, and friends provide a meaningful role in the decision process about changes to driving behavior (Ang et al., 2019, 2020; Johnson, 1998). Although living arrangements can impact preferences, spouses are the preferred choice by many older adults to engage in the initial conversation about driving (D’Ambrosio et al., 2007). Family members also provide practical and social support to enable the continuance of lifestyles and quality of life (Ang et al., 2019; Jones et al., 2018; 2020; Musselwhite & Shergold, 2013). For example, the preferred alternative to driving is being a passenger in a family member or friend’s car (Jones et al., 2018). For these reasons, it is important to understand the perspective of family members who are often best placed to initiate a conversation about driving.
Despite the preferences of older adults for family member involvement, the experiences of those who attempt conversations about driving with older relatives vary widely. Conversations about driving between older adults and their family members occur infrequently or are in response to concerns about safety (Betz et al., 2019) with the preface to stop the person from driving rather than maintenance of driving (Connell et al., 2013; Johnson, 1998). In one study, only 26% of family members reported ever talking to their older relative about driving (Connor et al., 2021). Varied experiences of conversations between family members and older drivers are reported, ranging from positive (Connor et al., 2021) to emotive or adversarial (Lafrance et al., 2022; Liang et al., 2015).
Conversations and decisions about driving may be challenging or avoided for several reasons. First, family members may not feel supported or lack the confidence to broach such conversations (Connell et al., 2013; Liang et al., 2015). Second, they may fear an increased burden on themselves once the older adult retires from driving (Connell et al., 2013). Third, they may have concerns about the reduced independence the older adult will experience when driving retirement occurs (Liang et al., 2015) or anticipate a negative reaction from the older driver (Connell et al., 2013; Söllner & Florack, 2019).
While these studies provide a descriptive account and identify the barriers to having a conversation with the older driver, there is little attention to the nuanced approaches which facilitate conversations with older drivers from the perspective of family members
The extant literature on family member experiences of approaching conversations with an older adult about driving provided the impetus for this study. The purpose was to explore the views and experiences of Australian family members having conversations about driving with older adults.
Design and Method
Study Design
This study was part of a broader research program using a co-design approach with advisory groups. The advisory groups included key experts and stakeholders (including older adults, the transport industry, gerontological nursing, law, human geography, marketing, primary health doctors, occupational therapy, eyecare and health promotion) to develop a decision aid for older drivers. This exploratory, cross-sectional study utilized an online survey to explore the views and experiences of Australian family members having conversations about driving with older adults. Ethics approval was obtained from the University of Wollongong Human Research Ethics Committee (ETH03735) and we followed the Standards for Reporting Qualitative Research (O’Brien et al., 2014).
Sample and Recruitment
For inclusion in the present study, participants had to: (i) self-identify as a family member of a current or retired driver aged 60 years or over; (ii) reside in Australia; (iii) understand written English; and (iv) have access to the internet. We chose the age of 60 for the current or retired older driver because this age marks the start of travel concession eligibility for states and territories of Australia (Australian Human Rights Commission, 2019).
Snowball techniques were used to recruit a convenience sample of family members between August and October 2020 (Sue & Ritter, 2012). Recruitment ceased after three reminders were emailed to the core contact list and our diverse networks were exhausted. Email invitations with a link to the survey were disseminated to networks of the research team including older adult social groups and email contact list of the Aged Dementia Health Education and Research (ADHERe) center. An information sheet informed participants prior to commencing, that the survey was anonymous. Voluntary completion of the online survey was accepted as tacit consent to participate.
Data Collection
The survey was administered through the web-based software system, Qualtrics (Qualtrics, Provo, UT). The development of survey questions was guided by: (i) the study aim; (ii) existing literature that reports family member concerns about driving and the absence of conversations (Betz et al., 2019; Connell et al., 2013) and; (iii) expert knowledge from core members of an advisory group (n = 12).
Content and face validity of the survey questions were achieved through consensus within the research team. Pre-testing of the survey was conducted online including end-to-end testing (Sue & Ritter, 2012) with two cohorts: (i) research team members, who were family members of current or retired older drivers or who had experience with fitness to drive assessments (n = 6); and (ii) a convenience sample of older drivers and family members who were not involved in the survey development (n = 4). Survey questions were revised based on feedback from the pre-test.
Open-ended survey questions.
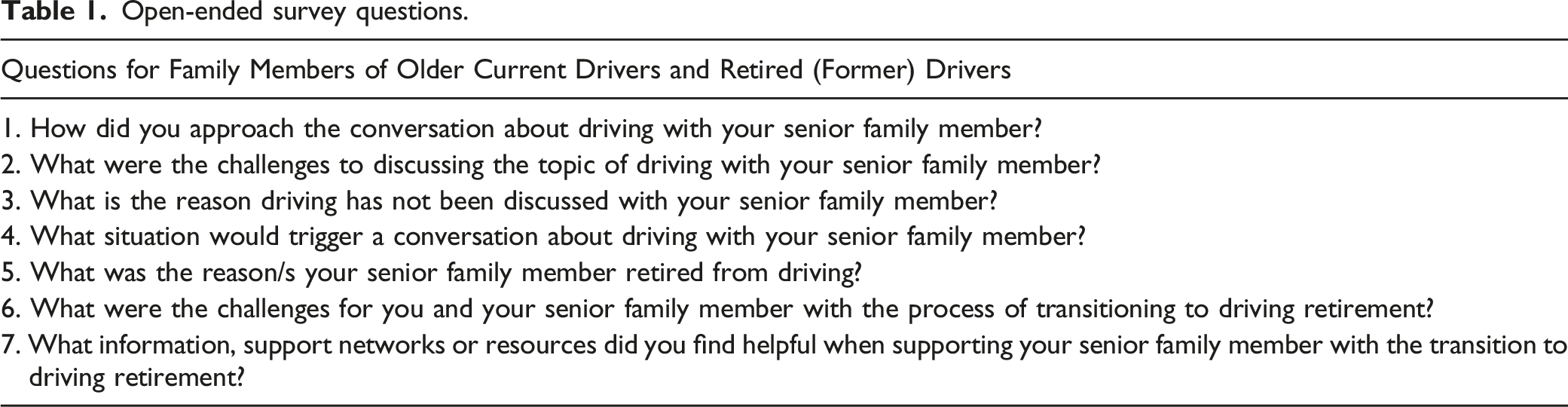
The format of the survey was designed to accommodate the needs of participants who may have been of a similar age to the older adult (e.g., spouse or partner). Design features included the use of a large font size, simple interface answer options, and clear presentation of questions (Sue & Ritter, 2012).
Data Analysis
The demographic characteristics of participants were analyzed using Microsoft Excel, version 16. Qualitative content analysis was guided by Elo and Kyngäs (2008) and Erlingsson and Brysiewicz (2017) to generate knowledge and understanding from the perspective of family members about the experiences of conversations about driving with older adults. Anonymized, qualitative data from the free-text responses were downloaded into Excel and then imported into NVivo Pro 12 (QSR International). Initially, the lead author became familiar with the data by reading the qualitative free-text responses. Using an inductive approach and staying close to the text, open coding of units of meaning (words or sentences) were identified and labeled. Next, using an iterative process, codes were organized into categories based on similar concepts to gain insight into the manifest content (Elo & Kyngäs, 2008; Erlingsson & Brysiewicz, 2017). Reflecting on the study aim, an iterative and interpretative process was applied to generate themes by combining similar categories to provide an understanding of the latent meaning of the content (Erlingsson & Brysiewicz, 2017). Themes and categories were extrapolated to generate a mind map and conceptual table that included quotes. Consensus about the appropriate assignment of labels with themes, categories, and exemplar quotes was achieved through discussions between authors.
Results
Participant Characteristics
Characteristics of study participants (n = 156).
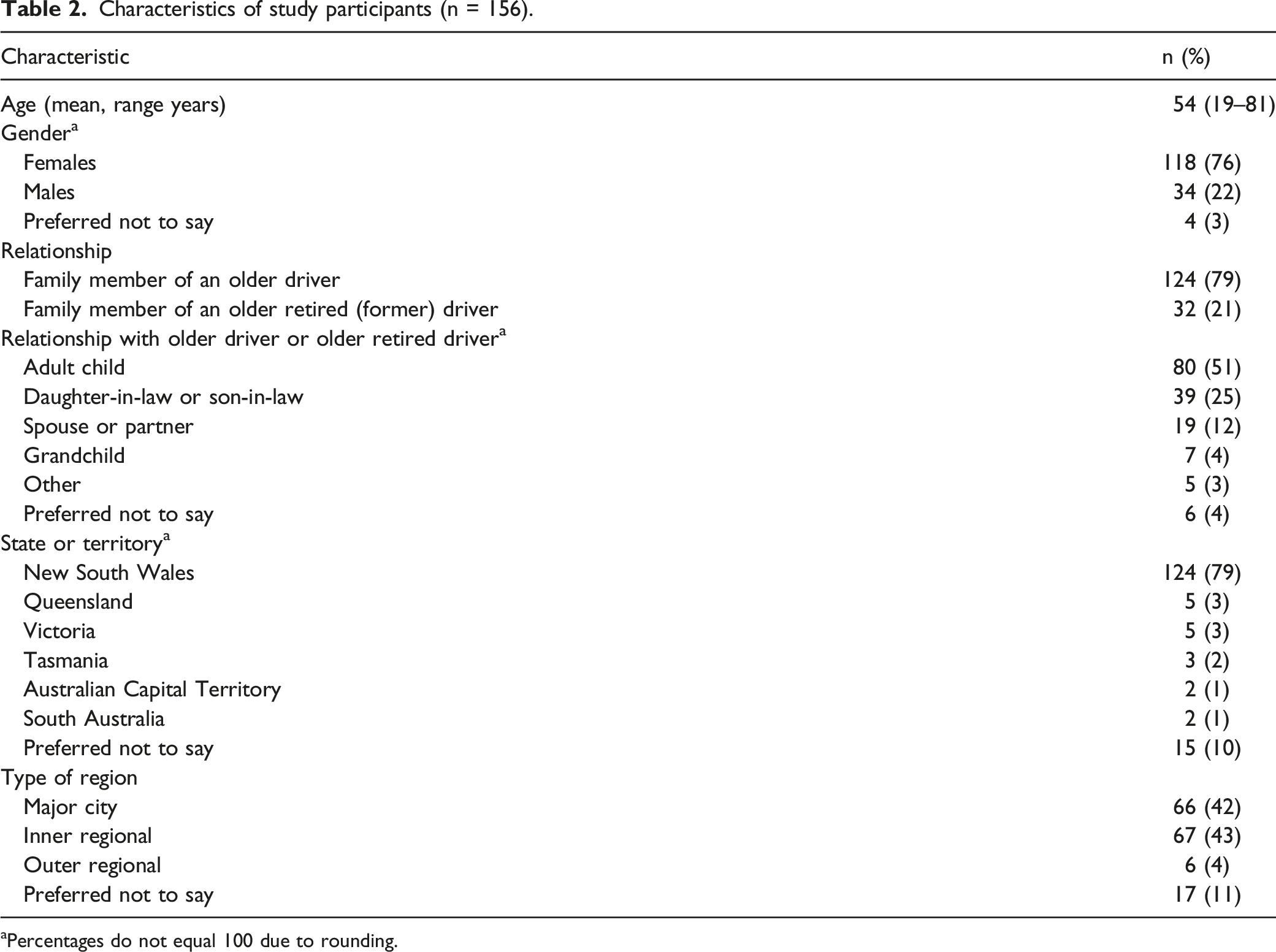
aPercentages do not equal 100 due to rounding.
Current and Retired (Former) Older Driver Characteristics
Characteristics of current and retired (former) older drivers (n = 156).
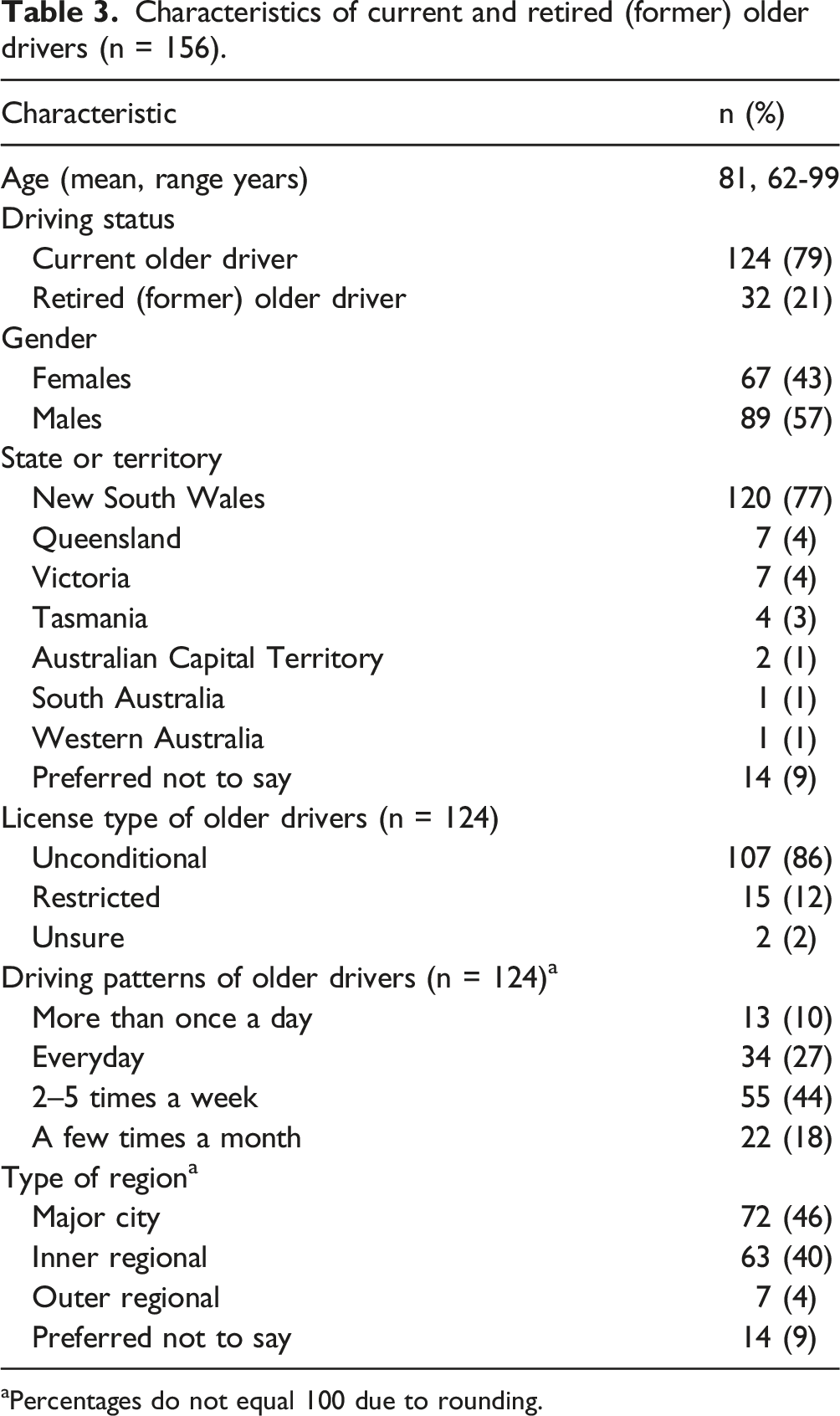
aPercentages do not equal 100 due to rounding.
Key Themes
Three themes were identified from the analysis, which are graphically depicted in Figure 1: (1) approaching the conversation, (2) the essence of conversations, and (3) defining the outcomes of conversations. Illustration of themes describing the experiences of family members with having conversations about driving with older adults.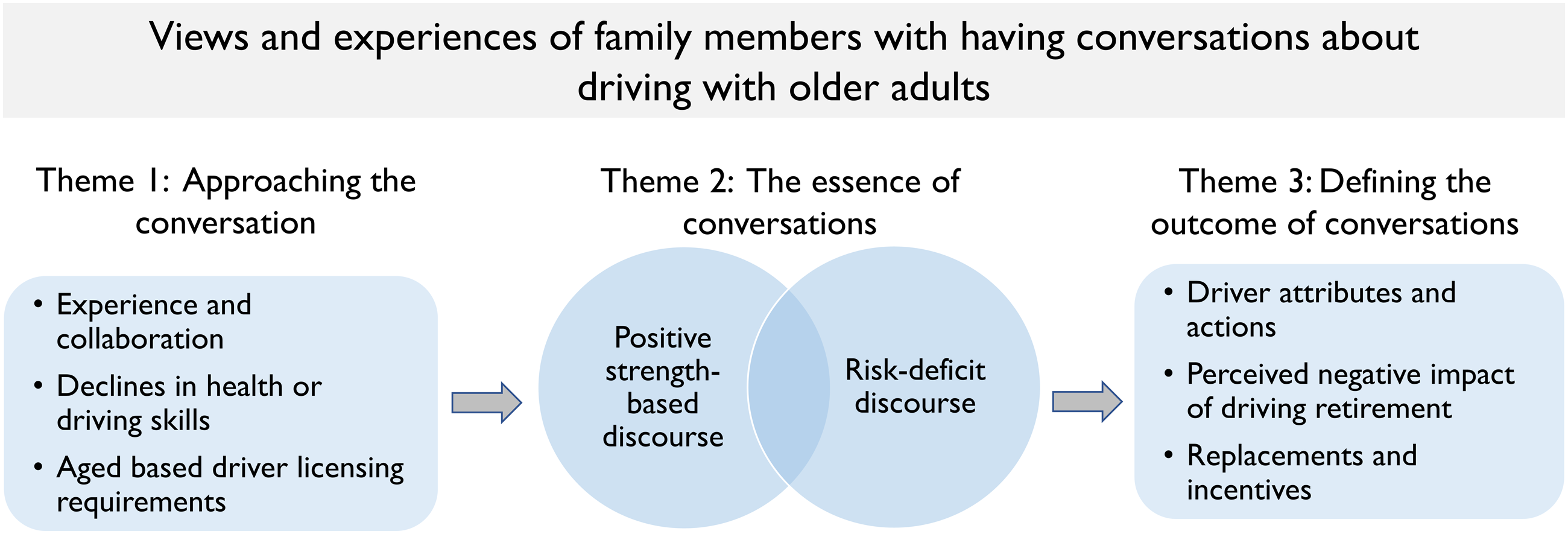
Theme 1: Approaching the Conversation
Participants identified several key triggers that prompted an attempt to discuss driving with current or retired (former) older drivers. Conversations initiated by the older adult were the ideal approach, as it led to less volatile dialogue and less need for resources or external support. Most conversations were initiated by family members either directly by themselves or with other support networks. Often, these types of conversations were triggered by declines in health or driving skills, or age-based licensing policies.
Experience and Collaboration
Family members who had prior personal or professional experience with driving conversations were confident in their perceived ability to initiate conversations about driving.
My previous experience with my
parents-in-law
meant I knew the ropes. (Female, adult child of older driver, age 59)
Some participants preferred to enlist the help of other family members to collectively approach the older driver. Others sought the advice of professionals such as general practitioners (GPs), the driver licensing authority or police to support them. Even so, there were individual differences in the perceived levels of support received from health professionals, and some family members questioned the role of the GP in the driving decision process. One adult child of an older retired driver highlighted how they felt unsupported by the older driver’s doctor in achieving the desired outcome of having his mother’s driver’s license canceled.
To get the doctor on side, which we never did. Doctor thought she was ok to drive, even though she was heavily medicated with pain killers due to osteoarthritis. We had to then contact the RMS [driver licensing authority] and ask the next step to get her license taken off her. We had to report that she was an unsafe driver as her doctor would not do this. (Male, adult child of older retired driver, age 66)
Contrastingly, family members also describe how the older driver refused to listen to the GP or describe a positive experience where the GP was crucial in supporting them with the decision process. Other family members questioned the suitability of the role of the GP in making decisions about driving.
I don’t think some GPs manage guiding older patients to retire from
driving—and
should they be the right ones to make this decision? Some elders are clearly dangerous and I wonder what the legal ramifications are for GPs who approve a licence for someone that clearly shouldn’t be behind a wheel! (Female, adult child of older retired driver, age 68)
Declines in Health or Driving Skills
Family members were motivated to start conversations about driving when they perceived the health of the older driver had declined, for example, deteriorating vision or reduced reaction time. Diminished driving skills were brought to the attention of family members because of damage to vehicles (scratches or scrapes) or car collisions or near misses. Sometimes these types of concerns were raised by friends, neighbors, or other family members which then led to a conversation about driving. One spouse of an older driver felt compelled to have a conversation when they witnessed the older driver had: …missed a few red lights when I was in the car. (Male, spouse of older driver, age 81)
Despite multiple attempts by one family member to have a conversation with the older driver, it was only when a serious car collision caused an injury to a loved one that a conversation and changes to driving behavior occurred.
My dad did ignore us until he wrote off the car and clipped his own walker my mother was holding and nearly killed her.
Well—not
quite, but she was thrown in the air and had stitches and heavy bruising with miraculously no broken bones. At least he stopped driving! (Female, adult child of older driver, age 52)
Numerous family members reported they had not yet initiated a conversation about driving. This was because there was no reason to, as declines in the health or driving skills of the older driver were not yet considered “serious” enough. A car collision, near miss, infringement, personal injury or feeling unsafe as a passenger were considered serious enough to warrant a conversation. Some participants were unsure how to approach the conversation while others believed that the older driver would have a negative reaction if they attempted to discuss the matter.
Aged-Based Driver Licensing Requirements
Aged-based licensing requirements (starting at 75 years in NSW) also prompted conversations about driving. Before, or after annual medical driver assessments or on-road driving tests was considered an ideal opportunity to initiate these conversations as families perceived that the older driver would be more receptive to discuss driving. Mum relocated to live near me and not long after she had an age-related driving test coming up. It was a natural trigger to discuss all the possible outcomes, although she was very confident that she would have no problems. (Female, child of older driver, age 59)
If the family member perceived that the older driver had good health and driving skills a conversation was not considered necessary. One dilemma posed was when the older driver passed a driving medical assessment or on-road driving test, but the family member perceived their driving to be unsafe. This made it difficult to have a conversation about alternatives to driving. Moreover, some family members were concerned that driver testing regimes did not adequately protect the older driver or identify those who posed a safety risk to other road users.
After failing [the] driving test, he was given another chance a few days later which he passed. He failed the first test by running a stop sign and speeding in a school zone. Hardly minor issues! (Female, grandchild of older driver, age 31)
Theme 2: The Essence of Conversations
The essence (or content) of conversations between family members occurred through two modus operandi; (i) the positive strength-based discourse, or (ii) the risk, deficit discourse. Most family members described using a single conversational discourse, although some also described using both positive and risk-deficit discourses during conversations with older drivers.
Positive Strength-Based Discourse
Positive discourse included content that validated the skills and experience of the older driver, placed the needs of the older driver as central to the conversations, or where the family member provided solution-oriented advice such as practical help, alternatives to driving, or ways to continue driving. One family member suggested self-regulation strategies as a way of a compromise to continue driving.
Suggesting that they only drive on familiar roads, locally. Asking to avoid long drives to metropolitan areas that are busier. (Female,
child of older driver, age 58)
Typical of the positive strength-based discourse were conversations underpinned by empathy, sensitivity, encouragement, or reassurance and focused on ways to continue driving. Positive discourse included conversations that reappraised the situation and normalized driving retirement, validated the older adults driving skills, or diverted the conversation to other external factors, such as deficiencies of other road users or benefits of reduced car usage. One participant used strength-based discourse to reinforce the competencies of the older driver. They also reframed the situation by avoiding the topics of dementia or memory loss so as not to reinforce the loss of cognitive skills that had already been experienced.
There was a lot of reassurance that her driving skills were not the problem it was the simple fact that she had stopped driving and the car was deteriorating. (Female,
daughter-in-law
of older driver, age not provided).
Risk-Deficit Discourse
Risk-deficit discourse approaches included an emphasis on declines in health or driving skills, being a danger to themselves or others, highlighting collisions or near misses, and failing tests or medical assessments. Expressions and terms used by participants were unsafe driving, dangerous, risky, concerning and highlighted specific health or driving declines.
We told her she was dangerous and had to stop. (Female,
daughter-in-law
of older retired driver, age 58)
Talked about declining ability in general decision making, memory and
mobility. (Female,
daughter-in-law
of older driver, age 64)
Theme 3: Defining the Outcome of Conversations
A range of factors influenced whether attempts at conversations with older adults about driving were considered challenging. They included the attributes and actions of the older driver, the perceived negative impact of driving retirement, acceptable replacements to driving, or incentives to change driving behavior.
Driver Attributes and Actions
Older drivers with self-awareness about declines in their health or driving ability tended to be receptive to having conversations about driving. They were also more likely to initiate conversations themselves or accept that driving retirement would occur at some point. Conversations with older adults exhibiting these types of traits were not perceived by family members to be particularly challenging.
He is very aware of his conditions and limitations and although he dreads the
thought of not being able to drive, he is accepting of the fact. (Female,
spouse of older driver, age 70).
In contrast, for other family members, the conversation was abandoned when there were negative emotive reactions from older drivers such as anger, defensiveness and resentment. These reactions were often attributed to the importance placed on sustaining independence, driving considered a “right” rather than a privilege and perceptions that the topic was an attack on the older driver’s competence. When older drivers were in denial, refused to engage in a conversation, lacked awareness of declines in driving skill or family members believed there would be a significant loss of independence, these conversations were considered more challenging.
Perceived Negative Impact of Driving Retirement
Both older drivers and family members believed that changes to driving behavior would be accompanied by a loss of independence and freedom, and this impacted whether conversations occurred. Participants reported that older drivers felt they would be a burden on others, and the family members themselves expected or had experienced increased responsibilities after the older adult had retired from driving. Participants identified that independence was highly valued by the older person. Sustaining driving was viewed as the only way to maintain their independence which justified encouraging their older adult relative to continue driving. It is her independence that she would be losing if she cannot drive and that is HUGE. She does only drive within a 20 minute sector, and I will still ask her to drive me at times so I can discretely check how she is going. (Female, child of older driver, age 52)
Replacements and Incentives
Conversations were viewed as challenging when there were no viable or acceptable alternatives that would effectively support the continued independence and freedom that driving affords. It was also difficult to explain the other options for transport. She has relied heavily on being able to drive, especially in a country town with limited transport. (Female, child of older driver, age 55)
Some participants reported specifically reframing the conversation to solution-oriented alternatives or self-regulation strategies to help prepare the older driver for driving retirement or to continue driving for longer. The availability of acceptable alternatives and incentives, such as discounted public transport or taxi vouchers were some of the solutions provided.
Fortunately, she lives in a location that has an excellent bus route (or had)
and was able to take a bus to shop, into the city and to the movies! Or to
catch a cab. Her mobility is now reduced and she can’t access the buses
now—so
mostly takes cabs when needed. (Female, child of older retired driver, age 68)
Discussion
For family members of older adults conversations and decisions about driving can be challenging. The findings from this study provide valuable insight into the way conversations about driving occur between family members and older drivers. Most family members in this study (76%) identified themselves as adult children, daughters-in-law or sons-in-law, highlighting the importance of the topic of driving to this cohort. In contrast to past research where only 26% of family members had engaged in a conversation (Connor et al., 2021), 61% of family members in this study had discussed driving with their older driver relative. Spouses or partners are the preferred choice for many married older adults to engage in the initial conversation about driving (D’Ambrosio et al., 2007). The inclusion of spouses and family members other than adult children may be one explanation for the disparity in numbers having had a conversation between our study and that of Connor and colleagues (2021).
Overall, family members' responses confirmed that driving is a sensitive subject to raise with an older adult. However, we found variation in family member experiences when conversations were initiated. Consistent with Lafrance et al. (2022), we found that for some family members, engaging with older adults about driving decisions can be challenging and emotive while for others easier to navigate (Connor et al., 2021). Challenges arise because driving maintains older adults' perceptions of individual freedom and their ability to live independently. These unique individual experiences were influenced by several factors including driver attributes and actions and willingness of the older driver to reflect on their health or engage in conversations, the importance placed on driving, the personal or professional experience of family members in initiating these types of sensitive conversations, and acceptable alternatives to driving.
Older drivers who were aware of their declining health and the impact this had on their driving skill were more likely to engage in conversations about driving. Conversely, those who feared the loss of independence, had limited self-awareness or were in denial about their declining health or driving skills were more likely to resist conversations about driving. Avoidance through denial or refusal to engage with decisions is a typical response by older adults when making decisions generally (Löckenhoff, 2018). Providing family members with alternate strategies or resources to approach conversations with older drivers would be beneficial.
Consistent with prior studies (Betz et al., 2019; Connell et al., 2013) declines in health or reduced driving skills, as evidenced by a car collision or near-miss, are often the subject of and the trigger for a conversation about driving by family members. Our findings also identify licensing renewal policies are a marked event that would prompt a conversation about driving. Family members who had not yet discussed driving overwhelmingly felt that a car collision or near-miss would trigger a conversation in the future. However, delaying conversations until these critical events occur could lead to the focus of conversations being on retirement, rather than maintenance of driving and the sudden or forced loss of driving privileges. Ideally, conversations should be initiated early and over a period of time so that planning for alternatives to driving can occur (Betz et al., 2016; Pomidor, 2019).
The essence of driving conversations between family members typically involved one of two discourses: a positive, strength-based discourse, or a risk-deficit discourse. The use of deficit discourse could be attributed to community perceptions of older age stereotypes which permeate societies across the globe and can lead to poor health outcomes for older adults (Chang et al., 2020). Family members raised concerns about ageist driver testing regimes and stereotyping of older adults driving abilities. Therefore, strategies are needed to address ageism across health and social decisions including those about driving.
Family members who embraced the risk-deficit discourse were directive and authoritarian, with some taking steps to prevent the older driver from continuing to drive. Opponents of the risk-deficit discourse approach assert the person’s strengths and qualities are not acknowledged or valued (Birt et al., 2017). Conversely, other family members positively reappraised the situation by providing solution-orientated advice, offered strategies to continue driving or validated the older adults' skills. This approach may promote optimism about securing future mobility and moderate the emotion that studies identify typically surrounds conversations about driving (Betz et al., 2016).
The findings have practical implications for family members and primary care professionals. First, reappraisal techniques should be considered by family members when initiating conversations about driving. Second, conversations with older adults should occur well before a critical event to facilitate the continuance of safe driving or prepare for driving retirement. Future studies should compare the views of older drivers and family members to identify differences in terms of the perceived effectiveness of various discourse approaches and content options when having conversations about driving. Further insight into how conflicting opinions between family members and health care professionals impact decisions about driving would also be beneficial.
Limitations and strengths
A diversity of perspectives, in terms of the range of intergenerational family members represented, was a strength of this study. The findings should be interpreted in the context of the following limitations. The cross-sectional design prevents establishing causality between different approaches to having conversations about driving and outcomes. In addition, a web-based survey may result in a biased sample toward those with higher technological literacy (Remillard et al., 2014). Convenience sampling with snowballing can lead to self-selection bias, meaning the findings may represent the views of family members with more interest in this topic which can skew the sample. In addition, the sample was not representative of the Australian population which may limit generalizability of the findings. Some groups were under-represented, for example, people from remote and rural areas (where driving may be even more valued due to a lack of public transport) and family members of drivers who were already retired (who could provide the perspective of hindsight when decisions around driving retirement needed to be made). Other personal or situational factors that were outside the scope of this study may also impact decisions about driving self-regulation or retiring from driving and warrant further investigation. For instance, data regarding socio-economic status, education level, social support, living arrangements, and cultural background may provide greater insight into the potential impact of these factors on conversations about driving. Furthermore, older adults may have perceived the content and approach to conversations to be different to that reported by the family members in this study.
Conclusion
Family members who anticipate challenging conversations about driving will often engage external support. Triggers for conversations include aged-based testing regimes, the accumulative impact of declines in driving skills and abilities, or critical events. We propose that family members consider: (1) initiating conversations well before critical events such as a car collision; and (2) using positive discourse and reappraisal techniques as older adults may be more amenable to engaging in conversations about driving.
Supplemental Material
Supplemental Material - “The Challenge is Not to Make Her Feel Old and Bad”: Exploring Australian Family Member Experiences of Conversations About Driving With Older Adults Using an Online Survey
Supplemental Material for “The Challenge is Not to Make Her Feel Old and Bad”: Exploring Australian Family Member Experiences of Conversations About Driving With Older Adults Using an Online Survey by Nadine Veerhuis, Theresa Harada, Karina Murray, Catherine Andrew, Victoria Traynor, and Melanie Randle in Journal of Applied Gerontology
Footnotes
Acknowledgments
We thank the family members for their time and for providing their views and experiences for this study. We acknowledge the contributions of the Driving Change Research Collaboration group from the University of Wollongong.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study, as part of a broader research project, was financially supported by a community road safety grant from Transport for NSW. Representatives from the funding body provided survey instrument feedback and assisted with snowballing recruitment, however, were not involved in data analysis, interpretation or reporting. The first author was also funded by an Australian Government Research Training Program (RTP) Scholarship.
Ethical Approval
This study was approved by the University of Wollongong Human Research Ethics Committee (ETH03735).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.