
Abstract
We examined the association between employment-related characteristics and the quality-of-care migrant live-in caregivers provide to older care-recipients. Structured interviews were conducted with 115 migrant live-in caregivers, 72 older care-recipients, and 117 relatives of care-recipients. We conducted correlations among dependent (quality-of-care), independent (quality of relationship between caregiver and informant, caregiver perception of work, and problematic employment conditions), and demographic variables, and performed a path analysis by conducting a series of multiple regressions. Quality-of-care was most highly correlated with quality of relationship between informant and caregiver. Quality of relationship was predicted by caregiver perceptions of work, which was negatively predicted by problematic employment conditions. In the relatives-based model, quality of relationship was significantly better when the care-receiver was female and the care-recipient needed more assistance with activities of daily living. The study clarifies the role of caregiver work characteristics for quality-of-care and highlights the crucial role of the relationship with the care-recipient.
Keywords
What this paper adds
• This is the first paper to examine the predictors of quality-of-care within the context of homecare provided by a migrant live-in caregiver. • Quality-of-care was found to be most highly and consistently significantly predicted by the quality of relationship between caregiver and informant, with the informant being either the older care-recipient or the closest relative of the care-recipient. • Employment conditions had a significant indirect impact on quality-of-care.
Applications of study findings
• Given the crucial role of relationships in the provision of care for frail older persons and those with dementia, caregivers, care-recipients, and their relatives need to be provided with tools to maximize the quality of those relationships. • Since employment conditions indirectly affect quality-of-care, a greater emphasis should be placed on providing live-in migrant caregivers with good work and living conditions. • In order to promote the quality of relationship between caregivers and care-recipients, the choice of caregiver should be based on considerations that are likely to promote such a relationship, including sharing a common language and cultural understanding.
Introduction
With the aging of populations worldwide, there is a growing demand for migrant live-in caregivers (hereinafter “caregivers”). Due to declines in co-residence of older persons and their adult children, and the increased participation of women in the workforce (Super, 2002), traditional family intergenerational care provision is expected to diminish (Pickard, 2015). Despite the need for paid caregivers, potential employees are often disinclined to participate in this employment sector due to poor living and working conditions frequently experienced by caregivers (Cohen-Mansfield et al., 2013; Green & Ayalon, 2018; Näre, 2013). To address this shortage, many countries allow care-recipients or their relatives to employ migrant caregivers from lower-income countries, offering the migrants benefits such as better living conditions than available in their home countries, and sometimes, the possibility of obtaining residential status (Bourgeault et al., 2010; Cohen-Mansfield et al., 2013). In Israel, the National Insurance Institute provides a governmental benefit toward hiring migrant caregivers for older persons with significant functional and/or cognitive impairment (National Insurance Institute of Israel, 2021).
Research that examined quality-of-care for older adults focused on settings other than home-based formal care. Studies of quality-of-care in nursing homes included developing quality-of-care indicators for nursing homes (Zimmerman et al., 1995), examining quality-of-care related to pain management (Hirdes et al., 2020), and investigating the impact of nurse’s aides’ private lives on quality-of-care (Tellis-Nayak & Tellis-Nayak, 1989). Regarding quality of family care in the home environment, studies included examining the effect of limited knowledge and stigma on the quality-of-care provided in the home for persons with dementia (Islam & Akter, 2021). The quality-of-care provided by migrant care-workers employed in residential facilities was also investigated (Ngocha-Chaderopa & Boon, 2016). In investigating the quality-of-care provided to older persons in their homes by paid migrant caregivers, Cohen-Mansfield et al. (2018) performed a factor analysis of a quality-of-care questionnaire which was answered by care-recipients receiving care and their relatives. Two factors emerged as characterizing quality-of-care: “caretaking” concerning provision of prompt care, and “knowing the person,” measuring interpersonal aspects of the care dynamic (Cohen-Mansfield et al., 2018).
Other studies that assessed quality-of-care provided to older persons generally used data provided by proxy respondents, such as relatives rather than care-recipients. Proxies have been found to be reliable sources for observable data such as patients’ symptoms, but less so concerning more subjective aspects of care-recipients’ experiences, such as emotions (McPherson & Addington-Hall, 2003). In studies where quality-of-care was based on care-recipients’ data, this was usually gathered through patient outcome data, for example, medication usage (Linn et al., 1977), or through satisfaction surveys (Cohen-Mansfield et al., 2000), in contrast to querying care-recipients directly about aspects of the quality-of-care they received.
The literature provides little insight into the likely predictors of quality-of-care that migrant live-in caregivers provide to older persons. Various aspects of relationship quality between caregiver and care-recipient, such as empathy and positive interactions, have been associated with quality-of-care, care outcomes, or care-recipient satisfaction, and have been advocated as cornerstones of good care (Beach & Inui, 2006; Kaplan et al., 1989; Mercer & Reynolds, 2002). In their examination of the nature of interpersonal relationships between live-in caregivers and older care-recipients, Teshuva et al. (2019) found the themes of emotional connection, reciprocity, effective communication, and meeting the older person’s care needs. An examination of caregivers’ burden and burnout revealed that care-recipients’ functional status and relationship with care-recipient had a direct impact on caregivers’ burden/burnout, with employment conditions and satisfaction with those conditions having an indirect effect (Cohen-Mansfield & Golander, 2021). In long-term care facilities, staff burnout was associated with poorer quality-of-care (Costello et al., 2019).
Employment conditions may require particular attention in the case of migrant live-in caregivers, given reports of poor working and living conditions (Spencer et al., 2012), excessive work (Gordolan & Lalani, 2009), insufficient breaks (Kalayaan, 2014), discrimination (Walsh & Shutes, 2013), over-control (Shinan-Altman & Ayalon, 2019), social subordination (Näre, 2013), verbal and sometimes physical abuse (Ayalon, 2008; Green & Ayalon, 2018), and malnourishment (Ayalon, 2008; Gordolan & Lalani, 2009). Even in countries with government-established work and living standards, such protections may be minimal (Cohen-Mansfield et al., 2017), and migrant live-in caregivers, care-recipients, and relatives may be unaware of caregivers’ rights (Green & Ayalon, 2015). Caregivers may not be able to take scheduled breaks if a substitute is unavailable. Inadequate working conditions and financial compensation can result in caregivers neglecting or abandoning their care-recipients (Salami et al., 2017).
Current research suggests that the relationship between caregiver and care-recipient, employment conditions, and caregivers' perceptions of their work may all influence quality-of-care, directly or indirectly. We examined the extent to which these caregiver-centered employment factors affect quality-of-care from the point of view of older care-recipients and their relatives (including many instances in which the care-recipient could not be queried because of dementia). This study is part of a larger investigation of care of older adults by migrant caregivers in Israel (Cohen-Mansfield et al., 2017, 2018, 2019; Cohen-Mansfield & Golander, 2021; Teshuva et al., 2019).
Methods
Participants
We recruited participants from 151 Tel Aviv and Jerusalem-area households that employed migrant live-in workers to care for older persons; our sample was recruited using the National Insurance Institute of Israel (66.45%), snowball referrals (18.55%), commercial databases of older persons (4.1%), or other means, including recruitment data from other studies (10.95%) (Figure 1). Recruitment method.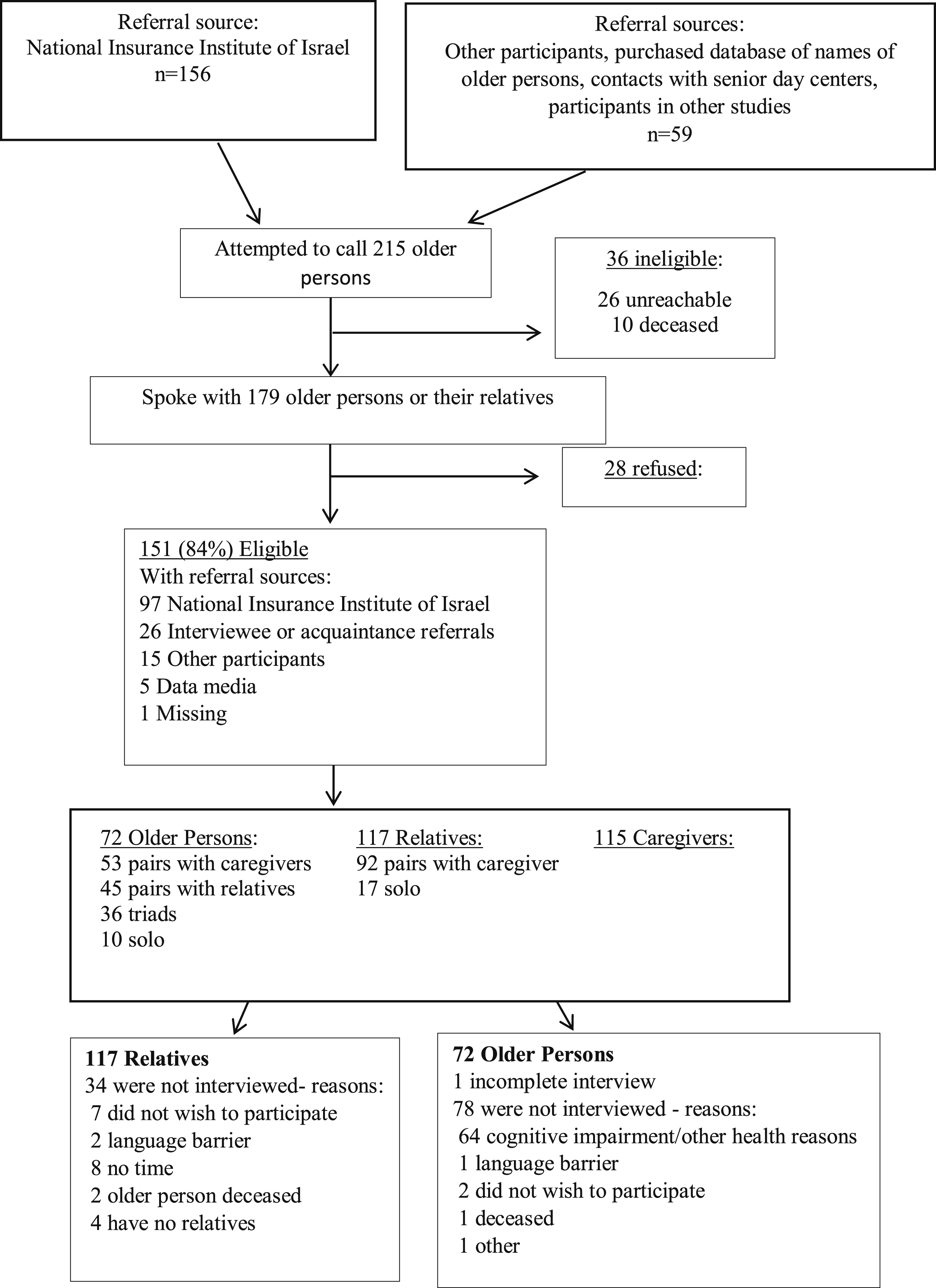
Ethical considerations
The Tel Aviv University Ethics Committee approved the study. All respondents signed a written informed consent form prior to participating in a structured interview.
Data collection
The structured interviews were carried out in English or Hebrew and lasted about 90 minutes. Most interviews were administered in the older person’s home. We aimed to interview as many of the triads—older care-recipient, relative, and migrant caregiver—as possible, but faced constraints, including cognitive and/or health problems for some care-recipients (as explained by their relatives), and language barriers or disinclination to participate by some migrant caregivers. Overall, we interviewed 115 migrant caregivers, 72 older care-recipients, and 117 relatives of care-recipients. Among these were 91 pairs of relatives and caregivers, 53 pairs of care-recipients and caregivers, and 36 triads.
Measures
Background variables
Participants’ demographic characteristics and outcome variables M (SD) or %.
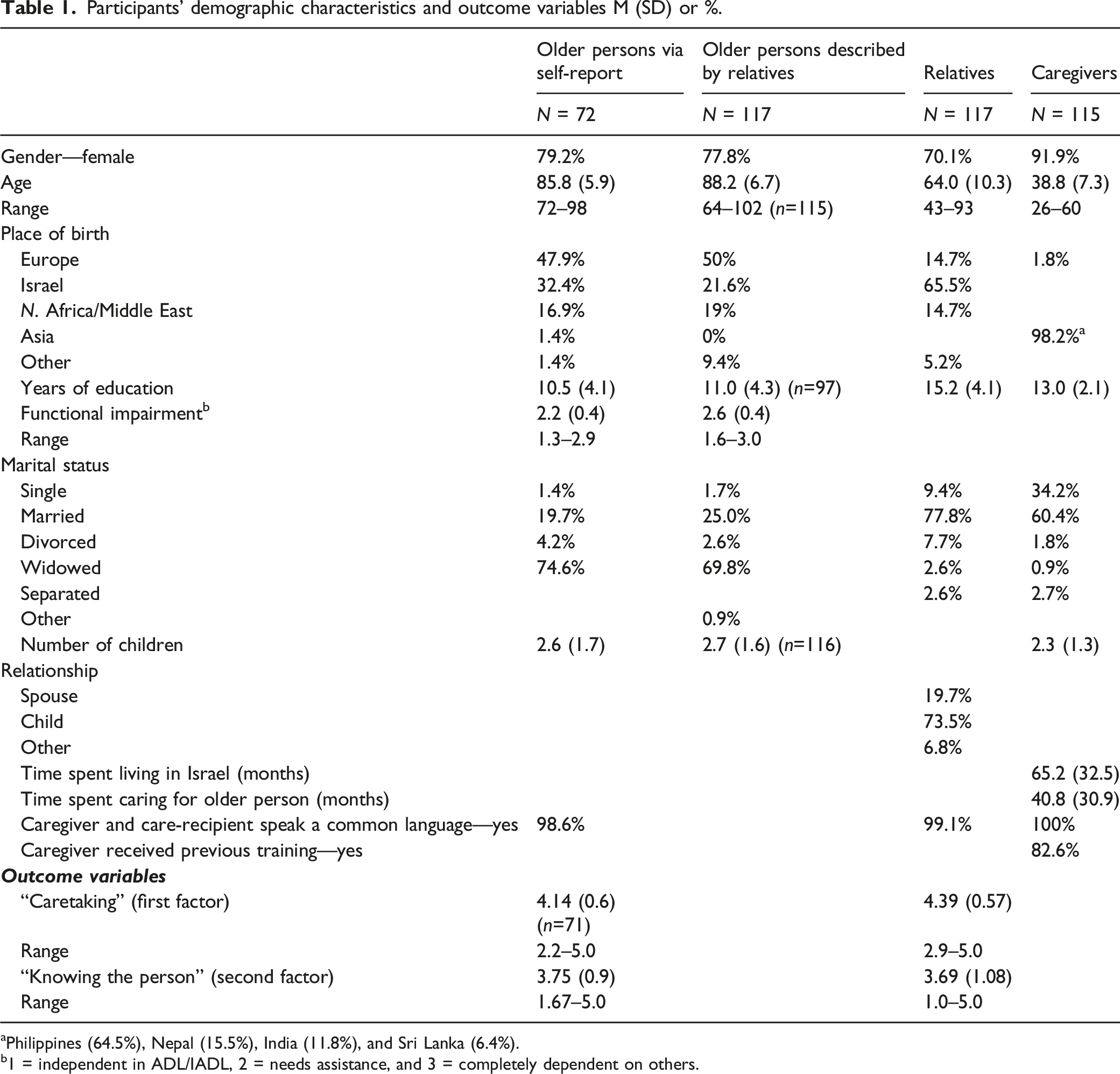
aPhilippines (64.5%), Nepal (15.5%), India (11.8%), and Sri Lanka (6.4%).
b1 = independent in ADL/IADL, 2 = needs assistance, and 3 = completely dependent on others.
Quality-of-care
Quality-of-care, the dependent variable, was measured according to care-recipients' and relatives' responses to the 8-item Quality-of-Care Questionnaire (QuCQ) developed for this population, based on the above-described factor analysis (Cohen-Mansfield et al., 2018). Items such as “To what extent does the caregiver provide you [the care-recipient] with support in the areas where you need help?” were rated on 5-point rating scales from “not at all” to “a very great extent.” Factor structures differed somewhat according to respondent but were conceptually similar. Since the factor structure, derived from relatives’ responses, contained much overlap between factors, we use the factor structure derived from care-recipients' responses for the evaluation of data gathered from either care-recipients or relatives. The first factor, care-taking, was composed of five items (regardless of respondent type): caregiver’s general quality-of-care, provision of support in needed areas, answering care-related needs, promptness in answering needs, and treating the care-recipient with respect (Cronbach’s alpha = 0.81 for care-recipients and 0.86 for relatives). The second factor, knowing the person, encompassed three items that measured the extent to which caregiver and care-recipient understand one another, caregiver knows care-recipient as a person, and caregiver recognizes care-recipient’s main concerns (Cronbach’s alpha = 0.69 for care-recipients and 0.74 for relatives). Among care-recipients, the first factor explained 43.37% of the variables' variance, whereas the second factor explained 20.90% of the variance. For relatives’ data, the first and second factors explained 52.97% and 15.50% of the variables' variances, respectively. (Cohen-Mansfield et al., 2018)
Independent variables
The measures used to assess the independent variables in this study (i.e., the predictors) are outlined below.
Quality of relationship with caregiver
This was measured via a ratings scale assessing the interpersonal relationship between caregiver and informant: care-recipients and relatives were asked to rate the quality of their relationship with the caregiver on a scale ranging from bad (1) to excellent (6).
Caregiver perception of work
This index consisted of eight items from a questionnaire originally developed by the CHEWE network, which studied coronary heart disease across Eastern and Western Europe, and presented a final report to the European Commission in 1996 (Pikhart, 2000). These items were used to evaluate caregivers’ perceptions of psychosocial job-related factors, such as “I have a lot of responsibility in my job” and “I experience adequate support in difficult situations” (where 1 = not at all and 5 = to a very great extent). This index also included an item, “In my work I am given a chance to be helpful to others,” extracted from the Minnesota Satisfaction Questionnaire (Weiss et al., 1967). Although this item was originally measured on a Likert scale measuring satisfaction (1 = not at all and 5 = extremely satisfied), we measured it in terms of caregivers’ agreement with these statements (where 1= not at all and 5 = to a very great extent) and utilized a mean value index. Reliability analysis revealed a Cronbach’s alpha of .80 (n = 99).
Problematic employment conditions
Based on Cohen-Mansfield et al. (2017), we included five items in the index: caregiver’s salary, whether problems arose due to the older person keeping a kosher kitchen, whether the caregiver was afforded sufficient heating/cooling when needed, access to laundry, and a comfortable bed. The item as to keeping kosher was selected based on previous research reporting tensions between some kosher care-recipients and migrant care-workers accustomed to a different lifestyle (Cohen-Mansfield et al., 2017; Freund & Band-Winterstein, 2019). Information concerning tensions related to keeping kosher was obtained based on reports of such a problem by care-recipients, relatives, or caregivers. Data regarding caregiver salary were obtained from the older person or relative and were dichotomized (as high or low) with the median of the sample as the cut-off point. When both the care-recipient and relative provided this information, an average was used due to high correlation (r = .845, two-tailed p < .001, n = 22). The remaining three items (i.e., sufficient heating/cooling, access to laundry, and a comfortable bed) were based on caregivers' responses and were dichotomized to indicate whether the condition, such as “access to laundry,” “bed comfort,” or “heating” was problematic. Higher scores indicate more problematic employment conditions.
Data analysis
Since the variable of caregiver’s perception of work was based on caregivers’ responses, it was missing for relatives and older persons whose caregivers did not participate in the study (n = 31 and 10, respectively). There were six relatives for whom all components of this variable were missing, even though the associated caregivers responded to part of the questionnaire. Therefore, regression analyses include 86 relatives and 53 older persons.
Univariate analyses involving means, standard deviations, and percentages—depending on the measurement of each variable—were used to characterize the demographic background of caregivers, relatives, and the older care-recipients who were interviewed, as well as the older care-recipients whose characteristics were derived from their relatives.
In order to understand the predictors of quality-of-care, we first conducted correlations between the two factors of quality-of-care according to each informant and the independent variables, as well as with the background variables. We examined the inter-correlations among the independent variables and the background variables of gender, age, and years of education. We then performed a path analysis by conducting a series of multiple regressions. First, we conducted a stepwise linear regression predicting each factor of quality-of-care by the other indices and controlling for gender, age, and years of education. We then tried to clarify significant predictors by examining regressions in which the significant predictors were the dependent variables and the remaining indices which did not enter the regression used as independent variables. This process underwent multiple iterations. While our data are cross-sectional, we use language that describes the impact of certain variables on other variables to describe the models being tested.
Results
Demographics
Descriptive statistics indicated that most participants were female: older persons (79.2% in older persons’ responses sample and 77.8% in relatives’ sample), relatives (70.1%), and caregivers (91.9%). Average age was 85.8 among older persons in older persons’ responses sample and 88.2 in the sample reported by relatives, 64.0 for relatives, and 38.8 among caregivers. Most of the relatives interviewed were children of the care-recipient (73.5%). Most caregivers stated they had received some sort of care-related training (82.6%). All older persons were dependent in at least some of their daily living activities with means indicating significant dependence as substantiated in the ADL/IADL ratings. (See Table 1.)
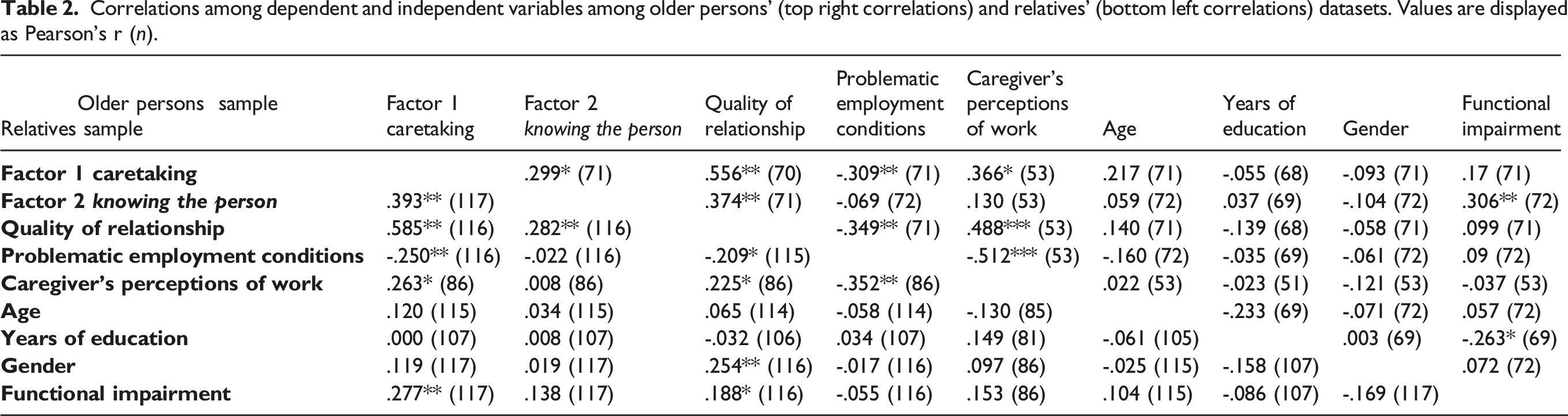
Correlations among dependent, independent, and background variables
Correlations among dependent and independent variables among older persons' (top right correlations) and relatives' (bottom left correlations) datasets. Values are displayed as Pearson’s r (n).
Regression analyses
Regression analyses predicting quality-of-care separately for older persons and relatives’ ratings – beta values and significance levels.
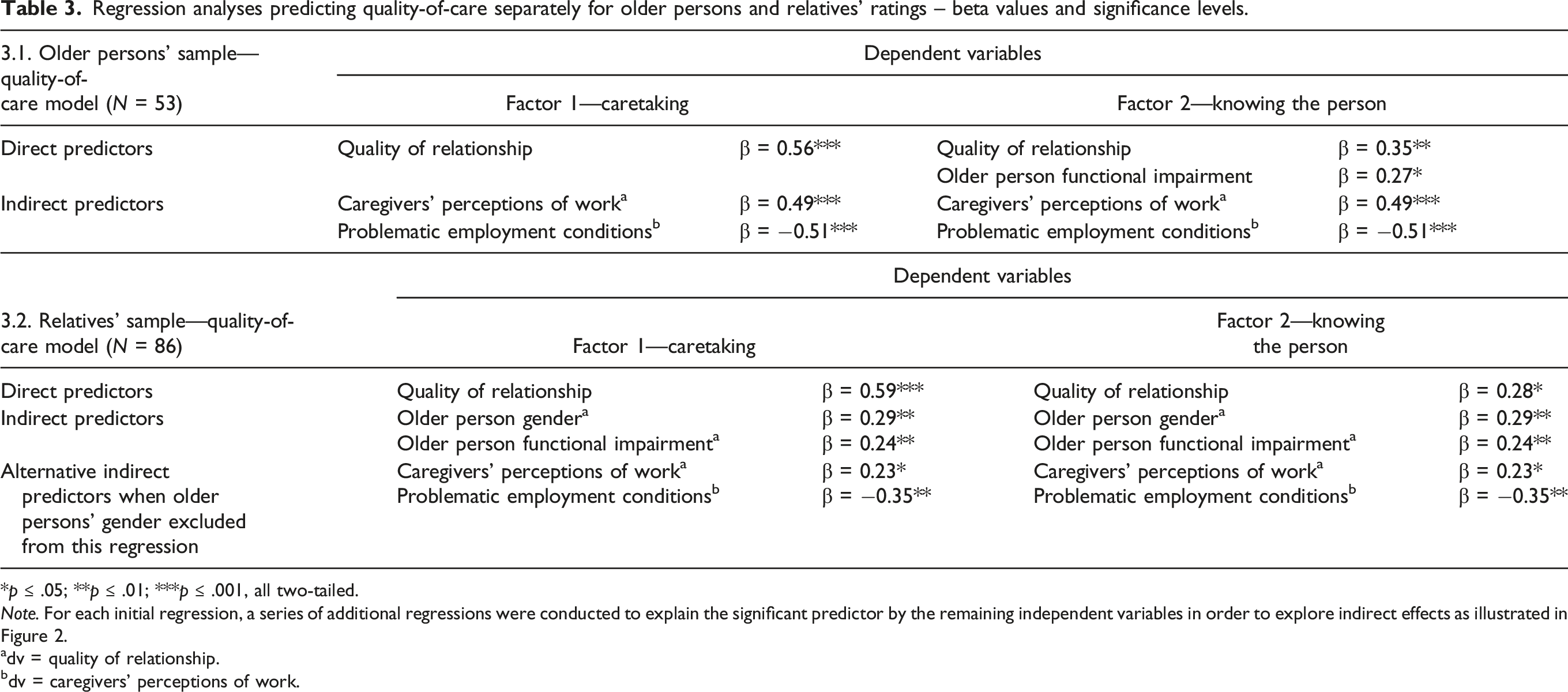
*p ≤ .05; **p ≤ .01; ***p ≤ .001, all two-tailed.
Note. For each initial regression, a series of additional regressions were conducted to explain the significant predictor by the remaining independent variables in order to explore indirect effects as illustrated in Figure 2.
adv = quality of relationship.
bdv = caregivers’ perceptions of work.
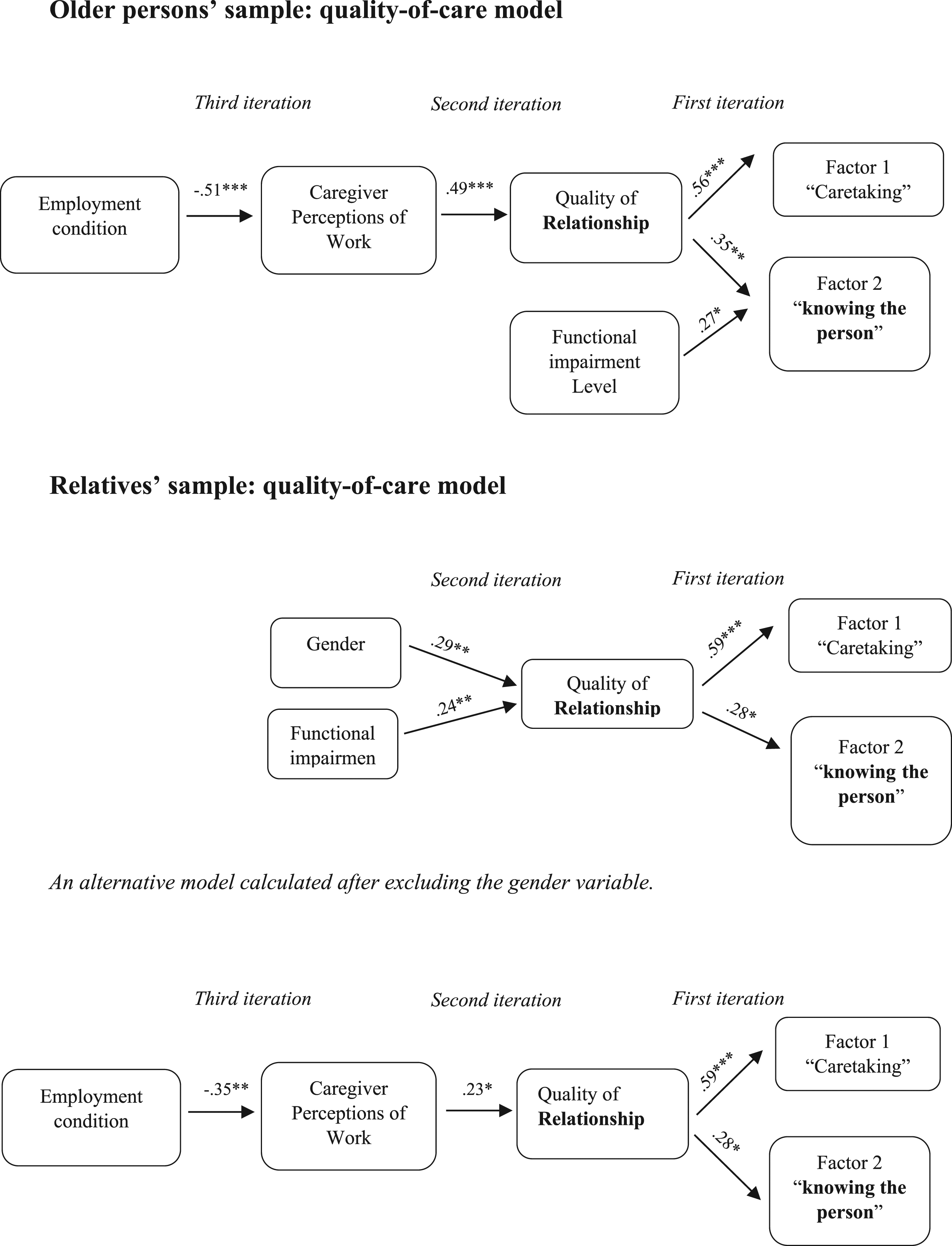
Predicting quality-of-care. Representation of the quality-of-care models according to each participant group sample.
Predicting quality-of-care: older persons (n = 53)
Caretaking
For the older persons' sample, in explaining the first factor, caretaking, only quality of relationship (F1,49 = 21.97, β = 0.56, p < .001) entered the regression equation. In turn, quality of relationship was significantly predicted by caregiver perceptions of work (F1,49 = 15.30, β = 0.49, p < .001, Table 3; Figure 2), which was significantly and negatively predicted by problematic employment conditions (F1,49 = 17.39, β = −0.51, p < .001, Table 3; Figure 2).
Knowing the person
For the older persons' second factor (knowing the person), significant predictors were older person’s functional impairment (ADL/IADL) (β = 0.27, p = 0.04) and quality of relationship (β = 0.35, p = 0.01). (F2,48 = 6.49, p < 0.01; Table 3; Figure 2). The predictors for quality of relationship were the same as those described under caretaking. (Table 3; Figure 2). The correlations with background variables, other than functional impairment, were not statistically significant in any of the iterations.
Predicting quality-of-care: relatives (n = 86)
Caretaking
Quality of relationship emerged as the only significant predictor for relatives' quality-of-care factor of caretaking (F1,79 = 41.00, β = 0.59, p < .001; Tables 3; Figure 2). Of the remaining variables, older person’s gender and older person’s functional impairment (ADL/IADL) significantly predicted quality of relationship (older person’s gender: β = 0.29, p < 0.01; older person’s functional impairment: β = 0.24, p = 0.03; F2,78 = 5.26, p< 0.01; Table 3; Figure 2). The care-recipient being a female and being more dependent on caregivers' help were associated with better quality of relationship with the caregiver. Removing the gender variable from the regression revealed that quality of relationship was significantly predicted by caregiver perceptions of work (F2,78 = 4.21, β = 0.23, p = 0.04; Table 3, alternative model and Figure 2). The final iteration revealed that problematic employment conditions was a significant predictor of caregiver perceptions of work (F2,78 = 11.16, β = −0.35, p = 0.001; Table 3; Figure 2).
Knowing the person
Relatives' factor 2 was predicted by quality of relationship (F1,79 = 6.83, β = 0.28, p = 0.01; Table 3). The predictors for quality of relationship were the same as those described under caretaking. (Table 3; Figure 2). Except for gender and functional impairment, as detailed above, the other background variables were not statistically significant predictors in any of the iterations.
Discussion
This is the first study to report on predictors of quality-of-care in the context of migrant live-in caregivers for older persons. We examined the perception of quality-of-care in two samples: older persons receiving care who, though dependent on caregivers, had the cognitive capacity to participate in the interview, and relatives of older care-recipients who rated quality-of-care based on their experience with the migrant live-in caregiver. The inclusion of the latter sample was necessary to investigate aspects of quality-of-care for care-recipients with advanced dementia.
All variables that described aspects of caregivers’ work–life experiences were predictive of quality-of-care, directly or indirectly. Quality of relationship between informant and caregiver was a direct predictor for both aspects of quality-of-care, caretaking and knowing the person, based on both relatives’ and care-recipients’ quality ratings. While this might seem obvious given our previous finding that relationship is a main component of quality-of-care within migrant live-in caregiver–care-recipient arrangements (Cohen-Mansfield et al., 2018), a question in the present study that explicitly assessed quality of relationship successfully predicted the entire construct of quality-of-care. This highlights the crucial role of relationship in provision of care in general (Mollon, 2014; Radwin, 2000; Thom et al., 2004), and for care of frail older persons in particular (Eustis & Fischer, 1991; Meyer et al., 2021; Wolff & Agree, 2004), and even more so for persons with dementia (Brooker, 2003; Fazio et al., 2018).
Live-in caregivers often serve as the sole social support for frail older persons (Ayalon et al., 2012), making the relationship essential for care-recipient wellbeing. The nature of the relationship can either facilitate or hinder requesting help with practical tasks and receiving it. While this finding should be considered robust, it may also reflect a bias, that is, when an informant has a better relationship with the caregiver, the informant is more likely to favorably characterize the quality of the caregiver’s work. Generally, there is congruence between the results based on older persons’ ratings and those of relatives. In both cases, employment conditions affect attitudes and perceptions of work, which in turn impact the quality of the relationship, which is the most potent predictor of quality-of-care as perceived by the “consumers”—care-recipients and their relatives.
The model based on older persons’ responses was essentially identical to that of relatives. Differences pertained to the impact of functional impairment, which was an additional direct predictor of the knowing the person factor in the older persons’ models. In contrast, functional impairment was a predictor of quality of relationship in the relatives’ models. In either case, greater dependence on caregivers was associated with a better relationship. The other difference was that female gender of older person predicted quality of relationship in the relatives’ sample. Only when the regression predicting quality of relationship excluded older person’s gender as an independent variable, did the work–life experiences of the caregiver (caregiver’s perception of work and problematic employment conditions) emerge as significant indirect predictors of quality-of-care in the relatives’ sample. We anticipated divergent results because older persons are the ones experiencing the caregiver’s services, whereas relatives can offer only their perceptions. Yet, very similar models emerged despite most relatives being adult children, 78.5% of whom did not reside with the older care-recipient. This concordance attests to the models’ robustness.
When including the gender of the older person in the models, the model based on the relatives’ sample changed somewhat. Instead of quality of relationship being explained by caregiver’s perceptions of work, which in turn, were explained by problematic employment conditions, quality of relationship was explained by gender and ADL/IADL, so that older female care-recipients and those with greater dependence on caregivers had a better quality of relationship (the most potent predictor of both components of quality-of-care). Since the vast majority (92%) of caregivers was female, it seems that female-to-female relationship building was easier and better than for mixed genders. Studies have found that compared to men, older women chose professional care more readily when level of disability increased (Carvalho et al., 2019). Therefore, using a formal caregiver may suit female care-recipients and positively impact the care-recipient–caregiver relationship.
The relationship between functional impairment and improved relationship with caregivers may be attributed to greater gratitude for caregivers when greater care needs are met or less friction with care-recipients about control when care-recipients are less able to exercise control. Our literature search did not find published research concerning the relationship between care-recipients’ functional impairment and quality of relationship with caregivers.
The strong association found between quality of relationship with caregiver and quality-of-care is consistent with reports that family members value the affective aspects of care (Sims-Gould & Martin-Matthews, 2010). This fits with Clarke and Hill (2012)’s statement that employees’ wellbeing is related to service-delivery outcomes. Quality of relationship and perception of work were significantly correlated. Caregivers' perception of their work seemed to provide a global sense of their job-related attitude, which, in turn, was predicted by problematic employment conditions. Thus, employment conditions do seem to affect quality-of-care, albeit indirectly. This finding should be considered within the context of employment conditions reported by this sample, which were better overall than reported in prior studies (Drori, 2009; Goldstein, 2010; Kalayaan, 2013, 2014). Nonetheless, our previous work did find adverse conditions, including failures on both the system level, like long working hours and inadequate time-off, and on an individual level, including uncomfortable bed, inadequate room temperature, and limited privacy for caregivers (Cohen-Mansfield et al., 2017).
The main contribution of this work is its pioneering examination of potential factors contributing to quality-of-care in the context of migrant live-in homecare. We also provide an initial model for the inter-relationships between quality-of-care, quality of relationships, perceptions of work, and problematic employment conditions.
Limitations
The main limitation of this study is the cross-sectional nature of the data. The variables included in both models (caretaking and knowing the person) could represent different directions or reciprocal relationships. Hence, it is difficult to determine causal effects. The size of our dataset dictated that we use path analysis to explore those relationships. Future studies with a larger dataset could explore other modeling approaches.
There are other factors that could affect quality-of-care which were not explored in our study, such as the nature and extent of job-training. Most caregivers reported having received training. Comments by caregivers indicated that this was provided by government agencies in their home countries. Such training likely varies by country, both in content (e.g., first aid, housekeeping, and cooking) and duration (Stilwell et al., 2004). Reports concerning training may also present a demand characteristic. Thus, future studies should examine the specific type of training received and caregiver knowledge and skill.
Considering our selection criteria, which required that interviewees speak either Hebrew or English, it is not surprising that most caregivers indicated having a common language with the older person. However, this may not represent the realities of other migrant live-in caregiver arrangements, as some researchers have found that language correspondence was rare in these circumstances (Spencer et al., 2012). Communication difficulties could pose a barrier to provision of care, its experienced quality, and the quality of care-recipient–caregiver relations. Accordingly, the impact of language barriers warrants further investigation.
Methodologically, we recommend that future studies include also asking relatives to rate the quality of the relationship between the care-receiver and the caregiver. While the assessment used for quality-of-care was subjective in that it was based on older persons’ and relatives’ perceptions, currently there are no objective measures of quality-of-care regarding homecare. Future studies could add more objective indicators, such as rate of functional change or use of observations from surveillance cameras. Additionally, caregivers should be queried about compensation issues.
We acknowledge that social desirability could bias responses by all participant groups. We tried to limit this by training interviewers to minimize bias and by promoting maximal interview privacy.
Conclusions
The results have significant implications for enhancing quality-of-care. Given the centrality of “quality of relationship,” efforts should be made to optimize conditions for a good relationship, such as assuring that caregivers and care-recipients share a common language, that individuals are paired based on shared cultural factors, and that means be developed to assist caregivers, relatives, and care-recipients in becoming familiar with each other’s cultural norms. When care-recipients are known to have had relationship problems, especially with previous caregivers, future caregivers should be given support to handle such situations. Acknowledging caregivers’ work as important and meaningful, and ensuring that care-recipients and relatives treat caregivers with respect may promote quality of relationship and thus also quality-of-care.
Although distantly related, problematic employment conditions do seem to have a significant, yet indirect role in quality-of-care. Therefore, systemic mechanisms are needed, not merely to enforce governmental standards regarding work and living conditions but also to ensure that older persons and their relatives have the resources to provide caregivers with proper conditions. While some elements, such as salary, are resource-dependent, others, such as room temperature and access to laundry, are more easily modified to improve caregivers’ conditions, with the potential to indirectly impact quality-of-care. Future research should examine whether systematically analyzing caregivers’ employment conditions, and preparing care-recipients and relatives to meet caregivers’ needs in order to improve the relationship, actually result in improved quality-of-care.
Supplemental Material
Supplemental Material - Predictors of Quality-of-Care Provided by Migrant Live-In Caregivers of Frail older Persons: A Cross-Sectional Study
Supplemental Material for Predictors of Quality-of-Care Provided by Migrant Live-In Caregivers of Frail older Persons: A Cross-Sectional Study by Jiska Cohen-Mansfield and Hava Golander in Journal of Applied Gerontology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the National Insurance Institute of Israel, the Minerva Foundation, the Israel Ministry of Senior Citizens, and the Herczeg Institute on Aging at Tel Aviv University.
Ethical Approval
Ethical approval was granted by the IRB of Tel Aviv University on 4 March 2010. No approval number was provided.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.