
Abstract
With an increasing aging population worldwide, there is a growing need for both palliative care and geriatric medicine. It is presumed in medical literature that both specialties share similar goals about patient care and could collaborate. To inform future service development, the objective of this review was to identify what is currently empirically known about overlapping working practices. This article provides a scoping literature review on the relationship between geriatric medicine and palliative care within the United Kingdom. The review encompassed literature written between 1997 and 2019 accessed via Scopus, Web of Science, PubMed, and Google Scholar. Three themes were identified: (a) unclear boundaries between specialties, (b) communication within and between specialisms, and (c) ambiguity of how older people fit in the current health care system. We suggest that more empirical research is conducted about the overlap between palliative care and geriatric medicine to understand how interprofessional working and patient care can be improved.
Introduction
Older patients often require more health care, especially in the last year of life (Higginson, 2016). In 2015, the United Nations predicted that worldwide, the number of older people will increase by 56% by 2030 (United Nations, 2015). In regions such as Europe and North America, the percentage of older people will increase to 25% (United Nations, 2015). Currently, in the U.K, 18% of the population is already 65 years and older, and this percentage is on the rise (Office for National Statistics, n.d.). With an aging population, there is presumably a larger need for both geriatric medicine and palliative care. This has become a concern for both policymakers and health care practitioners within the United Kingdom (Higginson, 2016), but there are questions about how this operates in practice.
Geriatric medicine is one of the largest specialties in medicine and can be defined as specialized care for older persons (Barton & Mulley, 2003). Palliative care, however, is concerned with the holistic symptom management, and often end-of-life care, of patients with life-limiting conditions. For the purposes of this article, these broad definitions have been used. Both specialties are known to provide care toward the end of a person’s life. To inform future service development around providing end-of-life care to older persons, the objective of this scoping review was to explore the current U.K. literature available on the working practices between the two specialties. Although palliative care has developed around the care for cancer patients, there is an increased call to include it in the care for other illnesses and patient populations (Skilbeck & Payne, 2005). At the same time, there has been a call for more integrated working within the National Health Service (NHS) in the United Kingdom to meet the changing demographics of patient populations (Goodwin et al., 2014). A European survey about palliative care provision for older patients identified considerable variability both within and between countries, with provision on geriatric wards being typically less developed than other service areas, suggesting that structures will need to adapt (Piers, 2010).
This review is concerned with the question, “What is known in the existing literature about the working practices at the intersection between geriatric medicine and palliative care in the United Kingdom?” A key focus of U.K. policy has been to improve partnership across the spectrum of palliative care provision (Gardiner et al., 2012). In this review, we are concerned with the extent to which this policy concern has sparked a growth in empirical evidence that explores the working practices between geriatric medicine and palliative care in this national context. By focusing on working practices, we take inspiration from the tradition within organizational studies known as “the practice perspective” to understand how different groups of professionals work together to deliver patient care (Nicolini, 2012, p. 214). This perspective recognizes the importance of understanding the detailed local patterns of activities of practitioners in terms of formal and informal rules of practice, specific social settings, and associated material tools and techniques. Understanding the interplay between the working practices of palliative care and geriatric medicine in these terms leads us to review existing literature covering the following topics: description of services; accounts of how care is provided; conceptualisations of the object of work; accounts of how professionals cooperate or fail to do so adequately; and analyses of how professional identities are created, maintained, or threatened during the course of practice (Nicolini, 2012; Nuutinen, 2005).
Method
Review Methodology
We followed the scoping literature review framework as described by Arksey and O’Malley (2005) to identify the gaps in literature with regard to the overlap in working practice between geriatric medicine and palliative care. We conducted the five steps outlined by Arksey and O’Malley: (a) identify a research question, (b) identify relevant studies, (c) select studies, (d) chart the data, and (e) collate, summarize, and report the results.
Search Methods
For the review, various databases were utilized, including Scopus, Web of Science, PubMed, and Google Scholar. Google Scholar was included to increase the likelihood that gray literature and postgraduate studies related to the topic could be included in the review. The search was limited to publications written in English between 1997 and 2019. Articles written before 1997 were excluded because much has changed in the provision and structure of NHS health care in the last 20 years and these older articles are unlikely to reflect current working practices. The purpose of this article was to explore the current research available within the United Kingdom, to focus on one health care system with a policy focus on integrated care; hence, articles on research conducted in different geographical areas were excluded. Moreover, terms such as palliative care, end-of-life care, and geriatrics have different meanings dependent on the health care setting they are used in; focusing on one health care system reduces confusion about what is being referred to in the research literature. Initially, we searched for terms such as geriatric medicine AND palliative care, but as the number of articles was limited, we broadened the scope by also searching for keywords indicating at collaboration within each specialty. Examples of this are the following: geriatrics/palliative care AND teamwork/practice, geriatrics/palliative care AND (interprofessional) communication. We included searches about end-of-life care to capture the presumed field of overlap for the two specialties in providing care toward the end of a person’s life.
Literature Selection
First, we identified relevant titles and abstracts (n = 90). Papers were excluded in this stage as it transpired that they were not about the right geographical location. Afterward, full articles (n = 18) were read (see Table 1). When reading, we were concerned with what perspective the literature was written from (e.g., which specialty and what type of health care professional), the method of study, and the type of article (editorial/review/research articles).
Papers Included in Review.
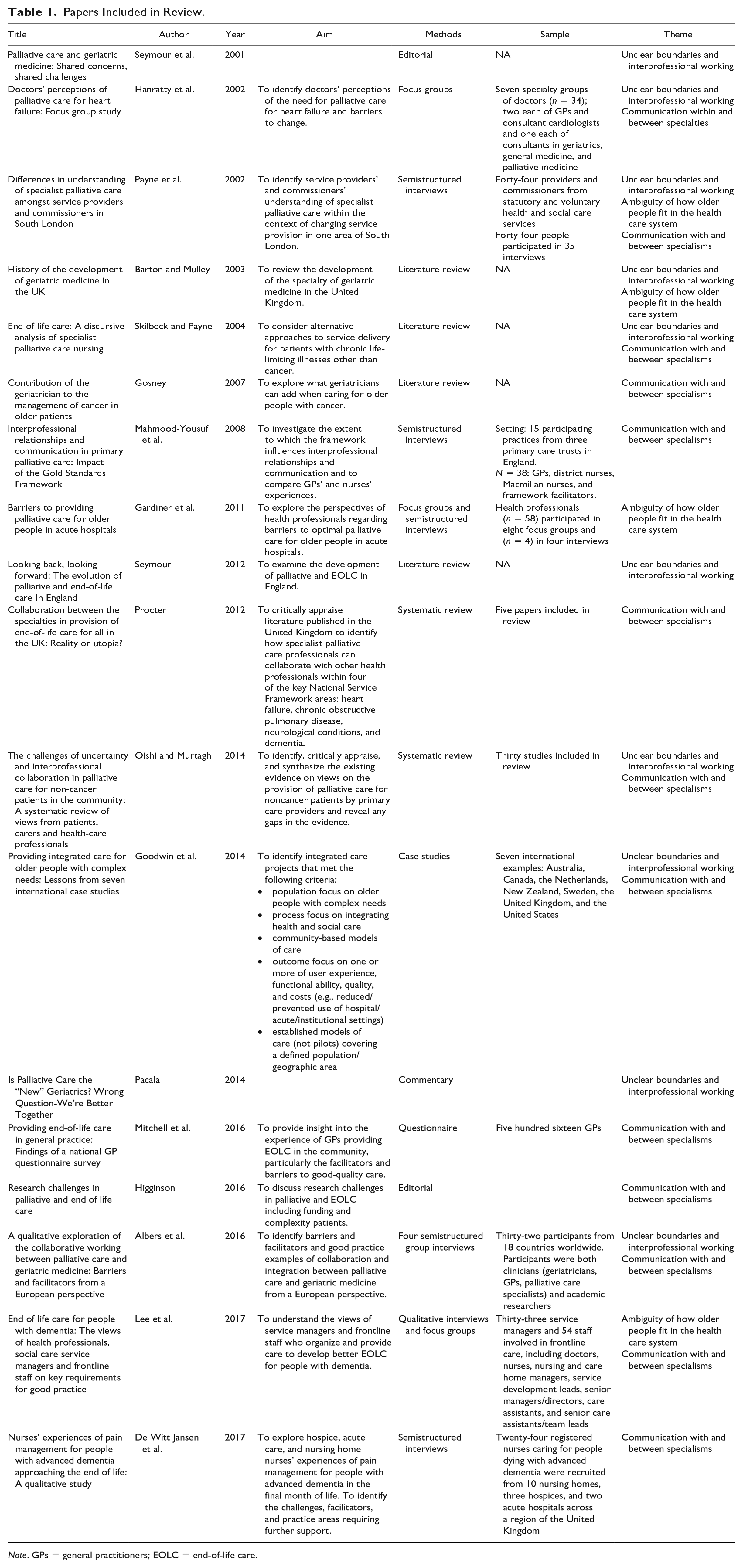
Note. GPs = general practitioners; EOLC = end-of-life care.
Analysis and Themes
The articles were read to identify themes regarding working practices between geriatric medicine and palliative care. We focused our lens on the way the two different disciplines worked together, or were assumed to work together, and within the included literature, three themes were identified: (a) unclear boundaries between the two specialties, (b) ambiguity of how older people fit in the current health care system, and (c) communication within and between specialties. These three themes will be discussed in the remainder of the article.
Results
The scoping literature review only identified one original empirical study that explored the overlap between palliative care and geriatric medicine which included data from the United Kingdom (Albers et al., 2016). Although both Seymour et al. (2001) and Pacala (2014) outline the common ground between the two specialties, both of their articles were opinion pieces/editorials. Two other articles were systematic reviews about interdisciplinary collaborations between generalists and specialist palliative care (Oishi & Murtagh, 2014; Procter, 2012). Overall, the scoping review identified very few research articles on current working practices and communication between palliative care providers and geriatricians.
The literature reviewed generally suggested an overlap and some integrated working between the two specialties within the British NHS. Seymour et al.(2001) identified the need for joint working practices between geriatrics and palliative care, describing three key common goals the specialties share in their care for older people: “managing those with the most complex needs; setting standards of good practice; and disseminating good practice through training, education and research” (Seymour et al., 2001, p. 270). Similarly, Pacala (2014) identifies various ways in which palliative care and geriatrics share a common ground, including goal-oriented care based on individual preferences; team-based interprofessional care models; proactive multidimensional assessment and identification of unmet needs; embrace of the biopsychosocial model of care and attention to psychosocial factors; attention to caregivers’ needs and inclusion of them in care planning and implementation; value-added service to particularly vulnerable and frail older adults. (p. 1969)
Consequently, the reviewed literature implies that due to these commonalities in approaches to care, the two specialties are well equipped to work together to provide care to older patients who may have palliative care needs. Yet, the scoping literature review only identified one original empirical study that explored the overlap between palliative care and geriatric medicine (Albers et al., 2016), indicating that this is still an underresearched, and perhaps underdeveloped, area of practice.
The following sections describe and discuss the three main themes found in literature in relation to working practices that can inform future service development and research. These include the following: unclear boundaries and implications for interprofessional working, communication within and between specialties, and ambiguity about how older persons are cared for within the health care system. Although we have separated these out into three themes, in practice, they impinge on each other in terms of how they affect working practices, and we have contextualized these findings with reference to wider literature about palliative care, geriatric medicine, and working practices.
Unclear Boundaries and Interprofessional Working
Although the literature reviewed overall suggested an overlap and some integrated working between the two specialties, it revealed unclear boundaries between these specialties. There are two identified reasons for this: variations in how the specialties are defined and a range in suggestions of what the overlap or interprofessional working should theoretically and practically be.
As part of our analysis, we examined the use of the terms geriatrics, geriatric medicine, palliative care, and palliative medicine within the identified articles. We found both a lack of definition of terms within articles and a lack of consistent use of the terms or definitions across the literature reviewed.
From the literature reviewed, defining geriatric medicine appears more straightforward than defining palliative care/medicine, which has undergone a shift in how the specialty is defined, perceived, and operates over the last several decades. Geriatric medicine, as a specialty, from its origin, has focused on the care for older patients as doctors argued that older people, on one hand, have different health care needs compared with younger people and may present illnesses differently (Barton & Mulley, 2003). Previous research demonstrates that different stakeholders have differing definitions of palliative care (Payne et al., 2002). Furthermore, while originally focusing on the care of cancer patients, the specialism of palliative care is opening the scope to include other types of patients, which could include older people with comorbidities (Seymour, 2012). This shift in palliative care suggests an increased overlap with geriatric medicine, as suggested in a number of the articles reviewed (Pacala, 2014; Seymour et al., 2001).
The boundaries between geriatrics and palliative care are, therefore, unclear, and an overlap has been identified in terms of what geriatricians and palliative care specialists do or could do (Pacala, 2014; Seymour et al., 2001). The reviewed literature states that certain geriatric medicine practices could benefit from palliative care, yet the role of geriatricians in the provision of palliative care is ill-defined (Gardiner et al., 2011). For example, Gosney (2007) argues for an increased role of the geriatrician in assessing older cancer patients as diagnosing symptoms specific to older people is their everyday practice (Gosney, 2007). The consensus in literature is that the two specialties are theoretically well equipped to work together due to their shared interests in older patients and providing care in the later years of life.
Despite these shared interests, these articles suggest there is limited understanding between the two disciplines in what they can offer each other (Albers et al., 2016; Seymour, 2012). There are a variety of views within each specialty, as well as between them, regarding the most appropriate role for collaboration in end-of-life care. Some geriatricians are reported as not seeing end-of-life care as part of their job, and hence keen for palliative care specialists to step in, whereas others see a palliative approach to end-of-life care as entirely within their repertoire of expertise and experience (Goodwin et al., 2014). Conversely, some palliative care specialists are reported as staking claim to a distinctive bundle of medical and psychological expertise, while others are keen to educate, upskill, and support other specialists to provide the basic elements of palliative and end-of-life care (Goodwin et al., 2014). There are, therefore, a variety of expectations about how the two specialties can work together in practice, ranging from education to working alongside each other on patient cases. While there is a theoretical shared object of work, how this is actioned in day-to-day delivery of care is not articulated in a consistent way, with considerable variation and perhaps an associated lack of clarity around professional roles and expertise.
Communication
Despite the assumption that the specialties should work well together in theory, these articles suggest that there is a clear need for more communication and clarification of responsibilities between the two specialties. The majority of articles that were included in this review acknowledge the need for “better communication” between the specialties or the need of more education—or cross-education—and knowledge with regard to palliative care, end-of-life care, and/or geriatric medicine.
It has been suggested that good communication is often the result of personal liaison rather than systematic processes (Gardiner et al., 2011). Albers et al. (2016) noted that interactions between professionals in the two specialties often took place in an informal and ad hoc way exemplifying this personal liaison approach. However, it was noted that patient care often involves more than two parties and that hierarchical systems in health care can hinder communication between specialisms. This hierarchical system can affect referral process to palliative care and decision-making about patient care (Payne et al., 2002). Furthermore, communication between professionals in the different specialties is influenced by their understandings of the role and scope of specific disciplines (Albers et al., 2016).
Ambiguity on the Placement of Older People Within Health System
Another factor in the working practices reviewed is understanding and identifying where older people fit in within the health care system. The multimorbidity that many older people experience provides a challenge to the current organization of health care as it becomes difficult to determine which specialism an older person should be referred to. Current knowledge on practice and referral is limited and mainly focused on specific symptoms and illnesses such as pain management (De Witt Jansen et al., 2017), heart failure (Hanratty et al., 2002; Oishi & Murtagh, 2014), or dementia (Lee et al., 2017). Within several specialties, interdisciplinary working is being promoted to improve the care for older patients. For example, one paper argues that geriatricians should work within oncology to assist with assessments and diagnosing comorbidities (Gosney, 2007). Similarly, Procter (2012) suggests that collaboration between specialist palliative care services and other specialties leads to better end-of-life care.
Discussion
This review starts with the premise that there are clinical and theoretical reasons to presume that geriatric medicine and palliative care can and should provide care to older patients, particularly near the end of life. For more than 15 years, there has been a call for more research on the overlap between geriatric medicine and palliative care (Albers et al., 2016; Goldstein & Morrison, 2005; Seymour et al., 2001) and the development of geriatric palliative care as an interspecialty collaboration (Morrison, 2013; Voumard et al., 2018). The current literature on the overlap between palliative care and geriatric medicine has mainly focused either on North America (Cao et al., 2015; Goldsmith et al., 2010; Kaasalainen et al., 2017) or the training of health care professionals (Braude et al., 2015; Mayne et al., 2014). As there have been multiple calls for research focusing on this area in the United Kingdom due to increasing patient and policy demand, this scoping literature review sought to assess the current interprofessional working between geriatrics and palliative care. However, despite this increased interest, surprisingly, little empirical research has been conducted in the United Kingdom that addresses the overlap between these two specialties and their shared working practices. In this discussion, we outline why this may be, the implications this underresearched area may have on patient care, and potential ways to improve the existing literature base.
Problems With Defining Specialisms
We intentionally limited the search to one health care system (the NHS in the United Kingdom) to avoid potential cultural variations in specialty definitions. However, we identified that the boundaries between the specialisms was not always clear in practice even in within one health care system. Moreover, many of the articles reviewed did not clearly define how they were using the terms or what services they were discussing, compounding the lack of clarity around professional boundaries.
The variation in defining the specialties can have implications for how they function in practice, making it unclear what roles, tasks, and services they cover, and what the scope for collaboration is. Some acknowledge that much palliative care is not provided by specialist palliative care services but by generalists such as GPs and district nurses (Gardiner et al., 2012); this previous review found similar themes as identified here. This indicates that describing the relationship between palliative care and any other area of medicine may be complicated if palliative care is seen as widespread and not a specific role or set of tasks. Moreover, in reality, patient care spans beyond both of these two specialties, and more could be done to understand how multiple groups of professionals work together and the training needed to enable this kind of interprofessional working (Lally et al., 2019).
While there is some movement to foster geriatric palliative care as an interspecialty (Voumard et al., 2018), it is notable that existing literature discusses how one form of specialty can be integrated into another, such as embedding palliative care into geriatric surgery or geriatric assessment (Gosney, 2007; Procter, 2012). A similar pattern was identified in a recent global review about maximizing the quality of life or older people at the end of life noting two service models have been developed: integrated geriatric care, emphasizing physical function, and integrated palliative care, focusing mainly on symptoms and concerns (Evans et al., 2019). Studies on integrated care, however, have revealed how stakeholders have different understandings of what integration looks like and how it should operate, which can raise questions about its effectiveness (Bone et al., 2014) and that there is also a lack of clarity in the empirical literature that describes what the integration is in practice (Borgstrom & Barclay, 2015). We, therefore, suggest that clarity around working practices should also be provided when describing integrated care.
This review highlights that poorly defining and describing areas of research can make it difficult to identify relevant literature. Consequently, because definitions of specialisms can vary, it is imperative that the research literature is clear about what it means when describing services and specialisms. This will enable more sophisticated meta-analysis of the empirical literature in the future as well as making it clearer how findings from one study can be possibly applied to other settings.
Interprofessional Education and Communication
One issue identified in literature that affects interprofessional working is communication between specialties. The lack of communication between geriatrics and palliative care specifically has been linked, at least in the United States, to limited resources and the potential threat of either of them disappearing as a distinct specialty (Pacala, 2014). Others suggest that the lack of interprofessional communication starts during the education of future health care professionals, as they are mainly educated with students from the same specialty (Lennon-Dearing et al., 2009). In addition, geriatric training is limited in medical education curricula and mainly absent in the training of those not specializing in gerontology or geriatrics (Caretta, 2015); similarly, palliative care education is often quite limited (De Witt Jansen et al., 2017).
When communication does occur, the literature suggests that it happens informally and in an ad hoc fashion (Kirby et al., 2014). This may be because of the unclear working boundaries, and it puts reliance on interpersonal relations for mediating these boundaries. Research on advance care planning for older adults—an example of where palliative care and geriatric care can coexist—indicated that trust is an important factor for interprofessional working (Bellamy et al., 2018). Research on collaboration with palliative care within hospitals has demonstrated that collaboration is fostered when specialist palliative care teams practice proactive communication, which can involve role negotiation and acknowledging colleague’s expertise (Firn et al., 2016). Further research could be conducted to examine what affects communication between these specialties in different settings, as well as the range and style of communication between professionals and how this influences working practices and patient care.
Implications for Patients Navigating Health Care Systems
The existing literature suggests little is known about the decision-making processes determining whether an older person is referred to geriatric medicine or palliative care. We speculate, based on research about referrals in other countries (Kirby et al., 2014), that this is currently decided on an ad hoc basis with each individual. Both the decision-making processes of older patients as well as those of health care professionals deserve more empirical investigation. Furthermore, as it is argued that a large proportion of care for older people is provided by generalists (Gardiner et al., 2012), a better understanding of the various stakeholders and who provides what type of care is necessary. This is especially important in a health care system that values “patient choice.” Because the provision and division of care is unclear for health care professionals, it cannot be expected that patients are informed about the options available, and this can have consequences for both patient experience and for the NHS in meeting its objectives about patient choice. While this review has focused on the United Kingdom, the findings resonate with other countries facing similar demographic changes and complexities in health care delivery (Albers et al., 2016). Drawing on the articles reviewed, in line with Procter (2012) and Gardiner et al. (2012), we propose, as there is a demographic shift in the patient population and the group of older patients presenting with comorbidities is predicted to rise, there will be the need for changes to how the health care system is currently organized. We propose that better understanding how care is delivered can inform this change.
Lack of Empirical Research and Areas for Future Research
One of the salient findings from this review is the relative lack of empirical papers compared with editorials, despite the theoretical and practical fit for collaborative working, and the policy acknowledgment about older people needing palliative care (Department of Health, 2001). Higginson (2016) argues that research in end-of-life and palliative care is underfunded compared with studies into the cure and prevention of life-limiting diseases. Both geriatric medicine and palliative care focus on caring rather than curing. Perhaps this lack of relative funding explains the paucity of empirical studies on the overlap between palliative care and geriatric medicine. Another element that might explain the limited research into the connection between geriatrics and palliative care is the lack of knowledge about and appreciation of the costs of palliative care (Gosney, 2007). Palliative care and its relationship to geriatrics do not feature on lists of priority areas for innovation to reduce service costs because the costs involved are not well understood. So, although there are assumptions that collaboration or integration would be beneficial, and a policy interest in increased integration, what forms it would take have yet to be fully identified or appreciated.
In the articles reviewed, the main methods used to explore the interface between geriatric medicine and palliative care have been focus groups (Gardiner et al., 2011; Hanratty et al., 2002) or semistructured group interviews with health care professionals (Albers et al., 2016). Although both of these methods are valid for gaining insights, they are also limited, and we need to understand the way methods shape what information is gathered. During focus groups, doctors are removed from their context of practice and they reflect on past experiences. In this, they can filter their perceptions and perhaps adapt and reconstruct them to illustrate a more ideal picture. Interviews can present similar limitations, but this can be mitigated to a certain extent by the breadth of the interview and skills of the interviewer. Individual interviews with stakeholders could be beneficial as they provide a safer space to discuss the limitations in service and care provision compared with group interviews. In various studies, hierarchy and power relations have been noted as an issue (Mahmood-Yousuf et al., 2008) within care settings, with doctors not listening to suggestions of nurses. It could, therefore, be argued that health care professionals change their answers within a group setting, and individual interviews could explore both the positive and the negative sides of communication and teamwork in a more in-depth way.
In addition, because current research is based on the reflections of health care professionals, removed from the workplace, it reveals little about the nature of ad hoc decision-making and collaboration within care settings. The findings of this review indicate that people are able to articulate what is not working, but little has been said about what is happening, how it is happening, and why. Future research could benefit from ethnographic research on everyday decision-making and interprofessional working to describe in more detail the working practices within and between the fields of geriatrics and palliative care. Observations within the health setting would provide a broader picture, revealing the complexity of decision-making and working practices. Such research could be informed by anthropological, sociological, and organizational study theories about interprofessional working. In line with Gardiner et al. (2012), we suggest that more empirical research within health care settings would provide a welcome addition to the paucity in studies on the realities of collaboration.
Contributions and Limitations of This Review
This review specifically focused on working practices between geriatrics and palliative care within the United Kingdom, identifying similar findings as previous reviews about palliative care more generally (Gardiner et al., 2012) as well as the lack of empirical research on working practices. We experimented with a variety of alternative search strings that included specific disease management (i.e., dementia); yet, we have kept the specific focus of this review for clarity and focus on the specialties of palliative care and geriatric medicine. This review focused on the United Kingdom to understand the working practices within one health care system. A similar review could be conducted about other countries or even compared working practices between countries, although there may be a similar lack of empirical evidence of working practices in literature as identified and discussed within this review.
Conclusion
To reflect the changing nature of health care due to the current and future demographic of older patients, more research is needed on the interprofessional working between specialisms. In particular, we have identified that very little is known about the working practices at the interface between palliative care and geriatric medicine and what has been identified highlights barriers to collaboration and integration. Literature suggests that theoretically the two should work well together as they share common goals in patient care; however, how this can best be done in practice is not yet well evidenced. The existing literature acknowledges that unclear professional boundaries and communication present current barriers to collaborative working. We suggest conducting more research on current working practices to identify current productive practice and further areas for improvement. In particular, there is potential for qualitative research to reveal more of the richness of actual practices: the ways in which effective collaboration sometimes emerges and is sometimes frustrated, how professional identities develop as more or less collaborative, and the implications this has for patient care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Open University Health and Wellbeing Priority Research Area funded the scoping review.