
Abstract
Objective
As epidemiological patterns of cannabis use and internalizing problems evolve globally, it is critical to reassess their associations—particularly in the post-legalization and post-pandemic context
Methods
Participants were assessed in the 2012 Canadian Community Health Survey's Mental Health Component (CCHS-MH; n = 25,113) and 2022 Mental Health and Access to Care Survey (MHACS; n = 9,861), two nationally representative cross-sectional epidemiologic surveys of Canadians aged 15+. Robust Poisson Regression analyses examined associations between frequency of cannabis use and past 12-month generalized anxiety disorder (GAD), major depressive episode (MDE), and suicidality assessed using the World Health Organization Composite International Diagnostic Interview.
Results
Between 2012 and 2022, the prevalence of GAD, MDE, and cannabis use (any and 2+/week) approximately doubled, while suicidality remained unchanged in the full sample but increased by 44% among youth. Across all models, cannabis frequency was consistently associated with a higher prevalence of GAD, MDE, and suicidality in a frequency-dependent fashion. Additive interactions between year and cannabis on each of the outcomes demonstrated stronger associations in 2022 versus 2012. For example, from 2012 to 2022, those using cannabis 2+/week (relative to no use) had a: (1) prevalence ratio (PR) for GAD of 2.3 (95% CI, 1.6–3.4) increase to 4.5 (3.8–5.2); (2) PR for MDE of 3.0 (2.3–3.9) increase to 5.2 (4.6–5.7); and (3) PR for suicidality of 3.0 (2.1–4.0) increase to 5.4 (4.7–6.1). Select moderation effects indicated associations between cannabis and MDE or suicidality strengthened more among youth (15–24 vs. 25+), and associations with GAD strengthened more among females.
Conclusions
Cannabis use was consistently related to a higher prevalence of internalizing problems, and these associations strengthened between 2012 and 2022. Given continued escalations in co-occurring cannabis use and internalizing problems, greater investment in early identification, intervention, and access to integrated substance use and mental health treatment is needed.
Plain Language Summary
This study found that cannabis use among Canadians is linked with anxiety, depression, and suicidality. From 2012 to 2022, both cannabis use and depression and anxiety disorders rose, with stronger links between them over time. These findings reveal a growing association between cannabis use and depression, anxiety, and suicidality in Canada. Policymakers and practitioners should consider strengthening prevention and intervention efforts to ensure both cannabis use and mental health are addressed together.
Introduction
Cannabis is one of the most commonly used substances, 1 with more than a quarter of Canadians aged 16 and older reporting past year cannabis use in 2023. 2 Since legalization in 2018, access to cannabis products has increased alongside modest increases in the prevalence and frequency of cannabis use (∼4–10%), particularly among emerging adults.3–5 Notably, cannabis use often co-occurs with depressive and anxiety disorders6–8 – leading causes of global disability9,10 – with prevalences having sharply risen over the past decade. 11 For example, the prevalence of past year generalized anxiety disorder (GAD) doubled between 2012 and 2022 among Canadians (from 2.6% to 5.2%) and nearly doubled for major depressive episode (MDE) (from 4.7% to 7.6%). 12 Increases in depression, anxiety, and suicidality (collectively referred to as internalizing problems) began at least a decade before legalization.13–15 Notably, some evidence suggests that internalizing problems further worsened during the COVID-19 pandemic,16,17 with affected individuals being more likely to increase their cannabis use. 18 Given these rapidly changing epidemiological trends, evolving sociocultural and policy landscapes, and increasing potency of cannabis, 19 it is important to examine how associations between cannabis use and internalizing disorders have changed over time to inform contemporary prevention and intervention efforts.
Before nonmedical cannabis legalization and the COVID19 pandemic, the co-occurrence of cannabis use and depression and/or suicidality had significantly increased between 2002 and 2012 among Canadians aged 15 and older. 13 By 2012, Canadians using cannabis at least monthly had over 3.5 times the odds of experiencing MDE or suicidality compared to those who did not report monthly cannabis use. 13 Strengthening of these associations suggests that: (1) the prevalence of depression and suicidality increased more among those using cannabis than those not, and/or (2) cannabis use increased more among those with depression or suicidality than those without. 15 The strengthening relationship between cannabis use and internalizing problems broadly (including anxiety or depression disorders or symptoms, suicidality, and psychological distress) has also been found in a number of US adult studies using general population or post-secondary school samples.20–24 However, some studies have found no change in the co-occurrence of cannabis and internalizing problems over time.25,26 These studies have explored trends prior to 2020, with no national Canadian trend analyses reported post-legalization.
Youth – spanning middle-late adolescence (∼age 15–17) and emerging adulthood (∼age 18–24) – face the highest risk of initiating cannabis use and developing internalizing problems compared to other age groups. 27 Youth have also experienced the largest increases in internalizing problems over the past two decades.11,12,14,15 Compared to youth not using cannabis, a meta-analysis found that youth who use cannabis have 1.4 times the odds of developing depression and 3.5 times the odds of attempting suicide.6,7 Over time, most studies of adolescents across Canada, the US, and Europe have found a strengthening of the association between cannabis use and internalizing problems25,28 or consistent co-occurrence over time,29–32 with few finding any weakening. 30 A study in the US found that state-level nonmedical cannabis legalization contributed to a near doubling of the association between depression and cannabis use among young adults. 23 While the prior Canadian study exploring co-occurring trends from 2002 to 2012 found youth experienced similar increases in associations over time compared to adults, 13 it is important to explore whether this finding has remained constant over the past decade given legalization, the pandemic, and continued escalation of youth internalizing problems.
Females report higher prevalence of internalizing disorders than males, and the gap has increased over time. 12 While females are typically less likely to use cannabis than males, females often experience higher prevalences of co-occurring cannabis use and internalizing disorders.7,33,34 Despite higher co-occurrence among Canadian females, 33 sex assigned at birth did not moderate changes in co-occurring cannabis use and depression or suicidality between 2002 and 2012. 13 However, more recent trend analyses in the US from 2008 to 2019 found the relationship between cannabis and suicidality strengthened more among females (particularly females aged 18–23) than males. 34 Continued exploration of sex differences is important to determine whether targeted prevention and intervention efforts are required, and to generate hypotheses regarding mechanisms driving trends in co-occurrence (i.e., sex-specific causal factors).
This study examines associations between cannabis use and GAD, MDE, and suicidality among Canadians and whether these associations changed between 2012 and 2022. Secondarily, this study explores whether associations differ based on developmental age or sex assigned at birth. We hypothesized that cannabis use and internalizing problems would be moderately correlated, and that associations strengthened between 2012 and 2022. We also hypothesized that associations and changes over time would be larger for: (1) females compared to males; (2) depression and suicidality compared to anxiety; and (3) youth compared adults. These hypotheses and analysis plans were pre-registered: https://doi.org/10.17605/OSF.IO/GB4Z2.
Methods
Design and Sampling
Data came from the 2012 Canadian Community Health Survey's Mental Health Component (CCHS-MH) 35 and 2022 Mental Health and Access to Care Survey (MHACS). 36 These are repeated cross-sectional surveys representative of Canadians aged 15 and older living in the provinces (Yukon, Northwest Territories, and Nunavut were not included). People living on reserves or other Aboriginal settlements, full-time members of the Canadian Forces, and persons living in collective dwellings were excluded.35,36
Data in 2012 were collected using interviewer-delivered standardized computer-assisted interviewing, with 87% conducted in-person in participant homes and 13% conducted over the phone. In 2012, the overall response rate was 68.9% (n = 25,113). 35 All data in 2022 were collected using computer-assisted telephone interviews due to the pandemic. In 2022, the overall response rate was 25% (n = 9,861). Nonresponse was addressed through weighting procedures. 36
At the variable-level, there was minimal missing data (<2% for each variable, from 0% for rurality to 1.7% for GAD). Overall, 4.73% of the sample was missing one or more variables of interest. A series of univariable robust Poisson regressions found missingness to be related to lower income, being older, higher internalizing disorders (MDE, GAD, and suicidality), and less drinking. Missingness was not significantly related to cannabis use, tobacco smoking, rurality, sex, or race. See Supplemental Materials for full results. Following pre-registered analysis plans, only complete data was used given missing was <5%.
Measures
Generalized Anxiety Disorder and Major Depressive Episode
Statistics Canada utilized the World Health Organization Composite International Diagnostic Interview to assess GAD and MDE according to Diagnostic Statistical Manual 4 (DSM-IV) criteria in the past 12 months.
Suicidality
Suicidality was measured with three items without skip patterns including suicidal ideation (‘seriously thinking about suicide or taking your own life’), suicidal plan (‘make a plan for attempting suicide’), and suicide attempts (‘attempt suicide’) in the past 12 months. Endorsing any item was operationalized as suicidality.
Cannabis Use Frequency
Respondents were asked about cannabis use following this statement: ‘the next section is about substances often used nonmedically’. In 2012, respondents were asked how often they used marijuana or hashish in the past 12 months. In 2022, respondents were asked how often they used cannabis or any preparation of the cannabis plant in the past 12 months. In both years, response options were never, <1/month, 1–3 times/month, 1/week, >1/week, and daily. Based on cell counts, categories were collapsed into never, <monthly, ≤1/week, and 2+/week.
Sociodemographic and Other Substance Use Covariates
Substance-related covariates included heavy episodic drinking and frequency of smoking cigarettes. Past-year heavy episodic drinking (5 + drinks on one occasion) was categorized as not in the past 12 months, <monthly, and monthly+. Past-month smoking was a continuous variable indicating the number of smoking days in the past month, ranging from 0 (never) to 30 (daily).
Other sociodemographic covariates included survey year (2022, 2012), biological sex (female, male; gender identity not measured in 2012), age 1 (15–24 years, 25 + years), race (racialized identity, white), rurality (rural, urban), and income (14-point scale $0–100,000+). In sensitivity analyses we considered birth cohort instead of age, where cohorts of interest were Millennials and Generation Zs, based on definitions used by Statistics Canada (born after 1981). Sex and age were also tested as moderators. Covariates were selected based on findings from a recent meta-epidemiological review. 37
Statistical Analyses
A series of models using Poisson regression with robust standard errors were fit for: (A) GAD, (B) MDE, and (C) suicidality. 38 Model 1 consisted of only survey year and cannabis use frequency. Model 2 built on Model 1 by adding an interaction term between survey year and cannabis use frequency. In Model 3, all sociodemographic and substance use confounders were added. In the final two models, three-way interactions between survey year, cannabis use frequency, and biological sex (Model 4) and developmental age (Model 5) were assessed. Model estimated risk in the exposed group (levels of cannabis frequency) and risk in the control group (no cannabis use) were used to calculate the absolute risk increase (ARI) and number needed to harm (NNH). Given the large sample size, we used a conservative P-value of <0.01 and conservative approach to interpret prevalence ratios (PRs) where those ≥1.32 were considered meaningful population effects. 39
In all models with interaction terms (models 2–5), both multiplicative and relative risk due to interaction (RERI) were evaluated.40,41 RERI is a measure of an additive interaction effect, or the increase (on the additive scale) of the outcome when both factors are present, compared to when they are both considered individually. Assessing multiplicative interactions provides effects on a relative scale, while additive interactions provide effects on an absolute scale.40,41
To disentangle age (developmental) and cohort (birth year) effects, a sensitivity analysis based on birth cohort was done similar to that by Grucza et al. (2008). 42 For all models including age (models 3–5), a secondary model was run replacing age with birth cohort. Based on definitions by Statistics Canada, birth cohort was split into older than Millennials (born before 1981), and Millennials/Generation Z (born 1981 or after).
All analyses were performed in R software version 4.4.2 accounting for normalized survey weights based on the Canadian population, and bootstrap replicate weights for variance estimation.
Results
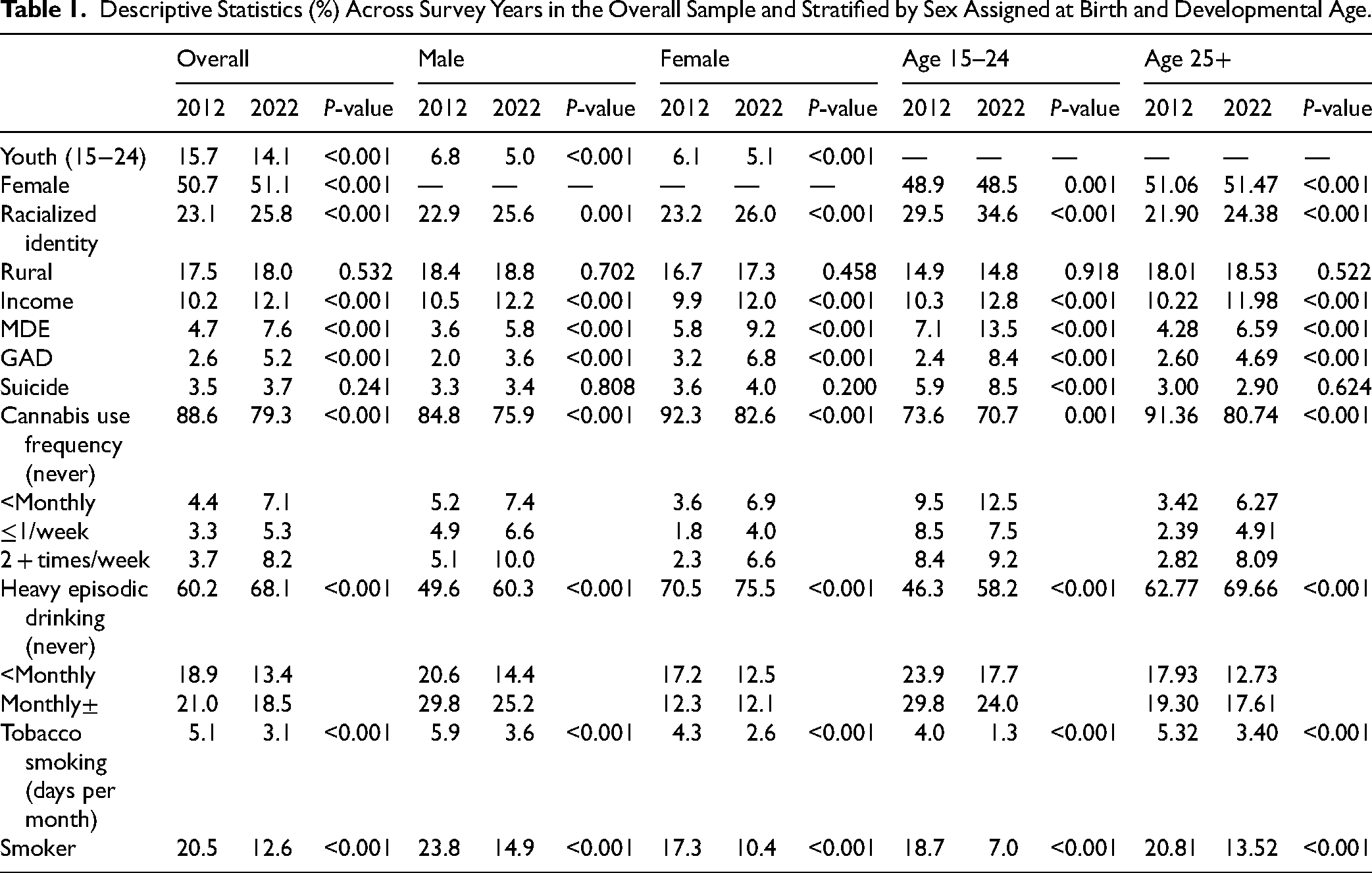
Between 2012 and 2022, prevalences increased for GAD from 2.6% to 5.2% and MDE from 4.7% to 7.6%, while suicidality remained unchanged at ∼3.5%. Frequency of cannabis use also increased with 11.4% reporting any cannabis use in 2012 – including only 3.7% reporting 2 + times/week – increasing to 20.7% in 2022 – including 8.3% reporting 2 + times/week. Notably, heavy episodic drinking and smoking decreased over time. These trends were similar for males and females and mostly similar across age groups except for suicidality, which saw a significant increase of ∼44% from 2012 to 2022 for youth, but not adults 25+. See Table 1 for descriptives and Table 2 for regression results (reported below).
Descriptive Statistics (%) Across Survey Years in the Overall Sample and Stratified by Sex Assigned at Birth and Developmental Age.
Robust Poisson Regression Results.
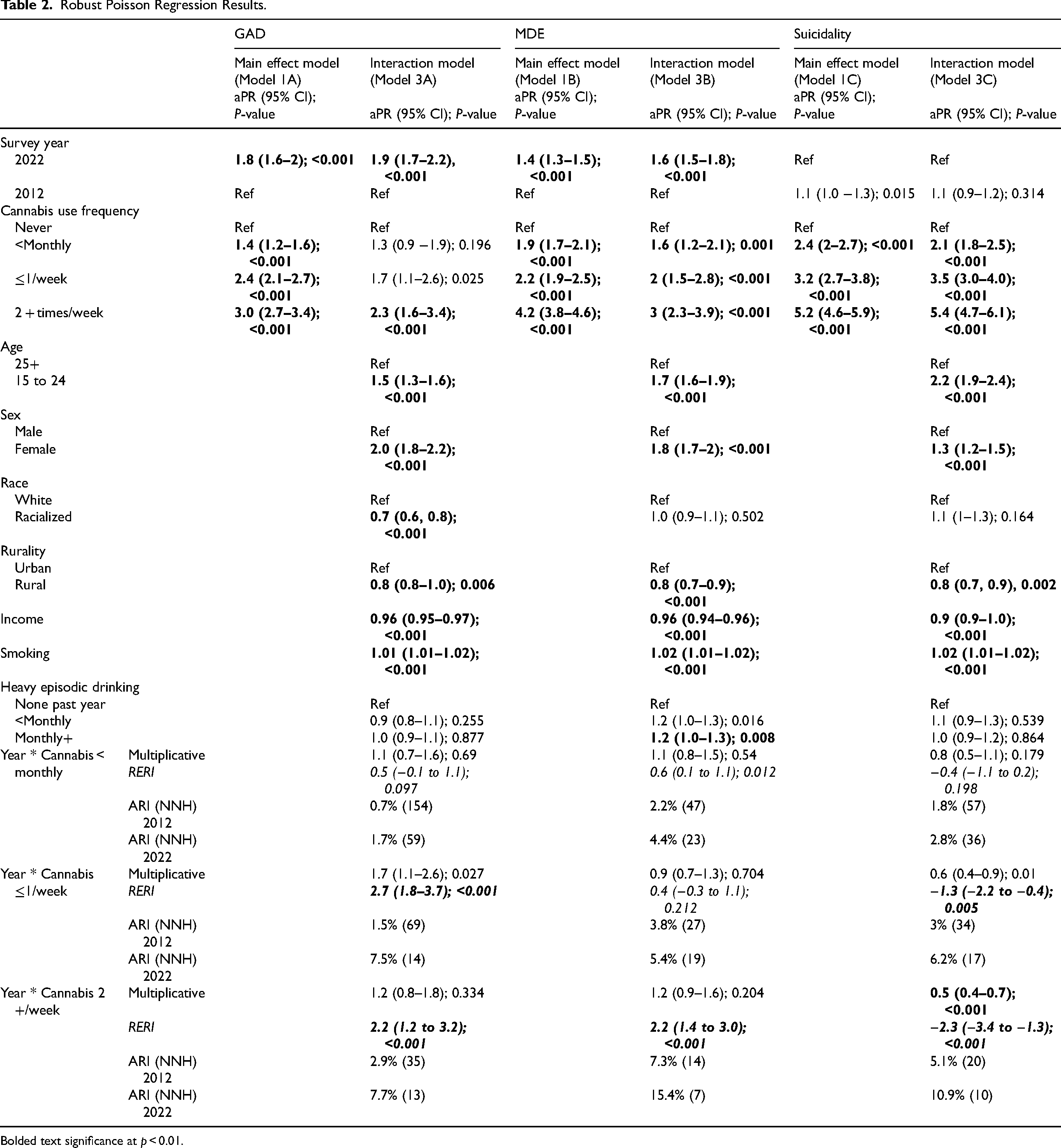
Bolded text significance at p < 0.01.
Across models 1A (GAD), B (MDE), and C (suicidality), cannabis use frequency was consistently associated with internalizing problems in a dose-response fashion. The PRs for GAD were 1.4 (95% CI, 1.2–1.6), 2.4 (2.1–2.7), and 3.0 (2.7–3.4) for <monthly, ≤1/week, and 2+/week, respectively. For MDE, PRs were 1.9 (1.7–2.1), 2.2 (1.9–2.5), and 4.2 (3.8–4.6) for <monthly, ≤1/week, and 2+/week, respectively. For suicidality, PRs were 2.4 (2.0–2.7), 3.2 (2.7–3.8), and 5.2 (4.6–5.9) for <monthly, ≤1/week, and 2+/week, respectively.
There was significant additive interaction between survey year and cannabis use frequency for all internalizing problems, while a multiplicative interaction was found only for suicidality. Overall, there was signal of strengthened associations between cannabis use and internalizing problems between 2012 and 2022, with the NNH for Canadians using cannabis 2+/week going from 35 to 13 for GAD, 14 to 7 for MDE, and 20 to 10 for suicidality. For GAD, the additive interaction model showed that using cannabis ≤1/week and 2+/week were more strongly associated with GAD in 2022 versus 2012. According to model 3A, the PRs for GAD were 1.3 (0.9–1.9), 1.7 (1.1–2.6), and 2.3 (1.6–3.4) in 2012 and 1.8 (1.4–2.1), 4.4 (3.6–5.1), and 4.5 (3.8–5.2) in 2022 for <monthly, ≤1/week, and 2+/week cannabis use respectively. In sum, we found absolute (additive) but not relative (multiplicative) interactions for monthly or more cannabis use and GAD over time. For MDE, there was only an additive interaction for those using cannabis 2+/week. According to Model 3B, the PRs for MDE were 1.6 (1.2–2.1), 2 (1.5–2.8), and 3 (2.3–3.9) in 2012 and 2.2 (1.9–2.5), 2.5 (2.1–2.8), and 5.2 (4.6–5.7) in 2022 for <monthly, ≤1/week, and 2+/week cannabis use, respectively. In sum, we found absolute (additive) but not relative (multiplicative) interactions for using cannabis 2+/week and MDE over time. For suicidality, using cannabis ≤1/week and 2+/week were more strongly associated with suicidality in 2022 (coded as 0) versus 2012 (coded as 1). Note that in these models, given suicidality decreased over time, the coding of year was flipped (2012 = 1, 2022 = 0) since RERI requires all effects to be positive. According to Model 3, the PRs for suicidality were 1.7 (1.1–2.3), 2.2 (1.4–3.0) and 3.0 (2.1–4.0) in 2012 and 2.1 (1.8–2.5), 3.5 (3.0–4.0), and 5.4 (4.7–6.1) in 2022 for <monthly, ≤1/week, and 2+/week cannabis use respectively. Given that both additive and multiplicative interactions were found, this means that the associations between cannabis use and suicidality was greater on both the prevalence difference and PR scales in 2022 compared to 2012. See Figure 1 for a visual representation of interactions.
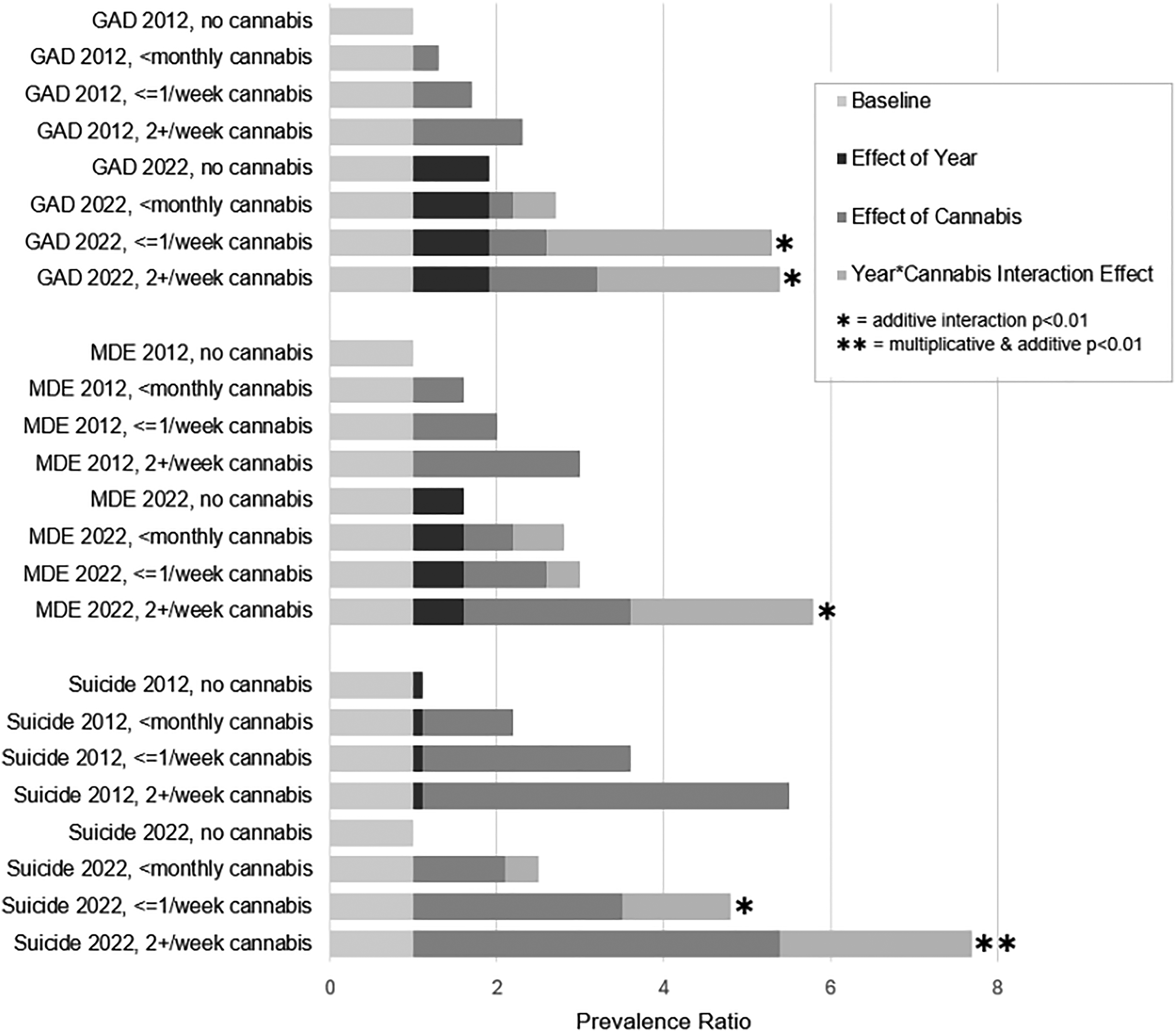
Visualization of the magnitude and composition of prevalence ratios for GAD, MDE, and suicidality between 2012 and 2022 at different levels of cannabis frequency. Prevalence ratios (PRs) indicating higher prevalence are above 1; as such, all PRs in the figure start at 1 since all reflect a higher prevalence given cannabis use relative to no use (baseline bar). The effect of cannabis bar reflects the increase in prevalence attributable to cannabis frequency in 2012. The effects of year bar reflects the increase in the prevalence between survey years. The year*cannabis interaction bar reflects the increase in the prevalence attributable to cannabis in 2022 that is larger than (or ‘added’ to) effects seen in 2012.
Being a youth and female were consistently associated with a higher prevalence of internalizing problems (GAD, MDE, and Suicidality). Developmental age did not moderate the association between cannabis use frequency and GAD over the two survey cycles, though there was some evidence of additive interaction for MDE and both multiplicative and additive interactions for suicidality (at one level of cannabis use frequency) over the two surveys. Developmental age moderated the relationship between 2+/week cannabis use and MDE (RERI = 3.3 [0.9, 5.7], P= 0.007) and between <monthly cannabis use and suicidality between surveys (RERI [2022 reference] = −4.5 [−6.5, −2.4], P < 0.001), whereby youth using cannabis in 2022 had a greater excess risk of MDE and suicidality than in 2012. Notably, birth cohorts did not moderate the temporal associations for GAD or MDE, although one multiplicative interaction (but not additive) for ≤1/week cannabis use and suicidality suggested weaker associations in 2022 for those born in/after 1981. Sex moderated the temporal associations between cannabis use frequency and GAD on the additive scale (not multiplicative), though only for <monthly cannabis use (RERI=2.3 [0.6, 3.9]; P = 0.007). Sex did not moderate the temporal associations for MDE or suicidality on either multiplicative or addictive scales. See Supplemental Materials for full results.
Discussion
In a representative sample of Canadians aged 15+ years, cannabis use was significantly associated with a higher prevalence of GAD, MDE, and suicidality, and these relationships strengthened between 2012 and 2022. In 2012, most point estimates of associations between cannabis use and internalizing problems (PRs 1.3 to 3.0) surpassed pre-specified thresholds for meaningful population effects. 39 In 2022, all associations (point estimates and confidence intervals) between any level of cannabis use and internalizing disorders (PRs 1.8 to 5.4) surpassed thresholds for meaningful population effects. 39 More frequent cannabis use consistently yielded stronger associations between use and internalizing problems, particularly between <monthly use and ≤1/week, with the largest effects for 2+/week. Specifically, those reporting using cannabis 2+/week in 2022 were roughly 5 times more likely to report an internalizing problem than those not using cannabis (4.5 times GAD, 5.2 times MDE, 5.4 times suicidality). There was some (inconsistent) evidence that the association of cannabis use with MDE and suicidality strengthened over time more among youth, aged 15–24, compared to adults, aged 25+. This did not appear to be driven by birth cohort effects. Additionally, there was some evidence that the association between cannabis use and GAD strengthened between survey cycles more among females compared to males. These results extend previous reports of a strengthening between cannabis use and internalizing problems found among Canadians prior to cannabis legalization and the COVID19 pandemic between 2002 and 2012, 13 albeit with recent strengthening found primarily on the additive, rather than multiplicative, scale.
The strengthened co-occurrence of cannabis use and internalizing problems found in this study is consistent with the aforementioned Canadian evidence 13 and more recent trend analyses in US and UK samples.20–25,28 This strengthening indicates that increases in GAD, MDE, and suicidality are more pronounced among Canadians who use cannabis, compared to those who do not. While repeated cross-sectional studies cannot establish causality, strengthened associations over time suggest increasing causal links between cannabis use and internalizing problems, or a growing influence of shared risk-related confounders (i.e., risk factors for both cannabis use and internalizing disorders), relative to protective confounding factors. 15 Notably, individuals often use multiple substances, 43 and temporal strengthening has been found between internalizing problems and other substances.14,44–46 However, in the current study, cannabis associations remained robust after adjusting for alcohol use and smoking, suggesting cannabis has distinct associations with internalizing problems.
While the current study cannot identify causal mechanisms, several hypothesized mechanisms specific to cannabis may be driving the strengthened co-occurrence, including increased cannabis potency, changes in public perceptions and motives, and reduced access to alternative reinforcers. 15 First, levels of delta-9-tetrahydrocannabinol (THC) in cannabis (referred to as its potency) have drastically increased over the past several decades. 47 Average THC levels were estimated to have been around 14% in 2012, 48 increasing to ∼20% in 2018 (2 months post-legalization). 49 New and more potent cannabis products – including cannabis extracts reaching 95%+ THC – have also become more popular.50,51 There is evidence suggesting higher potency contributes to greater risk of psychotic disorders among youth 52 and greater risk for internalizing problems. 53 Second, public perceptions related to cannabis have been changing over the past decade, with higher social acceptability of nonmedical use 54 and reductions in perceived risk of harm related to regular use, 22 possibly contributing to reduced stigma. There are also higher perceived therapeutic benefits of cannabis observed over time, despite minimal to no evidence of psychotherapeutic benefit of cannabinoids to manage internalizing problems.55–57 Cannabis is also easier to access post-legalization and the price has decreased, possibly further facilitating self-medication.4,58 Shifts in perceptions have been particularly pronounced among people with internalizing problems. 22 Altered perceptions alongside ease of access may be driving greater use of cannabis to cope with internalizing problems, which may have been exacerbated during the pandemic when there was restricted access to alternative coping strategies. 18 Third, high inflation and the rise in financial insecurity – the so-called affordability crisis – may limit access to substance-free alternative activities (e.g., entertainment, hobbies, exercise) contributing to more cannabis use for leisure.15,59,60
There are several limitations to consider when interpreting these results. First, while the 2012 (69% response rate) and 2022 (25% response rate) surveys had similar content and sampling frames, sampling and data collection strategies (and resulting non-response rates) were not identical across cycles.35,36 Notably, 2022 surveys were entirely conducted over the phone due to the pandemic, with higher non-response rates; recent comparisons of standardized mental health surveys conducted over the telephone compared to face-to-face show comparable prevalence estimates. 61 Though nonresponse was higher in 2022, Statistics Canada compared MHACS estimates to the 2021 Census and found strong alignment: 75% of 95% confidence intervals from the MHACS contained census values, and all estimates were within 2% (100 + values compared). 36 Non-response was accounted for through weight adjustments, using response homogeneity groups to ensure weights were distributed to similar respondents within age by gender by population groups. 36 The design, along with empirical comparisons, suggest minimal bias from non-response. Weighting reduces, though cannot eliminate, response bias; unmeasured differences and factors such as survey mode, pandemic context, and response rates likely influenced characteristics of participants over time. Second, these data come from repeated cross-sectional surveys and thus results should be interpreted as epidemiological trends, not causal analyses. Third, although internalizing problems were assessed using structured diagnostics, cannabis use was assessed via coarse measures of frequency, lacking gold-standard timeline follow-back measures 62 and measures of onset and duration, limiting inferences about developmental patterns and cumulative exposure effects. Fourth, although common sociodemographic and substance-related covariates were adjusted for, there remains a risk of bias from residual and unmeasured confounding (e.g., family factors, physical health factors, traumatic experiences). 37 While these may explain some of the observed associations or changes over time, given the magnitude of effects (particularly at high frequency of use), we would not expect the overall interpretation of findings to differ.
Conclusion
Between 2012 and 2022, cannabis use significantly strengthened among Canadians aged 15 and older. This occurred alongside escalations in internalizing problems, with a near doubling in the prevalence of GAD and MDE and substantial increases in suicidality among young Canadians. Over this time, the prevalence of internalizing problems increased more rapidly among Canadians who used cannabis compared to those who do not. These findings suggest that previously documented strengthening of the associations between cannabis use and internalizing problems among Canadians pre-legalization (2002–2012) 13 have continued to strengthen leading up to and post legalization. Findings should be interpreted with caution due to use of cross-sectional data and potential for residual confounding. Given the strengthened co-occurrence of cannabis use and internalizing problems, greater investment in integrated substance use and mental health prevention, early intervention, and treatment is needed. Enhancing harm reduction and integrated care efforts could include incorporating internalizing disorder-related recommendations into Canada's Lower-Risk Cannabis Use Guidelines, 63 ensuring routine cannabis screening in mental health care – and vice versa – in line with best practice,64–66 and developing integrated interventions or strengthening shared care pathways address concerns together. 67
Supplemental Material
sj-docx-1-cpa-10.1177_07067437261420701 - Supplemental material for Changes in Cross-Sectional Associations Between Cannabis Use and Anxiety, Depression, and Suicidality in a Nationally Representative Sample of Canadians From 2012 to 2022: Évolution des relations transversales entre la consommation de cannabis et la dépression, l’anxiété et les idées suicidaires au sein d’un échantillon représentatif de Canadiens à l’échelle nationale, de 2012 à 2022
Supplemental material, sj-docx-1-cpa-10.1177_07067437261420701 for Changes in Cross-Sectional Associations Between Cannabis Use and Anxiety, Depression, and Suicidality in a Nationally Representative Sample of Canadians From 2012 to 2022: Évolution des relations transversales entre la consommation de cannabis et la dépression, l’anxiété et les idées suicidaires au sein d’un échantillon représentatif de Canadiens à l’échelle nationale, de 2012 à 2022 by Jillian Halladay, Chris Ji, Katholiki Georgiades, André McDonald, Matthew Sunderland, Tim Slade, Cath Chapman and James MacKillop in The Canadian Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
JM is a principal in BEAM Diagnostics, Inc. and consulted to Clairvoyant Therapeutics, Inc. No other authors have any conflicts of interest to declare.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JH is funded by a Health Systems Impact Embedded Early Career Researcher award co-funded by the Canadian Institutes of Health Research, McMaster University, and St. Joseph’s Healthcare Hamilton (HS3-191640). AJM is supported by a Fellowship from the Canadian Institutes of Health Research (CIHR) (MFE-193995). CC is supported by an Australian National Health and Medical Research Council Investigator Grant Fellowship (GNT2026552) and a Centre of Research Excellence Grant PREMISE Next Generation (GNT2035308). JM is supported by the Peter Boris Chair in Addictions Research and a Canada Research Chair in Translational Addiction Research (CRC-2020-00170). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.