
Abstract
Background
Infectious disease outbreaks have been associated with significant psychological distress and trauma. In Canada, the COVID-19 pandemic's social disruptions have heightened mental health risks. While global studies report elevated posttraumatic stress disorder (PTSD) symptoms, Canadian findings remain limited and inconsistent. This meta-analysis estimated pooled prevalence of PTSD symptoms in Canada during the COVID-19 pandemic and examined potential moderators.
Methods
A comprehensive search strategy was executed by research librarians across five databases (APA PsycInfo, CINAHL, Embase, MEDLINE and Web of Science) and on LitCovid. The PRISMA guidelines were used for data extraction and reporting. Random-effects meta-analyses were conducted to estimate pooled PTSD symptoms prevalence and explore potential moderators using the metaprop command in STATA/SE 19.5.
Results
Thirty studies conducted between 2020 and 2022, with 52,565 participants aged 18 and older were included (65% weighted women). The pooled prevalence of PTSD symptoms was 22.2% (95% CI, 15.7% to 29.4%; I2=99.69). Prevalence was 32.1% in women, 26.1% in men (p = 0.399) and ranged from 16.1% in Quebec to 29.7% in Ontario (p = 0.091). Meta-regressions showed lower PTSD symptoms prevalence in Quebec (B=–0.16, p = 0.029). No significant differences in PTSD symptoms were found according to sex, healthcare worker status, assessment tool used, or data collection year.
Conclusions
This meta-analysis reveals a concerning prevalence of PTSD symptoms in the Canadian population during the COVID-19 pandemic. Contrary to expectations, no significant differences were found by sex or healthcare worker status, suggesting widespread psychological distress across the population. However, the substantial heterogeneity across studies limits the interpretation of these findings in the context of the COVID-19 pandemic. The results emphasize the need for inclusive and accessible mental health responses and further research on post-pandemic Canadians’ mental health. Future studies should better disaggregate data by sex, age and race to address disparities and inform targeted public health policies and interventions.
Introduction
Research during health crises related to infectious diseases, such as Severe Acute Respiratory Syndrome (SARS), Middle East Respiratory Syndrome (MERS), HIV/AIDS and Ebola virus disease, has shown significant and enduring psychological repercussions.1–3 The COVID-19 pandemic, declared as a global public health emergency and pandemic by the World Health Organization in March 2020, 4 exacerbated mental health vulnerabilities and increased common mental health problems, as demonstrated by several meta-analyses.5,6 In Canada, prolonged lockdowns, social isolation and economic insecurity, contributed to a deterioration in the population's psychological well-being and an influx of healthcare utilization for mental health concerns such as depression, anxiety, suicidal attempts and eating disorders.7–9
Although infectious disease pandemics do not always correspond to the types of events traditionally associated with PTSD symptoms, such as natural disasters or violent assaults, several studies have demonstrated that these health crises can themselves constitute traumatic events.1,10,11 These studies have reported high prevalence of PTSD symptoms among both survivors of epidemics, their relatives, people in regions affected and healthcare workers (e.g., Ebola virus disease, HIV/AIDS). For instance, studies conducted in the Democratic Republic of the Congo reported high PTSD symptoms prevalence ranging from 24.3% to 58.81% among Ebola survivors and individuals living in affected areas.10–12 Similarly, a meta-analysis estimated a 28% prevalence of PTSD symptoms among people living with HIV/AIDS. 13
In the case of the COVID-19 pandemic, potential sources of trauma were numerous and often cumulative: constant fear of being infected or infecting loved ones; anxiety over the possibility of dying or witnessing a loved one succumb to the illness; sudden loss of loved ones; inability to grieve under normal conditions due to public health restrictions; loss of employment and income; prolonged isolation; emotional overload from continuous exposure to alarming information; and abrupt disruption of daily routines.7–9
For many individuals, particularly those with pre-existing psychological vulnerabilities, these experiences may have triggered intense traumatic stress reactions. 14 Recognition of the traumatic potential of the COVID-19 pandemic has led the conduction of many studies on PTSD symptoms worldwide, particularly among healthcare workers. 15 Globally, several systematic reviews have examined the prevalence of PTSD symptoms in the context of COVID-19.15,16 An early meta-analysis of studies worldwide conducted in 2020 found a prevalence of 21.94%, 17 while another meta-analysis conducted the same year that included other coronaviruses found a pooled PTSD symptoms prevalence of 21.5%. 18 Subsequent meta-analyses reported similar pooled prevalence, including one comprising 63 studies conducted in 24 countries, which found a pooled prevalence of 17.52%, with particularly high rates among health care professionals. 19 A systematic review of studies using longitudinal data during the COVID-19 pandemic found no significant changes in PTSD symptoms prevalence over the course of the pandemic, but reported that North America had the highest levels of PTSD symptoms in its population, compared to Europe. 15
In Canada, data on the prevalence of PTSD symptoms in the context of COVID-19 are limited and show significant variability. According to the Canadian COVID-19 and Mental Health Survey (CCMHS) conducted by Statistics Canada, the prevalence of PTSD symptoms was 6.9% in 2020. 20 However, other independent studies have reported higher rates. For example, a study involving 3,852 healthcare workers in the Greater Toronto Area found a 50.2% prevalence of moderate to severe PTSD symptoms. 21 Another study conducted in Quebec with 4,914 adolescents and young adults reported a prevalence of 20.3%. 22 This heterogeneity underscores the need for a synthesis of available data to better understand the impact of the pandemic on Canadians’ mental health in terms of PTSD symptoms. It also speaks to the need to explore moderator analyses, such as demographic factors, that may explain between-study heterogeneity.
This systematic review and meta-analysis aim to (1) estimate the pooled prevalence of PTSD symptoms in the context of the COVID-19 pandemic in Canada and (2) examine potential moderators related to PTSD symptoms, such as demographic, geographic and methodological characteristics of the studies.
Methods
Registration
The systematic review protocol was registered with PROSPERO (#CRD42024552536). Some adjustments were made to better reflect the characteristics of the included studies. First, although the Cochrane Risk of Bias Tool and Newcastle-Ottawa Scale (NOS) were initially planned in the protocol based on the expectation of having more longitudinal studies, the included studies were predominantly cross-sectional. Therefore, the JBI Critical Appraisal Checklists were deemed more appropriate, as they are better suited for systematic reviews of prevalence studies (providing different options) and allow for a more accurate assessment of methodological quality. Second, the registration protocol did not initially specify the exclusion of studies based on a quality assessment score, we decided to apply this criterion given the large number of studies published during the pandemic with lower methodological quality, as it was the case in previous meta-analyses.17,23,24 This approach ensured that only studies meeting an acceptable standard of rigor were included, thereby strengthening the validity and reliability of our findings. Finally, the protocol initially indicated the use of the “metafor” package in R, the analyses were ultimately conducted with the “metaprop” command in STATA/SE 19.5, which provides equivalent statistical procedures for meta-analyses of proportions. This change was made for reasons of practicality and consistency, without affecting the results or their interpretation.
Search Strategy
This current review focuses on identifying studies that investigate the impact of COVID-19 on the mental wellbeing of Canadians. To find relevant studies, a research librarian with experience in planning various knowledge synthesis projects drafted, developed and implemented a search strategy to find pertinent published articles across five electronic databases: APA PsycInfo (Ovid), CINAHL (EBSCOhost), Embase (Ovid), MEDLINE (Ovid) and Web of Science (Clarivate). The strategy was informed, in part, by others used in previously published reviews on COVID-19.25,26 Also, search strategies on mental health were also consulted. 27 Finally, a search filter for retrieving studies conducted in Canada was consulted and adapted. 28 A draft search strategy was initially designed by the research librarian for APA PsycInfo (Ovid) using a combination of pertinent subject headings along with relevant keywords. After receiving feedback from the principal investigator, the search was finalized and then adapted for the other databases. The final strategy was executed on 25 January 2024. The complete search strategy is available in Supplemental file 1. A date limit was used to identify studies published after 2020. No other limits were imposed during the search process. To complement the database searches, a simpler strategy was used to find references on LitCovid, an up-to-date curated list of references related to research on COVID-19. Once searches were completed, results were exported from databases and then imported into Covidence, an online tool used to manage various steps of a review's screening phases. Duplicate references were identified and removed once imported into Covidence. Additional duplicates were identified and excluded manually while screening references.
Selection Criteria
Articles that met the following inclusion criteria were included in the review: (1) published on SARS-CoV-2, COVID-19 or Coronavirus; (2) conducted in Canada; (3) written in English or French; (4) studies published from January 2020; (5) empirical studies with quantitative data; (6) longitudinal and cross-sectional design studies; (7) studies assessing mental health outcomes; and (8) studies that scored 5 or higher on the quality assessment tool, but all PTSD studies assessed met this criterion. Studies not meeting these criteria were excluded from the review.
Process for Selection
The studies went through a comprehensive review procedure using Covidence™. Each step of the process was carried out by three pairs of authors (ES, RC, SWK, KO, ES, WPD). In cases of disagreement, a third author (SMMMF) was consulted to reach consensus. Intercoder reliability was 95.7%.
Quality Assessment
The JBI Critical Appraisal Checklists for Qualitative and Cross-sectional Research was used to evaluate the methodological quality of quantitative studies, encompassing possible bias, conduct and analysis. 29 Each criterion was assessed through nine questions: (1) Was the sample frame appropriate to address the target population?; (2) Were study participants recruited appropriately?; (3) Was the sample size adequate?; (4) Were the study subjects and setting described in detail?; (5) Was data analysis conducted with sufficient coverage of the identified sample?; (6) Were valid methods used for the identification of the condition?; (7) Was the condition measured in a standard, reliable way for all participants?; (8) Was there appropriate statistical analysis?; (9) Was the response rate adequate, and if not, was the low response rate managed appropriately? Each criterion met attributed one point to the study, which needed a minimum of 5 points to be included.29,30 The quality assessment was first done independently by three pairs of authors (ES, RC, SWK, KO, ES, WPD). All conflicts were settled by a third author (SMMMF). The outcomes of the quality assessment are delineated in Table 1.
Characteristics of Included Studies (N = 30).
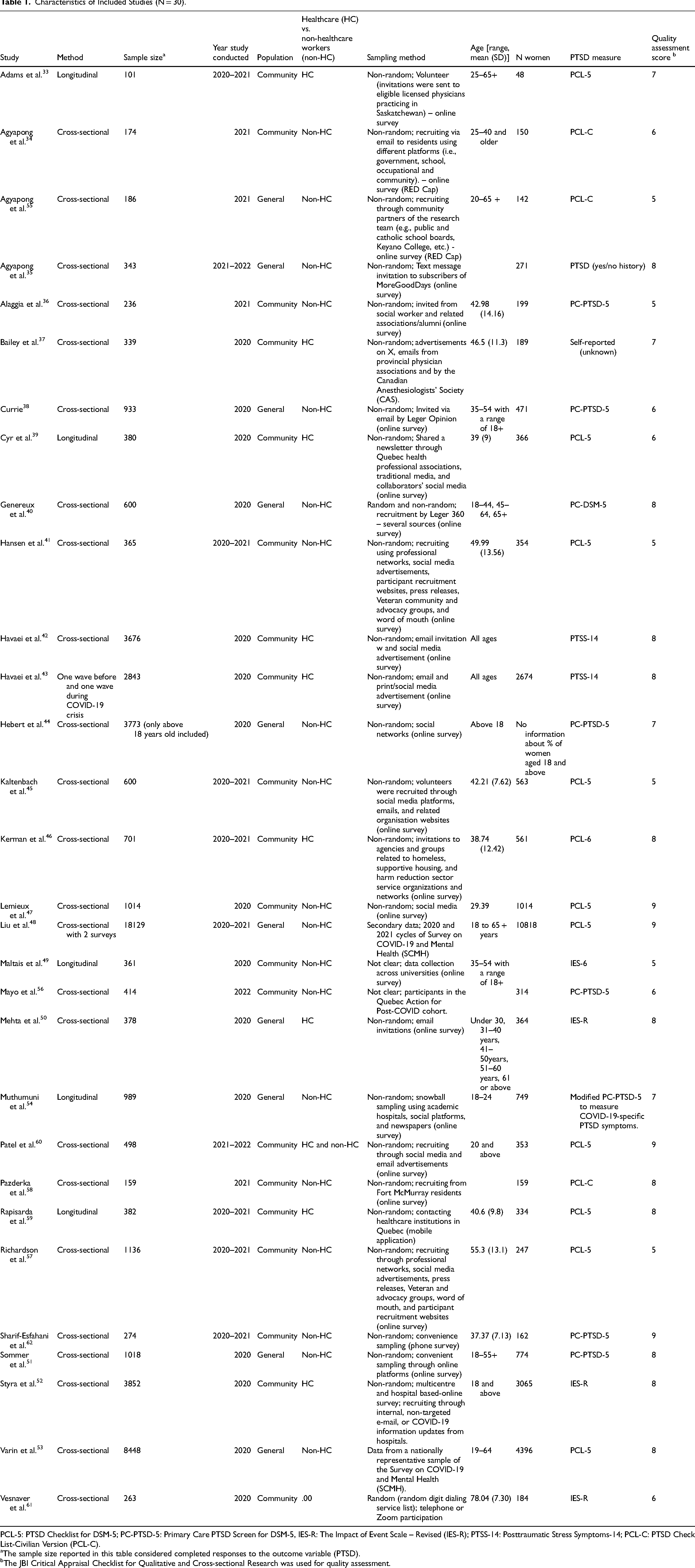
PCL-5: PTSD Checklist for DSM-5; PC-PTSD-5: Primary Care PTSD Screen for DSM-5, IES-R: The Impact of Event Scale – Revised (IES-R); PTSS-14: Posttraumatic Stress Symptoms-14; PCL-C: PTSD Check List-Civilian Version (PCL-C).
The sample size reported in this table considered completed responses to the outcome variable (PTSD).
The JBI Critical Appraisal Checklist for Qualitative and Cross-sectional Research was used for quality assessment.
Data Extraction
The search strategy was initially designed to identify articles on several mental disorders, but for the present article, only data related to PTSD symptoms were extracted and analyzed. The authors used Microsoft Office Excel to extract data from the 1170 selected articles. Groups of two authors worked independently to extract data and then compared their findings for accuracy and consistency. The gathered information was organized and displayed in a table format. This data included author names, publication years, titles, sample demographics (age, sex, ethnicity), methodology details (study design, measures), evaluation timeframe (lifetime or last year), population type (community or general), as well as risk and protective factors. Additional details can be found in Table 1.
Statistical Analysis
The prevalence of PTSD symptoms was computed using the “metaprop” command in STATA/SE 19.5. A random-effects meta-analysis was conducted to estimate the pooled prevalence of PTSD symptoms. The prevalence estimates were transformed using the Freeman-Tukey double arcsine transformation to stabilize the variance. 31 The I2 statistics were used to test statistical heterogeneity. The I2 values of 25%, 50% and 75% are regarded as low, moderate and high heterogeneity across studies, respectively. 32 A funnel plot was examined to assess potential publication bias, which was further evaluated using Egger's test. A set of subgroup analyses and meta-regressions were performed to explore heterogeneity between studies. Subgroups included evaluation period (past week/past 2 weeks and past month), tool (PTSD Checklist for DSM-5 (PCL-5), Primary Care PTSD Screen for DSM-5 (PC-PTSD-5), The Impact of Event Scale – Revised (IES-R), and other tools), sex (male and female participants), type of sample (community and population), year study conducted (2020, 2021, 2020–2021, and 2021–2022), healthcare worker status (no vs. yes), and province (Alberta, Ontario, and Quebec). Regarding healthcare worker status, we excluded three papers from this subgroup analysis that included social workers and mixed of essential workers and healthcare workers. We included Alberta, Ontario and Quebec in subgroup analysis as there were at least four studies per category. The decisions for other subgroups were made based on the criterion of having a minimum of four categories within each group. Meta-regression analyses were performed to compare the prevalence estimates with a reference group. The reference group for the evaluation period was within the past week/past two weeks, for the tool it was PCL-5, for sex it was male participants, for the year study conducted it was year 2020, for study type it was cross-sectional studies, and for the province it was Ontario. We also conducted meta-regression analyses based on other covariates including women proportion (as study characteristics) and quality assessment score.
Results
A total of 10,176 studies were identified and imported into Covidence™ for initial screening, and 4,961 duplicates were removed. Title-abstract screening of 5,215 articles resulted in the exclusion of 3,895. A total of 1,319 full-text articles underwent eligibility assessment, and 667 were excluded for various reasons: 324 did not assess mental health and COVID-19, 91 full texts were unavailable, 2 were not in French or English, 160 had the wrong study design, 18 were duplicates, 46 included pre-2020 data, and 26 were not conducted in Canada and, 622 did not provide data on PTSD symptoms. Ultimately, 30 studies reporting data on the prevalence of PTSD symptoms were retained for data extraction. More information is presented in the PRISMA flow diagram (Figure 1).
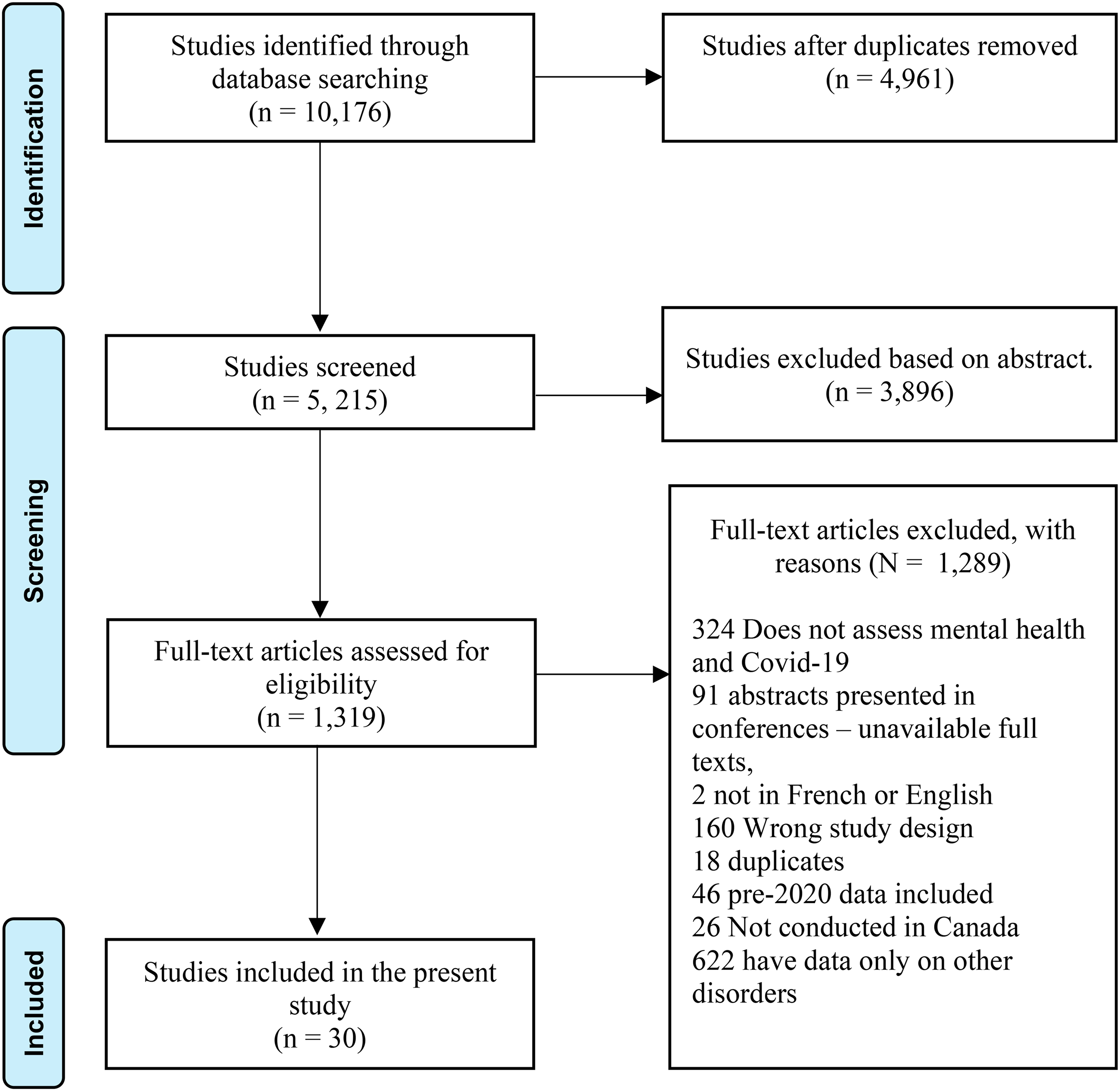
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of the review search process.
In total, 30 studies with a sample of 52,565 individuals were included in the meta-analysis.33–62 Among these studies, four studies were conducted in Ontario, six studies were conducted in Quebec, six studies conducted in Alberta, and the rest of the studies conducted in other provinces or across Canada. Fifteen studies were conducted in year 2020, five studies were conducted in 2021, eight studies were conducted in 2020–2021, and two studies were conducted in 2021–2022. Seventeen studies did not clarify sample distributions regarding race/ethnicity while 13 studies clarified sample distributions regarding race/ethnicity. Of 13 studies that clarified the sample distribution regarding race/ethnicity, none reported the prevalence of PTSD symptoms for racial groups. After sending emails to authors concerning PTSD symptoms over racial groups, we only received information from three studies, which were not enough to conduct subgroup analyses. It is worth noting that the population of study “Sharif-Esfahani et al. 62 ” was Syrian refugees and study included race differences in the regression analysis. 54 The mean quality assessment was 7.07 (SD = 1.39; Min = 5; Max = 9). Study characteristics (weighted women % = 65.50) are presented in Table 1. The funnel plot (Supplemental file 2) shows asymmetry, suggesting potential publication bias. However, publication bias was also tested using Egger's test. No significant result was observed (z = −.76, p = 0.450), indicating that publication bias is unlikely given this quantitative result.
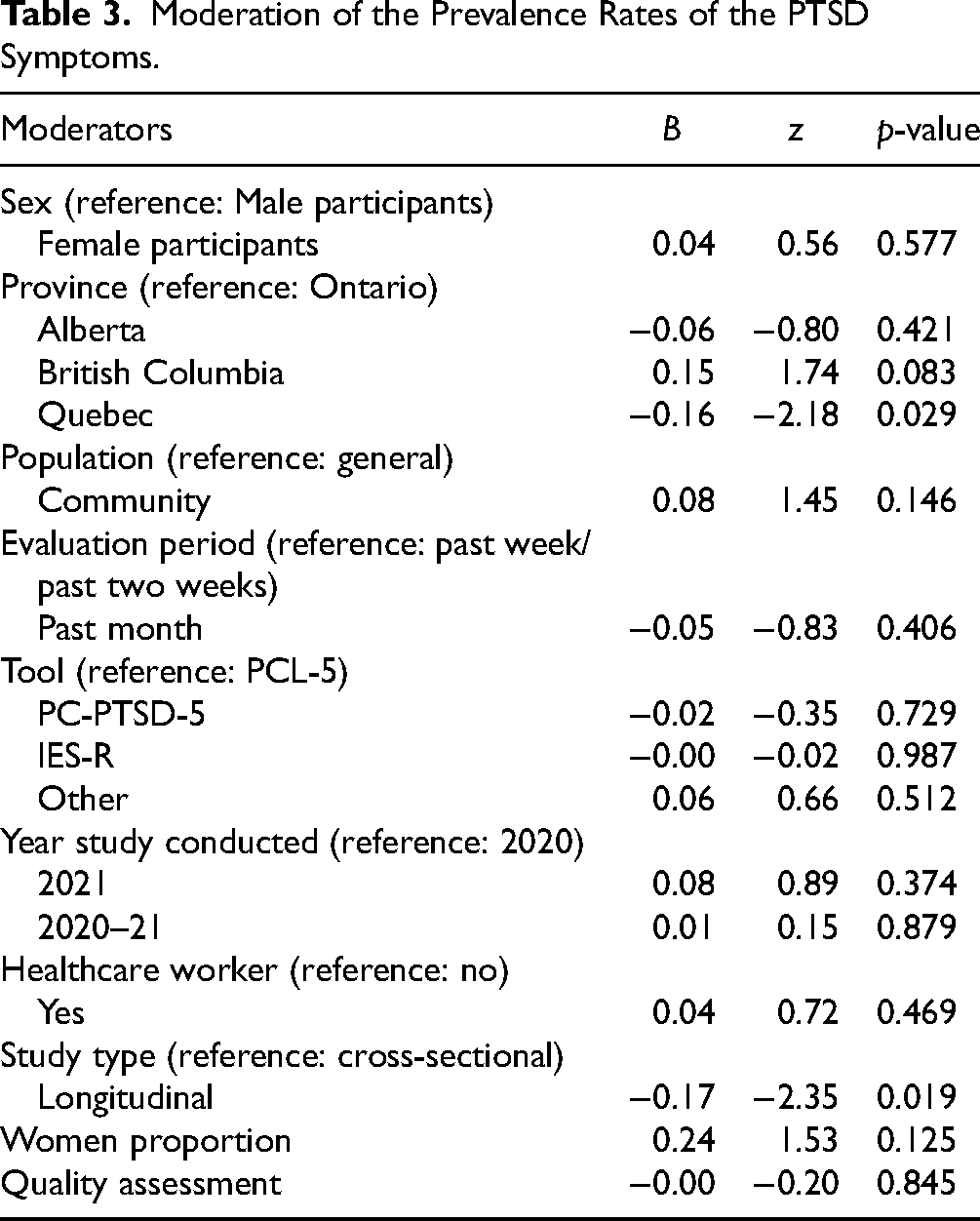
The pooled prevalence of PTSD symptoms was 22.2% (95% CI, 15.7% to 29.4%; Table 2; Figure 2). A high heterogeneity among studies (I2 = 99.69) was observed. The prevalence of PTSD symptoms was 32.1% and 26.1% among women and men, respectively; however, this difference was not statistically significant (p = 0.399). Moreover, the prevalence of PTSD symptoms was 29.7%, 26.7% and 16.1% in Ontario, Alberta and Quebec, but it was only marginally different (p = 0.091). Likewise, no statistically significant differences regarding population, evaluation period, tool, year study conducted and healthcare worker status were found (Table 2). Meta-regression analyses showed that studies with a longitudinal design were negatively associated with the prevalence of PTSD symptoms (B = −0.17, p = 0.019). Moreover, Quebec was negatively associated with the prevalence of PTSD symptoms (B = −0.16, p = 0.029), suggesting lower prevalence of PTSD symptoms reported in Quebec (Prevalence = 16.1% [95% CI, 10.3% to 22.9%]) compared to Ontario (Prevalence = 29.7% [95% CI, 15.1% to 46.7%]). No statistically significant associations were found for sex, population, evaluation period, tool, year study conducted, healthcare worker, women proportion and quality assessment (Table 3).
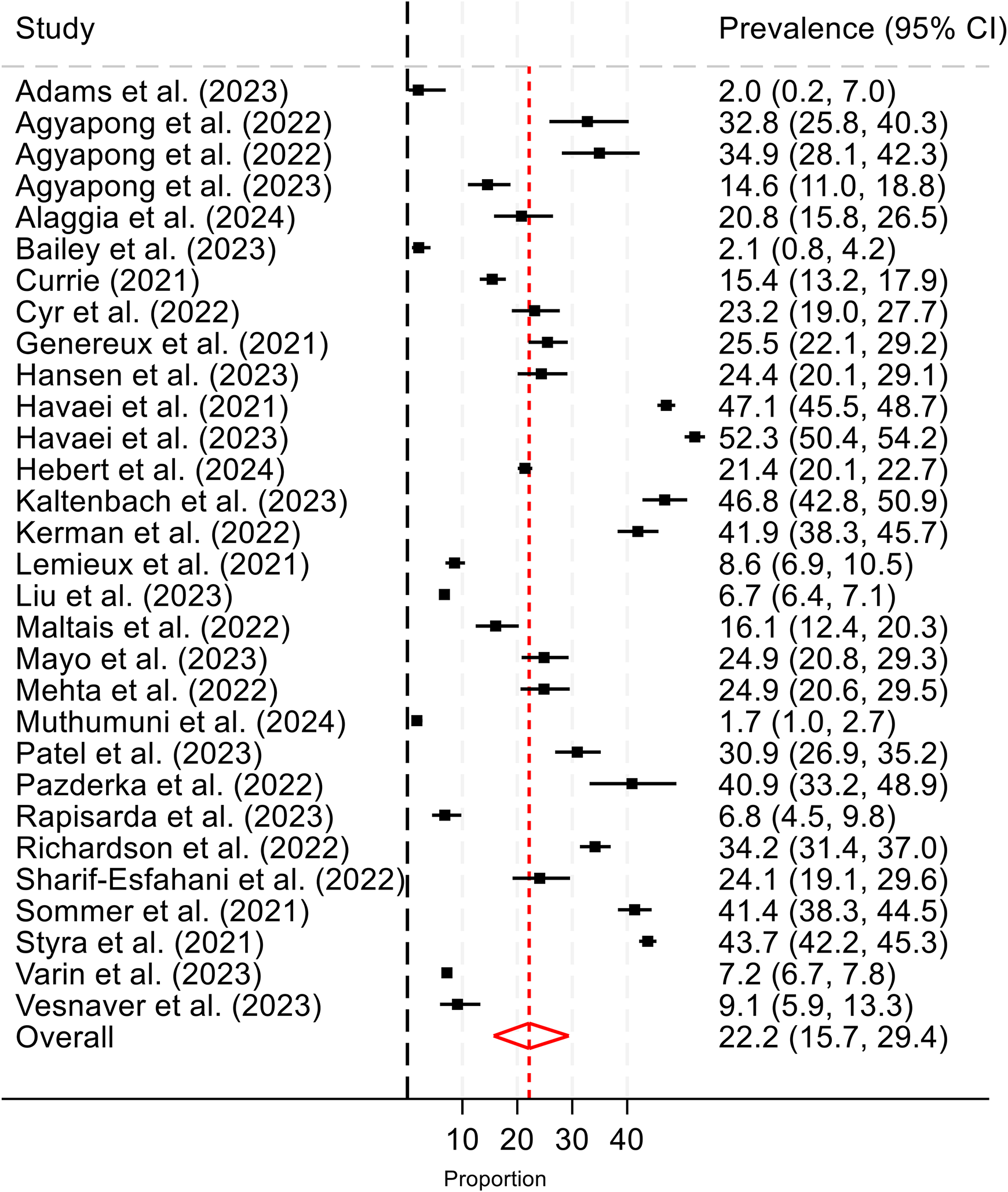
The pooled prevalence of PTSD symptoms across 30 studies.
Prevalence of PTSD Symptoms According to Potential Moderators.
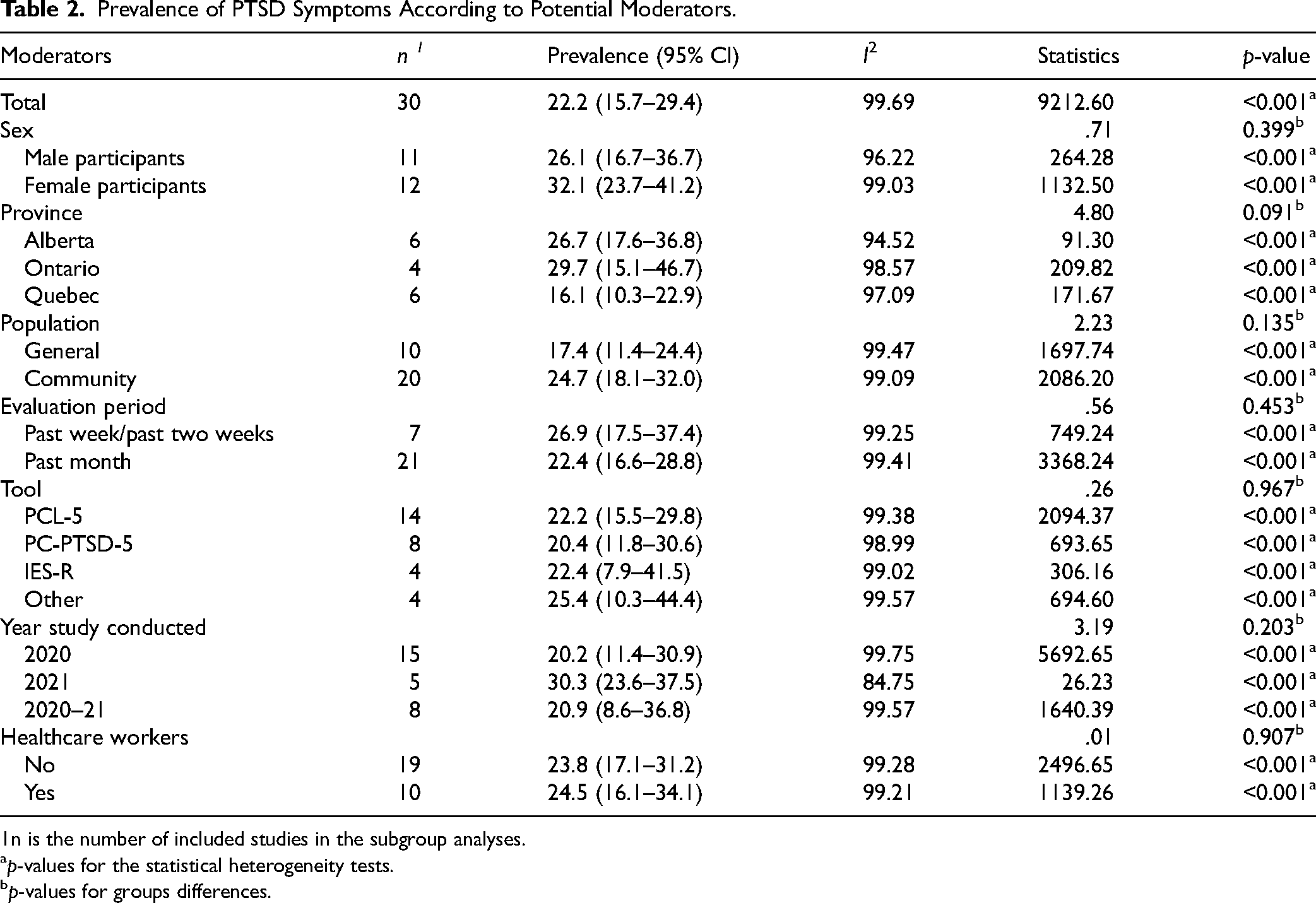
n is the number of included studies in the subgroup analyses.
p-values for the statistical heterogeneity tests.
p-values for groups differences.
Moderation of the Prevalence Rates of the PTSD Symptoms.
Discussion
This meta-analysis, which included 30 studies and a total of 52,565 participants in Canada, revealed that more than one in five individuals (22.2%) experienced significant PTSD symptoms during the COVID-19 pandemic in Canada. This rate is high and exceeds estimates observed in several international contexts. For example, a meta-analysis of 63 studies conducted in 24 countries among general, clinical and at-risk populations (n = 124,952) found a pooled prevalence of PTSD symptoms of 17.5% (95% CI, 13.9% to 21.9%), 19 while another study estimated this prevalence at 15% (95% CI, 11% to 21%). 63 Similarly, in general population samples during the pandemic, a systematic review of studies conducted in 24 countries reported a prevalence of 18% (95% CI, 15% to 20%). 16
Moreover, even among populations most exposed to COVID-19, such as survivors, the reported pooled PTSD symptoms prevalence rates are sometimes lower than those observed in the present meta-analysis. A meta-analysis of 13 studies with COVID-19 survivors (n = 1,093), found a pooled prevalence of 16% (95% CI, 9% to 23%). 64 Similarly, a meta-analysis among healthcare workers reported a pooled prevalence of 21.5% (95% CI, 10.5% to 34.9%). 18 These comparisons suggest that the Canadian context may have generated particularly high levels of distress during the COVID-19 pandemic, possibly due to systemic factors such as social inequalities, limited access to psychological care, widespread social isolation in the population (including older adults), heightened social polarization during this period and the number of cases and deaths. 65 Although socioeconomic inequalities and limited access to psychological care are generally greater in many Low- and Middle-Income Countries, the societal systems in which populations are embedded differ markedly. In Canada, the more formalized mental health and social support infrastructure may facilitate greater recognition and reporting of symptoms, which could partly explain the higher observed prevalence of PTSD symptoms.
The high prevalence observed in the present study is consistent with those reported in other North American studies. Indeed, a meta-analysis found that individuals living in North America had a higher prevalence of PTSD symptoms (23.3%; 95% CI, 18.5% to 28.0%) compared to those living in Europe (14.4%; 95% CI, 12.2% to 16.6%). 15 This convergence of findings highlights that PTSD symptoms constitute a major public health issue in the North American context during the COVID-19 pandemic. It may reflect the influence of geopolitical and social context on psychological distress levels.9,65
Before the COVID-19 pandemic, PTSD symptoms were already a notable public health concern in Canada. The most important study among the general population was published more than 15 years ago. It reported that 9.2% of Canadian adults met criteria for PTSD at some point in their lives, with higher rates observed among women. 66 These pre-pandemic prevalence rates provide an important benchmark for understanding the impact of COVID-19. Globally, prevalence estimates of PTSD symptoms vary widely depending on the population and context. For instance, a study found that cultural and regional factors can influence the prevalence of PTSD symptoms across populations. 67 Similarly, large-scale meta-analyses have estimated the prevalence of PTSD symptoms at 15–22% in populations exposed to conflict or about 30% for those exposed to natural disasters.68,69 These pre-pandemic figures highlight that a considerable proportion of individuals experience PTSD symptoms even outside of pandemic conditions.
A striking result of our study is the absence of significant differences across various demographic and geographic subgroups. Notably, no significant differences were observed between men and women, nor between healthcare workers and the rest of the population. These results contrast with many previous studies that show generally higher PTSD symptoms prevalence among women. 70 It is possible that the severity of the pandemic crisis produced high and homogeneous levels of psychological distress across all groups, temporarily erasing usually observed disparities. The non-significant difference between men and women may also be due to the number of studies that reported prevalence of PTSD symptoms disaggregated by sex and introduce a statistical bias. Similarly, although healthcare workers presented a slightly higher PTSD symptoms rate (24.5%, 95% CI, 16.1% to 34.1%), this difference was not significant compared to the general population (23.8%, 95% CI, 17.1 to 31.2). This absence of significant difference may be explained by an exceptionally high prevalence in the overall Canadian population, reducing contrasts between subgroups. However, the pooled prevalence found among healthcare workers remains notably higher than what was found in an umbrella review of seven meta-analyses, which revealed a pooled prevalence of 13.5% (95% CI, 9.1% to 18%) among healthcare professionals during the pandemic. 71 Moreover, the pooled prevalence found in the present meta-analysis is higher than that found in the seven meta-analyses included in that umbrella review.
The only significant difference observed is between Quebec and Ontario, with Quebec showing a lower prevalence. This can be partly explained by school closures: province-wide shutdowns in Quebec lasted only 9 weeks, compared to over 25 weeks in Ontario, not including additional regional closures. 72 These extended closures placed a heavy burden on the whole families, who had to balance remote work, online learning and childcare, while access to emergency childcare remained strictly limited. Many parents were forced to leave their jobs or rely on grandparents, often putting their health at risk. Employer expectations of sustained productivity during this period exacerbated the strain, particularly for mothers from marginalized groups, who disproportionately experienced the so-called “she-cession”—facing fewer promotions and higher burnout rates. 72
Limitations
This study presents several limitations. First, despite Canada's racial and ethnic diversity, very few of the included studies disaggregated data by ethnic origin. Of the 13 studies that documented the racial or ethnic distribution of participants, none reported PTSD symptoms prevalence according to these groups. Two exceptions stand out: one studied Syrian refugees, 62 and one included racial variables in their regression analysis, but did not provide specific rates. 54 This lack of racial disaggregation is a major limitation, preventing a nuanced understanding of mental health inequalities. Second, few articles disaggregated data by sex, province, or age, which limits the interpretation of possible variations between these groups. This could obscure clinically important differences and compromise the development of targeted intervention strategies. Third, the majority of included studies were cross-sectional, limiting the ability to establish causal links between pandemic-related exposures and PTSD symptoms. The use of varied measurement tools, inconsistent data collection periods and the lack of detailed participant information further increase the observed heterogeneity. In addition, although Egger's test did not detect publication bias (z = –.65, p = 0.513), the possibility of bias related to the non-publication of null results cannot be entirely ruled out. Finally, we observed substantial heterogeneity across studies, which reduces the certainty and limits the generalisability of our findings. Despite efforts to account for this variability by incorporating population characteristics (e.g., healthcare workers vs. non-healthcare workers; general vs. community populations), sampling methodology, and by testing covariates through meta-regression, a high degree of heterogeneity persisted. Such variability may also reflect the wide variety of instruments used in the studies to screen for probable or clinical PTSD, or differences in cutoff thresholds across studies. Interpretation of these findings should therefore remain nuanced, attentive to the diversity of study contexts and methods.
Conclusions
This meta-analysis reveals a high and concerning prevalence of PTSD symptoms in the Canadian population in the context of the COVID-19 pandemic. Contrary to expectations, no significant differences were observed by sex or profession, suggesting generalized psychological distress across society. These results underscore the importance of an inclusive and accessible mental health response. They call for further studies to assess the current state of mental health in the Canadian population in terms of post-traumatic stress symptoms now that the COVID-19 pandemic is behind us. They also highlight the need for better data disaggregation in future research, to document inequalities related to sex, age, province, racial background and ethnic origin. It is indeed unacceptable that Canadian research continues to be published without any effort to include different racial groups and disaggregate data in order to capture and address racial disparities. Such an approach is essential to guide public policies and clinical interventions toward equitable and effective mental healthcare in Canada.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437251408179 - Supplemental material for Prevalence and Correlates of Post-Traumatic Stress Disorder Symptoms During the COVID-19 Pandemic in Canada: A Systematic Review and Meta-analysis: Prévalence et corrélats des symptômes du trouble de stress post-traumatique pendant la pandémie de COVID-19 au Canada : Revue systématique et méta-analyse
Supplemental material, sj-docx-1-cpa-10.1177_07067437251408179 for Prevalence and Correlates of Post-Traumatic Stress Disorder Symptoms During the COVID-19 Pandemic in Canada: A Systematic Review and Meta-analysis: Prévalence et corrélats des symptômes du trouble de stress post-traumatique pendant la pandémie de COVID-19 au Canada : Revue systématique et méta-analyse by Jude Mary Cénat, Wina Paul Darius, Seyed Mohammad Mahdi Moshirian Farahi, Taddele Cherinet Kibret, Eden Samson, Runzhi Chen, Seung Won Kuk, Khanyisa Ogbuaku Jnr, Evelyn Steacy, Patrick R. Labelle, Sheri Madigan and Rose Darly Dalexis in The Canadian Journal of Psychiatry
Supplemental Material
sj-docx-2-cpa-10.1177_07067437251408179 - Supplemental material for Prevalence and Correlates of Post-Traumatic Stress Disorder Symptoms During the COVID-19 Pandemic in Canada: A Systematic Review and Meta-analysis: Prévalence et corrélats des symptômes du trouble de stress post-traumatique pendant la pandémie de COVID-19 au Canada : Revue systématique et méta-analyse
Supplemental material, sj-docx-2-cpa-10.1177_07067437251408179 for Prevalence and Correlates of Post-Traumatic Stress Disorder Symptoms During the COVID-19 Pandemic in Canada: A Systematic Review and Meta-analysis: Prévalence et corrélats des symptômes du trouble de stress post-traumatique pendant la pandémie de COVID-19 au Canada : Revue systématique et méta-analyse by Jude Mary Cénat, Wina Paul Darius, Seyed Mohammad Mahdi Moshirian Farahi, Taddele Cherinet Kibret, Eden Samson, Runzhi Chen, Seung Won Kuk, Khanyisa Ogbuaku Jnr, Evelyn Steacy, Patrick R. Labelle, Sheri Madigan and Rose Darly Dalexis in The Canadian Journal of Psychiatry
Footnotes
Acknowledgements
We extend our acknowledgements to Farid Mansoub Bekarkhanechi, Jihane Mkhatri, Julianna Mazzitelli, Jeremiela francois, Olivia Onesi, Kathy Josiah, Binty-Kamila Bangoura, Mia Mbiya Mwepu, Rand Kelargy for the help during the first steps of the project.
Author Contributions
Dr. Cénat and Dr. Moshirian Farahi have full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: Cénat, Moshirian Farahi, Darius, Labelle, Dalexis. Acquisition and extraction of data: Darius, Moshirian Farahi, Kibret, Samson, Chen, Kuk, Ogbuaku, Steacy, Labelle, Cénat. Statistical analysis: Moshirian Farahi and Cénat. Interpretation of data: All the authors. Drafting of the manuscript: Cénat, Moshirian Farahi, Darius, Labelle, Dalexis. Critical revision of the manuscript for important intellectual content: Madigan, Cénat, Moshirian Farahi, Dalexis. Administrative, technical, or material support: Darius, Moshirian Farahi, and Cénat. Supervision: Cénat.
Data Availability
They are available on request from the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.