
Abstract
• This paper provides valuable insights into the psychological burdens and long-term care (LTC)-specific challenges experienced by healthcare workers (HCWs) during the pandemic. • In addition to COVID-19-related stressors, LTC workers are especially vulnerable during the pandemic due to systemic and intersectional inequalities. • Despite many challenges and pressures, some HCWs reported immense satisfaction and pride in caring for LTC residents during the pandemic.
• Finding from this study can inform best practices and development of mental health policies to support HCWs, as well as address intersectional inequalities within the LTC sector. • Programs to reward, encourage, and build resilience among HCWs in LTC should be expanded to mitigate the multi-faceted impacts of the COVID-19 pandemic. • Occupational supports in LTC settings should address staffing and ongoing systematic challenges that disproportionately harm some HCWs over others.What this paper adds
Applications of study findings
Introduction
The COVID-19 pandemic has severely disadvantaged many groups, including older adults and those living in long-term care (LTC) homes. Across the Organization for Economic Co-operation and Development (OECD) countries, 93% of COVID-19 deaths were among those age 60 or older (OECD, 2021). Amongst 16 other OECD countries, Canada reported the highest proportion of all COVID-19-related deaths (∼81%) among LTC residents during the initial wave of the pandemic (Canadian Institute for Health Information [CIHI], 2020; Comas-Herrera et al., 2020). In Canada, the profound impact of the pandemic in the LTC sector was attributed to pre-existing deficiencies including economic and operational difficulties (Estabrooks et al., 2020). Pre-pandemic, LTC homes in many countries, including the United States (US), Canada, Germany, Spain, United Kingdom (UK), and Denmark, were plagued for decades by underfunding, overcrowding, inadequate facilities, and a lack of appropriate regulation and oversight (Bourgeault et al., 2010; Estabrooks et al., 2015; Langins et al., 2020). Moreover, limited resources (human and non-human) including long-standing staffing shortages in the LTC sector have resulted in an increased use of part-time and casual workers and workers holding multiple jobs. Since the pandemic, staffing shortages have worsened with over 86% of LTC homes in Canada reporting at least one staffing related challenge in 2020, and a 71–77% increase in overtime hours and absenteeism in the sector (Clarke, 2021). In addition to the staffing inadequacies, many Canadian LTC homes face existing infrastructure challenges, including older buildings, poor technology and lack modern resources that are necessary to deliver quality resident care (Langins et al., 2020). In many cases, the facility size, design, and age of LTC homes, including shared rooms, narrower hallways and limited space for social gatherings, make physical distancing and segregation of infected residents and other safety measures difficult to implement (Estabrooks et al., 2020), thus enabling easier transmission of the virus (Applegate & Ouslander, 2020).
Emerging evidence (Fisher et al., 2021; Kang et al., 2020) suggests that the unpreparedness of health systems to tackle the pandemic and worsening LTC conditions across many of the OECD countries have severely impacted the health and well-being of healthcare workers (HCWs) (e.g., care aides, nurses, physicians, social workers), as many report high stress and mental problems such as anxiety, panic attacks, and depressive symptoms. A Canadian longitudinal study found the prevalence of anxiety and depression had increased by 10%–15% among nurses in all healthcare sectors during COVID-19 compared to pre-pandemic; cross-sector analysis, however, showed the largest increase in these mental health symptoms were experienced by nurses in LTC (Havaei et al., 2021). Similarly, a 2020 study from the US reported that 50% of LTC workers are at increased risk of severe illness from COVID-19, including hospitalization and death (Gibson & Greene, 2020). Although HCWs in all sectors faced tremendous stress during the pandemic, HCWs in LTC encounter additional challenges and stressors, such as job insecurity, chronic low pay, temporary and part-time work compared to their counterparts in other sectors (International Labour Organization, 2018; Osman, 2020). On average, across the OECD countries, women hold about 90% of the jobs in the LTC sector, and earn significantly less than half the national median annual earnings (OECD, 2021). In Canada, unregulated care providers (73%), immigrant and racialized women are overrepresented among care workers in LTC (Estabrooks et al., 2015)—a group that has been especially vulnerable during the pandemic due to systemic and intersectional inequalities (Lightman, 2022). The unstable and precarious nature of employment in the LTC workforce (e.g., part-time, under-paid) requires critical attention.
Throughout the pandemic, LTC homes have been in the media spotlight, eliciting much needed and long overdue discussions on potential redesign of the sector (Estabrooks et al., 2020). While there are emerging studies recounting the experiences and mental health concerns of general HCWs (Gialeb et al., 2022; Muller et al., 2020), only a few have focused on the experiences of HCWs in LTC. Despite the critical role that LTC workers continue to play in supporting the needs of residents and their families, little is known about the psychological and mental health impact of COVID-19 on this precarious workforce. This review aims to synthesize the available evidence on the experiences of HCWs in LTC during the COVID-19 pandemic to shed light on their unique challenges, and effective strategies for improving HCWs’ mental wellbeing during and post-pandemic. The study findings will shed light on the global LTC workforce, resident care outcomes, and offer strategies to support this vulnerable healthcare sector.
The Review
Aim
The aim of this scoping review was to synthesize the evidence pertaining to the experiences of HCWs in LTC during the COVID-19 pandemic.
Research Question
The review sought to answer the following research question: What are the experiences of HCWs in LTC during the COVID-19 pandemic?
Methods
Study Design
This scoping review was guided by the five stages described in Arksey and O’Malley’s (2005) framework, with recommendations from Levac et al. (2010) for advancing the methodology of scoping reviews. This methodology was chosen due to its capacity to support knowledge synthesis pertaining to an exploratory research question, various types of evidence, and gaps in a research field area (Levac et al., 2010). The scoping review results were reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) guidelines (Page et al., 2021).
Data Sources
In consultation with an experienced health sciences librarian trained in conducting systematic reviews, an appropriate search strategy was developed, revised, and updated for the following databases: CIHNAL, AgeLine, PsycINFO, MEDLINE, OVID, and Google Scholar. The search strategy, including an eligibility checklist, was developed to identify studies on HCWs in LTC.
Eligibility Criteria
Inclusion criteria required results to be peer-reviewed empirical research studies published in English between March 1, 2020, and June 1, 2022, with no restrictions in terms of country, thus establishing a broad review of the literature on LTC HCWs’ experiences during the COVID-19 pandemic (see Supplementary Table 1). Qualitative, quantitative, and mixed method studies were included. Review studies, commentaries, and policy reports/briefs were excluded.
Search Strategy
A systematic and comprehensive search strategy was created using the medical subject heading (MeSH) for relevant studies that met the inclusion criteria. Under supervision of the project lead (SB), two of the study authors (AI and AH) independently searched the computerized databases using the finalized string of search terms and combined Boolean key search terms such as, “COVID-19,” “novel coronavirus 2019,” “SARS-CoV-2,” “health care worker,” “mental health,” “nurse,” and “long-term care” (see Supplementary Table 2). Search terms were adapted to each databases search format (e.g., separating the sting of phrases into different search boxes separated by “AND”). The reference lists of all relevant articles and “related citations” were hand-searched for additional articles and studies not identified in our original search. All potentially relevant studies were scrutinized against pre-specified inclusion criteria to confirm eligibility in and contribution to our study.
Study Selection and Abstraction
The study selection was an iterative process involving three interrelated steps: (1) title and abstract reviews, (2) full-article reviews, and (3) reviewers’ examination of reference lists from full articles to identify articles for possible inclusion. The authors used Covidence online software (https://www.covidence.org/), the standard platform for Cochrane Reviews, to manage study selection. Initially, 25,708 articles were identified using the search design and inclusion criteria, of which, 21,900 duplicates were removed, yielding a total of 3808 articles. Each of the team members independently screened/scrutinized the titles and abstracts against the selection criteria and indicate “Yes” or “No” whether to be included or excluded. Ambiguities and disparities were discussed and resolved with a third reviewer. Abstracts that met the eligibility criteria automatically moved to the full text review list in Covidence for the research team to perform a complete review of the articles (n = 192). Once all titles and abstracts were reviewed twice and all discrepancies arbitrated during regular bi-weekly Zoom meetings, the research team performed full-text reviews of the resulting 74 articles. In the second phase of study selection, each team member was randomly assigned a set of articles for full-text review using the same inclusion and exclusion criteria––approximately 18 articles per reviewer. The third and final phase involved examining (i.e., hand searching) the reference lists of included articles for additional pertinent studies that were not previously identified, resulting in a total of 40 articles for review (see Figure 1). PRISMA flow diagram of literature search and screen process (Page et al., 2021). 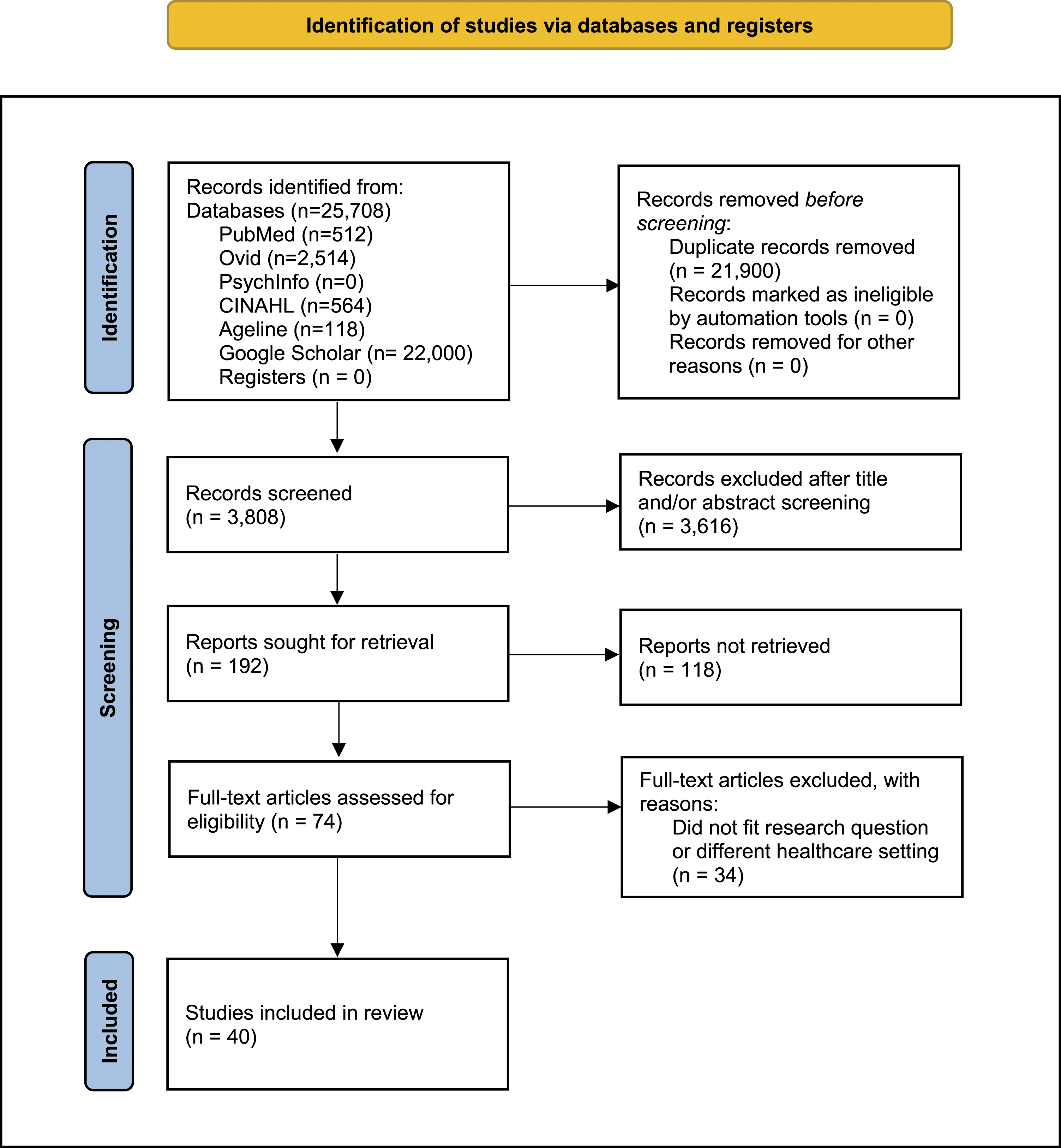
Data Extraction
Article Summary.

Synthesis
Given the emergence of the COVID-19 literature and the limited number of relevant articles, no meta-analysis or formal assessment of the methodological quality or appraisal of individual studies was performed and/or explored in depth. Because of the broad nature of scoping reviews, no rating of quality or level of evidence is provided, thus recommendations for practice cannot be graded (Joanna Briggs Institute, 2016). However, each stage of the Arksey and O’Malley’s (2005) framework provides both clarity and rigor of the review process. The analysis was conveyed in prose to outline and explain the results, which allowed key concepts from the research questions to be used as the initial coding categories (Hsieh & Shannon, 2005). The findings from the included studies were synthesized into thematic groups using thematic content analysis.
Findings
The initial search strategy identified 25,708 records, of which 40 studies were included in the final review, consisting of 18 (45%) qualitative studies, 14 (35%) quantitative studies, and 8 (20%) mixed-method studies (see Table 1). Most of the publications were from Europe (e.g., Spain, Netherlands, UK) and North America. Figure 1 displays the PRISMA Flow Diagram summarizing the literature search and the screening process used to identify studies for inclusion in this review.
Thematic analysis
To synthesize the core concepts underpinning the scoping review, findings were categorized/organized according to three interrelated themes pertinent to our study aims, while recognizing that experiences/emotions are rarely discrete categories: (i) carrying the load; (ii) building pressure and burning out; and (iii) working through it. The themes were named based on the data extraction and discussion within the research team.
Carrying the Load
Carrying the load refers to the cognitive, socio-emotional, and psychological burden carried by HCWs throughout the pandemic and the impact on their health and wellbeing. This burden, or “emotional load” (Dohmen et al., 2022), was directly linked to work-related demands and tremendous responsibilities placed on HCWs in the LTC sector. Twenty-five of the 40 studies reported negative emotions and internal struggles that diverse groups of LTC workers (i.e., care aides, nurses, physicians) experienced in caring for infected and dying residents. Some of the emotions described include a deep sense of sadness, helplessness, anger, frustration, discomfort, and fatigue caused by high-intensity work and concerns for residents’ safety as many were dying from COVID-19, and what HCWs felt could have been preventable. Many of the workers reported psychological consequences of working in LTC such as uncertainty and fear and described how witnessing suffering and preventable deaths illuminated both “their individual devaluation as low-paid formal caregivers, and that of their aging residents, by the larger society” (Freidus & Shenk, 2020, p. 206). One care home staff in the US described a sense of helplessness and frustration as they witnessed immerse grief by stating: “they’re literally smothering to death; they’re literally choking to death. And all you can do is sit there and hold their hand and try to make them comfortable... This possibly could have been prevented” (Freidus & Shenk, 2020, p. 204).
The effects of carrying this emotional burden and feelings of guilt often led to “internal conflict” and “moral distress” for HCWs (Dohmen et al., 2022). Most HCWs conveyed a deep-seated grief, anxiety, and concern for the quality of life of residents as many deteriorated. One Maltese nurse expressed that “[h]er emotional turmoil was associated with moral distress of not being able ‘to be a nurse’ in the current circumstances” (Scerri et al., 2022, p.6) as a result of COVID-19 mitigation measures. These statements reflected HCWs’ concerns regarding the precautionary measures that were put into place to ensure physical distancing, in particular the ban of visitors and the psychological toll on both residents and caregivers. To cope with the pandemic-induced stressors, HCWs adopted various strategies, including seeking support/guidance from peers and leadership, which they felt was integral to their wellbeing. A study of 720 Portuguese LTC staff identified teamwork (78%), and staff training (70%) as key strategies to ensure staff wellbeing and a safety culture (Brito Fernandes et al., 2021).
Building Pressure and Burning Out
Building pressure and burning out refers to the chronic emotional and interpersonal stressors that HCWs experienced as job demands rose. Twenty of the 40 studies reported various symptoms associated with staff burnout, which are categorized as: physical (chronic fatigue, extreme exhaustion), emotional (fear, anger, frustration), cognitive (mental fatigue, difficulty in making decisions), and behavioral (cynicism, negativism). More profoundly, there were reports of increase in burnout syndromes, especially intensified emotional exhaustion and lack of personal accomplishment (Krzyzaniak et al., 2021; van Dijk et al., 2022), resulting in job dissatisfaction and high turnover. One British care home staff said, “I burned out in the end. [...] In hindsight, it was so draining because it was constant. And it was constant fear, and I think fear is the just the worst thing, the fear from getting ill and my actions making someone ill—or my lack of actions, I should say. That’s a horrible thought to have” (Bunn et al., 2021, p. 395). In other instances, staff including carers and managers were “overburdened and burned out” and experienced “emotional upset” (Giebel et al., 2022, p. 10) when working with dying patients/residents. In fact, a national study of aged care facility workers in Australia found that 33% of respondents suffered from burnout during the pandemic (Krzyzaniak et al., 2021), underscoring the immense impact of COVID-19 on the mental well-being of LTC workers.
In all the studies reviewed, HCWs reported feeling physically and emotionally exhausted due to longer workdays and unmanageable workloads associated with a constantly changing environment, monitoring and documentation processes, screening staff and visitors, and providing additional communication and support to residents and their families. In a sample of 1669 Dutch nursing home staff, 19.1% reported high levels of depressive symptoms and 22.2% burnout (van Dijk et al., 2022). Another study with Spanish nursing home workers (n = 335), found that social pressure from work and emotional exhaustion were negatively related to their professional satisfaction (r = −0.14, p < 0.05; r = −0.42, p < 0.01, respectively), while contact with death and suffering and social support at work were positively related to professional satisfaction (r = 0.20, p < 0.01; r = 0.25, p < 0.01, respectively) (Blanco-Donoso et al., 2021). LTC workers also expressed mental exhaustion, as one Austrian carer stated, “I was at home and really started to cry. Because my nerves just felt like they could not take anymore. Hopefully it’s over soon, because otherwise I’ll break” (Hoedl et al., 2022, p. 6). In referencing the long-standing deficiencies that existed within the LTC sector pre-and during the COVID-19 pandemic, one HCW noted that “we and all the patients are the victims of politicians. I barely worked and lived before the coronavirus, but now I’m a zombie” (Leskovic et al., 2020, p. 668).
In addition to burnout, HCWs reported experiencing mental health conditions including generalized anxiety disorder and post-traumatic stress disorder (PTSD) related to the ongoing exposure to the traumatic events and in performing day-to-day tasks. One nurse in a US study was quoted stating: “I have PTSD... Going through this trauma, I’m still trying to come out of it.... I say that I don’t think I mentally could do it, but I sit here, and I tell myself, like I just told you, if I had to do it, I would do it again...” (Freidus & Shenk, 2020, p. 205). This statement reflects the ongoing stressors that HCWs continue to face since the emergence of the pandemic. An Italian study found that HCWs, especially women, who had recently been in contact with COVID-19-positive patients or colleagues were more likely to report moderate-to-severe symptoms of anxiety (22%) and PTSD (40%) (Riello et al., 2020). Similarly, in a sample of 390 Irish nursing home staff, 38.7% reported a WHO-5 score ≤32, indicating significantly low mood and poor wellbeing, and 13.8% reported suicidal ideation and suicide planning (Brady et al., 2022). Excessively high levels of mental and emotional exhaustion were consistently reported by HCWs in almost all the articles (Blanco-Donoso et al., 2021; Corpora et al., 2021; Prados et al., 2022). Participants emphasized that they did their best to offer quality care to residents while working under exceptionally challenging circumstances. While most of the articles reported increased burnout and dissatisfaction with the LTC work environment, none explicated mentioned high staff turnover. A study of German managers in LTC facilities (n = 833), however, found a significant association between the perceived pandemic-specific and general demands and intention to leave the profession (Pförtner et al., 2021). Overall, all the articles stressed the importance of supportive work environments.
Working Through It
Working through it represents that structural and systemic barriers and challenges that exists within the LTC sector that HCWs constantly had to overcome in caring for residents throughout the pandemic. Twenty-two of the 40 studies reported HCWs’ concerns about the LTC work environment including the facility size, design, and/or age of the home (e.g., narrowing hallways, shared accommodations), short-staffing, lack of preparedness and safety, availability/lack of job resources such as personal protective equipment (PPE) (Blanco-Donoso et al., 2020; Tomaszewska et al., 2022). Many studies commented on how the pandemic has worsened the already precarious working conditions in LTC pre-COVID-19 including the lack of social, economic, and professional recognition of LTC workers compared to their counterparts in other sectors.
HCWs also expressed fear of contagion (contracting the virus) and of infecting their loved ones when working under conditions of extensive contact with suffering and death of residents. The fear of getting infected and infecting others was a primary cause of concern shared among HCWs of all job types. In a multi-national study conducted in Spain, Italy, Peru, and Mexico, a geriatric nurse stated, “Ofcourse I am afraid, I am terrified to think that I have it without knowing, and that I am infecting the residents ... and that is very scary” (Sarabia-Cobo et al., 2021, p. 872). Due to short staffing, many HCWs felt a sense of obligation to return to work even if their own lives were at risk as one UK care staff noted, “I’ve had so many people say to me in my personal life, ‘I’m still going to work even if I test positive’ because I can’t afford not to work” (Bunn et al., 2021, p. 394). The stigma associated with contracting and transmitting the virus caused many HCWs to withdraw from friends and family leading to increased loneliness and social isolation. A certified nursing assistant in a study of American staff summed up the duality of the fear by stating: “You’re not only worried about yourself and your residents, but you’re worried about bringing it home as well” (Snyder et al., 2021, p. 6). While HCWs continue to risk their lives to care after patients, some felt attacked for upholding the COVID-19-related infection control policies/practices. In an Australian study, 43% of aged-care facility workers reported unfair or abusive treatment by family or friends of residents (Krzyzaniak et al., 2021). Many HCWs felt that they were being blamed for “bringing in the virus to the LTC site from their community” (Lightman, 2022, p. 7)—sentiments that some HCWs felt were prejudicial and discriminatory because of their race/ethnicity, further highlighting the widespread racial and social inequalities that LTC workers experienced at work.
Support and recognition were commonly cited as important factors in motivating HCWs especially during the pandemic (Giebel et al., 2022; Lethin et al., 2021; Lightman, 2022; Nyashanu et al., 2022). Many workers reported a sense of disappointment, felt undervalued, and unrecognized even though they were doing their best to adapt to the evolving crisis. One Canadian care home staff said, “You are my hero! You are doing essential work, blah blah blah’, you know guys, what about money? We didn’t get enough to be secure, you know” (Lightman, 2022, p. 6). HCWs felt that they were not being appreciated for their contributions. In a multi-country qualitative study of geriatric nurses, one Spanish health worker described a sense of under-appreciation stating: “Governments have failed...there has been no foresight, we are abandoned, exhausted...we fight alone” (Sarabia-Cobo et al., 2021, p. 873). Similar sentiment was expressed by care home staff and family carers in the UK, as one person was quoted saying, “I’m a bit angry with the government really and in another way, I can see that they’ve got to keep everybody safe” (Giebel et al., 2022, p. 6). In another study, a nurse in Slovenian nursing home was quoted saying that; “The politicians have sacrificed us. We will totally burnout and the elderly will die due to COVID-19. We are worth nothing to them!” (Leskovic et al., 2020, p. 668). The sense of despair and disappointment was also attributed to the lack of recognition for their contribution in the healthcare system compared to their counterparts in hospitals (Nyashanu et al., 2022), no designated time off, and delays in receiving PPE and testing at the peak of the pandemic.
Despite the enormous burden of distress and potentially traumatic events experienced by HCWs in LTC homes, some studies (Blanco-Donoso et al., 2021; Dohmen et al., 2022) highlighted the positive feelings experienced by HCWs including a sense of duty and commitment to care and gratification and fulfillment working during the crisis and how their work contributed to the greater good of society. For instance, participants reported feelings of pride, satisfaction in helping others (Hung et al., 2022) and professional fulfillment in providing care to residents during the pandemic. HCWs who had more social support at work experienced higher levels of professional satisfaction despite the demanding work conditions.
Discussion
This paper presents the results of a scoping review examining the experiences of HCWs in LTCs during the COVID-19 pandemic. While emerging research during the pandemic has considered the experiences of HCWs broadly, a relatively smaller body of evidence has focused on the experiences of those working in LTC––a sector that has been greatly impacted by the pandemic (Ghaleb et al., 2021). Thematic findings from this review highlight the unique challenges and burdens experienced by HCWs in LTC across many job types (e.g., care aides, nurses, physicians, social workers, managers) and in different countries including the US, Canada, UK, Spain, and Italy (Di Mattei et al., 2021; Rabow et al., 2021), and points to areas for future practice and research.
Findings of this review indicate that the psychological and emotional burden experienced by HCWs related to the COVID-19 pandemic are directly linked to structural and environmental factors within the LTC sector (Boamah et al., 2021a). In particular, the unpreparedness of this sector, rapid spread of the COVID-19 virus/illness, the high rate of resident mortality, and concerns about physical distancing measures and other COVID-19-related policies created moral distress and immerse pressure for front-line staff (CIHI, 2020; Comas-Herrera et al., 2020), and increased loneliness and social isolation for residents and their families (Boamah et al., 2021b). These findings align with emerging research from various countries including Italy (Di Mattei et al., 2021) and the US (Rabow et al., 2021), which have documented widespread grief, anger, and mental distress experienced by HCWs.
Our findings suggest a need for LTC-specific strategies to improve the health and wellbeing of front-line staff. Promoting positive mental health and coping through supportive workplace environments will not only benefit HCWs, but also improve the quality of care and life of residents and their family caregivers (Boamah et al., 2021b). Strategies that could be employed include expanded sick leave and mental health policies for HCWs that promote psycho-emotional and physical health. While so-called “mental health days” among HCWs have been documented in countries such as Australia (Lamont et al., 2017), they do not appear to be widely available or documented across other jurisdictions. There also remain significant barriers and stigma associated with taking time off for mental––rather than physical––health reasons. Given the impact of COVID-19 on both HCW wellbeing and patient care, there is an urgent need to evaluate best practices for supporting HCWs exposed to workplace-related stressors, while considering factors that might predispose workers to severe burnout and turnover.
Results of this review indicate that HCWs in LTC settings particularly geriatric nurses (Sarabia-Cobo et al., 2021) and other care staff (Leskovic et al., 2020) experienced high stress, anxiety, and depression, which heightens their risk of burnout. This finding is noteworthy given the mounting evidence including systematic reviews linking COVID-19 to poor patient care and burnout among HCWs in other sectors (Al Maqbali et al., 2021; Pappa et al., 2020). As such, policymakers and LTC leaders must provide essential resources for workers (e.g., PPE, virus testing policies), adopt strategies to support mental health concerns (e.g., counseling, employee assistance programs) and daily needs of staff outside of work (e.g., childcare), and improve crisis leadership skills (Wu et al., 2020). Other strategies could include evaluating COVID-19 responses within organizations and HCWs’ first-hand perspectives, which can inform the refinement of best practices whilst simultaneously curbing future harm amongst HCWs (Stelnicki et al., 2020). Furthermore, lessons learned from the pandemic can aid in structuring better staffing and workload management tools to improve staff work experiences (Udod et al., 2021).
Despite the challenges and hardships experienced by LTC workers during the pandemic, our findings suggest that their care work has been at times rewarding. These experiences suggest that not all pandemic-related experiences in LTC have been negative. This finding is thought to align with emerging COVID-19 research. For example, a recent study (Ke et al., 2021) of nurses working in hospitals in Wuhan, China found that most front-line nurses maintained a strong commitment to their work throughout the pandemic. Future research and practice should, therefore, consider means of acknowledging and rewarding HCWs for their ongoing work while building resilience among staff as the pandemic continues. These factors can serve to protect HCWs from burnout and other harmful secondary outcomes related to COVID-19 (Baskin & Bartlett, 2021). Further, in the context of LTC, there is growing work precarity and social marginalization as well as worsening of workplace inequalities and intersectional racism. The results of this review confirmed that research must address intersectional inequalities within LTC to better support HCWs during and post-pandemic (Lightman, 2022). As such, every effort must be made to prioritize principles of cultural safety and eradicate systemic barriers that exacerbate mental distress among HCWs and hinder quality of resident care.
Strengths and Limitations
This scoping review has several overarching strengths. The studies included were published in 12 countries, suggesting that the results are not country or region-specific. In other words, while LTC policies and structures may differ across countries, the experiences and challenges faced by HCWs in the included studies (i.e., stress, burnout, fear) were consistent across diverse geographical regions/locations. Only studies published in the US, Canada, and Australia reported significant fears and anxiety among HCWs linked to PPE shortages, indicating possible differences in contagion preparedness levels and supply chain effects across different regional and/or national LTC systems. With this in mind, future studies should examine whether trends in HCW experiences differ across countries that operate exclusively public LTC homes versus countries that offer a mix of public and private LTC services. As well, more studies are needed to identify possible contextual and occupational factors that may shape or mediate long-term impacts of the pandemic.
This scoping review was limited by the fact that studies not yet published (after June 2022) or translated in English have been missed and/or excluded. Also, detailed findings are not compared across worker type/role (e.g., nurses, care aides) as many studies included in this review did not often specify how the results differed by role. In line with scoping studies, the quality of evidence identified was not explored in-depth. Despite this, we are confident that the findings are meaningful, widely applicable given the various regions represented among included studies and offer valuable insight into the impacts of COVID-19 to date and lay the foundation for studies of long-term effects in the future.
Implications
Our exploration of literature identified a multitude of workplace factors which impact HCWs’ job performance and wellbeing, and addressed a crucial knowledge gap in the growing body of COVID-19-related research. Going forward, researchers, practitioners, and decision-makers are urged to consider means of supporting HCWs in LTC in order to promote their wellbeing, and those of their care recipients. Future research into HCW supports must consider: (1) how existing workplace supports have fallen short in the context of COVID-19; (2) how and to what extent current promising approaches at various levels (e.g., directed funding mechanisms, wellness coaching) can be administered in additional settings/contexts; and (3) how specific sub-groups of HCWs in LTC (e.g., racialized women) can be empowered and protected from disproportionate burden. The psycho-emotional and social health of HWCs must be both protected and supported through critical enhancements to the LTC sector. Findings from this review can inform future research agenda to highlight gaps in knowledge regarding the long-term and system-wide impacts of the pandemic on LTC staff and residents. Additionally, studies should consider investigating how COVID-19 may have affected HCWs during co-occurring climate-related disasters such as hurricanes and wildfires and the additional strain they placed on the already unstable healthcare systems. In doing so, researchers can develop context-specific strategies and interventions to strengthen health systems across the globe.
Our findings also point to areas for improvement within and beyond the LTC context to support HCWs and residents/patients alike. Several regions have begun to implement promising strategies in response to the growing need for expanded HCW supports. For example, an innovative program in the US trained advanced nursing students to provide one-on-one wellness support to nurses working in a COVID-19 hotspot via wellness coaching sessions with coaching support focused on eating, sleep, stress, and physical activity guidance (Teall & Melnyk, 2021). Program results show immense promise as 94.7% of participating nurses felt the program contributed to improved mental and physical health (Teall & Melnyk, 2021). Given the findings from this review, exceptional measures must be in place to retain LTC workers. In Canada, US, and other countries, the federal government has implemented programs such as, the new Recruitment and Retention Incentive Programs, to attract and retain skilled HCWs to LTC homes with the highest level of staffing need to help safeguard the health of residents and their families. In terms of improved support for compensation and benefits, so-called “pass-through” or “directed payment” programs (Feng et al., 2010), and more recently, the “Patriot Pay” plan, a temporary bonus or increase in hourly wage, have been implemented in several US states since the COVID-19 pandemic to ensure that essential workers receive high compensation than the unemployment insurance rate (Romney, 2020). These funding mechanisms not only reduces the incentive for second job holding and turnover but are essential for minimizing the spread of the virus thus ensuring safety of residents and better outcomes (Loomer et al., 2022). Given these promising approaches, policymakers and LTC administrators are urged to consider additional means of supporting staff through such creative and innovative programs.
Additional recommendations for supporting HCWs during and post-COVID-19 include creating safe and healthy work environments for staff and providing appropriate recognition (e.g., reward system, flexible working hours) to show appreciation for the significant role and contributions that HCWs make to the healthcare system, and in doing so, foster resilience among workers and increase organizational commitment (Greenberg, 2020). Protecting the psychological and mental health of HCWs should be of outmost importance for all health care leaders and organization. Health care administrators and leaders are urged to provide specialist counseling services for HCWs to ensure that trauma and strain linked to work do not manifest into long-term psychological impacts (Brophy et al., 2021). The vast scientific literature on psychological trauma, exposure, and consequences during the COVID-19 pandemic shows that some individuals, including those from racialized and immigrant groups are at even higher risk of experiencing psychological distress and adverse outcomes (Greenberg, 2020). Yet, only few studies have focused on specific psychological support intervention programs for HCWs despite the WHO’s urgent call for tailored and culturally sensitive mental health interventions and psychological support programs for HCWs (Holmes et al., 2020). With the awareness of a growing work precarity, social marginalization, and worsening of workplace inequalities and intersectional racism in healthcare as highlighted in this review, LTC leaders and administrators should pay particular attention to HCWs in high-risk groups. Moreover, policymakers and leaders must recognize potential psychological difficulties some workers may face and implement “return to normal work” interviews as an approach to ensure HCWs’ mental health and identify the presence of pertinent stressors (e.g., bereavement or burnout), which can help reduce absenteeism rates and staff shortages (Greenberg, 2020). Other innovative strategies to support HCWs could include digital approaches such as remote psychological first aid (PFA) and online platforms or learning packages where experts with direct pandemic experiences from the front-line provide advice and evidence-based mental health guidance to other HCWs, including self-care strategies (e.g., shift work, breaks, healthy lifestyle behaviors), and managing emotions/coping (e.g., anxiety, moral injury) (Blake et al., 2020). Studies in the UK and Malaysia (Blake et al., 2020; Sulaiman et al., 2020) have shown the PFA protocol to be an effective method of assessing the psychological impacts of COVID-19 remotely via mobile application and phone calls, and can help people in distress and support them to cope well with their psychological, emotional, and social needs/challenges. Given the immense pressure faced by HCWs and LTC facilities during this time, significant improvements are unlikely to take place without strong leadership and meaningful improvements to working conditions.
Conclusion
This paper shed light on the immense pressure that HCWs globally faced during the height of the COVID-19 pandemic and the tremendous impact on their mental and physical health and wellbeing. The findings also highlighted the extreme vulnerabilities within the LTC sector. With the rising death toll in LTC coupled with the human resource issues and lack of pandemic preparedness, every effort must be made to address these long-standing systemic challenges to redress the workforce crisis in LTC and avoid more catastrophic outcomes presently and in future pandemics. By taking steps to build supportive work environments for HCWs and staff empowerment, LTC homes can limit many of the harmful secondary effects of the pandemic.
Supplemental Material
Supplemental Material - Experiences of Healthcare Workers in Long-Term Care during COVID-19: A Scoping Review
Supplemental Material for Experiences of Healthcare Workers in Long-Term Care during COVID-19: A Scoping Review by Sheila A. Boamah, Rachel Weldrick, Farinaz Havaei, Ahmed Irshad, and Amy Hutchinson in Journal of Applied Gerontology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Canadian Institutes of Health Research (#478306).
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.