
Abstract
Objective
To assess the association between municipality altitude and quality of life (QOL) of older people in Colombia.
Methods
Cross-sectional study with data from the Colombian Demographic and Health Survey Older Adult Questionnaire 2015 (N = 13,970). QOL was measured in six domains: physical health, psychological health, functional status, social relations, medical history and economic status. Regression analyses were carried out adjusting by individual and contextual level variables.
Results
Low altitude was associated with better QOL: physical health (OR = 1.92, 95%CI 1.47−2.52), psychological health (OR = 1.59, 95%CI 1.26−2.00), functional status (OR=1.80, 95%CI 1.45−2.23), social relations (OR = 2.16 95%CI 1.73−2.70), and medical history (OR = 1.57, 95%CI 1.37−1.81). Economic status was not associated with altitude.
Discussion
Living at high altitude was associated with lower QOL for Colombian older adults. This finding encourages further study of high altitude and health outcomes among older adults in Colombia and other countries with populations living at high altitudes.
Introduction
The vast majority of the world’s population lives close to the sea or at low altitudes above sea level (National Geographic, 2011), including most people in high-income countries, where most medical research is conducted (Yegros-Yegros, et al., 2020). This fact may explain the dearth of research around the world on the health consequences of living at high altitudes. In some countries, however, including Mexico, Colombia, Ecuador, Bolivia and Nepal, the majority of the population lives at high altitudes. While living at high altitude has health implications for all people, it could have particular implications in the quality of life (QOL) of older people (Levine et al., 1997; Sakamoto et al., 2017).
As people age, their organs naturally experience loss of function. Environmental factors that produce discomfort for all people, such as winter cold, become particularly taxing for older people (Goodwin et al., 2001). Similarly, the effects of residing at high altitude above sea level, which moderately affect all people, may be particularly discomforting for older people. Organ loss of function (particularly lungs and heart), that comes naturally with aging, may reduce the body’s capacity to adapt to environmental factors such as residing at high altitude.
According to Levine, Zuckerman and de Filippi, older people’s moderate altitude exposure “is associated with hypoxemia, sympathetic activation, and pulmonary hypertension resulting in a reduced exercise capacity” (Levine et al., 1997). Gonzalez-Garcia, Barrero, and Maldonado observed that patients with chronic obstructive pulmonary disease residing at high altitude experienced more severe exercise intolerance, desaturation, and dyspnea than patients residing at sea level, due to decreased inspired oxygen pressure and the partial pressure of arterial oxygen as a consequence of lower barometric pressure at altitude (Gonzalez-Garcia et al., 2021).
This paper explores the idea that residing at high altitude above sea level, may be a factor affecting the QOL of older people.
The concept of QOL is increasingly recognized as a variable construct, which largely depends on the individual’s subjectivity. People all over the world are setting “good quality of life” as their primary goal for the last decades of their lives rather than just “long life” (Wilhelmson et al., 2005).
While the importance of ‘quality of life’ is widely acknowledged worldwide, the concept has a subjective component and it has been related to an elusive term: ‘well-being.’ The World Health Organization (WHO) defines quality of life as the “individuals’ perception of their position in life in the context of the cultures and value systems in which they live and in relation to their goals, expectations, standards and concerns” (The WHOQOL Group, 1995). This definition adds another subjective aspect: ‘Personal values.’ The WHOQOL Group proposes an instrument to measure QOL, including six domains: Physical health, psychological health, level of independence, social relationships, environment, and spirituality (religion or personal beliefs). (The WHOQOL Group, 1995).
In the same vein, the Center for Disease Control and Prevention (CDC) interprets QOL as a subjective evaluation of the aspects of life, and defines it as “an individual’s or group’s perceived physical and mental health over time” (Centers for Disease Control and Prevention, 2013). The CDC also proposed the concept of health-related quality of life (HRQOL), which includes the subjective evaluation of physical and mental health, and their correlates (functional status, social support, socioeconomic status, and health risks) (Centers for Disease Control and Prevention, 2013).
In the absence of a consensus on the scope and meaning of the concept of quality of life, the aforementioned definitions of QOL are the most frequently used to analyze this multi-faceted concept. Other definitions are available—QOL has been approached as a concept determined by the subjective judgment of the person rather than on ratings provided by others. This subjective judgment tends to reflect a multidimensional conceptual approach for QOL in older adults (Post, 2014).
The worldwide demographic transition experienced today, associated with the ageing process, has led to an increase in the burden of diseases due to the rising prevalence of chronic diseases, and functional limitations, which are related to lower QOL among older people. (Botero de Mejía and Pico Merchán, 2007). Elosua demonstrated in 2010 that the most important subjective factor regarding quality of life in older adults was health (Elosua, 2010), which can be attributed to the negative effect that chronic diseases produce at a physical and psychological domain (feeling of worthlessness, changes in daily life and conducts, and financial implications) (Alpi & Quiceno, 2012).
Some characteristics of the broad context have been related to an individual’s health. These characteristics are crime, safety, income and economy, quality of water, green areas and altitude (Avriel et al., 2011; Lora & World, 2010).
In Colombia, according to the last census (2018), there are 6,808,641 people above 60 years of age, which correspond to 13.5 per cent of the population (Departamento Administrativo Nacional de Estadística, 2018); from which 21.2 per cent reports some degree of dependency which affects their daily life (Flórez Nieto et al., 2019). While there are few studies conducted in some Colombian cities that attempted to characterize QOL of old people (Ocampo-Chaparro et al., 2013; Cardona-Arias et al., 2014), these studies do not consider contextual factors including altitude above sea level.
This study analyzes the impact of altitude above sea level on quality of life (QOL) with a large sample of older people. Since Colombian older adults living at different altitudes share a national culture and many contextual characteristics, the variation in exposure to high altitude among this population provides a valuable opportunity to broaden our understanding of this understudied determinant of health.
The population of older people in Colombia is exposed to a wide range of altitudes above sea level. In this study, we aim to contribute to the study of QOL in older adults by assessing its association with altitude at the municipality level in all regions of Colombia.
Materials and methods
Study design and participants
Cross sectional study conducted using data from the Older Adult Questionnaire; a nationwide survey for people over 60 years of age focused on demographic and health topics. The Older Adult Questionnaire is part of the Colombian Demographic and Health Survey (DHS) (Ojeda et al., 2011). This survey follows the approach and methodology of the global DHS Program surveys of the US Agency for International Development (USAID), which collects cross-country comparable data in developing countries worldwide. The older adult questionnaire was developed as a standardized questionnaire module of the same program (The DHS Program, 2021).
The basic approach of the DHS Program is to collect data that are comparable across countries. To achieve this, standard model questionnaires have been developed, along with a written description of why certain questions or sections have been included. These model questionnaires—which have been reviewed and modified in each of the seven phases of The DHS Program—form the basis for the questionnaires that are applied in each country. Typically, a country is asked to adopt the model questionnaire in its entirety, but can add questions of particular interest. However, questions in the model can be deleted if they are irrelevant in a particular country.
The study initially included the total number of adults over 60 years of age who were sampled by the Colombian DHS and answered the older adults questionnaire-i.e; 15,880 older people from 258 municipalities. The Colombian DHS included a representative sample of 99 per cent of the Colombian population using households as the sample unit. The households were selected randomly after following a stratified cluster sampling methodology to assure rural areas and minority representativeness. Only households from dispersed rural areas, with less than 1 per cent of the Colombian population, were excluded. The data was collected by Profamilia from November 2009 to November 2010. The household response rate was 80.1%. In 5.4% of households, respondents were unavailable to answer the survey, in 1.9% of households, participation in the survey was declined, in 6.3% the dwelling was empty, and in 6.2% of households, other reasons prevented participation in the survey. The individual response rate within households was above 90%. (Ojeda et al., 2011). Out of the 15,880 people who participated in the older adult questionnaire, only 13,970 older adults answered the QOL module of the survey. The study includes these 13,970 respondents.
Outcomes
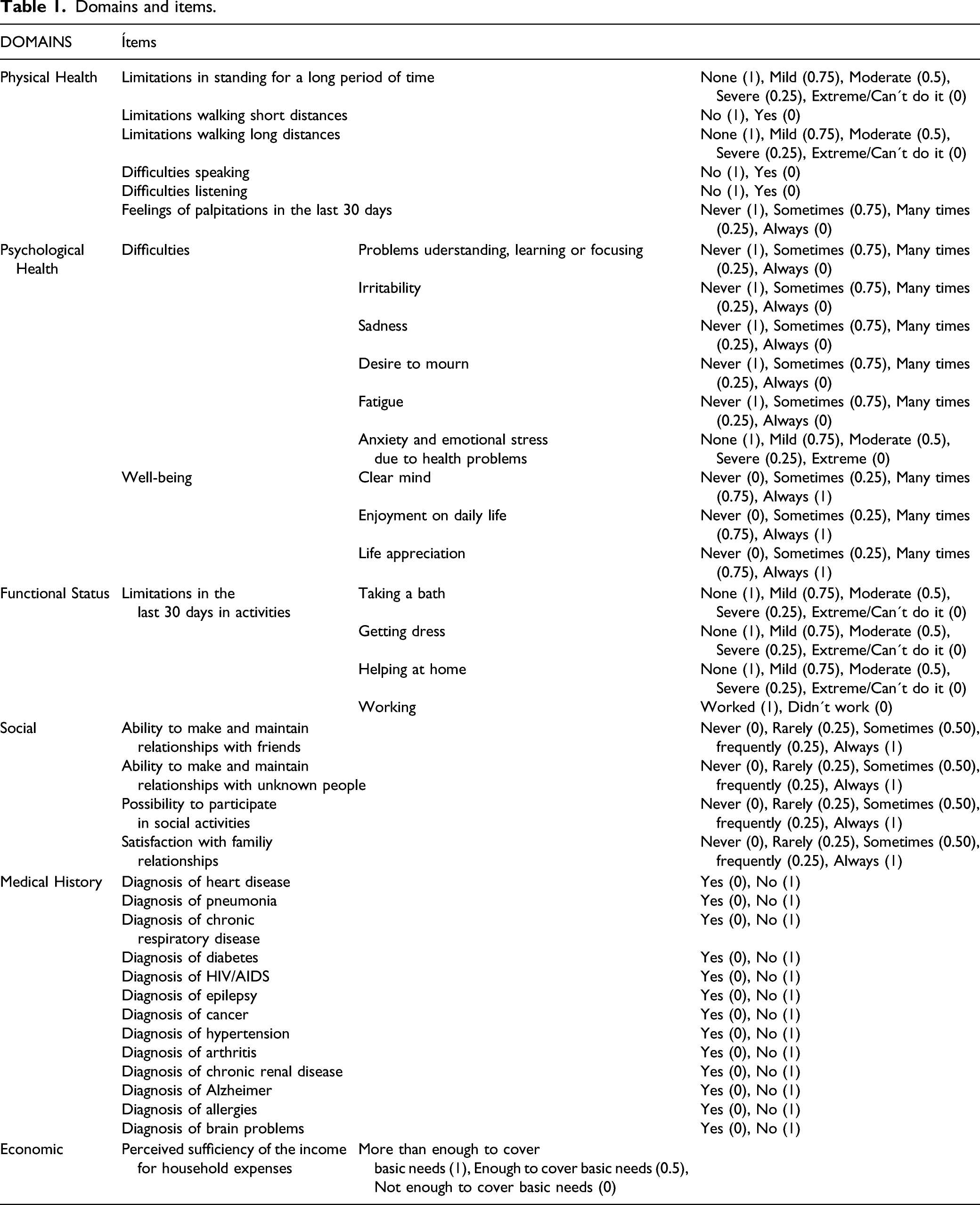
QOL was evaluated creating scales based on the domains proposed by the WHO (“The World Health Organization Quality of Life assessment (WHOQOL): position paper from the World Health Organization,” 1995) and the data available. The scales were developed by adding the scores of relevant individual items, as they were defined by the group of experts assembled by DHS at the request of the Colombian Government, and sponsored by Profamilia, the Colombian Ministry of Social Protection, the Colombian Institute of Family Welfare (ICBF), and USAID. The committee that developed the questionnaires included experts from Profamilia, the Colombian Ministry of Social Protection, the Colombian Institute of Family Welfare (Instituto Colombiano de Bienestar Familiar, ICBF), the Colombian Statistical Agency (Departamento Administrativo Nacional de Estadística, DANE), the Colombian Department of Planning (Departamento Nacional de Planeación, DNP), UNICEF, the National Cancer Institute (Instituto Nacional de Cancerologia), the Health Department of Bogota (Secretaria Distrital de Salud), the Planning Department of Bogota (Secretaria Distrital de Planeación), the Social Services Agency of Bogota (Secretaria Distrital de Integración Social), the National Health Institute (Instituto Nacional de Salud, INS), Fundación Santa Fe (research hospital), Universidad de los Andes, the Colombian Ministry of Education, and the Colombian Ministry of Agriculture (Ojeda et al., 2011). The scale has not been validated. QOL was assessed considering the following domains: • The physical health domain was measured by a self-assessment of health condition. It included the following items: limitations in standing for a long period of time, limitations for walking short or long distances, difficulties speaking and listening and feelings of palpitations in the last 30 days. • The psychological health domain included difficulties for understanding, learning or focusing, irritability, sadness, desire to mourn, fatigue, anxiety and emotional stress due to health problems. It also included items related to well-being such as clarity of mind, enjoyment of daily life, and life appreciation. • The functional status domain was evaluated considering limitations in the last 30 days performing activities such as taking a bath, getting dressed, household chores, and working. • The social domain considered the ability to make and maintain relationships with friends and unknown people; as well as the possibility to participate in social activities or nutritional programs (community public dining rooms where older adults can share and interact with people). • The medical history domain asked if participants had diagnosis of heart disease, pneumonia, chronic respiratory disease, diabetes, HIV/AIDS, epilepsy, cancer, hypertension, arthritis, chronic renal disease, Alzheimer, allergies, brain problems or any other chronic conditions. • The economic domain was determined by the perceived sufficiency of income for household expenses.
Domains and items.
Independent Variable
Altitude refers to the elevation of the municipality in meters above sea level (masl). The minimum altitude was 0 m, the maximum 3800 m, the mean 939 m, the median 744 m and the standard deviation 909 m above sea level. In Colombia, the municipalities correspond to territorial entities of the State with political and administrative autonomy, and whose main purpose is the general welfare and improvement of quality of life of its population (Ley 136 de, Congreso de Colombia, 1994). In this study, the municipality’s altitude refers to the altitude of the town center, from each municipality’s official website. While there may be minor variations in altitude across neighborhoods within one municipality, the town center’s altitude is generally where most people live.
Considering the literature on high altitude and the representativeness of the various altitudes in Colombia, the variable was recoded into low, moderate, and high for analysis purposes. To establish the cut points, we considered the tertiles of the variable (0–197, 197–1443 and 1443-3800) as well as the category of high altitude, above 1500 masl, defined by Paralikar and Paralikar. Low altitude was defined as 0 to 200 masl, moderate altitude as 200 to 1500 masl and high altitude above 1500 masl (Paralikar & Paralikar, 2010).
Control Variables
Individual Level Variables
The following variables were included in the analyses: age (in years), gender (male/female), head of household (yes/no), wealth index (measure index created by the DHS that accounts for the household relative wealth. Wealth index is a composite variable calculated using a principal components analysis, which includes items on ownership of selected assets such as housing building materials, water access and sanitation facilities), employed (yes/no), education (dummy variables: “No education”, “Elementary school”, “High school”, “Higher education”), lives with couple (yes/no), social security (dummy variables: “Contributory”, “Subsidized”, “Special”, “Not Known”, “Not affiliated”), and ethnicity (a self-determined decision) in Colombia, the majority of the population does not identify with any ethnic group.
Other variables considered, but not included in the analysis due to multicollinearity, were number of people living in the household, contribution to household income and expenses, family links, economic activity and area of residence.
Contextual Level Variables
The contextual variables included the following social and geographic characteristics: homicide rate measured as violent deaths per 100 thousand inhabitants (Acero, 2010); unsatisfied basic needs (UBN), measured by the Colombian National Department of Statistics, considers the dwelling’s building materials, access to public services, household income, economic dependency, and children school attendance (Departamento Administrativo Nacional de Estadística, 2018); and quality of water measured by the Risk of Quality of Water Index for human consumption in 2015. This index measures the quality of water in terms of its effect on human health, considering the physical, chemical and microbiological characteristics of the water (Instituto Nacional de Salud, 2015; Ministerio de Salud y Protección Social, 2014).
Statistical Analysis
SPSS 23 (IBM Corp., 2015) was used to create the database and to conduct descriptive analysis, and HLM 7 (Scientific Software International, 2011) for the multilevel statistical analysis, via graphic interface display in windows. We used Hierarchical Linear Modeling (HLM), a complex form of ordinary least squares regression, to analyze variance in the QOL domains when considering individual and municipality characteristics of the older people in Colombia.
The contextual and individual variables were described through measures of central tendency for numerical variables (mean and standard deviation) and proportions for categorical variables.
Multilevel models were used to assess the variation of QOL, analyzed as six independent domains, considering both contextual and individual variables simultaneously. The multilevel analysis consisted of two levels. The first level (individual) was composed of variables portraying individual demographic and socioeconomic characteristics; the second level (municipality) included contextual variables. The association between contextual variables and each domain of QOL was tested through multilevel binary logistic regression using fixed effects models with robust standard errors, providing the odds ratio (OR), the 95 per cent CI and the variance. Non-adjusted and adjusted models were reported.
Results
The full sample consisted of 15,880 adults over 60 years of age. Data was complete for 13,970 individuals who answered the QOL module of the survey.
Descriptive statistics of Individual variables for full data and study sample.
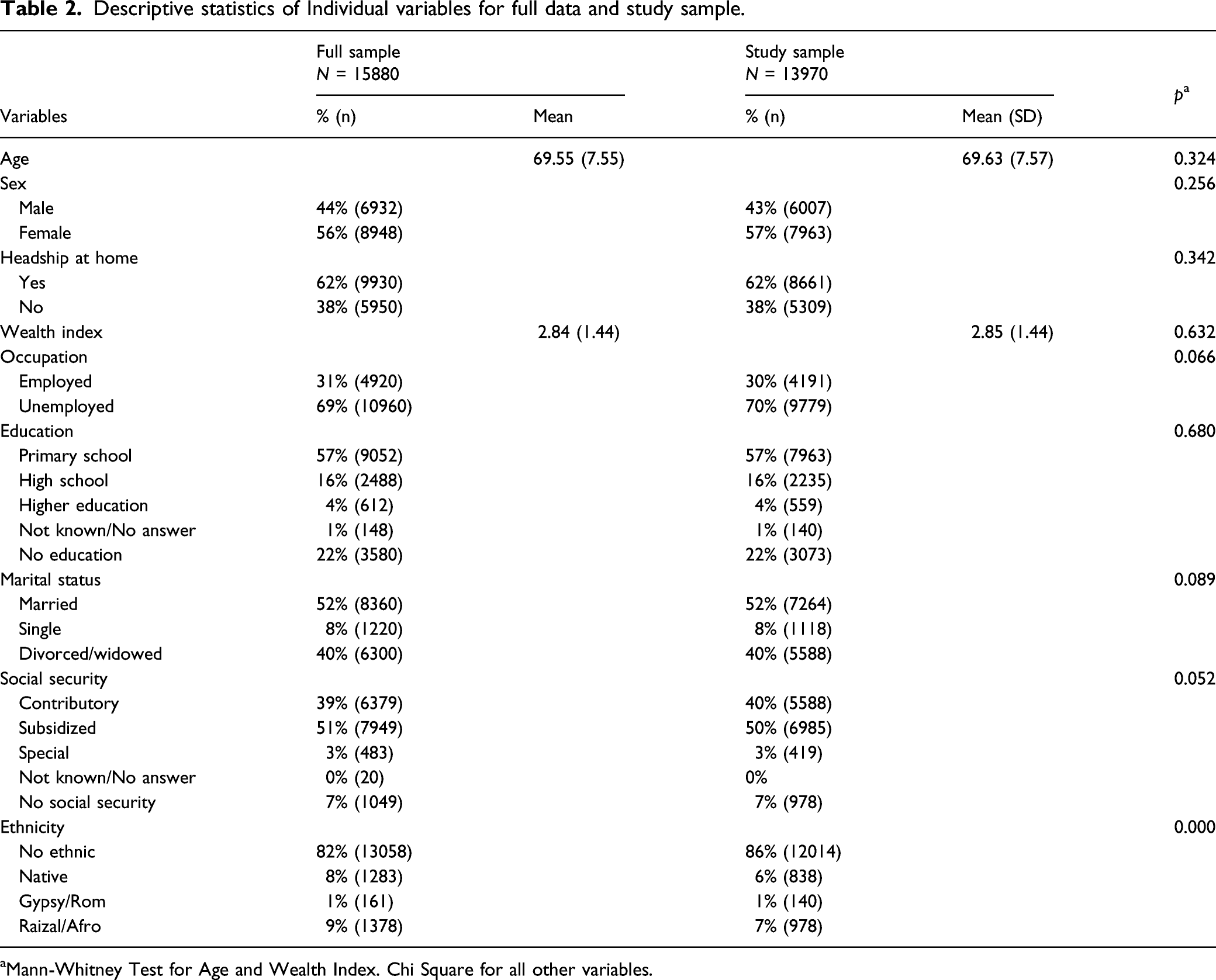
aMann-Whitney Test for Age and Wealth Index. Chi Square for all other variables.
Non-adjusted association between contextual variables and quality of life domains.
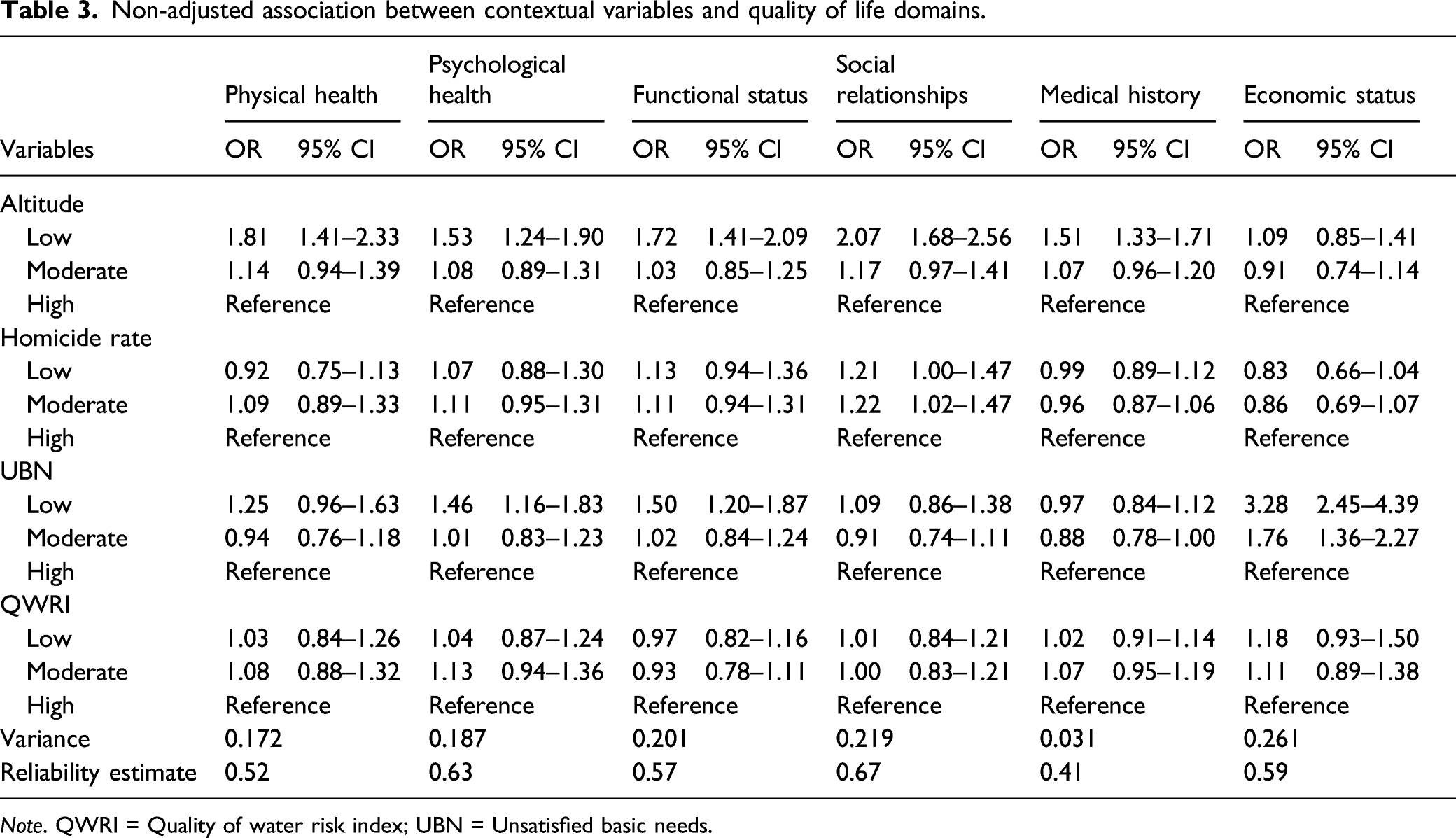
Note. QWRI = Quality of water risk index; UBN = Unsatisfied basic needs.
Adjusted association between contextual and individual variables and quality of life domains.
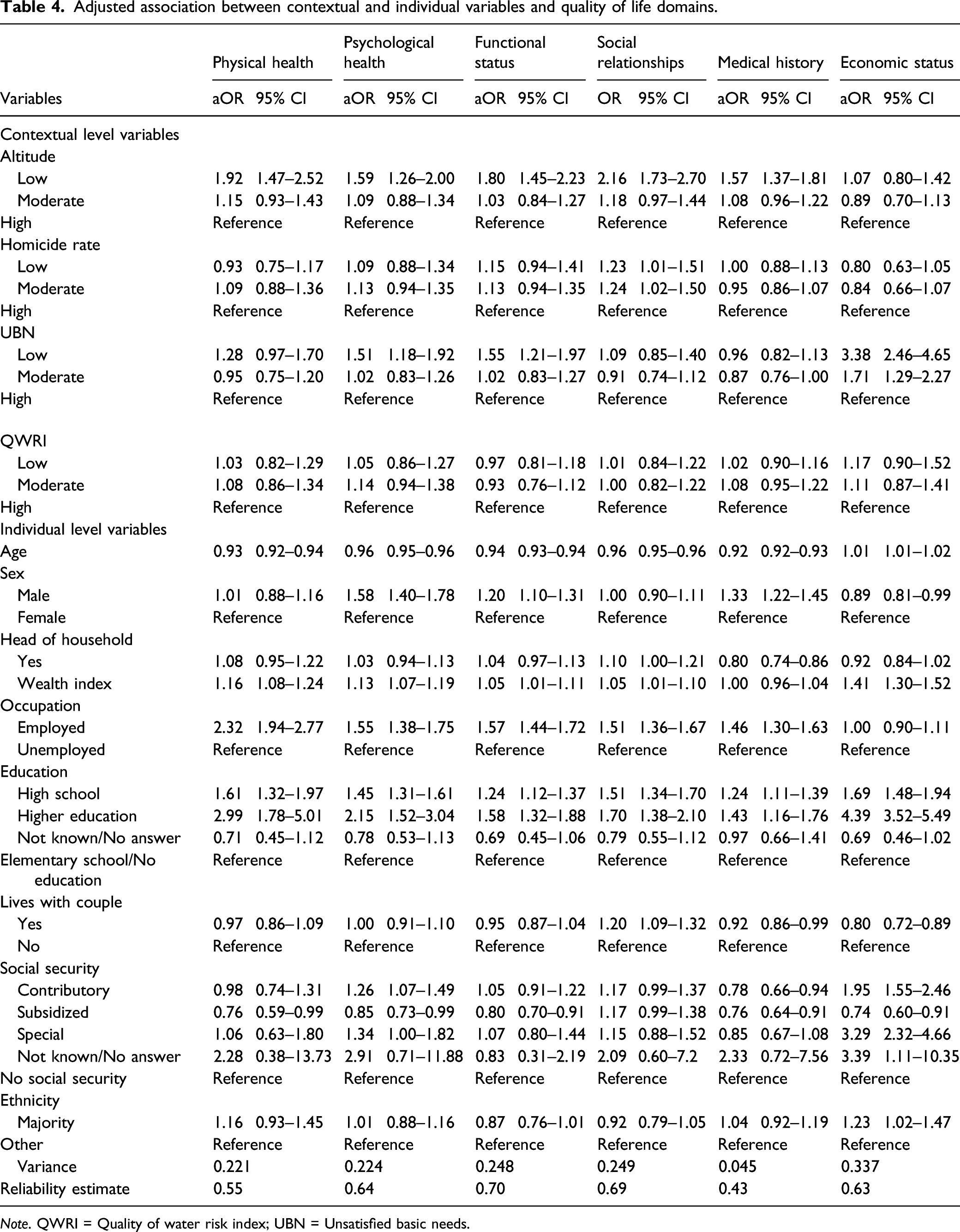
Note. QWRI = Quality of water risk index; UBN = Unsatisfied basic needs.
Quality of water and head of household were not associated with quality of life in the adjusted model.
Discussion
This study found that older people living at low altitude (0-200m above sea level) reported higher scores in the physical health, psychological health, functional status, social relations, and medical history domains of quality of life, than older people living at high altitude (1500m above sea level or higher). The economic domain of QOL was not associated with altitude.
As altitude increases, a progressive reduction in barometric pressure, air temperature and air humidity is observed. Barometric pressure determines the inspired and the alveolar oxygen partial pressure; with high altitude, the alveolar oxygen partial pressure declines, leading to a condition known as hypobaric hypoxia (Parati et al., 2018). Hypobaric hypoxia deprives the body’s tissues of oxygen from the air, affecting the body’s ability to transfer oxygen from the lungs to the bloodstream. Lower oxygen transfer affects the oxidation of complex chemicals to produce energy in the body. Normal saturation levels are lower at higher altitudes above sea level (Tannheimer & Lechner, 2019).
The ageing process leads to a gradual deterioration of physical health, which at some point affects the mental and functional status of an individual and might end up limiting essential activities of daily life (National Research Council, 2001). Deterioration of older adults’ physical health may impair oxygen transport, which may be particularly challenging for people living at high altitudes. Older adults might experience a greater reduction in work capacity when subject to altitude than healthy younger individuals (Levine et al., 1997).
A cross-sectional study by Urrunaga-Pastor et al., aimed at evaluating factors associated with poor physical performance of older adults living in high Andean communities, did not find an association between poor physical function and chronic high altitude, after adjusting for medical, functional and cognitive variables (Urrunaga-Pastor et al., 2019).
Levine, Zuckerman and de Filippi observed that the physiological response to hypobaric hypoxia in older population was similar to that reported in younger healthy subjects, considering that ageing does not appear to impair the physiological adaptive response to either acute or chronic hypoxia. However, they also reported that patients with coronary artery disease had limited maximal aerobic power in absolute terms, at both sea level and moderate altitude. In that same study, older adult patients tolerated moderate altitude of 2500 m well, but it was predicted that at higher altitudes, above 4000 m above sea level, activities of daily living would require more relative work rates for this population, resulting in a markedly impaired functional capacity. Despite extensive research into the pathophysiology of high-altitude exposure, there is few data available regarding the effects of altitude especially on older adults, with or without significant comorbidity (Levine et al., 1997).
In our study, adults above 60 years of age living in low altitudes reported better QOL in five of the six domains evaluated. Low altitude positively affected the physical and functional status domain. This could probably be attributed to the improvement of older adults’ health condition when exposed to higher barometric and inspired oxygen partial pressures at low altitudes —at low altitudes the air that we breath contains more oxygen—, being health status a self-determined measure. Likewise, a better QOL was reported for the psychological health domain. The evaluated older population considered having better general well-being when living at low altitudes, this is probably secondary to the improvement of their health-related problems due to higher oxygen availability at low altitudes, which allowed them to have a greater enjoyment of daily life.
Nonetheless, we cannot discard other potential factors that could impact the association between high altitude and QOL, including culture and weather-related lifestyles. Various studies have considered potential association between climate and economic prosperity (Anderson et al., 2007; Van de Vliert et al., 2000) or climate and happiness (Florida et al., 2013). Since temperature is inversely related to altitude above sea level, climate could partially explain the association between high altitude and QOL.
Our results also showed that low altitude positively affected the social domain. This could be correlated with better ability of the older people to make and maintain relationships with friends and unknown people, as well as their confidence and capacity to participate in social activities when they enjoy better health. Some studies have shown that social activities and the importance of family and friendship are related with well-being in older adults living at residential aged care facilities (Thomas et al., 2013), yet other studies have reported that community has no impact on QOL, at least in residential homes for old people (Suganya, 2016). The medical history domain was also associated with better QOL. As suggested above, older adults’ health condition improves when exposed to higher barometric and inspired oxygen partial pressures at low altitudes.
In a few studies, although including younger individuals, altitude has also been related with better HRQOL; in a Kibbutz, in the Dead Sea region, both healthy people and those with chronic diseases had better HRQOL (Avriel et al., 2011). A low altitude location has been recommended for some people with chronic diseases, such as congestive heart failure, as it has shown benefits in QOL scores and 6-minute walk measure (Gabizon et al., 2011).
The strengths of this study include the use of a representative sample of the Colombian population. The statistical model using multilevel binary logistic regression allowed a multilevel analysis of contextual variables associated with the domains of QOL in the framework of individual variables assessed; this resulted in an appropriate method to examine the association between contextual and individual variables, and quality of life. The outcomes in QOL were evaluated creating scales based on the domains proposed by the WHO and the data available.
This study has multiple limitations that must be considered. First, causality cannot be inferred because of its cross-sectional design, the results should be interpreted with caution as they present only associations and not causal relations. Nevertheless, cross-sectional studies are important for identifying indicators and variables for further research. Other limitations of the present study were the auto-assessed questionnaire, which can lead to response biases, and the difference between the initial sample and that with complete data. In particular, majority population is slightly overrepresented in the sample, largely due to language limitations among indigenous groups. We could not include autonomy in the analysis because the original questionnaire did not include this concept for older population. Finally, other potential factors that could impact the association between altitude and QOL, including culture and weather-related lifestyles, were not included in the study.
Conclusions
A significant finding of this study is the strong association between altitude and QOL of older people in Colombia. Since most QOL studies have been conducted in developed nations, where the exposure of older people to this main factor is low, the findings of this study suggest the need to consider this element when designing public policies aimed at older people, especially in developing countries.
The findings confirm previous studies that related contextual variables with QOL. Altitude at the municipality level was associated with the quality of life of Colombian older adults even after adjusting for individual demographic and socioeconomic characteristics. Altitude, which is not a modifiable factor, should be taken in account when evaluating individual patients.
Footnotes
Acknowledgments
To Milciades Ibañez for his statistical advice.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study did not represent any risk for participants since it involved the analysis of secondary data with no identifying information. It was approved by the ethics committee of the corresponding author’s university.