
Abstract
Objective:
To identify sociodemographic, lifestyle, and psychological correlates of flourishing mental health (i.e., feeling good and functioning well) in a population-based sample of young adults.
Method:
Data for this cross-sectional study were drawn from the ongoing Nicotine Dependance in Teens study, Québec, Canada. Of 799 participants in cycle 23, 792 (mean (SD) age = 30.6 (1.0) years) provided data on positive mental health using the Mental Health Continuum - Short Form (MHC-SF) and were retained for analysis. Each potential correlate was studied in an unadjusted model, a model adjusted for age and sex, and a model adjusted for age, sex and other covariates related to the specific correlate of interest.
Results:
Of 792 participants retained for analysis, 39.4% (39.9% of females; 38.8% of males) reported flourishing mental health. Variables associated with higher odds of flourishing included attended university (OR: 1.44 [1.05, 1.99]), being in a relationship (OR: 1.64 [1.22, 2.21], being employed (OR: 1.97 [1.27, 3.11]), high sleep quality (OR: 3.45 [2.53, 4.73]), meeting leisure screen time guidelines (OR: 2.12 [1.59, 2.85]), and relatively high levels of coping ability (OR: 3.11 [2.58, 3.80]). Variables associated with lower odds of flourishing included living alone (OR: 0.58 [0.38, 0.86]), relatively low household income (OR: 0.37 [0.20, 0.64]), and high depressive (OR: 0.05 [0.01, 0.15]) and anxiety (0.17 [0.09, 0.29]) symptoms.
Conclusions:
Sociodemographic (education, relationship status, employment status, and income), lifestyle (sleep, screen time), and psychological (coping ability, depressive and anxiety symptoms) factors are correlates of flourishing mental health in this population-based sample of young adults. Results provide a foundation for future research to inform the development of effective programs targeting specific subgroups to promote positive mental health in young adults.
Introduction
Early adulthood is a transitional period that begins in late adolescence and lasts well into the third decade of life. 1 During this period, young adults navigate multiple new life roles and responsibilities (e.g., changes in relationships, education, and residential status) that can challenge their mental health and increase the risk of developing mental disorders.2-4 Research on young adults’ mental health to date has largely focused on common mental disorders including depression and anxiety.3,5-9 However, low levels of positive mental health are associated with limitations in daily life (e.g., missed days of work, physical conditions) 10 even in the absence of symptoms of mental disorders. From a public health perspective, poor mental health is associated with a notable economic burden in developed countries. 11 To acquire more comprehensive understanding of overall mental health and its determinants in young adults, as well as to develop effective mental health promotion programs and maximize resources targeting young adults, it is crucial to consider positive mental health alongside mental illness.
In 2002, Keyes introduced the concept of “complete mental health” to distinguish positive mental health from the traditional focus on mental illness. 2 In Keyes’ two-continua model, positive mental health and mental disorders are independent but related concepts. 2 Positive mental health includes emotional well-being (i.e., the experience of positive emotions such as joy), psychological well-being (i.e., positive functioning in various aspects of life, including but not limited to self-acceptance and personal growth), and social well-being (i.e., positive social functioning such as social acceptance and integration). 12 Keyes' model and related measurement scale, the Mental Health Continuum-Short Form (MHC-SF), enable the classification of individuals into three categories of positive mental health: flourishing, moderate, and languishing. 2 The term flourishing refers to a high level of positive mental health, and is a combination of feeling good (i.e., hedonic well-being) and functioning well (i.e., eudaimonic well-being).2,13 Languishing refers to low levels of both positive emotions and positive functioning, and moderate is intermediate between flourishing and languishing. 2
While mental health challenges often manifest in late adolescence or the second decade of life, various emerging circumstances, including diminishing work opportunities and rising costs of education and independent living, serve as examples of broader societal shifts that have extended the transition to adulthood, making it more complex and varied. 14 Mental health and illness symptoms fluctuate during this period, 15 highlighting the importance of promoting positive mental health to reduce the risk and severity of mental health issues. Promoting mental well-being in young adults ages 28 to 34, and particularly during the childbearing years, can enhance well-being and foster better parenting practices, which in turn may reduce the likelihood of children experiencing early mental health challenges.16,17 Addressing mental health during emerging adulthood can prevent issues from escalating into chronic conditions, promote resilience and reduce the future prevalence of mental health challenges, thereby contributing to long-term public health benefits.
According to the Canadian Community Health Survey - Mental Health 15 (CCHS-MH 2012), 71.1% of Canadians ages 25 to 44 years had flourishing mental health in 2012, a lower proportion than among adults ages 45 to 64, 65 to 74, and 75 or over (i.e., 74.4%, 79.6%, and 78.3%, respectively). Interestingly, these prevalences are higher than those typically reported in many other countries.10,18,19 Higher levels of flourishing are associated with fewer missed work days, 2 better academic performance among students, 20 better physical health, 6 effective learning, high productivity, strong creative skills, 21 and prosocial behavior.3,22,23
A wide range of factors are associated with mental disorders in young adults including sex, income, education, 24 physical health, physical activity, sleep, screen time, body image, substance use, social support, and violence/discrimination.3,6-9,25,26 In contrast, few studies identify factors related to positive mental health, especially among young adults. Understanding the distribution of positive mental health over a wide range of traits and behaviors will allow for better identification of subpopulations at risk of low levels of positive mental health, which could lead to an increased risk of developing mental disorders. 27 The present study aims to address this gap by identifying sociodemographic, lifestyle, and psychological correlates of flourishing mental health in a population-based sample of young adults.
Method
Data was drawn from Nicotine Dependance in Teens (NDIT), a longitudinal study that included 1294 participants ages 12 to 13 years at NDIT inception in 1999 to 2000, in a purposive sample of 10 high schools in Montreal, Canada. The sample included a mix of French and English-language schools, urban, suburban, and rural schools, and schools located in neighborhoods of low, moderate, or high socioeconomic status. Self-report questionnaires were completed every three months by students in the 10 study schools from Grade 7 to Grade 11, for a total of 20 data collection cycles during high school. After high school, self-report questionnaires were completed in Cycles 21 to 25 when participants were age 20.4, 24.0, 30.6, 33.6, and 35.2 years on average. At NDIT inception, participant characteristics were comparable to those of same-age youth participating in the 1999 provincially representative Québec Child and Adolescent Health and Social Survey. 28
Cross-sectional data for the current analyses were drawn from Cycle 23 (2017 to 2020) of NDIT. Cycle 23 is the first to incorporate positive mental health data in NDIT, providing a valuable opportunity to explore the unique mental health challenges and opportunities experienced by young adults, a group that has generally been underrepresented in research. To compare characteristics of participants at inception with current participants, data on sociodemographic variables (i.e., age, sex, born in Canada, and mother university-educated) were drawn from Cycle 1 (i.e., at NDIT inception). The NDIT study was approved by the Ethics Research Committee of the Centre de Recherche du Centre Hospitalier de l’Université de Montréal. Participants (who had all attained legal age in cycle 23) provided informed consent.
Study Variables
Positive mental health was measured using MHC-SF, which comprises 14 items selected to represent emotional well-being (three items), psychological well-being (six items), and social well-being (five items). Responses for all items were assessed in a 6-point Likert-type scale ranging from never (0) to always (5) in the past month. In previous work, the internal consistency and the composite reliability of the subscales of the MHC-SF were relatively high according to Cronbach's alpha coefficient (i.e., >.70 for all three subscales) and Jöreskog's rho (0.79 to 0.90). 29 The Cronbach's alpha of the MHC-SF subscales in NDIT Cycle 23 ranged from .84 to .91. Based on Keyes 3-level categorization of positive mental health (flourishing, moderate, languishing) using the MHC-SF scale, 2 flourishing mental health (yes, no) was defined as experiencing at least one of the three emotional well-being items and at least six of the 11 psychosocial functioning items (i.e., social and psychological well-being) always or most of the time during the past month. All other participants were categorized as not flourishing. Evidence that the categorization is valid is available.2,10,13
Factors investigated as potential correlates of flourishing mental health were selected based on a literature review and availability of data on the variable in NDIT. All factors were measured in Cycle 23, except sex which was measured in Cycles 1 to 11. These included 10 sociodemographic factors, eight lifestyle factors, and three psychological factors.
Sociodemographic factors included age, sex (male, female), lives alone (yes, no), lives with children (yes, no), lives with parent(s) (yes, no), in a relationship (yes, no), attended university (yes, no), currently a student (yes, no), currently employed (yes, no) and annual household income (<$29,999, $30,000–$100,000, ≥$100,000 CAN$, don’t know). All sociodemographic variables except age were used as categorical variables in the analyses.
Lifestyle factors included past-year daily cigarette smoking status (yes, no), past-year weekly/daily binge drinking (yes, no), and past-year daily marijuana, cannabis, and hashish use, (yes, no). Movement behaviors included team sport participation (yes, no), meeting moderate-to-vigorous physical activity (MVPA) guidelines (yes, no), sleep quality (low, high), work/school screen time (mean hours/week), and meets leisure screen time guidelines (yes, no). Meeting MVPA guidelines (at least 150 min per week 30 ) was assessed using the short version of the International Physical Activity Questionnaire. Sleep quality over the past month was reported from poor to excellent. Hours of screen time per day was measured using questions adapted from the Ontario Student Drug Use and Health Survey. 31 All lifestyle variables except work/school screen time were used as categorical variables in analyses.
Finally, psychological factors included general coping ability (poor to excellent), depressive symptoms (none/mild, moderate/severe), and general anxiety symptoms (none/mild, moderate/severe). The general coping ability variable 15 was used as a continuous variable. Depressive symptoms were measured using the major depressive inventory 32 which comprises 12 items inquiring about the frequency of depressive symptoms in the past 2 weeks with responses ranging from at no time (0) to all the time (5). We used a cutoff score of 25 to differentiate participants with at least moderate depressive symptoms from participants with no depressive symptoms or mild symptoms. 32 In NDIT, the internal consistency measured using Cronbach's alpha was α = .89. Anxiety symptoms were assessed using the general anxiety disorder questionnaire which includes seven items measuring the frequency of anxiety symptoms in the past 2 weeks, with response options ranging from not at all (0) to nearly every day (3). A cutoff score of 10 was used to identify participants with at least moderate anxiety symptoms (yes, no). 33 In the NDIT sample, the internal consistency measured using Cronbach's alpha was α = .91. Depressive and anxiety symptoms were used as categorical variables in the analyses.
Table S1 in the Supplemental Material describes questionnaire item(s) for each study variable, response options, recoding for analysis, data on psychometric properties and validity if available, and references.
Data Analysis
Descriptive analyses included checking for missing data, identifying outliers, and assessing distributions. Means (SD) and medians (IQR) were computed for continuous variables, and proportions were computed for categorical variables. To minimize issues of multiple testing, we conducted a set of three logistic regression models for each potential correlate of flourishing mental health (yes, no). Each set comprised an independent study which addressed a specific hypothesis (one per potential correlate) within which only three statistical tests were performed (i.e., an unadjusted model (Model 1), a minimally adjusted model with a common set of covariates (age, sex) across all potential correlates (Model 2), and a more fully adjusted model which added covariates over and above age and sex based on VanderWeele's Disjunctive Cause Criterion 34 (Model 3).
All statistical analyses were conducted using R software version 4.1.3.
Results
Of 1,294 NDIT participants who completed Cycle 1 (at NDIT inception), 799 (56.1% female, mean (SD) age = 30.6 (1.0) years) completed the cycle 23 questionnaire and 792 (61.2% of 1294) were retained for analyses. Among those not retained (n = 502), 495 did not complete Cycle 23 and seven participated in Cycle 23 but did not provide data on positive mental health. Participants retained were younger on average than those not retained. Relatively more participants retained were female and had university-educated mothers (Table 1). For Cycle 23, missing data did not exceed 8% for any variable.
Selected Characteristics of Participants Retained and Not Retained in Cycle 23, NDIT 1999-2020.
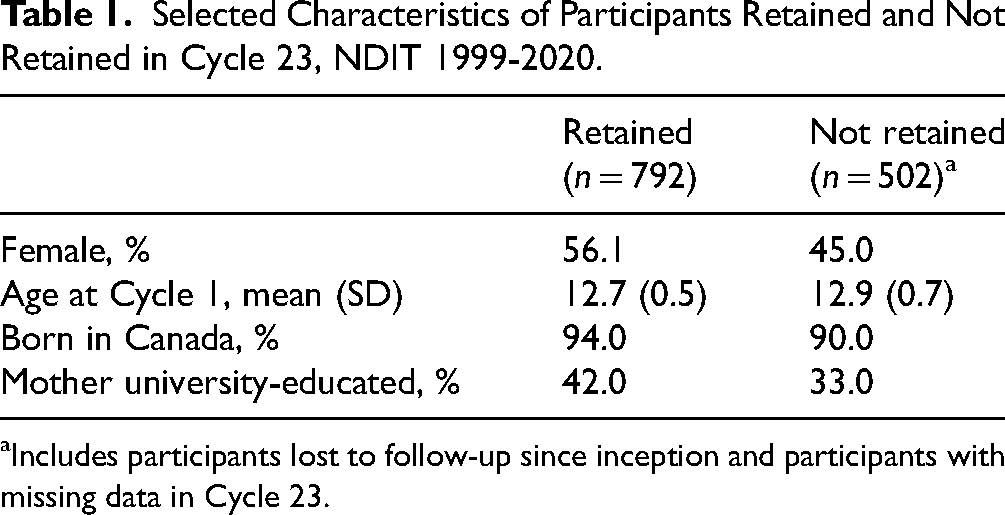
Includes participants lost to follow-up since inception and participants with missing data in Cycle 23.
Of 792 participants retained for analysis, 39.4% reported flourishing mental health including 39.9% of females and 38.8% of males. Table 2 shows the proportion of participants that reported flourishing mental health according to each potential correlate. The highest proportions of flourishing were observed among participants with very good (55.4%) or excellent (70.3%) coping ability, high sleep quality (51.1%), meeting leisure screen time guidelines (50.2%), an annual household income ≥$100,000 (48.0%), and currently being a student (47.1%). The lowest proportions of flourishing were observed among participants with poor coping ability (0.0%), moderate/severe depressive symptoms (3.4%), moderate/severe anxiety symptoms (12.1%), poor/fair sleep quality (23.5%), and participants with an annual household income <$29,999 (24.7%).
Proportion of Participants With Flourishing Mental Health in Each Category of Each Potential Correlate, NDIT 1999-2020.
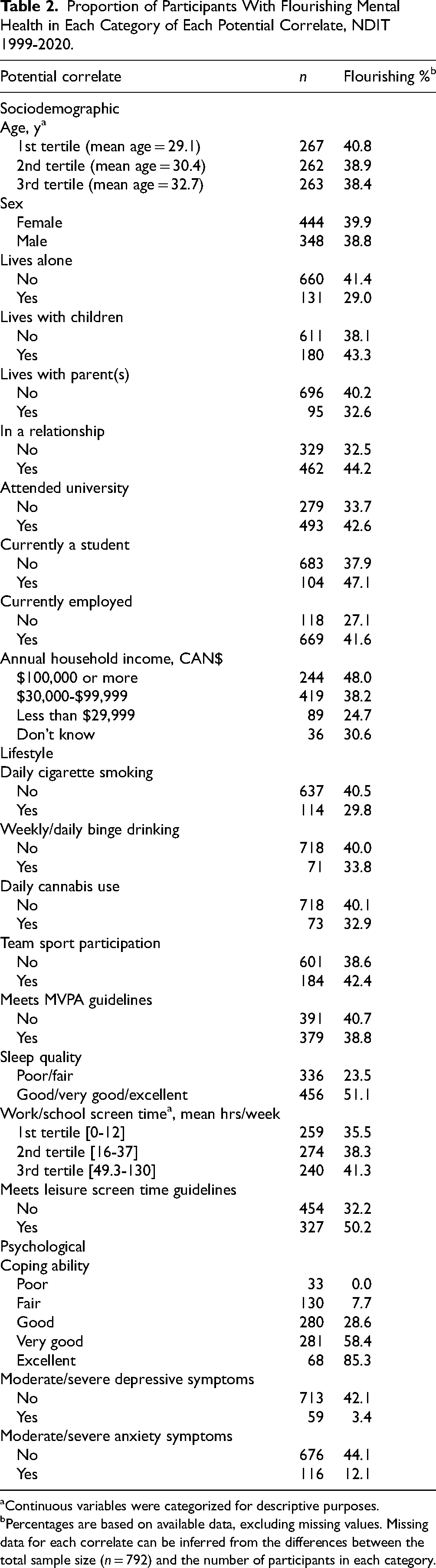
Continuous variables were categorized for descriptive purposes.
Percentages are based on available data, excluding missing values. Missing data for each correlate can be inferred from the differences between the total sample size (n = 792) and the number of participants in each category.
Table 3 shows the results of the unadjusted (Model 1) and minimally and fully adjusted logistic regression models (models 2 and 3). Ten of the 21 potential correlates investigated were associated with flourishing mental health in fully adjusted multivariable models (Model 3). For sociodemographic variables, we observed that being in a relationship (OR [95% CI]: 1.64 [1.22, 2.21]), attended university (OR [95% CI]: 1.44 [1.05, 1.99]), and being currently employed (OR [95% CI]: 1.97 [1.27, 3.11]) were associated with higher odds of flourishing mental health. Living alone (OR [95% CI]: 0.58 [0.38, 0.86]) and having lower annual household income (OR [95% CI]: 0.37 [0.20, 0.64]) were associated with lower odds of flourishing mental health. For lifestyle variables, high sleep quality (OR [95% CI]: 3.45 [2.53, 4.73]) and meeting leisure screen time guidelines (OR [95% CI]: 2.12 [1.59, 2.85]) were associated with higher odds of flourishing mental health in fully adjust models. For psychological variables, higher levels of coping ability (OR [95% CI]: 3.11 [2.58, 3.80]) were associated with higher odds of flourishing mental health whereas reporting depressive (OR [95% CI]: 0.05 [0.01, 0.15]) or anxiety symptoms (OR [95% CI]: 0.17 [0.09, 0.29]) were associated with lower odds of flourishing mental health.
Odd Ratios and 95% Confidence Intervals for Potential Correlates of Flourishing Mental Health in Young Adults (n = 729-792), NDIT 1999-2020.
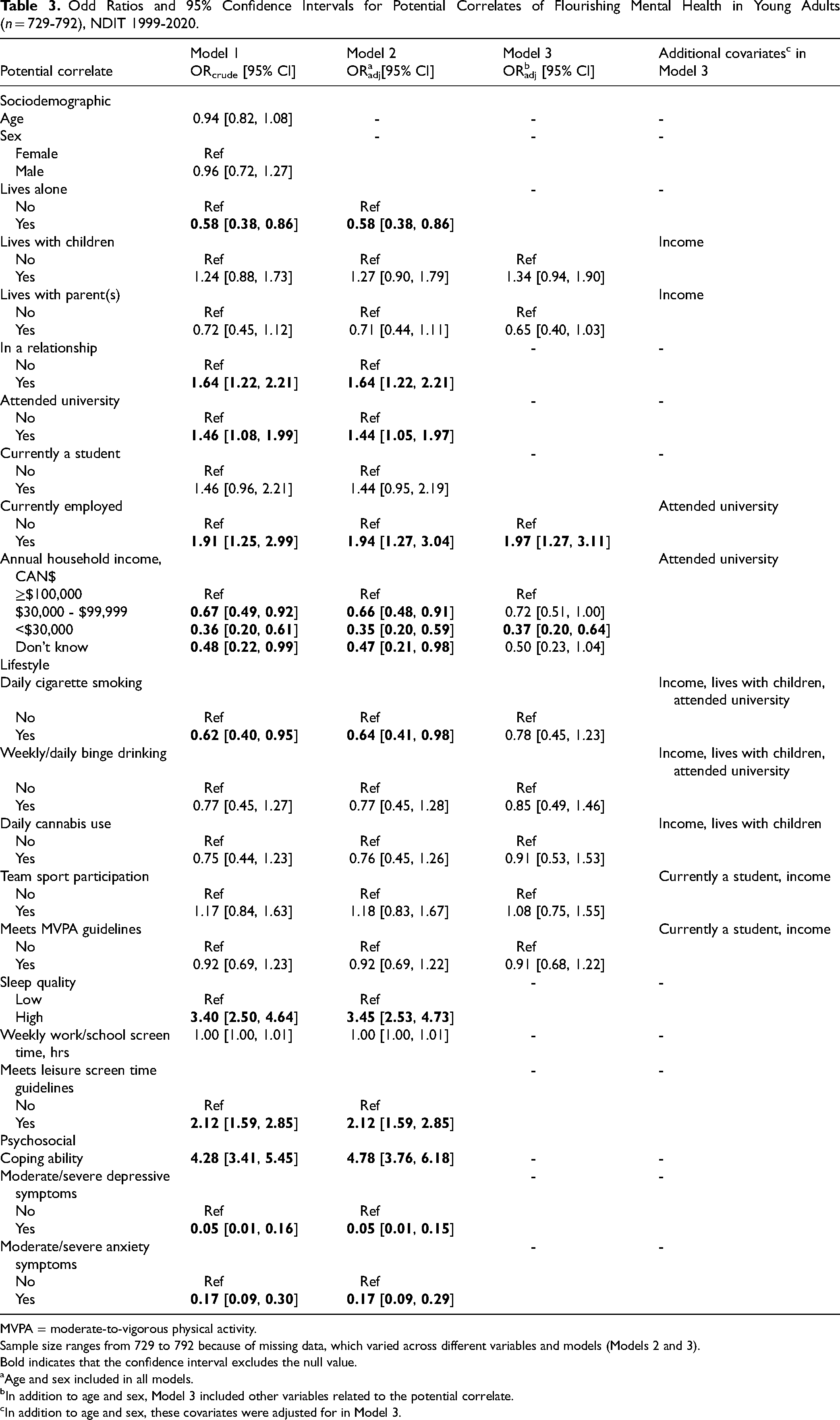
MVPA = moderate-to-vigorous physical activity.
Sample size ranges from 729 to 792 because of missing data, which varied across different variables and models (Models 2 and 3).
Bold indicates that the confidence interval excludes the null value.
Age and sex included in all models.
In addition to age and sex, Model 3 included other variables related to the potential correlate.
In addition to age and sex, these covariates were adjusted for in Model 3.
Discussion
In this study, we describe flourishing mental health according to a range of potential correlates in a population-based sample of young adults. The proportion of young adults with flourishing mental health (39.4%) was markedly lower than the 71% observed among Canadians ages 25 to 44 in the CCHS, 6 but does align with proportions observed in other studies using the MHC-SF.18,19,35,36 Differences with CCHS 2012 data may relate to the younger age of NDIT participants. The following paragraphs discuss findings on the correlates of flourishing.
Consistent with previous studies,37,38 we detected an inverse association between living alone and positive mental health. Only 5% of NDIT participants who lived alone were in a relationship, possibly reflecting a personal preference to live alone. However, 72% of single adults ages 20 to 34 in Canada intend to eventually form a union and 67% would like to have children. 39 Because the number of people living alone in Canada is increasing, 40 the issue of lower mental health in this subgroup is of high societal importance. Participants in our sample who were in a relationship had higher odds of positive mental health, which aligns with extant literature.41,42 In addition to the social interaction inherent in cohabiting, being in a strong relationship can be very fulfilling 43 ; it can contribute to a sense of security and happiness, 44 and reduce feelings of isolation and loneliness. 45 Healthy relationships buffer life stresses 46 and often bring a sense of purpose and commitment by working toward shared goals. 47 Studies on communication patterns and overall quality of the relationship are needed to identify the underpinnings of the association between being in a relationship and positive mental health.
Consistent with previous studies,3,6,48-50 higher education was positively associated with flourishing mental health. Possible mechanistic underpinnings include availability of education-related resources (e.g., income, health insurance), cognitive skills, and social integration. 51 NDIT participants with flourishing mental health were more likely to be employed, which also aligns with the literature. 52 Employment can provide a sense of purpose, a structured routine, skill development and social interaction, 53 all of which contribute positively to mental health. Research on what constitutes an optimal job/workplace given an individual's context is needed to better understand the association between employment and positive mental health. Additionally, employment generates an income, which is associated with happiness.54,55 Our study supports reports of a positive linear association between income and positive mental health.3,6,48 People with flourishing mental health likely generate higher levels of income by being more productive, 13 and higher levels of income lead people to access more resources, which may lead to flourishing.
Concordant with past work,49,56,57 cigarette smoking was inversely associated with positive mental health. From a eudaimonic perspective, smoking can contribute to social isolation as it becomes less socially acceptable. 58 Moreover, the addictive nature of nicotine can be a barrier to making positive lifestyle changes, 59 thus hindering personal growth and self-improvement efforts which are linked to positive mental health. From a hedonic perspective, when not smoking, smokers might feel dependance symptoms such as irritability, anxiety and hedonic dysregulation (i.e., the feeling that there is little pleasure in life, and once-rewarding activities lose their appeal). 60 However, in our analysis (Model 3), after adjusting for income, living with children, and education, the confidence interval for the estimate encompassed the null, indicating no association between daily smoking and positive mental health. This suggests that these covariates may play a role in the relationship between smoking and mental health, highlighting the importance of considering socioeconomic and life circumstances when examining this association. Enabling young adults to flourish may contribute to reduced engagement in risky/unhealthy lifestyle behaviors such as smoking, and if so, promoting positive mental health is an important goal for health promotion efforts. 56
The present study adds to growing evidence on the association between positive mental health and movement behaviors (i.e., physical activity, sleep, and sedentary behavior). Our finding of no association between meeting MVPA guidelines and flourishing contradicts previous reports.61-63 This could be because we used a dichotomous variable to represent this exposure, which reduces variability in the measure substantially. About half of NDIT participants met MVPA guidelines, with some doing the minimum time required and others attaining more than three times the recommended time. It is possible that an association cannot be detected because of reduced variability (i.e., meeting MVPA guidelines might not be the optimal threshold to explore this association). Similar to previous work, 64 our results show a strong positive association between sleep quality and positive mental health, a relationship that might be bidirectional. 65 As bedtime procrastination is higher at younger ages, 66 future studies should evaluate interventions prioritizing sleep quality to maximize mental health and well-being in young adults. Meeting Canada's 24-Hour Movement Guidelines for Adults (18-64 years old) guidelines on screen time is associated with higher odds of flourishing mental health. Regardless of potential benefits, excess screen time can limit more healthful activities such as physical activity and social interactions. 67 Guidelines reflect growing awareness of the integrated nature of movement behaviors that together influence mental health outcomes. 68 Investigating the link between well-being and risky behaviors such as screen use increases understanding of factors that lead to, and ways to prevent, engagement in such behaviors.
Consistent with studies in other populations,6,22,27,69,70 depressive and anxiety symptoms were associated with lower positive mental health. Although distinct constructs, depression and positive mental health are inversely correlated in adults.27,69,70 In a 10-year longitudinal study, improvements in mental well-being predict declines in mental distress, while declines in mental well-being predict improved mental distress. 69 Our results align with studies supporting that positive mental health and anxiety are related but distinct constructs.2,27 Notably, participants were asked about current symptoms, rather than diagnoses. To inform the development of effective interventions, research is needed to identify what predicts, enhances, and maintains flourishing in young adults with and without symptoms of mental disorders.
Limitations
Limitations of this study include its cross-sectional design which precludes causal inference. Bidirectionality of the associations investigated could not be ascertained. Data on numerous factors possibly associated with positive mental health (e.g., discrimination, spirituality, violence, parenting style) were not collected in NDIT. Measurement error especially in self-report data, is possible. For example, socially undesirable behaviors such as binge drinking and cigarette smoking may be underreported. The relatively small sample size may have limited the ability to detect some associations. Use of a purposive sample at inception and loss to follow-up over time may have limited generalizability of the findings. Loss to follow-up is also a possible source of selection bias.
Implications
This study identifies correlates of flourishing mental health that are amenable to public health interventions among young adults in Canada. Future longitudinal studies can help determine whether these are causal. In the interim, correlates of flourishing mental health identified herein may indicate subgroups which could benefit from targeted intervention to promote positive mental health.
Conclusion
Findings on the correlates of flourishing mental health in this study contribute to growing understanding of the association between positive mental health and sociodemographic, lifestyle, and psychological indicators among young adults. If the findings are replicated, program planners may need to consider the correlates identified herein in conceptualizing public health strategies to improve positive mental health in young adults.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437251347166 - Supplemental material for Sociodemographic, Lifestyle, and Psychological Factors Associated With Flourishing Mental Health in Young Adults: Facteurs sociodémographiques, liés au mode de vie et psychologiques, associés à une bonne santé mentale chez les jeunes adultes
Supplemental material, sj-docx-1-cpa-10.1177_07067437251347166 for Sociodemographic, Lifestyle, and Psychological Factors Associated With Flourishing Mental Health in Young Adults: Facteurs sociodémographiques, liés au mode de vie et psychologiques, associés à une bonne santé mentale chez les jeunes adultes by Yasmien Deis, MSc, Jennifer O’Loughlin, PhD and Isabelle Doré, PhD in The Canadian Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Isabelle Doré is supported by an FRQS Junior 2 salary award. Jennifer O'Loughlin held a Canada Research Chair in the Early Determinants of Adult Chronic Disease 2004-2021. The NDIT study was supported by the Canadian Cancer Society (grant numbers 010271, 017435, 704031).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.