
Abstract
Scholars have long investigated the factors that affect health outcomes in less-developed countries. One debate that has increasingly intensified in recent years is the democracy and health relationship in comparative international context. Scholars argue that democracy does affect country-level health outcomes in less-developed countries, while others argue democracy does not affect country-level health outcomes. I estimate the effect of numerous democracy indexes on child mortality and infant mortality in developing countries using fixed effects regression models with heteroskedasticity-robust standard errors clustered by country. I find that multiple aspects of democracy exert significant beneficial effects on child mortality and infant mortality in less-developed countries.
One of most pressing issues facing humanity is the problem of child mortality and infant mortality in developing countries. 1 The problem is quite intuitive, but it is especially worth noting that the child mortality rate and infant mortality rate is much higher in many of the world’s developing countries relative to numerous countries within the Global North (World Bank 2020). Also, the United Nation established the Sustainable Development Goals in 2015, which are a set of 17 interrelated development goals. Goal 3 is to achieve good health and well-being more generally and to achieve specific targets. Within this broader goal, there is the specific target of ending preventable deaths of newborns and children under five years of age by 2030. Furthermore, a more specific goal is that all countries get their child mortality rate to at least as low as 25 per 1,000 live births. Of course, many countries need to substantially accelerate their progress on reducing their child mortality rate, and, as a logical extension, their infant mortality rate, to reach this specific goal by 2030 (World Bank 2020). Without a doubt, the importance of investigating the factors that affect child mortality and infant mortality in developing countries cannot be overstated.
Social scientists have long debated the factors that affect health outcomes in comparative international context. One debate that has intensified in recent years is the democracy and health relationship. Much scholarship finds that democracy exerts a beneficial effect on health outcomes and social welfare outcomes more broadly (Besley and Kudamatsu 2006; Frey and Al-Roumi 1999; Klomp and De Haan 2009; Lake and Baum 2001; Lena and London 1993; London and Williams 1990; Moon and Dixon 1985; Tsai 2006; Wickrama and Mulford 1996; Wigley and Akkoyunlu-Wigley 2011; Young 1990; Zweifel and Navia 2000). A growing body of scholarship, however, has somewhat eroded confidence in our scholarly understanding of the relationship between democracy and health outcomes in comparative international context (Burroway 2012, 2016; Noble 2019; Ross 2006; C. L. Shandra, Shandra, and London 2012; Swiss et al. 2012; Weede 1993; Wejnert 2008). The democracy and health relationship is one of the most intensely debated areas of scholarly dialogue in the comparative international social sciences but more research is needed for social scientists to draw more definitive conclusions about the democracy and health relationship in cross-national context.
In this analysis, I address the issue outlined in the preceding discussion. Using fixed effects (FE) panel regression models with heteroskedasticity-robust standard errors clustered by country, I present new cross-national evidence on the effects of democracy on child mortality and infant mortality in less-developed countries from 1990 to 2016. I also control for economic development, total fertility rate, secondary school enrollments as a percentage of gross, trade openness, exports to high-income countries (HICs), and international nongovernmental organizations (INGOs). Net of relevant statistical controls, results indicate that indices of multiple aspects of democracy exert significant beneficial effects on child mortality and infant mortality in less-developed countries from 1990 to 2016.
Important and pioneering work has been done on this topic, but I improve upon the limitations of some of the previous research on the democracy and health relationship in the following ways. First, I use more expansive cross-sectional longitudinal data than some of the previous research that investigates the effect of democracy on related health outcomes, which can lead to more precise parameter estimates (e.g. Burroway 2012; Frey and Al-Roumi 1999; London and Williams 1990; Moon and Dixon 1985; C. L. Shandra et al. 2012; Swiss et al. 2012). Second, I use econometric methods that account for unobserved heterogeneity. Not accounting for country heterogeneity can cause bias in pooled ordinary least squares (Wooldridge 2009). Third, I analyze a more contemporary time period, with the temporal scope of the analysis being from 1990 through 2016. Overall, this analysis improves upon the important work that has been done by addressing some of the limitations of previous scholarship.
I begin the analysis by providing an overview of some of the previous literature on the democracy and social welfare nexus and theorizing some of the ways in which democracy can affect health outcomes in developing countries. Then, I state the specific propositions I derive from the theorization. Next, I delve into a description of the data set, dependent variables, independent variable of interest, control variables, and methodological approach. Then, I briefly summarize the results of the analysis. I then conclude by discussing the significance of the results in the discussion and conclusion section in addition to relating the findings to broader scholarly discussions in the comparative international social sciences.
Reviewing Cross-national Studies on the Democracy and Social Welfare Relationship
Table 1 presents a summary of previous studies on the democracy and social welfare relationship. I note the authors of the study, the method used, the democracy and social welfare measure used, and the general result from the analysis. Please note that this table is not a representation of every study conducted on the democracy-social welfare relationship but provides a general overview of some of the important work on this topic.
Reviewing Cross-national Studies on the Democracy and Social Welfare Relationship.
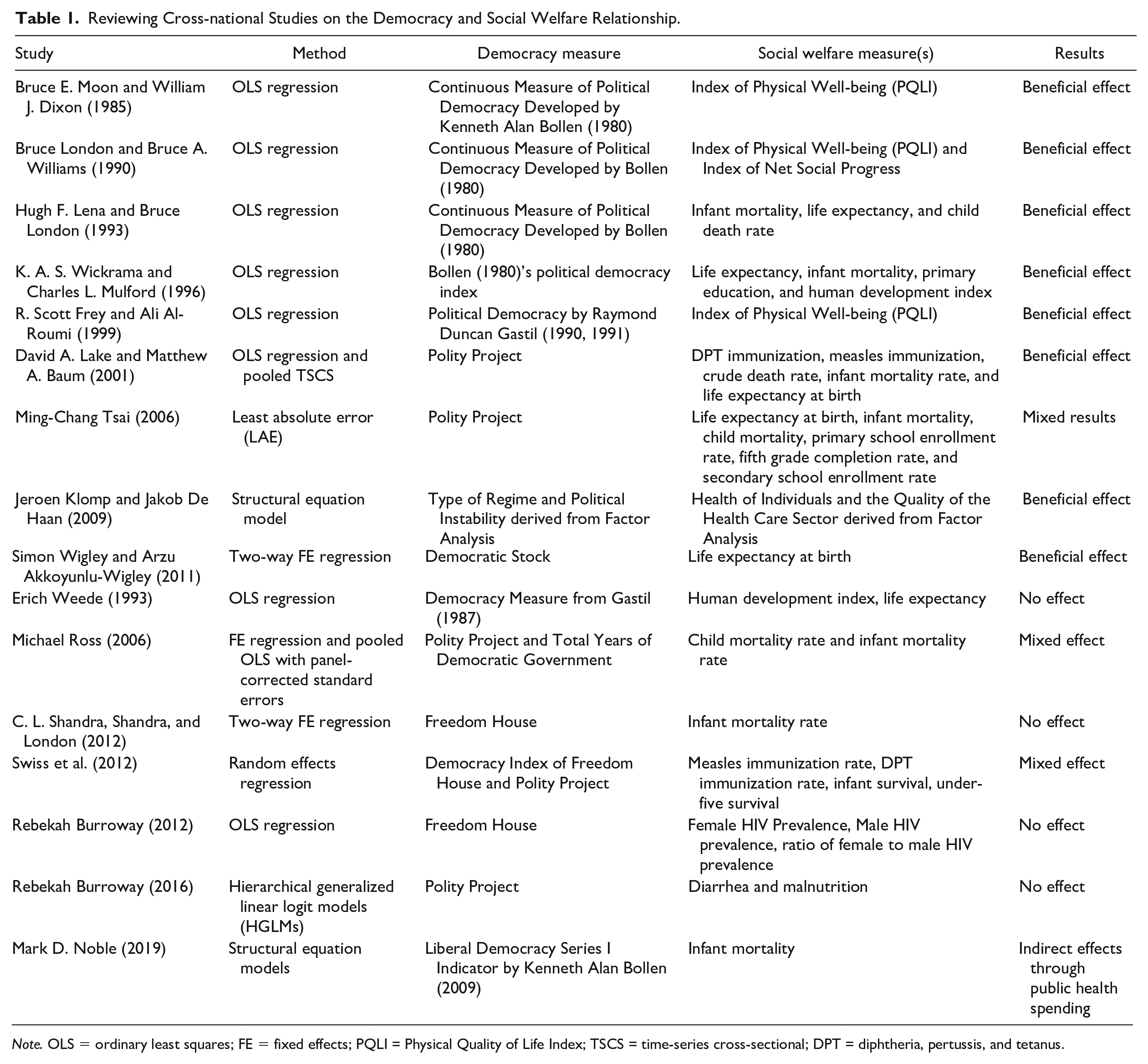
Note. OLS = ordinary least squares; FE = fixed effects; PQLI = Physical Quality of Life Index; TSCS = time-series cross-sectional; DPT = diphtheria, pertussis, and tetanus.
It is quite clear from Table 1 that many of the pioneering studies conducted during the 1980s and 1990s find that democracy exerts a beneficial effect on various forms of social welfare. Many of these studies used the continuous measure of political democracy developed by Kenneth Alan Bollen (1980), ordinary least squares regression, and the Index of Physical Well-being. Interestingly, with the incorporation of more powerful econometric methods such as FE estimation and random effects estimation, the substantial conclusions from the studies reported in Table 1 appear to be slightly more mixed than the general conclusions made from earlier decades. It is difficult to state what is at the root of these mixed findings for the studies conducted in recent years, but it is still important to note that these studies use slightly different measures of democracy and social welfare. Also, as with almost any scientific endeavor, there are limitations to many of these studies. I build on the important studies that have been conducted on the democracy-social welfare relationship in this analysis, as detailed in the introduction.
Theorizing Democracy and Health
Here, I theorize some of the ways in which democracy may impact health. The below theorization focuses on numerous aspects of democracy as defined by the varieties of democracy (V-DEM) data set: electoral democracy, liberal democracy, participatory democracy, deliberative democracy, and egalitarian democracy. The theoretical reasons described below suggest that each democracy index will exert a beneficial effect on health outcomes in less-developed countries.
I proceed in the following manner. First, I break down what each democracy index measures according to the V-DEM data set. Second, I touch on some reasons why these decomposed aspects of democracy may affect child mortality and infant mortality in developing countries.
Electoral Democracy
There are multiple principles of electoral democracy according to the V-DEM data set. One is the value of making rulers responsive to citizens through electoral competition for the electorate’s approval under circumstances when suffrage is extensive (Coppedge et al. 2021b). Also, political and civil society organizations can operate freely, while elections are clean and not marred by fraud or systematic irregularities (Coppedge et al. 2021b). Furthermore, elections affect the composition of the chief executive of the country (Coppedge et al. 2021b). Between elections, there is a freedom of expression and an independent media capable of presenting alternative views on political issues (Coppedge et al. 2021b).
This form of democracy can affect child mortality and infant mortality in developing countries through a variety of ways. It is assumed that politicians want to stay in political office or obtain political office (Ghobarah, Huth, and Russett 2004). Politicians are thus speculated to cater to the needs/demands of the population to garner political support (Frey and Al-Roumi 1999), where the needs/demands of the population can be social services that affect child and infant health. Indeed, numerous social scientific studies indicate that democracy is associated with increased social service spending (Avelino, Brown, and Hunter 2005; Baqir 2002; Brown and Hunter 2004; Kaufman and Segura-Ubiergo 2001; Przeworski et al. 2000), which has quite intuitive implications for child and infant health. Also, political candidates seeking to obtain political office or remain in political office can make promises to increase spending on social services, which can then affect child and infant health in developing countries (Lake and Baum 2001). Furthermore, politicians can face political consequences if they do not “follow up” on their campaign promises (Ruger 2005). The case of Uganda’s 1996 election gives some illustration as to how democracy may affect child and infant health in less-developed countries. Uganda president Yoweri Museveni promised increased access to education if re-elected (Stasavage 2005). Museveni then fulfilled his campaign promise shortly after winning re-election (Stasavage 2005).
Liberal Democracy
There are a few principles related to liberal democracy. In a nutshell, the quality of democracy from this index is evaluated by the limits placed on a government. Limits on an executive power can be achieved through constitutionally protected civil liberties, a strong rule of law, an independent judiciary, and effective checks and balances (Coppedge et al. 2021b).
Governments with less checks and balances are speculated to have less political incentive than democracies to meet the needs of their constituencies as politicians are chosen by political elites (Marshall and Gurr 2020). For example, autocratic policies may be more interested in portraying a positive impression to others than serving the needs of their population (Besley and Kudamatsu 2006; Ruger 2005). Furthermore, autocracies are in the position to repress demands for social services (Brown and Hunter 1999). Also, autocracies generally do not face oppositional parties that can “poke holes” in their policies (Ruger 2005). Autocracies may also repress media outlets and individuals that critique a government’s actions (Ruger 2005; Sen 1999). In sum, numerous processes partially tied to principles related to liberal democracy give some theoretical reasons to expect that this democracy index exerts a beneficial effect on child mortality and infant mortality in less-developed countries.
Participatory Democracy
The focus of the participatory democracy index is as follows. First, this index of democracy takes suffrage for granted and emphasizes engagement in civil society organizations, direct democracy, and subnational elected bodies. This index focuses on active participation by citizens in a political process, whether electoral or nonelectoral.
Citizens who are engaged in political and social issues affecting their country may learn about disease outbreaks, famine, and so forth, which can then affect child and infant health. Also, individuals being engaged with their elected officials may learn about their government’s policies that may impact health such as new initiatives to prevent child mortality. Increased participation of a country’s population in the political process can allow individuals to evaluate and protest a government’s policies (e.g. Sen 1999). Engagement in civil society and with elected bodies may allow for one to critique a government’s policies. Also, elected officials can inform voters of their campaign promises and how their proposals are better than the current government’s policies, which may generate additional resources that improve child/infant health. Furthermore, citizens may learn about diseases and other social services that can impact child and infant health with increased participation in political processes (Ruger 2005).
Deliberative Democracy
Deliberative democracy focuses on other aspects of democracy. This index focuses on the process by which decisions are reached in a polity. The V-DEM data set categorizes deliberative processes as one in which public reasoning focused on the common good motivates political decisions as opposed to, say, emotional appeals, scapegoating, or coercion. Furthermore, deliberative democracy requires that there is a respectful dialogue among informed and competent individuals who are open to persuasion at all levels (i.e., from preference formation to final decision).
Some potential ways in which this democracy index may impact health are quite intuitive. First, political decisions being motivated by improvements in the common good (i.e., improvements in the social and material conditions of the polity) rather than, say, scapegoating or appeals to emotions may affect the allocation of resources to poor communities, which then affects child mortality and infant mortality. Also, hostile dialogue between oppositional parties may detract from the successful implementation of policies that equally distribute resources to the citizens of a polity and acting on such policies.
Egalitarian Democracy
Egalitarian democracy also entails its own unique principles. This index of democracy posits that immaterial and material inequalities inhibit the exercise of formal rights and liberties and diminish the ability of citizens from all social groups to participate. Egalitarian democracy is achieved when rights and freedoms are protected equally across all social groups, resources are distributed equally across social groups, and groups and individuals enjoy equal access to power.
The reasons this form of democracy may impact the two response variables of interest in this analysis are also somewhat more intuitive than the other indices. First, resources being more equally distributed across social groups has clear implications for child health and infant health in developing countries, where resources are already quite scarce in the Global South and early deaths can for the most part be prevented with simple, cost-effective interventions. Thus, increased egalitarian principles in a polity should be inversely associated with child mortality and infant mortality in developing countries as increases in this aspect of democracy are associated with increases in the allocation resources and the ability for individuals with the ability to demand such resources from their government. Also, with increasing access to power, groups of individuals may be able to demand increased access to resources that impact child and infant health (medical services, social services, and so forth), which can then affect mortality rates (Sen 1999).
It is important to clarify certain aspects of the theorization on the democracy and health relationship in less-developed countries. First, it is important to recognize the theorization does not describe all the ways in which democracy may affect health outcomes in less-developed countries. Indeed, a potential relationship between democracy and health is incredibly complex. Second, the research design does not all for the parceling out of the exact ways in which democracy affects child mortality and infant mortality in less-developed countries. Thus, how democracy affects health in less-developed countries is beyond what I can infer from the statistical analysis I present here. In sum, there are numerous theoretical reasons to expect that democracy exerts a beneficial effect on child mortality and infant mortality in less-developed countries.
Summary of Propositions
I derive the following propositions from the above discussion.
I now turn to a description of the analysis, where I describe the data set, the sample, the response variables, explanatory variable of interest, control variables, and methodological approach used to assess the effect of democracy on child mortality and infant mortality in less-developed countries. I then summarize the results of the analysis in the Results section. I then discuss the significance of the results in the discussion and conclusion section.
The Analysis
Data Set
I analyze unbalanced country-level cross-sectional longitudinal data in this analysis. I gather the country-level panel data from three sources. The first source of data is the Union of International Association’s Yearbook of International Organizations (UIA 1990–2016). 2 The Union of International Association’s Yearbook of International Organizations data provide the data on INGOs. The second source of data is the V-DEM data set (Coppedge et al. 2021a). The rest of the country-level data are from the World Bank’s World Development Indicators (World Bank 2020). Developing countries are identified if they are not classified as high-income in the World Bank’s income classification of countries, which is a commonly used way to identify developing countries in the comparative international social sciences (e.g., Mejia 2021a, 2021b). The appendix lists the countries included in each analysis. Table 2 reports the descriptive statistics and Table 3 reports the correlation matrix for the analyses.
Descriptive Statistics.
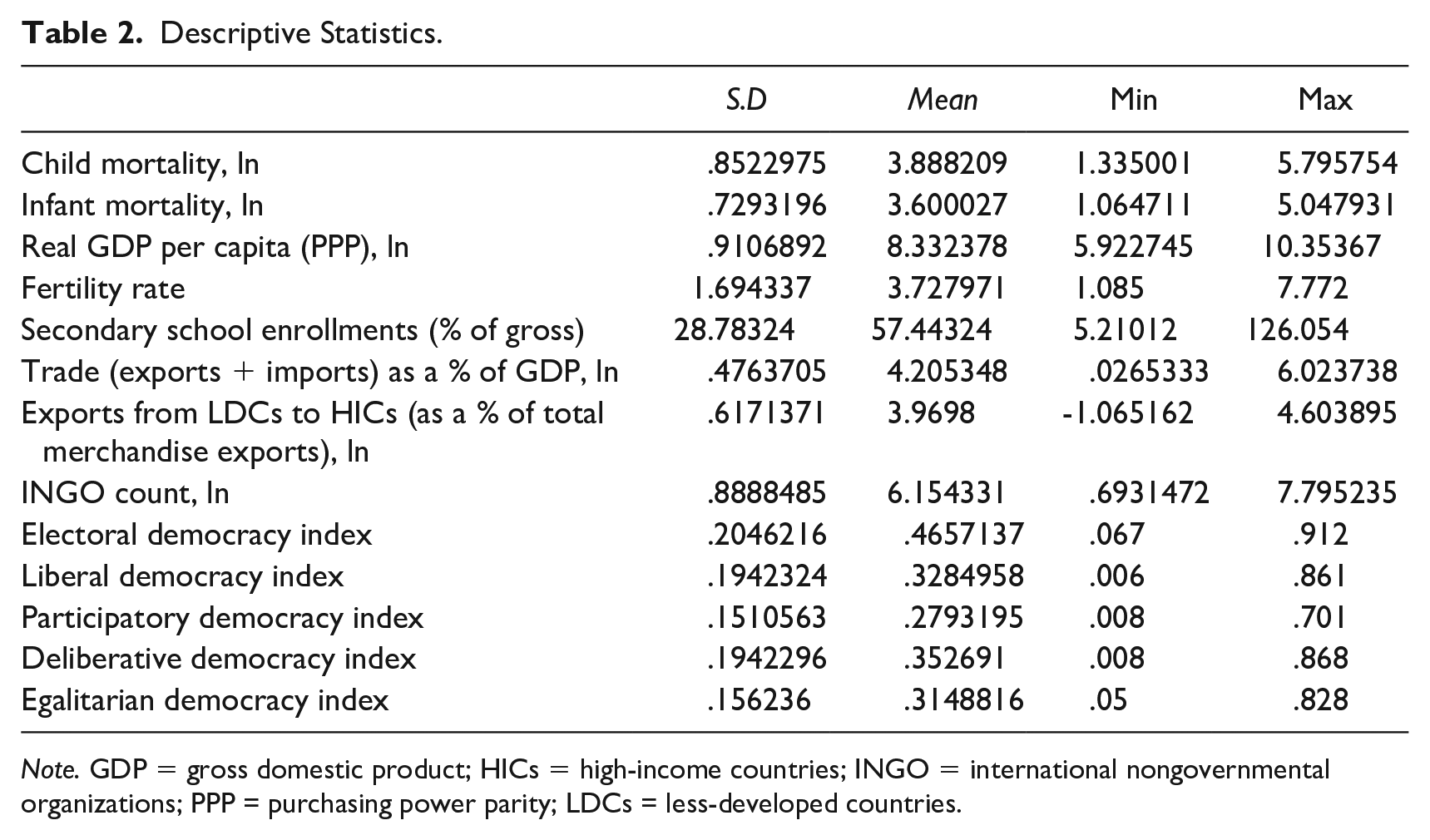
Note. GDP = gross domestic product; HICs = high-income countries; INGO = international nongovernmental organizations; PPP = purchasing power parity; LDCs = less-developed countries.
Correlation Matrix.
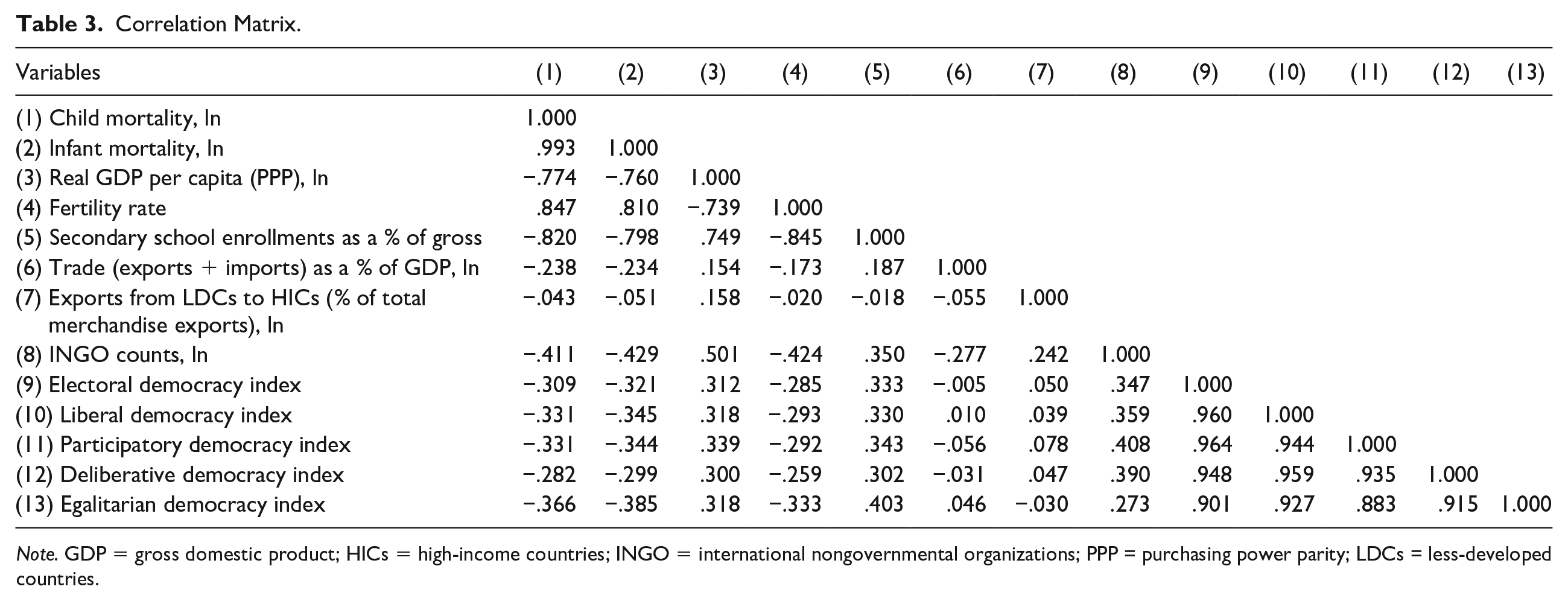
Note. GDP = gross domestic product; HICs = high-income countries; INGO = international nongovernmental organizations; PPP = purchasing power parity; LDCs = less-developed countries.
Response Variables
Child mortality and infant mortality
I analyze two response variables in this analysis. The first response variable is the natural logarithm of a country’s child mortality rate (per 1,000 live births). I take the natural logarithm of this variable to address excessive skew. The child mortality rate is the number of deaths that occur in a given country before an individual reaches the age of five. The second response variable is the infant mortality rate (per 1,000 live births). I take the natural logarithm of this variable as well to account for excessive skew. The infant mortality rate is the number of deaths that occur in a given country before an individual reaches the age of one.
Explanatory Variables of Interest
Democracy
I measure democracy using the five democracy indices from the V-DEM data set. The five democracy indices are electoral democracy, liberal democracy, participatory democracy, deliberative democracy, and egalitarian democracy. I touch on these explanatory variables in the theory section above, but I refer readers to the V-DEM codebook at (https://www.v-dem.net/) for an even more in-depth description of these democracy indices.
Other Relevant Explanatory Variables
Economic development
I measure economic development as the natural logarithm of real GDP per capita (PPP) in 2011 international dollars. Controlling for economic development is quite common in the comparative international social sciences. Also, modernization theory (e.g., Rostow 1960) would posit that economic development exerts a beneficial effect on health outcomes in developing countries as economic development can affect standards of living. Also, Glenn Firebaugh and Frank D. Beck (1994) posit that economic development is positively associated with wages, which can then affect health outcomes in developing countries. The relationship between economic development and health is one of the most established relationships in the comparative international social sciences (e.g., Brady, Kaya, and Beckfield 2007; Clark 2011; Firebaugh and Beck 1994; J. M. Shandra et al. 2004, 2005).
Fertility
I also control for a country’s total fertility rate, which is the number of children that would be born to a woman if she were to live to the end of her childbearing years and bear in accordance to age-specific mortality rates of the specific year (World Bank 2020). I posit that fertility is positively associated with child mortality and infant mortality as increased in fertility, especially in a resource-scarce environment, might be associated with decreased resource consumption per individual, which could then affect the mortality measures I focus on here (Kentor 2001; London 1988; Shen and Williamson 1999).
Secondary school enrollments
I also control for a country’s secondary school enrollments as a percentage of gross. Controlling for secondary school enrollments is quite common when investigating health outcomes. Also, gender stratification theory posits that education exerts a beneficial effect on health outcomes in developing countries as education can signify a woman’s status/autonomy in less-developed countries (e.g., Mason 1986). Education may also affect fertility, which can then decrease mortality rates (Caldwell 1979). Furthermore, cross-national research finds education exerts a beneficial effect on health outcomes (e.g., Burroway 2012; J. M. Shandra et al. 2004, 2005). I expect to find similar results here. 3
Trade openness and exports to HICs
I also include a measure of trade openness and exports to HICs. Trade openness is measured as trade (exports + imports) as a percentage of GDP. Exports to HICs is measured as exports to HICs as a percentage of total merchandise exports. Both variables are log transformed to account for excessive skew. Classical economics scholarship (e.g., Ricardo 1817) posits that trade is inversely associated with economic growth, thereby reducing mortality in developing countries as such countries pursue their comparative advantage (Ricardo 1817). World-systems analysis (e.g., Chase-Dunn 1989; Wallerstein 1974, 2004) and dependency theory (A. G. Frank 1967, 1978) would posit that trade is associated with decreased economic growth, thereby affecting child mortality and infant mortality in less-developed countries.
World society embeddedness
I also include a measure of world society embeddedness (e.g., Boli and Thomas 1999; Meyer et al. 1997). I measure world society embeddedness as the count of INGOs that report having members in a given country. 4 Measuring world society embeddedness in the aforementioned way is quite common in the comparative international social sciences (e.g., Boli and Thomas 1999; D. J. Frank, Longhofer, and Schofer 2007; Hironaka 2014; Mejia 2020, 2021c). I take the natural logarithm of this variable to account for skew. I posit world society embeddedness is inversely associated with child mortality and infant mortality in less-developed countries. I posit such a relationship for multiple reasons. One is that there is discourse at the global level around the issue of mortality and health more generally (e.g., Chabbott 2002, 2014). Health and mortality are generally identified as issues in the international community. Nation-states and international organizations are some of the major actors tasked with addressing such issues (e.g., Chabbott 2014; D. J. Frank, Hironaka, and Schofer 2000). The aforementioned actors are also embedded in larger social structures where they are expected to make “progress” toward such issues, despite the development level of a country (e.g., Meyer and Rowan 1977). In a nutshell, INGOs may pressure nation-states to allocate more funding to social services by informing domestic activists and intergovernmental organizations of nation-state failures (Murdie and Hicks 2013). Furthermore, INGOs may directly provide funds to individuals (Sparr and Moser 2007). Overall, there are numerous theoretical reasons to expect that INGOs exert a beneficial effect on child mortality and infant mortality in developing countries.
Methodological Approach
In this analysis, I use FE panel regression models to address unobserved heterogeneity (

where


where lambda
Results
I report the analysis results in Tables 4 and 5. I report six models in each table. Model 1 is treated as a simple baseline model, which consists of the real GDP per capita, fertility, secondary school enrollments, trade, exports from LDCs to HICs, and the INGO count measure. Models 2 through 6 consist of the predictor variables included in Model 1 plus one of the democracy indices.6,7 In each model, I report the constant and the number of observations. Unstandardized coefficients are presented first, while heteroskedasticity-robust standard errors clustered by country are enclosed in parentheses. I also provide the values of R2 within as FE models focus on variation within-cases.
Unstandardized Coefficients from the Regression of Child Mortality (ln) on Selected Explanatory Variables: Fixed Effects Panel Regression Models of 95 Developing Countries, 1990–2016.
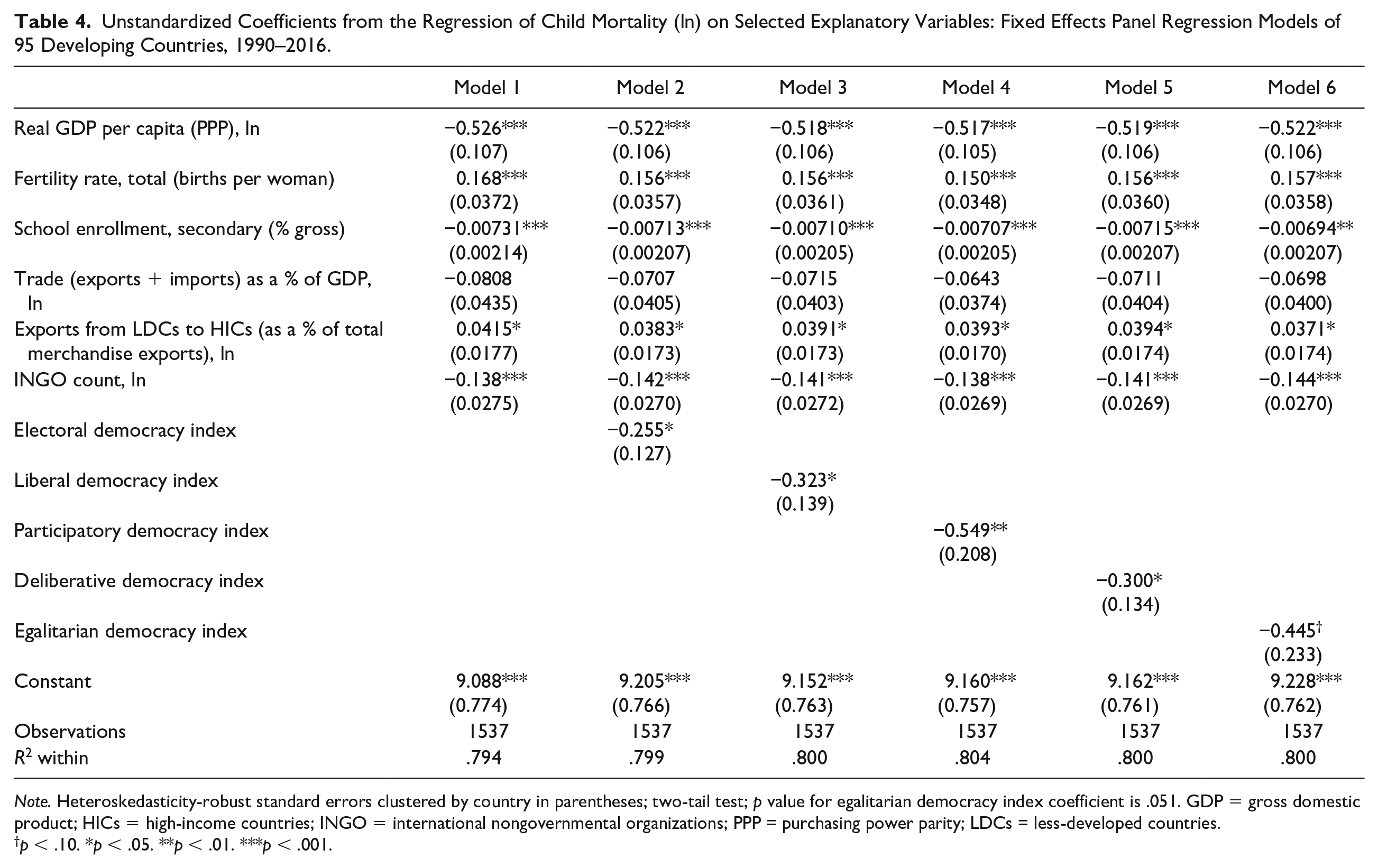
Note. Heteroskedasticity-robust standard errors clustered by country in parentheses; two-tail test; p value for egalitarian democracy index coefficient is .051. GDP = gross domestic product; HICs = high-income countries; INGO = international nongovernmental organizations; PPP = purchasing power parity; LDCs = less-developed countries.
p < .10. *p < .05. **p < .01. ***p < .001.
Unstandardized Coefficients from the Regression of Infant Mortality (ln) on Selected Explanatory Variables: Fixed Effects Panel Regression Models of 95 Developing Countries, 1990–2016.
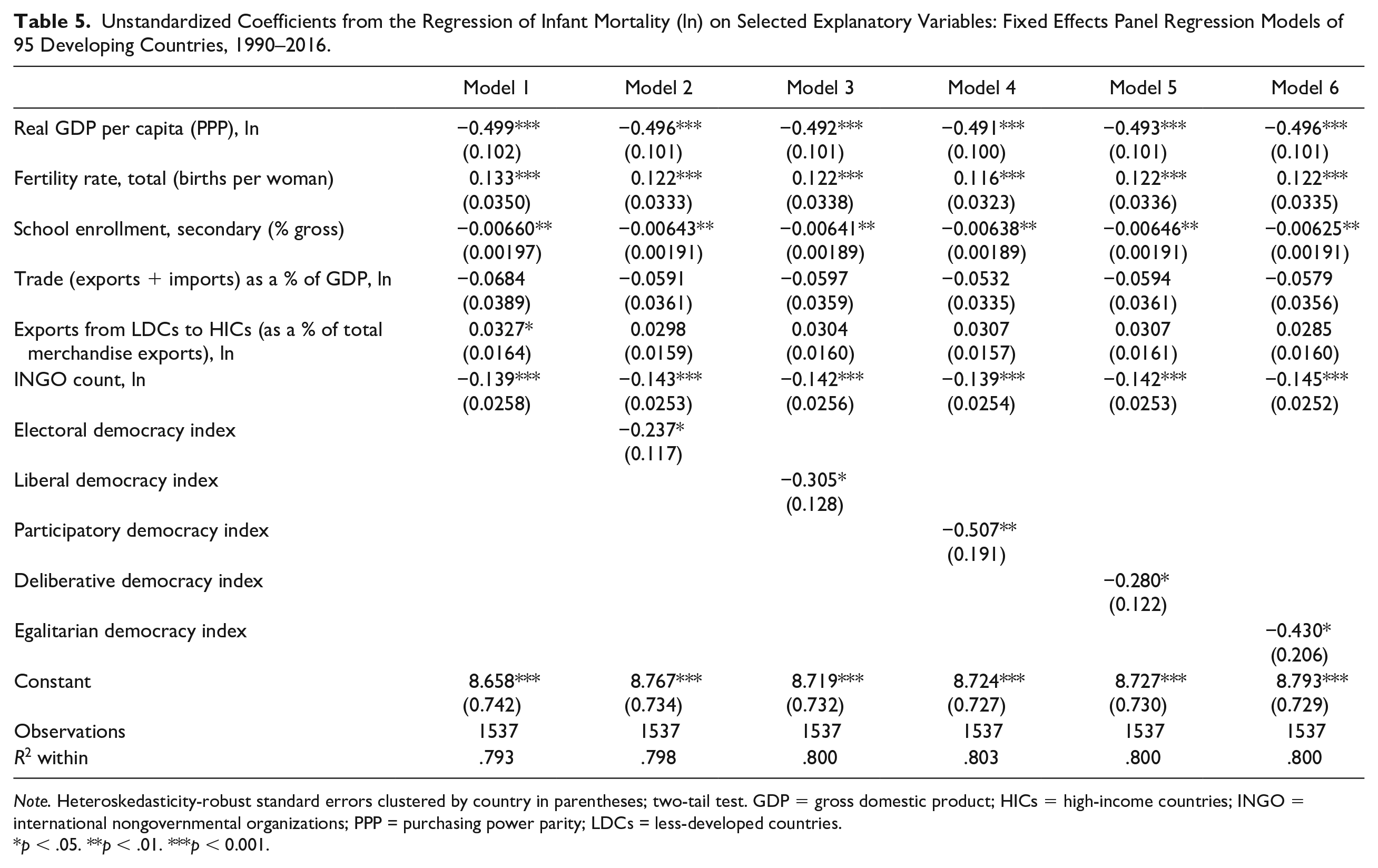
Note. Heteroskedasticity-robust standard errors clustered by country in parentheses; two-tail test. GDP = gross domestic product; HICs = high-income countries; INGO = international nongovernmental organizations; PPP = purchasing power parity; LDCs = less-developed countries.
p < .05. **p < .01. ***p < 0.001.
Findings for the child mortality analyses are reported in Table 4. The unstandardized coefficients for real GDP per capita are, as expected, negative in direction and statistically significant across all the reported models in Table 4. Also as expected, the coefficients for total fertility rate are positive in direction and statistically significant across all the relevant models. Secondary school enrollments exerts a consistent statistically significant beneficial effect on child mortality in Models 1 through 6. The coefficients for the trade openness measure do not reach statistical significance in the models this variable is included in. However, exports from LDCs to HICs consistently exerts a significant harmful effect on child mortality. The unstandardized coefficients for INGO counts are negative in direction and statistically significant in all of the relevant models of Table 4. Similarly, each democracy index exerts a significant beneficial effect on child mortality in the models reported in Table 4. The p-value for the egalitarian democracy index unstandardized coefficient is .051.
Table 5 reports the findings for the infant mortality analyses. I consistently find that economic development exerts a statistically significant beneficial effect on infant mortality, although this is not too surprising. Fertility consistently exerts a statistically significant positive effect on infant mortality across Models 1 through 6. As expected, the unstandardized coefficients for secondary school enrollments are negative in direction and statistically significant across all the models reported in Table 5. The coefficients for trade openness and exports to HICs do not consistently reach statistical significance in the models I report in Table 5. INGOs exert a statistically significant negative effect on infant mortality in the models reported in Table 5. Furthermore, each democracy index is found to be inversely associated with infant mortality in developing countries.
Discussion and Conclusion
In this analysis, I help advance the comparative international literature that investigates the impacts of democracy on health outcomes. Foremost, I theorized some of the ways in which democracy can impact health outcomes in developing countries, with particular attention to specific aspects of democracy such as electoral democracy, liberal democracy, participatory democracy, deliberative democracy, and egalitarian democracy. I then derived a proposition from the theorization, which is that each of these aspects of democracy will be inversely associated with child mortality and infant mortality in developing countries. To evaluate the theorization, I estimate the effect of five democracy indices from the V-DEM data set on child mortality and infant mortality in developing countries using FE panel regression models with heteroskedasticity-robust standard errors clustered by country. Results from FE regression models indicate that each democracy index exerts a statistically significant beneficial effect on child mortality and infant mortality in developing countries, net of statistical controls.
The analysis makes numerous contributions to the comparative international social scientific literature and the social sciences more broadly. Without a doubt, a debate that has intensified in recent years is the democracy and health relationship in comparative international context. Over the past decades, scholarly understanding of the democracy and health relationship seemed to be quite solidified as a plethora of empirical scholarship found that democracy exerts a beneficial effect on health outcomes (e.g., Besley and Kudamatsu 2006; Frey and Al-Roumi1999; Klomp and De Haan 2009; Lake and Baum 2001; Lena and London 1993; London and Williams 1990; Moon and Dixon 1985; Tsai 2006; Wickrama and Mulford 1996; Wigley and Akkoyunlu-Wigley 2011; Young 1990; Zweifel and Navia 2000). A growing body of scholarship challenges our scholarly understanding of the effects of democracy on health outcomes in comparative international context (Burroway 2012, 2016; Noble 2019; Ross 2006; C. L. Shandra et al. 2012; Swiss et. al. 2012; Weede 1993; Wejnert 2008). I contribute to this debate by providing new estimates of the effects of democracy on child mortality and infant mortality in developing countries, where I consistently find that democracy exerts a beneficial effect on child mortality and infant mortality in developing countries, which helps to further solidify our social scientific understanding of the democracy and health relationship in comparative international context.
There is another key contribution stemming from this analysis. I also extend the democracy and social welfare literature by evaluating the effects of more nuanced aspects of democracy than much of the previous literature by incorporating the V-DEM democracy indices (Coppedge et al. 2021a). I find that even more specific aspects of democracy, as measured by the V-DEM democracy indices, continue to impact health outcomes in less-developed countries. Thus, even more specific aspects of democracy such as egalitarian democracy and deliberative democracy are associated with decreases in child mortality and infant mortality in developing countries, net of statistical controls. The incorporation of these democracy indices suggests that the ways in which democracy affects health outcomes are more diverse than previously thought, where increases in principles related to egalitarian, liberal, participatory, deliberative, and egalitarian democracy are inversely associated with child mortality and infant mortality in developing countries. Overall, it is the author’s hope that the findings presented here spark further scholarly discussion regarding the effects of democracy on health outcomes as additional research is needed to give even further confidence to the results I present here or contradict them.
There are other important findings to discuss. First, I consistently find that economic development exerts a beneficial effect on child mortality and infant mortality. There are debates whether the effect of economic development on child mortality and infant mortality in developing countries decreases, increases, or remains stable over time (e.g., Brady et al. 2007; Clark 2011; Firebaugh and Beck 1994). However, I find that economic development exerts a statistically significant beneficial effect on both health measures I focus on in this analysis, which gives even further confidence to our social scientific understanding of the economic development and health nexus. I also find that fertility exerts a statistically significant harmful effect on child mortality and infant mortality in developing countries, which makes intuitive sense and is quite consistent with the findings of previous cross-national research. I also observe a significant inverse relationship between education and both response variables I focus on in this analysis, which contributes to previous comparative international studies that find similar relationships (e.g., Caldwell 1979; J. M. Shandra et al. 2004, 2005) Overall, it is quite clear that there are a variety of unique intranational processes affecting child mortality and infant mortality in less-developed countries.
The results also indicate that global cultural processes also affect child mortality and infant mortality in less-developed countries rather than aspects related to global political-economy. I consistently find that INGOs exert a statistically significant beneficial effect on child mortality and infant mortality in developing countries, which is quite consistent with the theoretical predictions of world society theory (e.g., Boli and Thomas 1999; Meyer et al. 1997). Also, with this analysis incorporating even stronger econometric methods to analysis cross-section and longitudinal data than previous studies on the effects of global culture on social welfare outcomes (e.g., J. M. Shandra, Shandra, and London 2010), I provide even stronger empirical support for the theoretical expectations of world society theory (e.g. D. J. Frank et al. 2000). It is also evident from this analysis that unique aspects of the world economy such as the vertical flow of exports from LDCs to HICs affects specific health outcomes.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.