
Abstract
Objective
Emergency telepsychiatry programs have demonstrated value in urban settings but remain under-studied in terms of their impact on access and flow. This pragmatic study assessed patients seen by a novel emergency telepsychiatry service over 4 years in Winnipeg, Canada, during a time of rapid system change. Outcomes were compared to a cohort of hospitalized individuals who received an in-person emergency psychiatric assessment during the same time period.
Method
Telepsychiatry assessments between January 1, 2018 and December 31, 2021 were logged and linked with administrative data to examine variables pre-consult, during the episode of care, and post-consult. For individuals admitted to hospital following the telepsychiatry assessment, we generated a comparison group of individuals admitted following in-person consult at the eligible sites. Emergency Department length of stay (ED LOS), hospital admission diagnosis and days in hospital were compared between groups.
Results
A total of 558 telepsychiatry consults were logged during the study period of which 520 (93.1%) were successfully linked to administrative data. The volume of telepsychiatry consults decreased over time in parallel with changes to in-person staffing and referring facility designation. Rate of admission following the telepsychiatry assessment was 50% or lower across all years. For comparison, 222 telepsychiatry and 756 in-person visits resulting in psychiatric hospital admission were identified. Telepsychiatry-triggered hospitalizations were more likely to be for individuals presenting during daytime (0801–1700 h) and with mood/suicidal chief complaints at triage (P < 0.001). No differences in overall ED LOS, admission diagnosis, or days in hospital were observed.
Conclusion
Telepsychiatry services in urban ED settings have the potential to offer access to timely consults in the absence of in-person care. This model can optimize resources and offer flexibility in the face of rapidly evolving and unanticipated health system changes.
Introduction
Over the past several years, Emergency Departments (EDs) in Canada have witnessed an immense surge in demand, outpacing available resources and personnel. 1 Contributory factors include a rise in psychiatric emergencies, which are also presenting as increasingly complex. 2 With gaps in community mental health systems, availability of personnel and fragmented referral pathways, the ED is often the primary and only access point for acute psychiatric distress.3–5
Concurrently, the use of emergency telepsychiatry has been growing worldwide to address lack of access to timely assessment,6,7 including an example in rural Ontario offering child and adolescent emergency assessments since at least 2015. 8 During the COVID-19 pandemic, there was a rapid rise in uptake of telepsychiatry amid concerns of viral transmission and heightened public anxiety.9–11 While rural emergency telepsychiatry programs have been shown to have positive impacts on access, equity, and cost-savings through reduced wait times, 12 as well as decreased transfer out of the home community when not required, 13 there has been less study of urban-based emergency telepsychiatry programs. 14
Urban EDs, despite greater concentration of psychiatric specialists, have distinct challenges, including a rising volume of psychosocially complex presentations and high rates of repeat visits.15,16 ED wait times and length of stay for mental health visits are significantly longer than for other ED patients. 17 There may also be unique facilitators of emergency telepsychiatry in urban centres compared to rural including a more conducive infrastructure for its use such as established clinical networks allowing rapid referrals, broader access to interpreters, and better technical support. 14 There remain implementation challenges, however, including licensure regulations and inconsistent reimbursements by insurance providers in some jurisdictions.14,18
To address limited access to in-person psychiatry in some North American urban centres, emergency telepsychiatry programs have been established with positive results. For example, North Carolina in the United States has a statewide emergency telepsychiatry program, which has been found to decrease cost to the system and to improve outcomes.19,20 Similarly, an emergency telepsychiatry program in an urban pediatric satellite community ED in the United States, attached to a large tertiary hospital, demonstrated a substantial decrease in median ED length of stay from 473 to 275 min. 21 Locally in Canada, emergency telepsychiatry models in Winnipeg 22 and New Brunswick 9 have been described as solutions to maintain psychiatric coverage in smaller community hospitals.
Despite growing acceptance, the evidence for the effectiveness of emergency telepsychiatry in the urban context remains lacking and is inconsistent, with large variability in models and little evaluation of Canadian programs. A recent scoping review 23 summarized 11 studies internationally on telepsychiatry consultation occurring in a mix of rural and urban ED settings, with approximately half of the studies involving hybrid models consisting of a mix of in-person and remote psychiatry coverage. Most studies supported that telepsychiatry reduced waiting time but had variable impact on total length of stay and hospital admission. 23 A second review that focussed on more recent publications only (2019–2021), again in a combination of rural and urban ED settings, found more homogenous favourable impacts on all outcomes. 24
In late 2017, we established the emergency telepsychiatry program in urban Winnipeg, Canada, to support several general hospitals serving individuals presenting with acute mental health needs where there was variable in-person psychiatric coverage. 22 Prior to the introduction of this program, patients were frequently transferred between sites within the city for emergency psychiatric assessment leading to unnecessary healthcare spending and critical incidents. The telepsychiatry program successfully sustained and continued through the COVID-19 pandemic, rapidly adapting to unique contextual changes along the way.
This pragmatic study examined the utilization of the hub-based emergency telepsychiatry program in Winnipeg across 3 sites over 4 years. It further examined patient characteristics and compared service outcomes for a subgroup of individuals hospitalized from the ED, comparing those assessed via telepsychiatry and those seen in-person by a psychiatrist in the ED. We hypothesized that telepsychiatry assessments would address a service gap created by the absence of in-person psychiatry coverage and that admission outcomes would be comparable to those assessments done in-person. Expanding the available data on how these models can integrate and perform within existing systems, especially within a Canadian context, is needed within the expanding literature and to inform how these models may be adopted as a solution to enhance access to emergency psychiatric care.
Methods
Study Design and Setting
This was a retrospective study using linked data obtained from administrative databases housed at the Manitoba Centre for Health Policy (MCHP) and a case list from the emergency telepsychiatry program operating in Winnipeg, Manitoba. A pragmatic approach was adopted due to rapidly changing system factors over the course of the evaluation and the resultant need to focus on real-world performance of the program.
Winnipeg's health authority operates 6 hospitals with Emergency and Urgent Care (UC) programs, as well as a single 24-h mental health walk-in Crisis Response Centre (CRC) accessible to adults living in and around the Winnipeg area (total population of approximately 749,607 (2021)). 25 Since 2016, several changes have been made to these sites in efforts to consolidate clinical pathways in the city, including closing psychiatric inpatient units at 2 hospitals resulting in reduced availability of psychiatric support to the EDs in those facilities.
In response to changes in the availability of in-person emergency psychiatric care at some of the smaller centres, we implemented an emergency telepsychiatry program in December 2017 that operated out of the CRC hub which is staffed 0800–2100 h by a Psychiatrist with Physician Assistant (PA), Psychiatry Resident and medical student support. 22 During the hours of operation, a psychiatrist is on site at the CRC to receive the consult requests from the referring site via telephone call and then supervises the team of PAs and trainees conducting independent or accompanied assessments depending on the clinical presentation. Any individual requiring a psychiatric assessment is suitable for referral, the only exclusion being that they cannot safely participate due to a high level of agitation. In rare situations, individuals are held for the in-person psychiatrist to see when available, or transferred to an alternative site that has in-person psychiatry available at all times. After hours, suitable individuals are held overnight for a consult to occur the next day.
The telepsychiatry program rolled out sequentially between December 23, 2017 and October 1, 2018, to three hospital sites in the city. Site A had no psychiatry inpatient unit, and sites B and C had recently closed inpatient units resulting in no or variable in-person psychiatry coverage in the ED. Where sites retained in-person psychiatry coverage in the ED, it was often divided between the ED and the hospital's medical and surgical units or could be restricted to assessment of mental health act presentations given limited availability. In 2019, sites A and C converted from EDs to UC centres that shifted towards lower acuity presentations. Public campaigning through media and the health authority's website, alongside ambulance and police transport protocols supported patients presenting to the correct site based on care needs, albeit not always with perfect precision. Concurrently, Site B was seeing higher acuity as it remained an ED and expanded in-person psychiatry hours were implemented. Additionally, the COVID-19 pandemic was declared in Manitoba in March 2020, which resulted in an initial reduction in visit volumes at the referring sites (see Figure 1 for a summary of the health system changes and coverage arrangements across the years of study).
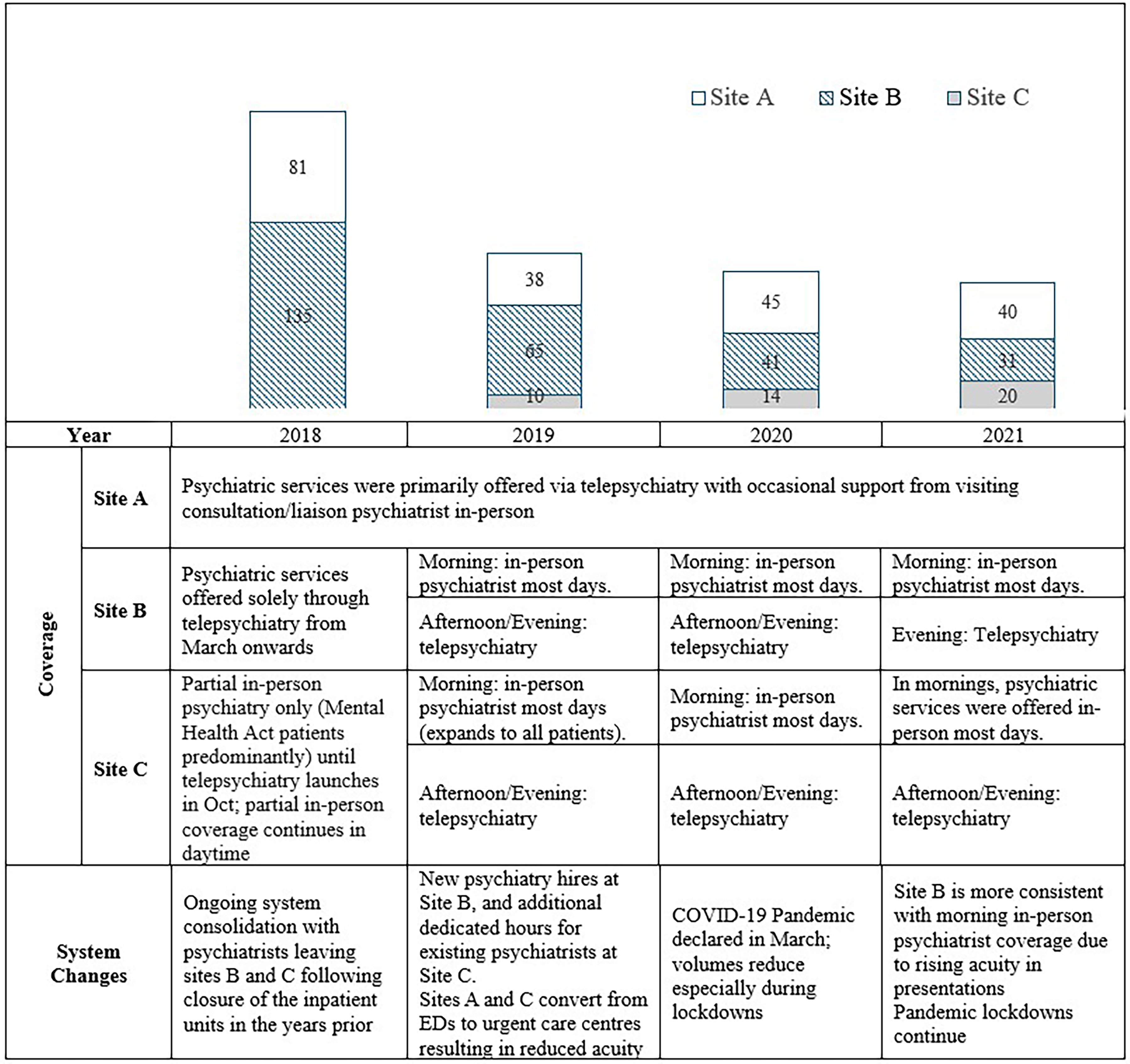
Annual rates of telepsychiatry consultation presented by site, with corresponding psychiatry coverage details and major health system changes (2018–2021).
This study included all individuals who received an emergency telepsychiatry assessment between January 1, 2018 and December 31, 2021. A comparison group of individuals who received in-person psychiatric assessments during this time was created but limited to the cohort of individuals who were hospitalized under psychiatry following the assessment due to the inability to identify cases seen by psychiatry from ED records alone.
Data Sources and Linkage
We used a case list generated by the emergency telepsychiatry program, representing all assessments completed during the study period. A file containing case identifiers and telepsychiatry assessment details was securely shared with Manitoba Health to de-identify the records by encoding the information into a format linkable to administrative data records housed at the MCHP. MCHP is an affiliate of the University of Manitoba in Manitoba, Canada housing de-identified data which are linked by an encrypted Personal Health Information Number with >95% linkage accuracy.26,27
All individuals in the program case list with a valid Manitoba Health card in the 1-year prior and 30 days following the index visit were linked to the databases at MCHP, including the Manitoba population registry containing demographic information, Emergency Department Information System (EDIS) which includes information on use of emergency services (all ED and UC centres) in Winnipeg, and Canadian Institute for Health Information-Discharge Abstract Database (CIHI-DAD) for hospital admission data. In addition to ED visits in EDIS, we extracted and linked visits from the CRC Clinical Health Record to be inclusive of crisis mental health visits that occurred at the CRC post-telepsychiatry assessment, since these data are not included in the MCHP repository. Note that the use of ED from here forward as it relates to the data descriptions refers to both EDs and UC centres.
Ethics Approvals
Approvals for this study were obtained from the University of Manitoba Research Ethics Board (HS25759) and the Provincial Health Research Privacy Committee (PHRPC) (P2022-125).
Variables
Demographic data included age at time of index visit, sex and neighbourhood income quintile derived from census data. Index visit variables included date of visit, time of visit (grouped into midnight-0800 h, 0801–1700 h, 1701-midnight), site, main complaint at triage (grouped as psychosis, mood/suicidal, anxiety/crisis, substance use, medical), Emergency Department length of stay (ED LOS) and outcome (discharge, admission to psychiatry). Prior health care utilization included ED visits in 30 days prior to index visit, and psychiatric hospitalizations in the 1-year prior. For those hospitalized, we captured admission diagnosis, mental health act status at time of admission, length of hospitalization in days, and whether discharge was planned for or occurred against medical advice. For those discharged, we captured 72-h, and 30-day repeat crisis visits (ED or CRC). Admission diagnoses were based on the CIHI-DAD primary diagnosis categorized as Mood/anxiety disorder/suicide attempt: ICD-10-CA F30-34, F38, F40, F41.0-41.3, F41.8, F41.9, F42, F43, F53.0, X44, X46, X57, X60-X84, T39, T40, T42.3, T42.4, T42.7, T43, T50.9, T58; Substance use disorder: ICD-10-CA F10-F19, F55, Z50.2, Z50.3; Psychotic disorder: ICD-10-CA F11.5, F12.5, F13.5, F14.5, F15.5, F16.5, F18.5, F19.5, F20, F22-25, F28, F29; Personality disorder: ICD-10-CA F21, F60, F61, F62, F69; Other mental disorder: anything ICD-10-CA F00-F99 not covered in other categories.
Comparison Group
A comparison group of individuals hospitalized to a psychiatry inpatient unit following an ED visit at one of the telepsychiatry sites was created. Those not in the telepsychiatry group were assumed to have been seen in-person in the ED or via transfer to another site for an in-person assessment prior to being admitted.
Data Analysis
All telepsychiatry cases were analyzed descriptively by year. Demographic, visit and outcome data were compared between the telepsychiatry, and in-person consult groups. Categorical variables were examined using Chi-square tests. Continuous variables were compared using Students t-test. Hospital and ED lengths of stay were compared using negative binomial regression and are presented as crude and adjusted relative differences, a relative difference of 1 indicating no difference. Variables adjusted for included hospital site, age group, low versus high income (income quintiles 1–2 vs. quintiles 3–5), time of day of ED presentation, sex, presenting complaint at triage, number of previous hospital admissions in the year prior, and the year of admission.
Results
There was a total of 558 telepsychiatry consults logged during the study period. Of these, 520 consults for 469 unique individuals were successfully linked (93.2%). As seen in Table 1, consult volume was highest in 2018 (n = 221) and lowest in 2021 (n = 91), in keeping with changes to psychiatric coverage over these years. Patterns in volumes by site were consistent with clinical consolidation and changes in psychiatry coverage that occurred. Individuals seen had a mean age of 38.9 years overall (95% CI 37.5, 40.3), with a high proportion of females, distributed across all income quintiles with higher representation among the lowest income group. A range of 7.2–11% of persons per year had an ED visit within the previous 72 h, and 14–22% had an ED visit between 72 h and 30 days prior to the consult occurring, indicating a group with high recurrent use of ED services. Similarly, in 3 of the 4 years, over 25% of the cases had a psychiatric hospitalization in the year prior, with rates being highest in 2020. Most presentations occurred during daytime hours, with chief complaints most frequently related to mood or suicidal concerns. Psychosis was not an uncommon complaint as were medical issues which featured neurological and cardiac concerns predominantly. Of note, these medical complaints were much more frequent in 2020 and 2021 during the peak of the COVID-19 pandemic.
Demographics, Prior Health Care Use, and Visit Details for Telepsychiatry Consults (n = 520). Percentages are for Each Year, Reported by Column.
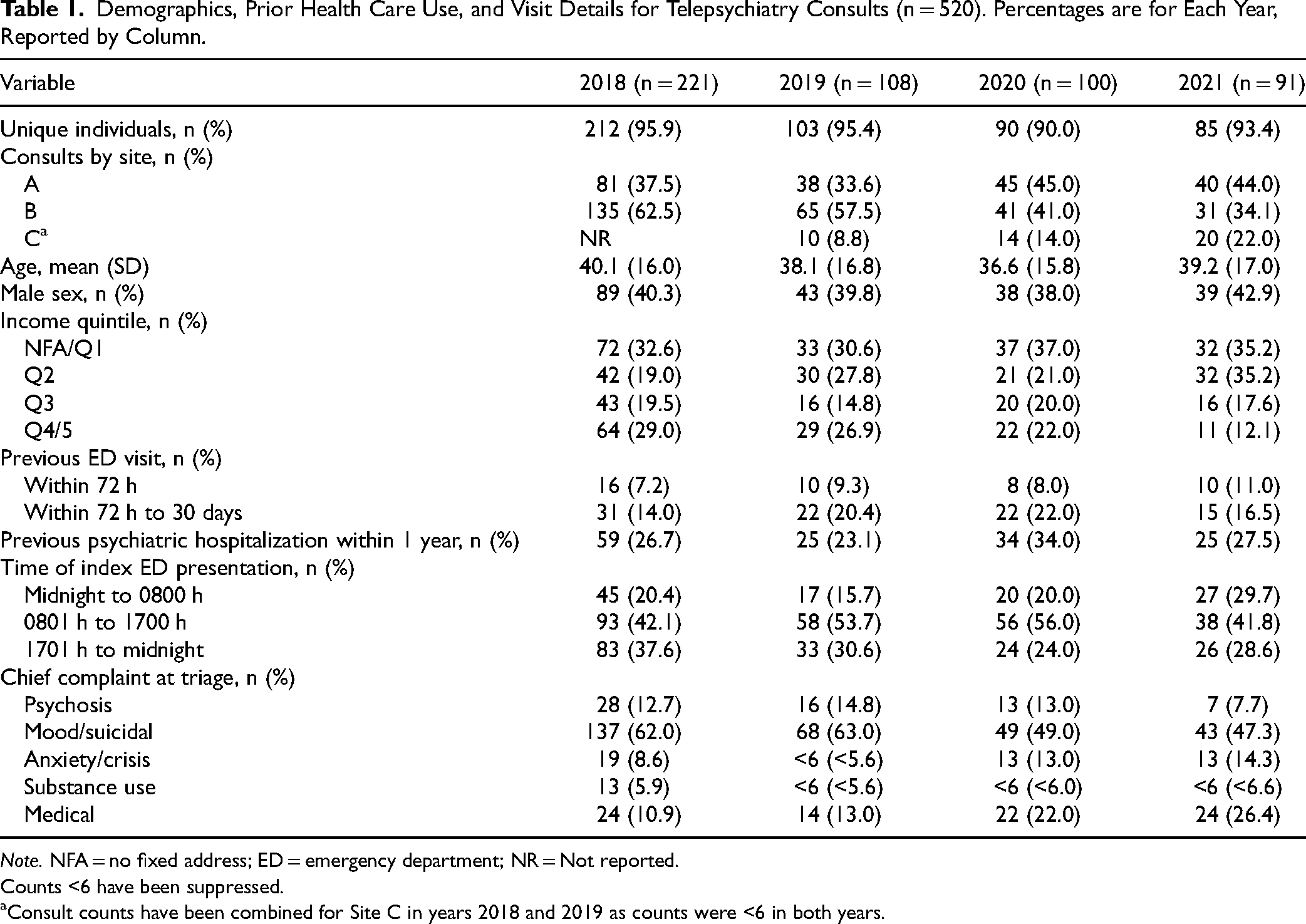
Note. NFA = no fixed address; ED = emergency department; NR = Not reported.
Counts <6 have been suppressed.
aConsult counts have been combined for Site C in years 2018 and 2019 as counts were <6 in both years.
In Table 2, time to psychiatry assessment appears to be fairly stable, whereas total time in the ED, hospitalization rates and repeat visit rates fluctuate more from year to year. In total, across all years, 25 (10.2%) assessments for individuals who were not directly admitted to hospital following the telepsychiatry consult (n = 245) resulted in a repeat presentation within 72 h of the ED visit that involved the telepsychiatry consult. This was not examined by year due to small cell counts. Thirty day repeat visit rates, inclusive of any ED, UC or the CRC were lowest in 2019 (25.5%) and highest in 2020 (35.2%).
Assessment Wait Time, ED Length of Stay and Disposition of Individuals Seen by Telepsychiatry (n = 520).
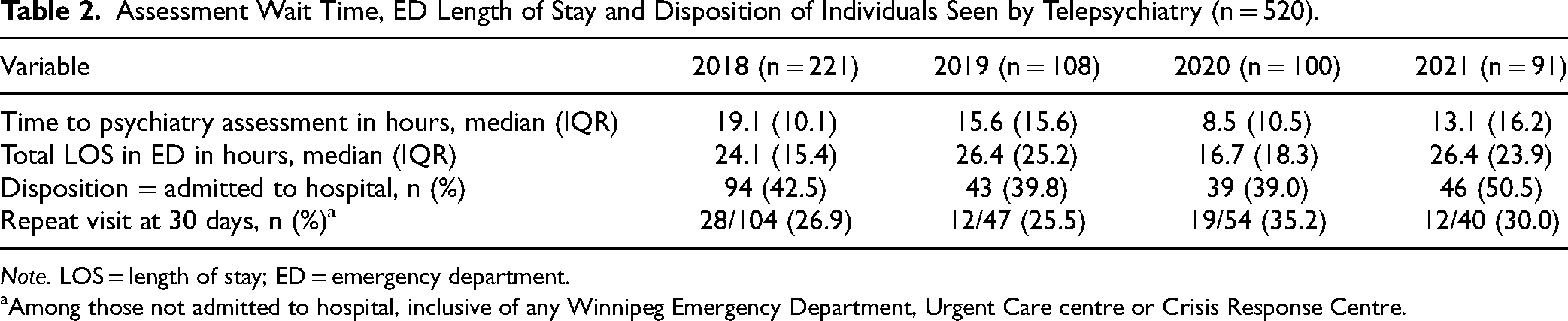
Note. LOS = length of stay; ED = emergency department.
aAmong those not admitted to hospital, inclusive of any Winnipeg Emergency Department, Urgent Care centre or Crisis Response Centre.
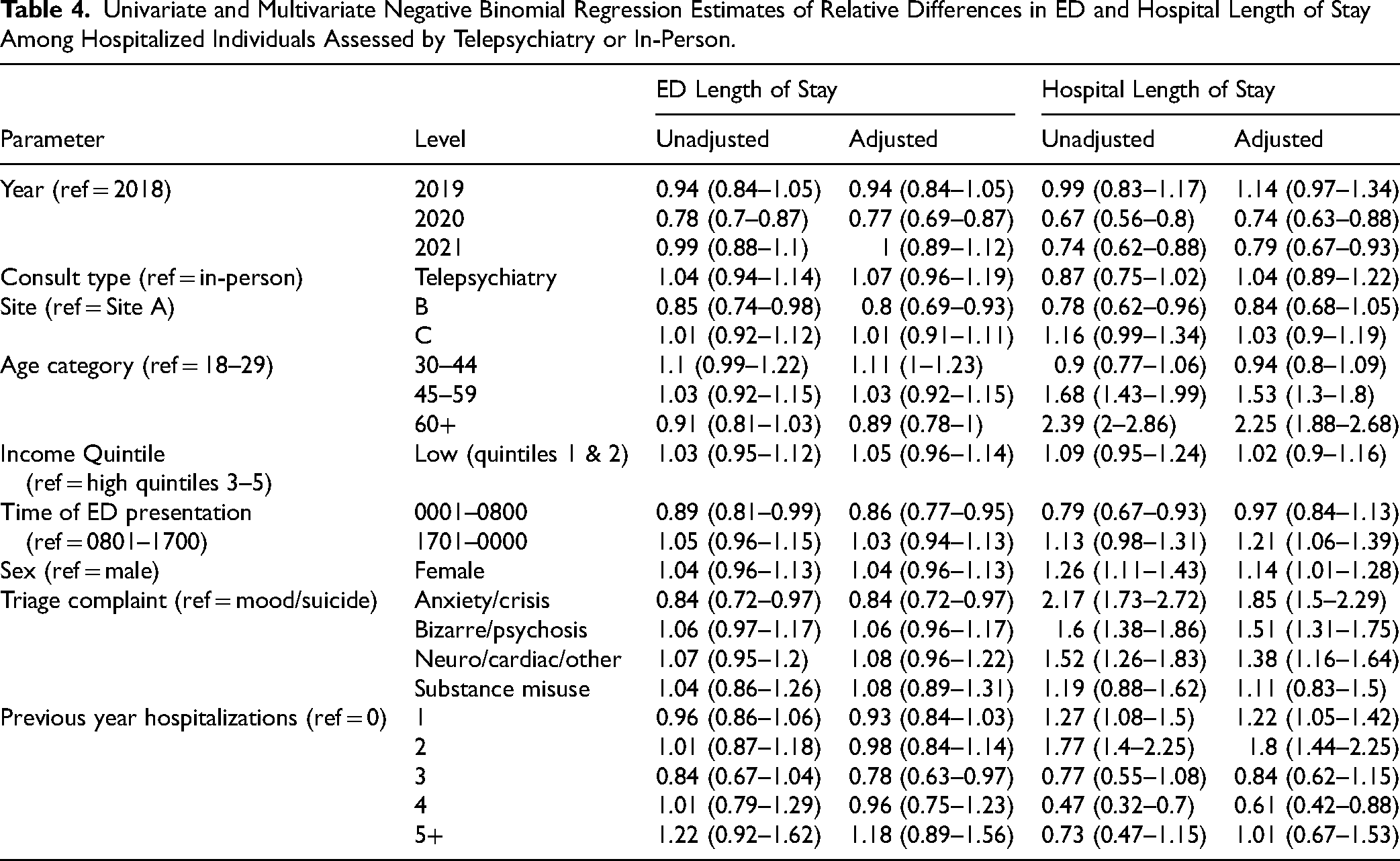
For the comparison analysis (Table 3), there were 978 admissions identified as originating from the 3 telepsychiatry sites. Of those, 222 were telepsychiatry consults (22.7%), and the remaining 756 (77.3%) were considered in-person consults. There were significant differences in the proportion of assessments occurring by telepsychiatry at the 3 sites (P < 0.001), and by year (P < 0.001), with a marked reduction in telepsychiatry after 2018 when more in-person coverage was implemented. Individuals seen by telepsychiatry were significantly more likely at site A, which had the least in-person coverage (P < 0.001), and in 2018 compared to other years (P < 0.001). Telepsychiatry cases more often presented to the referring site between 0801 and 1700 h (P = 0.002), and with mood/suicidal complaints at triage (P < 0.001). The in-person group was more often admitted involuntarily (52.2% vs. 33.0%, P < 0.001). There were no significant differences in admission diagnosis or if discharge was planned or not. There were no significant differences in the adjusted relative differences in ED LOS (1.07, 95% CI .96–1.19) or admission LOS (1.04, 95% CI .89–1.22). In the adjusted model (Table 4), presentations in 2020, presentations to site B and overnight presentations had shorter ED LOS, older age was associated with shorter ED LOS and longer hospital LOS, and previous hospitalizations as well as more severe persistent diagnoses were associated with longer hospital LOS.
Characteristics and Admission Outcomes Among All Individuals Hospitalized Following Psychiatric Consultation, Compared Between Those Seen by Telepsychiatry and Those Seen in-Person.
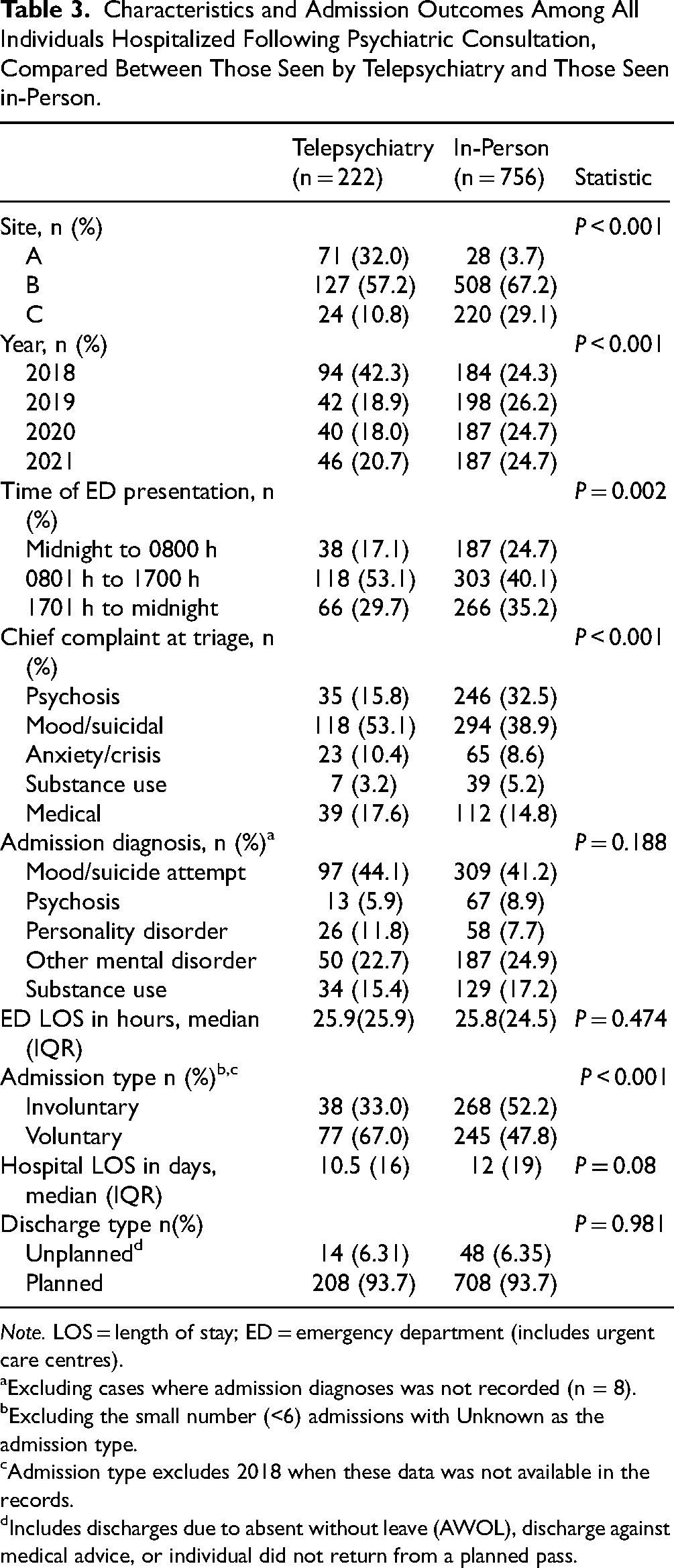
Note. LOS = length of stay; ED = emergency department (includes urgent care centres).
aExcluding cases where admission diagnoses was not recorded (n = 8).
bExcluding the small number (<6) admissions with Unknown as the admission type.
cAdmission type excludes 2018 when these data was not available in the records.
dIncludes discharges due to absent without leave (AWOL), discharge against medical advice, or individual did not return from a planned pass.
Univariate and Multivariate Negative Binomial Regression Estimates of Relative Differences in ED and Hospital Length of Stay Among Hospitalized Individuals Assessed by Telepsychiatry or In-Person.
Discussion
In this study, spanning 4 years of an urban emergency telepsychiatry service, we have shown that the program was able to fill gaps in access to emergency psychiatric assessment and adapt to major changes in clinical service organization that occurred. The profiles of individuals seen remained fairly constant over the years of study, with changes seen in site-specific service delivery reflective of clinical consolidation efforts and fluctuating in-person coverage. Additionally, it adapted to changes in designation of sites as UCs versus EDs which had a resultant impact on the nature of clinical presentations. Comparing in-person and telepsychiatry consults, there were no differences in the ED length of stay or hospital admission duration after adjusting for patient and clinical presentation variables supporting that regardless of how the individual was assessed, the outcome appeared to be similar.
To our knowledge, this is the first study to analyze health service outcomes of urban emergency telepsychiatry in a Canadian-based program. Evaluation of a pilot suburban program in New Brunswick that launched during the pandemic assessed satisfaction and barriers to the service noting high satisfaction among patients and psychiatrists. 9 Consistent with our comparisons, a study of a similar hybrid urban program in New York State (combining telepsychiatry with in-person ED psychiatric support at many of the sites) also found no significant differences in outcomes studied between the telepsychiatry and in-person assessment groups. 28 Our study is among few to compare more in-depth details of the ED presentation between telepsychiatry and in-person consultation groups. A small pilot study in the Netherlands demonstrated no difference between the chief reason for presentation to the ED between individuals seen by telepsychiatry or in-person, with suicidal ideation or attempt being the highest in both. 29 Conversely, our results indicated a higher rate of suicidal presentations in the telepsychiatry group compared to more psychosis in the in-person group which could reflect site and time of day of arrival and/or prioritization of these assessments for in-person due to urgency or mental health act status. Admissions that were preceded by in-person consultation were also more likely to be involuntary. In any case, these results lend support for the value of telepsychiatry to supplement in-person services in urban settings when human resources are limited or unpredictable.
The fortunate establishment of this program in the years prior to the COVID-19 pandemic avoided the need to transform services when that public health crisis hit, in contrast to other centres that may have struggled to rapidly adopt virtual care. Overall, the pandemic saw the rapid virtualization of psychiatric care, 11 with mixed uptake in emergency settings despite strong rationale for its use where access to psychiatrists is strained. When available, patients often prefer in-person care over telemedicine 30 and there are clinical presentations where an in-person assessment may be more amenable (e.g., acute behavioural emergencies—agitated and intoxicated patients, severe cognitive impairments, instances where comprehensive physical examinations are necessary31–33). Additionally, there is some efficiency to in-person staffing as telemedicine may increase ED provider and staff burden at referring sites due to the co-ordination and accompaniment requirements for the assessment.9,24,34 Despite describing more challenges compared to the psychiatrists, ED administrative and nursing staff in the New Brunswick pilot program still frequently had a favourable view of the program overall. 9 That said, a hybrid model, when possible, may be more acceptable to health regions needing to enhance access to emergency psychiatric care than a model that offers only telepsychiatric care.24,35 We did see an association between site and ED LOS, with the site receiving the highest acuity presentations and over time adopting the most in-person psychiatry time alongside the supplemental telepsychiatry option (site B), having the shortest ED LOS. As reported previously, 22 our team carefully assessed and planned for the anticipated barriers to implementation of our service, with continued attention to this over time as additional health system changes occurred. This type of continuous quality improvement is instrumental for the long-term success and viability of any new program. 36
Limitations of this study included factors that affected service delivery during the study period and factors affecting data quality. Most notably, multiple system-level changes occurred over the course of this study that affected demand for and utilization of the telepsychiatry program. Most health systems are complex, 37 and studying the impact of an intervention within this real-world changing system is challenging. The program had to adapt to the system needs over time and as a result the evaluation evolved to a more pragmatic one.
With respect to data, we lost some records due to inability to link cases as a result of incomplete Manitoba Health coverage throughout the entire data extraction period. Unlinked cases may have higher representation of lower socioeconomic status or immigrant persons. Additionally, we were limited to retrieving ED data from Winnipeg only as other sites in the province do not report in EDIS. It is possible that some individuals may have relocated or used services elsewhere prior to or following their telepsychiatry consult. Finally, despite our best efforts, the comparison group was limited to a cohort of hospitalized individuals due to there being no reliable way to identify the occurrence of an in-person emergency telepsychiatry consult within the administrative ED record. As such, we assumed that anyone admitted who was not on the telepsychiatry case list was an in-person consult. We used several conservative strategies to verify this assumption.
Conclusions
Overall, we have shown that this Canadian urban-based emergency telepsychiatry service, operating hybrid with partial in-person staffing, effectively filled a gap in access to psychiatric consultation and was able to adapt to rapid and unexpected changes in local healthcare organization. Flexible models such as this have the potential to enhance and promote rapid access to necessary care, while addressing human resource constraints.
Footnotes
Acknowledgments
The authors acknowledge the contributions of Jocelyne Lemoine, MA who provided project co-ordination support, Evan Hildahl, MD and Lee Taylor, MSc for assistance with data extraction. The authors additionally acknowledge the Manitoba Centre for Health Policy for use of data contained in the Manitoba population research data repository under PHRPC#2022-125. The results and conclusions are those of the authors and no official endorsement by the Manitoba Centre for Health Policy, Manitoba Health, or other data providers is intended or should be inferred. Data used in this study are from the Manitoba Population Research Data Repository housed at the Manitoba Centre for Health Policy, University of Manitoba and were derived from data provided by Manitoba Health and Shared Health Manitoba.
Consent to Participate
Consent was waived as this was a retrospective analysis of health administrative data.
Data Availability
Data used in this article was derived from administrative health and social data as a secondary use. The data was provided under specific data sharing agreements only for approved use at Manitoba Centre for Health Policy (MCHP). The original source data is not owned by the researchers or MCHP and as such cannot be provided to a public repository. The original data source and approval for use have been noted in the acknowledgments of the article. Where necessary, source data specific to this article or project may be reviewed at MCHP with the consent of the original data providers, along with the required privacy and ethical review bodies.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
Ethical approvals for this study were obtained from the University of Manitoba Research Ethics Board (HS25759), Shared Health Research and Innovation, and the Provincial Health Research Privacy Committee (P2022-125).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Frank J Clancy memorial research fund (University of Manitoba).