
Abstract
Formal and informal networks of resources are critical to supporting the growing number of older adults aging in place (AIP). Data are needed from aging-service providers about assets and barriers that impact their abilities to support AIP during the pandemic, as well as emergent needs resulting from response measures. A series of World Café workshops were conducted with aging-service providers in Salt Lake City, Utah, to understand supportive factors, service gaps, and future needs. Novel domains to support AIP in the context of the pandemic were identified: digital access and literacy, social isolation and mental health, and emergency preparedness. Issues related to access, equity, and affordability were identified as overarching themes across domains. Issues reflect concern over how the pandemic exacerbated socioeconomic and cultural disparities impacting older adults who benefit from aging services. Networks of advocacy and support are needed to bolster resources for older adults, caregivers, and aging-service providers.
Keywords
• Distinct challenges have arisen as a result of the COVID-19 pandemic which require aging-service providers to support older adults who are aging in place in new ways. • Emergent needs raised by the pandemic are prioritized by service providers from Area Agencies on Aging and other partnering organizations in this study, and focus on digital access and literacy, social isolation and mental health, and emergency preparedness. • Strategies to promote effective initiatives and policies are described by aging-service providers, including greater cultural competence, reduced barriers to information, expanded networks of support for caregivers, and increased choice in modalities and communication platforms.
• Understanding pandemic-related gaps and challenges through the perspectives of aging-service providers on local and regional levels contributes to the ability to inform future planning, policy, and funding that support older adults aging in place. • Innovations harvested through experiences of aging-service providers can inform the design of support measures to promote the well-being of older adults and their caregivers in a sustainable, coordinated, and long-term manner. • Socioeconomic gaps that the pandemic has exacerbated require awareness, attention, and response in order to ensure equity, access, and inclusiveness in aging.What this paper adds
Applications of study findings
A disproportionate impact of the COVID-19 pandemic falls on the health and well-being of older adults, bringing attention to the significant role that aging-service providers play in supporting older adults who live independently (Grasselli et al., 2020; Richardson et al., 2020). Community-dwelling older adults have been uniquely impacted by the pandemic as public health guidance warns of the need to maintain physical and social distance (Scott et al., 2021). Instructions to isolate at home and restrictions on social events have contributed to reduced social interactions and increased loneliness among older adults (Finlay et al., 2021). Increased depression and reduced quality of life have also been attributed to pandemic response measures (Lebrasseur et al., 2021). Older adults’ subjective evaluations of their own aging were impacted by the pandemic, as negative perceptions of aging increased while positive perceptions decreased (Seifert, 2021). Digital technologies have been identified as a tool to reduce loneliness and isolation (Banskota et al., 2020; Finlay et al., 2021); smart technologies such as sensors, apps, and medical monitoring devises increase one’s ability to age in place, yet there remains a need to address gaps in access and literacy in order to help connect older adults to online community services (Barbosa et al., 2019; Delello & McWhorter, 2017) and leverage technology to support aging in the place where one prefers.
Alongside public health orders to stay home during the pandemic, older adults have long reported preferences for remaining in their homes and communities instead of moving into supportive housing or assisted living (AARP Research, 2018). The desire to age in place is often motivated by a sense of attachment and familiarity that people have for their homes and communities (Golant, 2020; Wiles et al., 2012). Even amidst the COVID-19 pandemic, only 29% of older adults reported planning to relocate to another community (Davis, 2021). To safely age in place, there is often a need to make home modifications (e.g., installation of grab bars, no-step showers, ramps, and smart-home systems) and have community service providers available to provide outside social supports (Canham et al., 2018; Fausset et al., 2011).
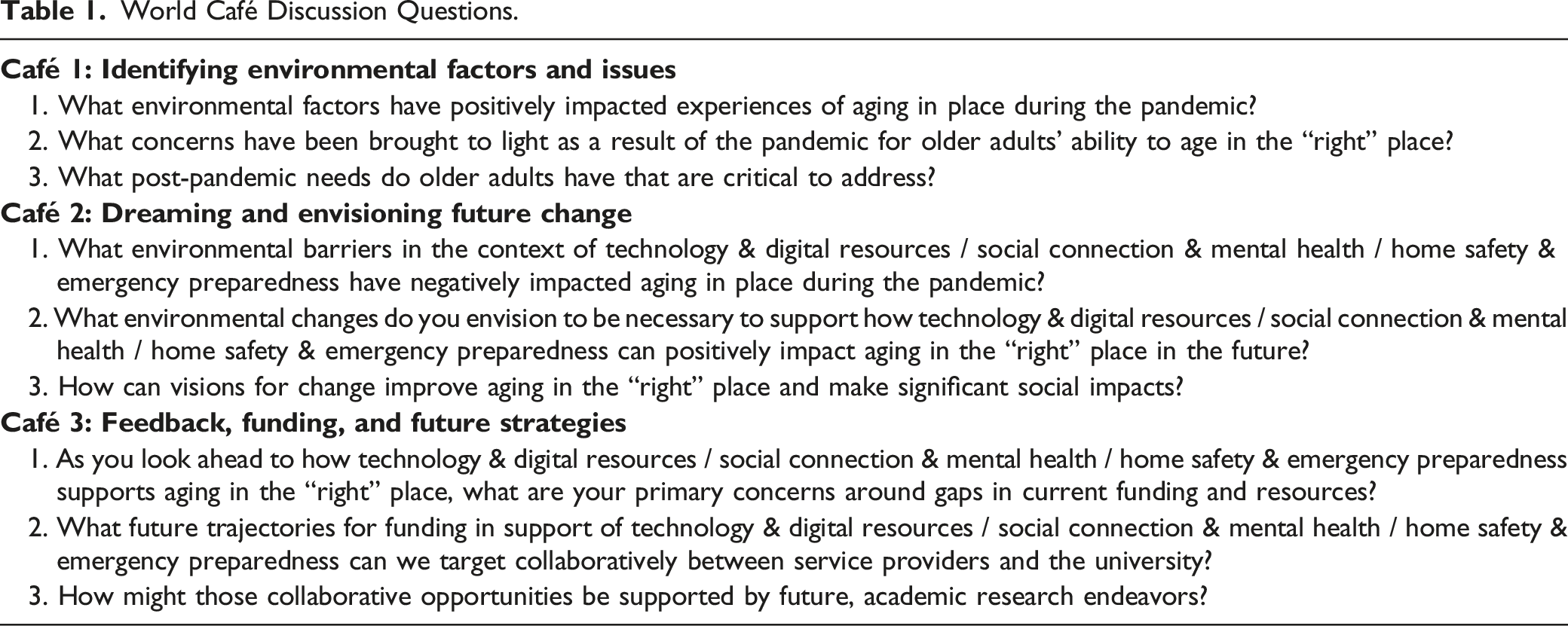
Given the importance of aging in place (AIP), and that of formal supports to age well, there is a need to systematically identify and describe how aging-service providers responded to pandemic conditions, and what community-specific solutions were developed to address rapidly changing needs (Gallo & Wilber, 2021). Attention to the ways that Area Agencies on Aging (AAA) leveraged expertise in service provision and community needs assessments is essential to navigating dramatic shifts in service delivery modes that have been precipitated by the pandemic (Wilson et al., 2020). To address this gap in the literature, we conducted a series of virtual World Café (WC) workshops with aging-service providers who shared experiences of supporting community-dwelling older adults and caregivers during the pandemic. Three research questions guided the WC workshop series: (1) What environmental factors have positively impacted experiences of AIP during the pandemic?; (2) What concerns have been brought to light as a result of the pandemic that have affected older adults’ ability to age in place?; and (3) What post-pandemic needs have been identified as critical to support AIP?
This article describes emergent concerns and future needs prioritized by aging-service providers, and center around topics of technology, mental health, and emergency preparedness. More significant systemic barriers that play into challenges to AIP exacerbated by the pandemic were identified around issues of equity, affordability, social and cultural stigmas, and caregiving. Collaborative initiatives that were created during the pandemic through the release of emergency federal response funds require strategies for future, long-term funding to be economically and socially sustainable. The knowledge garnered from needs and responses in these areas can be used to guide future policy and planning that support inroads to healthy AIP among community-dwelling older adults.
Methods
WC workshops host critical dialog among individuals with similar problems or interests in order to share knowledge and foster collaborative learning (Brown & Isaacs, 2005). This method originated in community development and is increasingly used in research as it creates a means to collect data that provide insight into complex issues through the lens of lived experiences and disciplined inquiry (Löhr et al., 2020). Seven principles guide the WC format and include (1) setting the context; (2) creating a hospitable space; (3) exploring critical questions; (4) encouraging contribution from all participants; (5) connecting perspectives; (6) listening for patterns and insights; and (7) harvesting and sharing discoveries (Brown & Isaacs, 2005). WCs are traditionally held in-person around café like tables, though virtual WC formats have been credited with giving participants more time for reflection than in face-to-face settings, potentially positioning participants to make a deeper contribution to topics (Gyllenpalm, 2002). We conducted virtual WCs over Zoom due to pandemic restrictions on in-person gatherings. Institutional approvals were obtained prior to the start of the study (IRB 00141945).
We recruited a group of 34 aging-service providers from the Salt Lake Valley in Utah to discuss challenges and opportunities to support older adults during the COVID-19 pandemic. Participants represented the federally designated Area Agency of Aging (AAA) for Salt Lake County and the State of Utah’s Division of Aging and Adult Services (DAAS) as well as major healthcare and non-profit organizations that serve older adults. The authors utilized a university-maintained database to identify aging-service providers who held leadership and administrative roles in their organizations during the emergency response period of 2020, and who expressed interest in receiving information about research studies. Participants were recruited through invitations circulated via email with information on the study, and participation was voluntary. An IRB-approved Informed Consent Cover Letter was sent to participants by email once they registered for the study. The informed consent document was verbally reviewed between researchers and participants prior to the start of WC sessions. Participants were free to discontinue participation in the study at any time.
Salt Lake County was chosen as the site of the study because of the researchers’ local connections. To contextualize demographic characteristics of this region, it is important to recognize net migration as a transformative factor as the state’s population is expected to grow by over 2.2 million people (a 66% increase) by the year 2060 (Kem C. Gardner Policy Institute, 2022). Salt Lake County is the largest county in the state; about 10% of Salt Lake County residents are over 65 years old; among those age 65+, the median age is 72.9; 44.9% are male and 55.1% are female; the vast majority of adults age 65+ (92.3%) self-identify as white; over half (58.8%) are married; over one-third (34.7%) self-report as having a disability; close to a quarter (21.0%) are active in the labor force; 11.0% are foreign born; and 7.2% live in poverty (Salt Lake County Aging Services, 2018).
World Café Discussion Questions.
Conversations were recorded, transcribed, and checked for accuracy. Any personal identifiers were removed to maintain anonymity. Researchers worked in sequential phases to thematically analyze data and identify central concepts (Braun & Clarke, 2006). Familiarization with data was ensured through reading transcripts and listening to audio recordings. The team of faculty researchers and assistants identified an initial set of codes based on the whiteboards, and a pair of research assistants independently coded transcripts using NVivo12 software (QSR International, 2018). Codes were cross-read by faculty researchers and assistants, and a codebook was developed by the research team. Codes were grouped into preliminary themes and reviewed by the team. Defining and reviewing themes supported the iterative nature of discerning meaning, synthesizing codes into overarching themes, and identifying patterns between themes.
Results
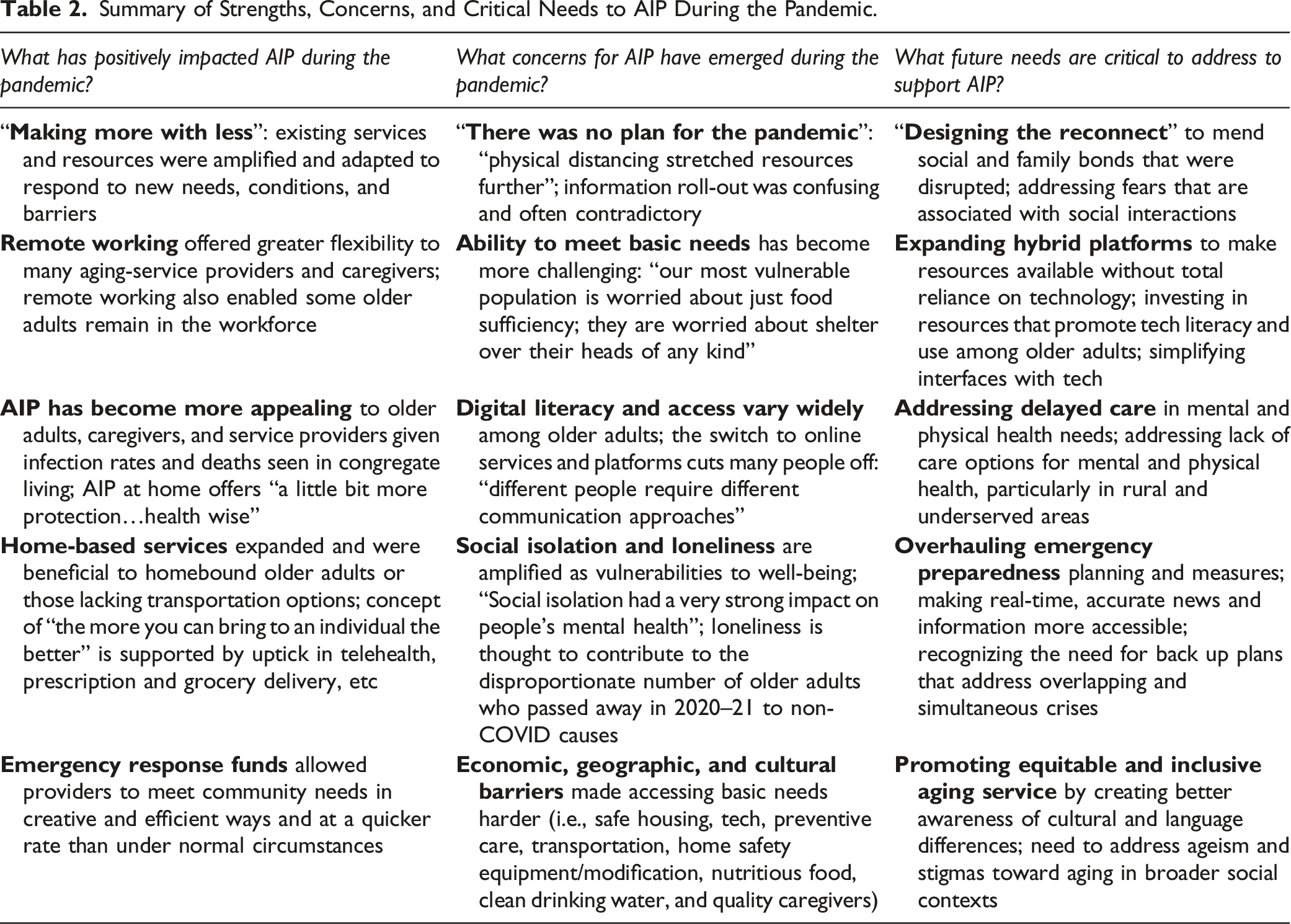
Summary of Strengths, Concerns, and Critical Needs to AIP During the Pandemic.
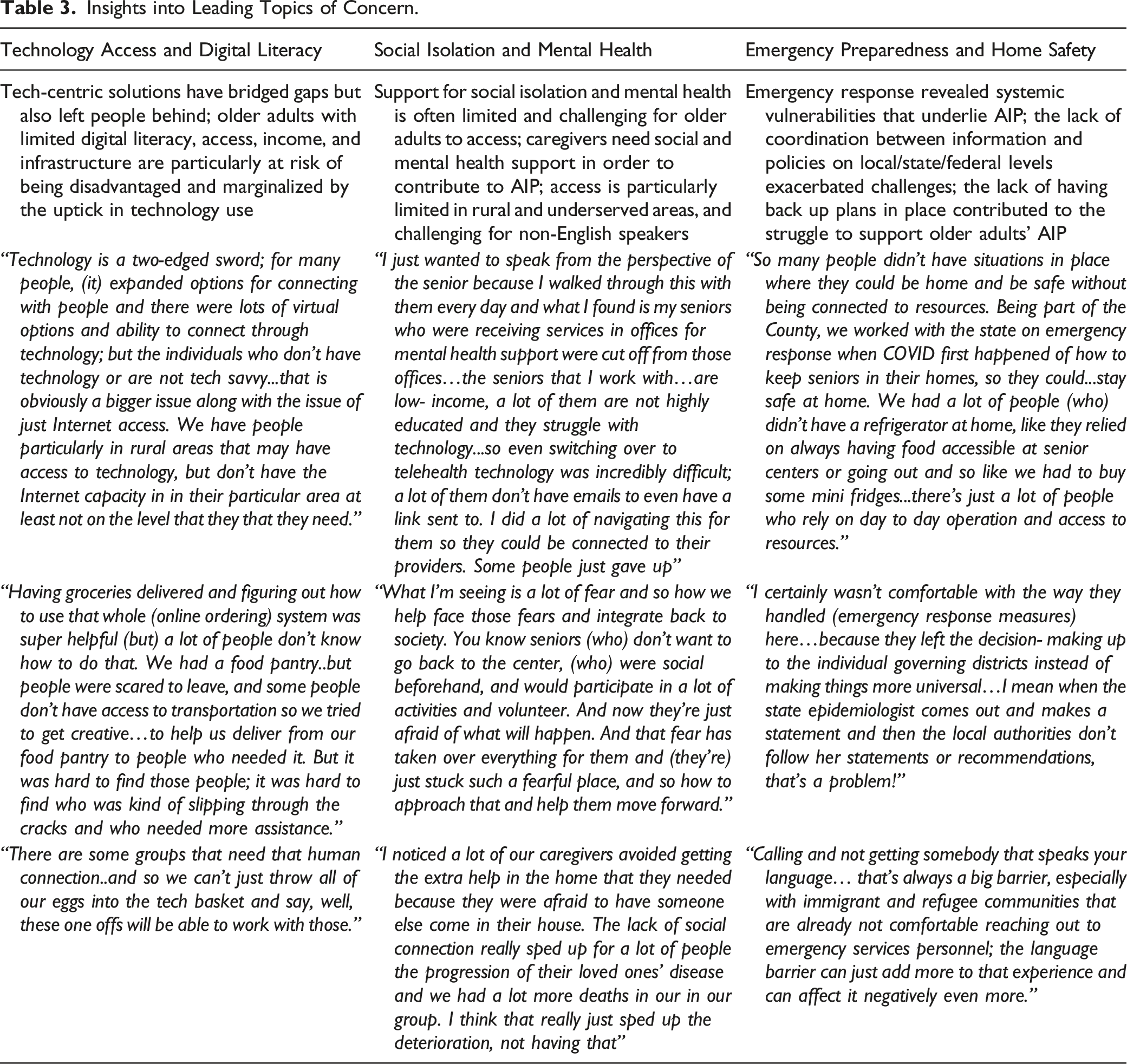
Insights into Leading Topics of Concern.
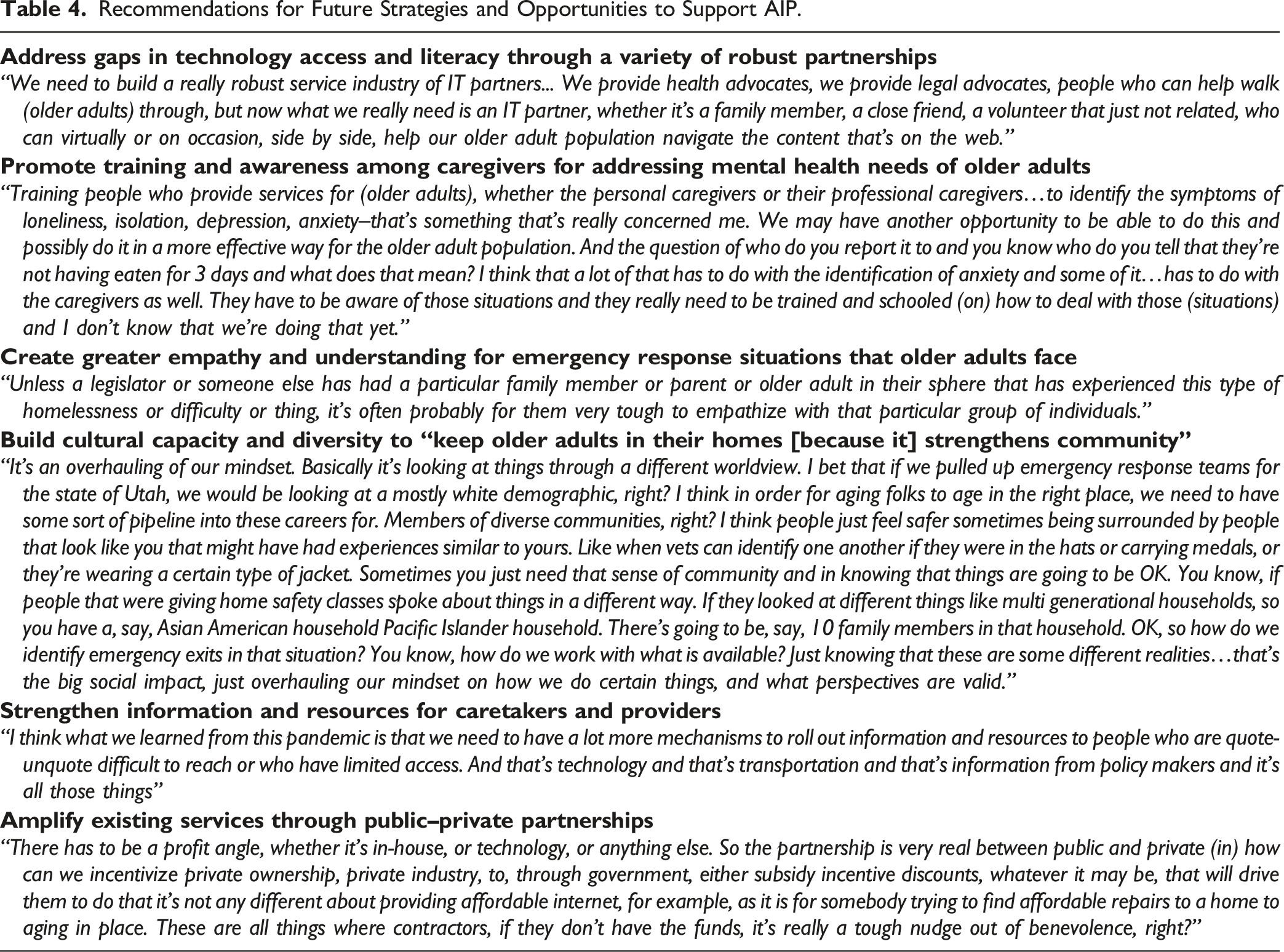
Recommendations for Future Strategies and Opportunities to Support AIP.
Technology and Digital Resources: “A Common Right”
There’s a lot of money going out into infrastructure right now…to build up the infrastructure of the broadband, all of that stuff. But it’s got to be affordable, and some of the programs out there right now are only short-term, like vouchers…to get access. We’ve got to have long-term access that’s really accessible; another great debate and public policy in the future of what is (and) should be a common right, kind of like we argue about health care how much you pay for and how much you should have access to; well, technology, I think is going to fall in that as well—the right to be able to connect the airwaves to get to stuff.—Participant
Increased use of technology was seen to create major advantages and disadvantages to supporting AIP, and participants differentiated between short-term and long-term impacts that the uptick in technology yields in the field of aging services. Advantages include enhanced abilities for caregivers and providers to support older adults’ health through remote monitoring and telehealth platforms. For example, telehealth visits made it more feasible for caregivers to attend doctor’s appointments with their loved ones regularly. Remote working also opened opportunities for providers to close service gaps. In some instances, remote connectivity allowed providers to identify vulnerabilities that might otherwise go unnoticed in home environments of older adults including situations of elder abuse.
However, digital access and literacy were two barriers to technology identified by participants. Concerns over access were described as largely dependent on existing infrastructure and broadband connectivity, which can be limited and unreliable in rural and underserved urban and suburban locations. Physical access to devices was also a concern, particularly for older adults who lack resources to access devices and instead rely upon physical places to use computers, such as libraries (which were shut down during the height of the pandemic response). Digital literacy is another barrier identified by participants; examples given which illustrate challenges brought on suddenly include needing to know how to scan a QR code to make an appointment for a vaccine shot or needing an email address to place an online order for grocery delivery. Gaps in digital literacy and access required service providers to invest an extensive amount of time and resources to address and were viewed as a significant contributor to the unsustainability of supporting AIP for some older adults.
Participants advocated that access and assistance with technology be “a common right” in future planning and policymaking. Creating hybrid service modalities was an integral part of future solutions envisioned to empower older adults, providers, and caregivers with a choice of platforms. Support to translate websites and mobile apps into different languages was identified as a need to make information and services available to non-English-speaking audiences. Participants pointed to the need for ongoing tech support in order to allow older adults, caregivers, and service providers to use technology effectively. Intergenerational opportunities were identified for the potential to help close the “digital divide” that keeps older adults disconnected from digital resources and communities. Measures to protect older adults from online scamming were additionally identified as a rapidly growing need.
Social Isolation and Mental Health: “Making it Personal”
Taking these personal stories of individuals who are struggling and who have been left behind because of the current climate and…making it personal for these policymakers who may not have individuals in their family who are struggling, homeless, and economically disadvantaged, and really facilitating these connections between these policymakers and these older adults so that we can have increased understanding and then have that policy, which is really how we begin to change.—Participant
Participants expressed admiration for the resiliency and innovation that resulted in response to the pandemic, and they shared examples of how outreach initiatives within their communities positively impacted the lives of older adults. For instance, new forms of micro-transit were created for older adults when bus services shut down; new curbside deliveries at libraries and retailers made accessing resources easier for older adults with mobility challenges; longstanding programs such as Meals on Wheels were converted to doorstep deliveries and drive-up deliveries. Senior centers, community centers, and places of worship, which were forced to close social activity programming, were converted to online portals for resources and information which helped bridge disruptions to connectivity.
Yet, participants underscored how the pandemic exposed vulnerabilities to social isolation and mental health. They described how the cancellation of social activities and shutdown of community centers exacerbated isolation for older adults who rely upon community places to maintain social connections and physical fitness; and how anxiety was amplified by mistrust of information, contradictory directives, and divisive political discourse. Participants discussed how frustration and outrage were commonly seen among older adults who felt that response measures took away basic rights, and for whom the sudden shift to a heavy reliance on technology was disorienting and polarizing. Compounding concerns include caregiver burnout, wherein caregivers “simply did not have the bandwidth” to provide additional social support for AIP needs. Participants voiced concerns about how remote working amplified burden on some caregivers. Additionally, there was concern for how isolation made things worse for older adults experiencing elder abuse and living alone with their perpetrators. Participants noted in a spike in the number of non-COVID-related deaths in 2020–2021 among community-dwelling older adults whom they served, which participants attributed to declines in mental and physical health and a failure to thrive.
Participants discussed the need to dismantle social stigmas around mental health and aging and advocated for creating greater awareness around recognizing and addressing symptoms of depression, anxiety, and distress. Training courses designed for service providers and caregivers were seen as necessary long-term solutions to increase knowledge of community-based resources for AIP. Addressing the scarcity of resources to support mental health was another component of short- and long-term needs. Participants emphasized the need to elevate empathy, the quality of care, and social outlets that help sustain mental health and wellness for caregivers as well as older adults.
Emergency Preparedness and In-home Security: “There was no Plan for the Pandemic”
What happens if the caregiver (to an older adult) has an emergency and they have to go to the hospital? Do they have people they can call in to come be with their loved one with dementia? Do they have neighbors nearby? Do they have organizations…walking them through? All these different scenarios…Everyone has these little webs of people and (yet) I think it's hard to think about these scenarios clearly.—Participant
The chain of “what if” scenarios that arise in emergency situations points to the web of caregivers, service providers, and neighbors/friends who play vital roles in supporting AIP. Participants shared myriad examples of how the Coronavirus Aid, Relief, and Economic Security (CARES) Act in 2020 and the American Rescue Plan Act in 2021 made flexible, short-term funding available to local and regional service agencies in the context of emergency response measures, therein allowing providers to respond to specific needs and constraints within communities and populations they serve.
Yet, despite the release of emergency funding, participants acknowledged how fundamentally unprepared organizations were for the scale of response that was required. The struggle to access accurate and consistent information was identified as a destabilizing factor for formal and informal support networks, and the politicized nature of communications at state and federal levels often polarized (rather than unified) response efforts. This was compounded with a struggle that aging-service providers faced when addressing cultural and language barriers, as well as finding the most vulnerable older adults, and meeting the needs of older adults and caregivers in rural communities. A lack of awareness around backup plans at governmental levels challenged the capacity to support AIP. Internally, service providers faced the steep obstacle of pivoting to remote working, providing more services virtually, and equipping staff to work from home. The capacity of caregivers to complement services led by providers was deeply compromised as caregiver burnout took a deep toll on networks that support AIP.
Participants emphasized the need for highly visible emergency management plans at individual, community, state, and federal levels. They advocated for proactive, asset-based community planning that builds additional formal and informal layers of support and incentivizes care coordination. The need for redundancy in backup emergency response measures was identified to address limitations that caregivers and service providers might face. Future needs also include making access to goods and services equitable and home modifications more accessible and affordable for older adults who wish to AIP; addressing gaps created by cultural and language barriers within aging services to ensure that information and resources can be widely accessed; and promoting diversity and pay equity in aging-related service workforce in order to stabilize and strengthen the care aide industry that serves older adults. Funding that supports emergency planning and disaster relief efforts is needed to sustain support networks that have become vital to older adults and their caregivers in the COVID-19 era.
Discussion
Themes from the WC workshops resonate with the literature on roles that aging-service providers play in the context of pandemic response (Hoffman et al., 2020; Karlin et al., 2021). Increased state and federal funding have affected access to services and support for many older adults, yet there is a need to look beyond immediate response measures to assess changes that have the potential to sustain impact, and to address unmet needs that have been exacerbated by the pandemic response (Young et al., 2020). Local-governmental and non-governmental organizations have been at the forefront of creating and implementing changes to services (Angel & Mudrazjia, 2020; Pendergrast, 2021). Findings from this study contribute to knowledge on how AAAs have mobilized to mitigate the impacts of the public health crisis and potential ways to sustain long-term positive impact for older adults (Sands et al., 2022; Wilson et al., 2020).
Technology has created new opportunities for older adults to access community resources during the pandemic (Brooks et al., 2022); however, the pandemic has also exposed dire consequences of the digital divide, or the diminished ability to access technology due to societal and social factors (Ramsetty & Adams, 2020). Gaps in internet access and digital literacy create unique impacts to AIP which shapes the health, financial, and social well-being of older adults (Martins Van Jaarsveld, 2020), all of which directly impact one’s ability to age in place. Internet access has become regarded an essential public service, yet remains unattainable for many households (Lai & Widmar, 2021). Long-term measures are needed to address digital equity, and further research is needed to understand how demographic factors, including age, gender, race, and ethnicity, shape technology use (Campos-Castillo & Laestadius, 2020).
Adverse effects of the pandemic have included increases in loneliness and social isolation among older adults, which present as critical challenges in meeting future needs (Banskota et al., 2020; D'cruz & Banerjee, 2020; Finlay et al., 2021; Weil, 2021). Barriers to services and interventions that target psychological distress in older adults include access to technology and digital literacy (Gorenko et al., 2020). While social connection is a known protective factor for older adults, when social interactions are suspended, isolation becomes an even more significant public health issue (Banskota et al., 2020; Sayin Kasar & Karaman, 2021). Older adults with dementia increasingly developed depressed moods and increased suicidal ideation due to loss of familial contact, social isolation, and confinement during the pandemic (Singh, 2017). The ripple effect of social isolation and delayed treatment for mental and physical health among older adults presents an immediate challenge facing aging-service providers. It reflects a larger need to change societal understandings and policies toward mental health and gain more societal acceptance that equitable access to telehealth technologies and transportation to healthcare providers is necessary for equitable aging.
Discussion of emergency preparedness and in-home safety highlights the critical role aging service providers often play helping older adults make modifications to their everyday living environments, which in turn helps support home as a place of personal and social meaning (Tanner et al., 2008). The impact of home modifications on reducing care needs of community-dwelling older adults is significant (Carnemolla & Bridge, 2019) and essential to reducing safety risks for older adults and prolonging aging in place. Among anticipated home repair and modification work, a recent survey found 71% said their home requires accessibility assists inside and outside, 61% said they need to build an emergency response system in the home, and 48% said they need to implement a smart-home device, such as a voice-activated home assistant (Davis, 2021). Barriers that limit the capacity to make home modifications include rising costs of building materials and limited availability of labor (McGarry & Falvey, 2021). The need to have emergency response plans in place, particularly for older adults with increasingly complex health and mobility needs, is integral to community caregiving, health promotion, and disease prevention (Mazumder et al., 2020). Challenges to serving rural, indigent, non-English speaking and ethnic minority older adults were highlighted as a critical vulnerability and emergent need to address through experiences of AAA response efforts in the United States (Fang, 2022).
The issue of support for caregiving was significant within the focus on technology, mental health, and emergency preparedness in this study, pointing to a need for greater attention and support for caregivers within pandemic response efforts (Cohen et al., 2021). Informal networks of caregivers are a critical component to support AIP among older adults who have been globally impacted because of the pandemic (Tur-Sinai et al., 2021). One-in-five Americans provides unpaid care to an adult with health or functional needs; almost 1-in-4 Americans cares for more than one person; and nearly 1-in-5 American caregivers is aged 65+ (AARP and National Alliance for Caregiving, 2020). As the COVID-19 pandemic has progressed, caregivers have reported feeling prepared to provide services for older adults compared to the beginning of the pandemic (Karlin et al., 2021). Caregivers experience high-stress levels due to government regulations, staff shortages, virtual service delivery, transitions to telemedicine, increased workload, and high demand for professional services (Karlin et al., 2021). Additionally, family caregivers often have less training compared to a professional caregiver and may have more limitations to visiting older adults for fear of spreading the virus (Karlin et al., 2021; Lebrasseur et al., 2021).
There were several limitations to this study. First, the WC workshops were conducted in 2021 when the second major wave of the pandemic was subsiding, and the experiences shared by aging-service providers reflect a distinct moment in time. Second, though our findings are strengthened in that participants represented a broad range of aging services (including transportation, health, and social services), participants generally held leadership roles within their organizations, which influence their perspectives and experiences. Third, recruitment was reliant on a university-maintained database which may represent only a portion of aging-service providers in the Salt Lake metropolitan region. Nevertheless, our sample size was an adequate number for the WC method.
Conclusion
This study identified concerns and needs to support AIP that aging-service providers uniquely experienced during the pandemic. The marginalization of older adults during the pandemic has been termed “an invisible human rights crisis” due to the physiological and psychosocial impacts of the pandemic on older adults (D'cruz & Banerjee, 2020). Changes in aging services that were made in response to the pandemic have potential for sustained impact addressing this crisis, yet there is a need to understand gaps and challenges in order to inform future efforts. Engaging aging-service providers with research evidence is necessary to guide future planning and policymaking efforts. Innovative partnerships and response measures that were largely catalyzed by emergency federal funding including the CARES Act, the American Recovery Act, and the freeing of Older Americans Act (OAA) funds require longer-term funding and holistic community response initiatives. As the number of Americans ages 65 and older will be more than double in the next four decades, areas of need to support AIP will only become more pressing.
Supplemental Material
Supplemental Material - Aging in Place Through the COVID-19 Pandemic: Perspectives from Aging Service Providers
Supplemental Material for Aging in Place Through the COVID-19 Pandemic: Perspectives from Aging Service Providers by Valerie Greer, Sarah L. Canham, Andy Hong, James Agutter, Ivis Garcia Zambrana, and Jess M. Van Natter in the Journal of Applied Gerontology.
Footnotes
Authors’ Note
IRB_00141945, Institutional Review Board, University of Utah.
Acknowledgments
We respectfully acknowledge that the University of Utah is located on the traditional and ancestral homeland of the Shoshone, Paiute, Goshute, and Ute Tribes. For contributions to this project, we would like to acknowledge research assistants Natalie Caylor, Kimberly Beck, Alannah Clay, and Timothy Gould. We would also like to thank our partner organizations for their support of this project and the invaluable insight of study participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was made possible by the Research Incentive Seed Grant Program, sponsored by the Vice President for Research at the University of Utah (51900493).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.