
Abstract
Objectives
Children with externalizing disorders commonly show emotion dysregulation and callous–unemotional (CU) traits. However, it is unclear whether emotion dysregulation and CU traits share underlying neurobiology that can be predictive of psychosocial treatment outcomes. In this preliminary study, we examined neural correlates of externalizing psychopathology dimensions and their prediction of treatment outcomes.
Methods
We analyzed a pilot sample of 17 children with an externalizing disorder (9–12 years; 10.45 ± 1.02) who underwent structural magnetic resonance imaging (MRI) before participating in a 15-week psychosocial group intervention targeting conduct problems. We examined cross-sectional associations between emotion dysregulation or CU traits and cortical thickness (anterior cingulate cortex [ACC] and insula) and amygdala volume at baseline. We then examined whether the pre-treatment brain–behaviour relationships were linked to reduction in conduct problems post-treatment.
Results
Lower ACC and insula thickness as well as amygdala volume was associated with greater levels of emotion dysregulation and CU traits at baseline (pre-treatment, r = |0.36–0.61|). There was a significant three-way interaction between emotion dysregulation/CU traits, left insula/right rostral ACC, and treatment (pre/post; β = −1.01 to 3.6). Overall, greater baseline insular and rostral ACC thickness was related to reductions in conduct problems following group-based psychosocial intervention regardless of baseline emotion dysregulation and CU trait levels.
Conclusions
The results provide preliminary evidence of shared neural signatures underlying both emotion dysregulation and CU traits. Additionally, alterations in frontolimbic brain structure may be useful predictors of pre-treatment associations with externalizing psychopathology dimensions and post-treatment behavioural outcomes.
Plain Language Summary Title
Frontal cortical thickness and externalizing psychopathology are associated with treatment outcomes in children with externalizing problems
Plain Language Summary
Children with externalizing disorders commonly show emotion dysregulation and callous–unemotional (CU) traits. However, it is unclear whether emotion dysregulation and CU traits share underlying neurobiology that can be predictive of psychosocial treatment outcomes. In this preliminary study, we examined neural correlates of externalizing psychopathology dimensions and their prediction of treatment outcomes. Among 17 children with externalizing disorders, we found that three brain regions (anterior cingulate cortex, insula, and amygdala) were associated with emotion dysregulation and CU traits prior to receipt of treatment. Furthermore, greater thickness of the rostral anterior cingulate cortex and insula at baseline was linked to decreased conduct problems following the intervention regardless of baseline emotion dysregulation and CU trait levels. The results provide early evidence that alterations in frontolimbic brain structure may be useful predictors of post-treatment behavioural outcomes.
Introduction
The prevalence of externalizing disorders has been increasing worldwide 1 and recent estimates show that rates of diagnosis range from 0.6% to 4.9% prior to the age of 7. 2 A first-line treatment for children with externalizing disorders is parent–child group interventions which have been shown to reduce behavioural problems in children with externalizing disorders, such as conduct disorders.3,4 However, these treatment options are less effective in children with higher callous–unemotional (CU) traits. 5 Elevated emotional and behavioural problems coupled with alterated brain development may interact with environmental risk factors leading to increased severity of externalizing behaviours which can persist into adulthood. 6 Given the impairment that elevated externalizing symptoms can confer throughout the lifespan, 7 it is critical to understand the biological and behavioural factors that may predict severity and persistence of symptoms and whether these relationships influence treatment outcomes.
Two dimensions of psychopathology, emotion dysregulation and CU traits, are associated with the severity of externalizing problems in children.8,9 Emotion dysregulation in childhood is characterized by elevated irritability and emotional lability, whereas CU traits include low levels of guilt and empathy. 8 Variation in the severity of these dimensions may predict treatment response in children with elevated externalizing behaviours.10–12 Although CU traits and emotion dysregulation have been studied separately and thought to be somewhat distinct dimensions of emotional versus behavioural dysfunction, 13 recent work suggests emotion dysregulation and CU traits overlap in children with externalizing disorders.14–17 Understanding the neurobiological overlap between these dimensions may provide insight into whether these are biologically distinct and have differing influences on the severity of externalizing psychopathology and treatment response.
Several studies have shown that heterogeneity of brain structure in corticolimbic regions is associated with variation in both emotion dysregulation and CU traits.8,18–24 The high comorbidity of symptom presentation among children with externalizing behaviours,16,25 along with overlapping structural neuroimaging findings may suggest that CU traits and emotion dysregulation have shared underlying neurobiological correlates. Our prior work found that decreased cortical thickness and subcortical volume in limbic regions were associated with elevated externalizing dimensions, including emotion dysregulation and CU traits, in a population-based sample of young children. 8 Additionally, we found that higher cortical thickness in key frontal regions at baseline was linked to reduced externalizing symptoms over time. These results provide some evidence that there may be shared brain networks underlying different externalizing psychopathology dimensions. Amongst the several regions that have been shown to be associated with externalizing psychopathology, three key regions have been consistently linked to externalizing symptoms, encompassing emotion dysregulation and CU traits. These regions include the anterior cingulate cortex (ACC),18,26 insula,19,20 and amygdala.21,22 The ACC and insula play an important role in top-down emotional regulation 27 through connections to the amygdala.6,28,29 Decreased volume/thickness of the ACC and insula may influence the top-down modulation of the amygdala30,31 potentially contributing to risk of emotional regulation impairment and externalizing psychopathology.
Current clinical guidelines support the use of group-based behavioural parent training programs and social-cognitive problem-solving interventions for children with externalizing disorders.11,32 Interventions such as the Coping Power Program 33 have been shown to be efficacious in reducing conduct problems for children with externalizing behaviours, including those with comorbidities.10,34 Although symptom changes are often examined pre- and post-intervention, few studies have explored whether baseline neurobiological factors are associated with psychosocial treatment benefits. Such an examination can elucidate the subset of children that are most likely to benefit from current interventions and inform more tailored approaches for those who do not benefit sufficiently. The present pilot study investigates the relationships between brain structure of specific cortico-amygdalar regions with emotion dysregulation and CU traits in a small small sample of children with clinically significant externalizing behaviours and examines whether baseline brain–behaviour relationships predict post-treatment changes in conduct problems. We first hypothesized that greater emotion dysregulation and CU traits (more impairment) would be associated with lower cortical thickness in the ACC and insula as well as reduced volume of the amygdala at baseline (i.e., pre-treatment). We also hypothesized that the relationship between increased ACC/insula thickness and lower emotion dysregulation or CU traits would be linked to reductions in conduct problems at post-treatment follow-up.
Methods
Participants and Procedure
Participants were drawn from a subset of a sample of children aged 9–12 years (n = 21) presenting to a clinic for children with disruptive behaviours who underwent treatment through the Coping Power program (n = 61), an established intervention that supports the development of emotional and behavioural skills to reduce externalizing behaviour and build more adaptive relationships. The clinic-modified program includes a 15-session child and parent component.33,35,36 The Coping Power child component includes modules to help children learn strategies to identify their feelings, regulate their emotions, challenge maladaptive thinking patterns and problem-solve. These skills are practiced through interactive group activities and generalized through home practice. The behavioural parent component includes modules that teach strategies to regulate parent emotion, challenge maladaptive parental thinking patterns and further develop skills to strengthen parent–child relationships, establish home routines and consistency, and provide effective consequences for children's misbehaviour.
The current study was approved by the Research Ethics Board; all parents consented with child assent. Participants received a $20 honorarium as well as a photo of their brain scan for participating in this study. Potential participants were screened at the initial assessment based on the following inclusion criteria: 9–12 years of age, estimated IQ > 70 on the Kaufman Brief Intelligence Test-Second Edition (KBIT-2), 37 and absence of a diagnosis of Autism Spectrum Disorder or Pervasive Developmental Disorder as determined by a pre-admission phone screening. Further inclusion was based on clinically significant externalizing behaviours as determined by a positive diagnosis of oppositional defiant disorder (ODD) or conduct disorder (CD) on the Diagnostic Interview Schedule for Children Computerized (C-DISC) 38 and/or an at-risk or clinically significant score of t > 65 on either of the aggressive or rule-breaking behaviour syndrome scales on the Child Behaviour Checklist. 39 Participants who met study inclusion criteria and enrolled in group treatment (i.e., the Coping Power Program 33 ) were invited to participate in the current pilot study, including baseline and post-treatment (i.e., following participation in the 15-week Coping Power program) magnetic resonance imaging (MRI) scanning. Following the removal of participants with poor quality scans and outlier values, there were 17 participants analyzed in the current study (details below).
Measures
Child Behaviour Checklist (CBCL)
The CBCL is a 113-item caregiver-report questionnaire used to assess behavioural and emotional problems in children and adolescents. 39 To measure emotion dysregulation for the cross-sectional (pre-treatment) analysis, we used the dysregulation profile raw score (i.e., sum of anxious/depressed, attention problems, and aggressive behaviour subscale scores). 40 Higher emotion dysregulation scores indicate greater problems.
Inventory of Callous–Unemotional Traits (ICU)
The ICU is a 24-item caregiver-reported questionnaire that assesses CU traits. 41 It has been widely used in children and youth with externalizing behaviours.23,42 There are three subscales to the ICU; uncaring, callousness, and unemotional symptoms, which can be summed to a total CU score. This total CU score was used in the cross-sectional (pre-treatment) brain–behaviour analysis. A higher total CU score indicates the presence of greater CU traits and severity.
Strengths and Difficulties Questionnaire (SDQ)
The SDQ is a 25-item caregiver-reported questionnaire that examines five behavioural domains: emotional symptoms, conduct problems, hyperactivity-inattention, and peer problems, which can be summed to produce a total difficulties composite score, in addition to a prosocial skills symptom score. 43 The SDQ was downloaded from www.sdqinfo.org. For the present study, the conduct problems raw subscale score was used to measure conduct problems pre- and post-treatment as an outcome measure of the group-based psychosocial treatment intervention, similar to prior work.44–46 A higher conduct problem score indicates greater problems.
MRI Acquisition and Processing
MRI data was collected on a 3 Tesla GE MR750 (General Electric, Milwaukee, WI) scanner using an eight-channel head coil. As part of a multi-modal sequence (40 min total scan time), an anatomical T1-weighted MRI was obtained (Sagittal BRAVO, Repetition Time (TR) = 6.7 ms, Echo Time (TE) = 3.0 ms, flip angle = 8, voxel size = 0.9 mm isotropic, duration 5 min). Prior to the first MRI appointment, participants were sent a social storybook, created for this specific study, with photos of the imaging facility and the steps taken to prepare for scanning. Participants were able to select a movie to watch during anatomical scans. Preprocessing of T1-weighted images was done using the fMRIprep pipeline. 47 Cortical thickness and subcortical volumes for all regions were derived using the Desikan-Killiany Atlas in FreeSurfer (v 5.3.0).48,49 The regions of interest (ROIs) included in the current study were left and right amygdala volume, insula thickness, and rostral and caudal ACC thickness (eight total regions), based on prior work implicated alterations of these regions being linked to externalizing problems.18–24,26 We limited the ROIs analyzed in the current study given the small sample size leading to limited power to detect effects. We chose to analyze the eight regions that have been consistently found to be implicated in the literature and show large effects.
Quality Control (QC)
We implemented a QC procedure to ensure that participants included in the analysis had good quality scans. 50 Visual QC was conducted by reviewing the output pages from the fMRIprep pipeline, and each scan was visually inspected by two independent raters for motion artefacts (L.P. and H.N.; see Nakua et al. 50 and Supplementary Section 2 for details; inter-rater reliability using Fleiss’ kappa, κ = .79). Of the 21 participants with available MRI scans, two participants failed visual and quantitative QC due to poor scan quality, resulting in 19 participants eligible for analysis.
Statistical Analysis
Due to the small sample size of the current pilot study and risk of influential outliers that may impact the interpretability of results, the data was qualitatively inspected for outliers prior to conducting the main analyses. First, using the ggplot2 package in R, we visualized box plots of each behavioural and brain variable and removed participants with outlier values (i.e., values above or below the third and first quartile; 1.5 × the interquartile range 51 ). Second, using the ggplot2 package in R, we visualized scatterplots of each behavioural and brain variable to determine data points that were qualitatively much higher or lower relative to other participants. Two outliers were identified and removed from subsequent analyses: one female participant with consistently low behavioural scores which may be indicative of parent/caregiver not reliably completing the administered measures and one male participant with unusually high cortical thickness values which could be due to noise.
Cross-Sectional Brain–Behaviour Associations
To investigate the relationship between brain structure and behaviour, we conducted a series of Pearson correlation analyses to estimate pre-treatment associations between cortical thickness and subcortical volume of ROIs, emotional dysregulation, CU score, and SDQ-derived conduct scores (baseline). We also assessed the precision of the associations (i.e., 95% confidence intervals [CIs]). SDQ-derived conduct problems were also included in these analyses as the outcome variable of interest in the subsequent linear mixed models. Given the small sample size and possibility of inflated Type-II errors for statistical inference, 52 we were primarily interested in the Pearson correlation value (effect) and 95% CI (precision) for this analysis, and less focus was given to p-value thresholds.
Linear Mixed Models Predicting Treatment Change in Conduct Problems
Separate linear mixed-effects models were fit to estimate the influence of the three-way interaction between time, baseline externalizing psychopathology dimensions (i.e., CBCL dysregulation profile/CU total score), and brain metrics (independent variable) on post-treatment conduct problems (dependent variable). There were five participants missing post-treatment conduct problem scores; however, all 17 participants were run given that linear mixed-effect models can handle missing data.53,54 Given the small sample size and preliminary nature of the current study, the ROIs included in this analysis were only those that surpassed a predetermined Pearson correlation cut-off from the cross-sectional correlational analysis (r > .30; moderate association
55
). Fixed effect covariates included time (pre- and post-treatment), CBCL dysregulation scores or CU trait scores, and thickness/volume of ROI, the interaction between these three variables, and pre-treatment SDQ-derived conduct problems. Random effects included participant IDs. Age was not included as a fixed effect covariate given the narrow age range. Models with a significant three-way interaction were interpreted. All analyses were run in R (version 4.1); the linear mixed-effects models were run using the lme4 package.
56
and the estimated means and CIs were run using the emmeans package.
57
See below for an example of the linear mixed effect model run (where kl refers to subject k and time/treatment l).
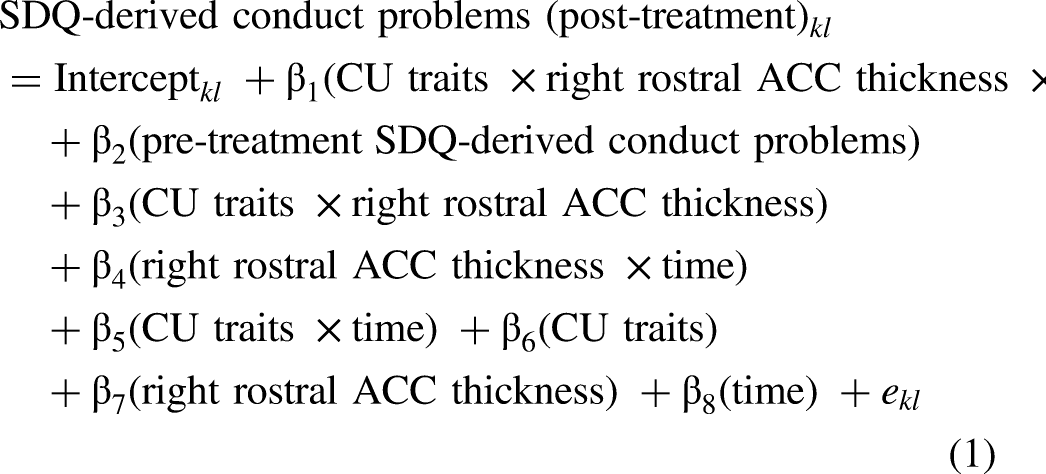

Results
There were 17 participants analyzed in the current study; demographic characteristics are summarized in Table 1. Within the sample, 58.8% were taking psychotropic medication at the time of assessment. Most participants came from mid- to high socioeconomic status (SES) homes, with 76.5% of primary caregivers having completed post-secondary education. There were five participants with missing post-treatment behavioural data. See supplementary information for further details on participant exclusion.
Participant and Caregiver Demographics (n = 17).
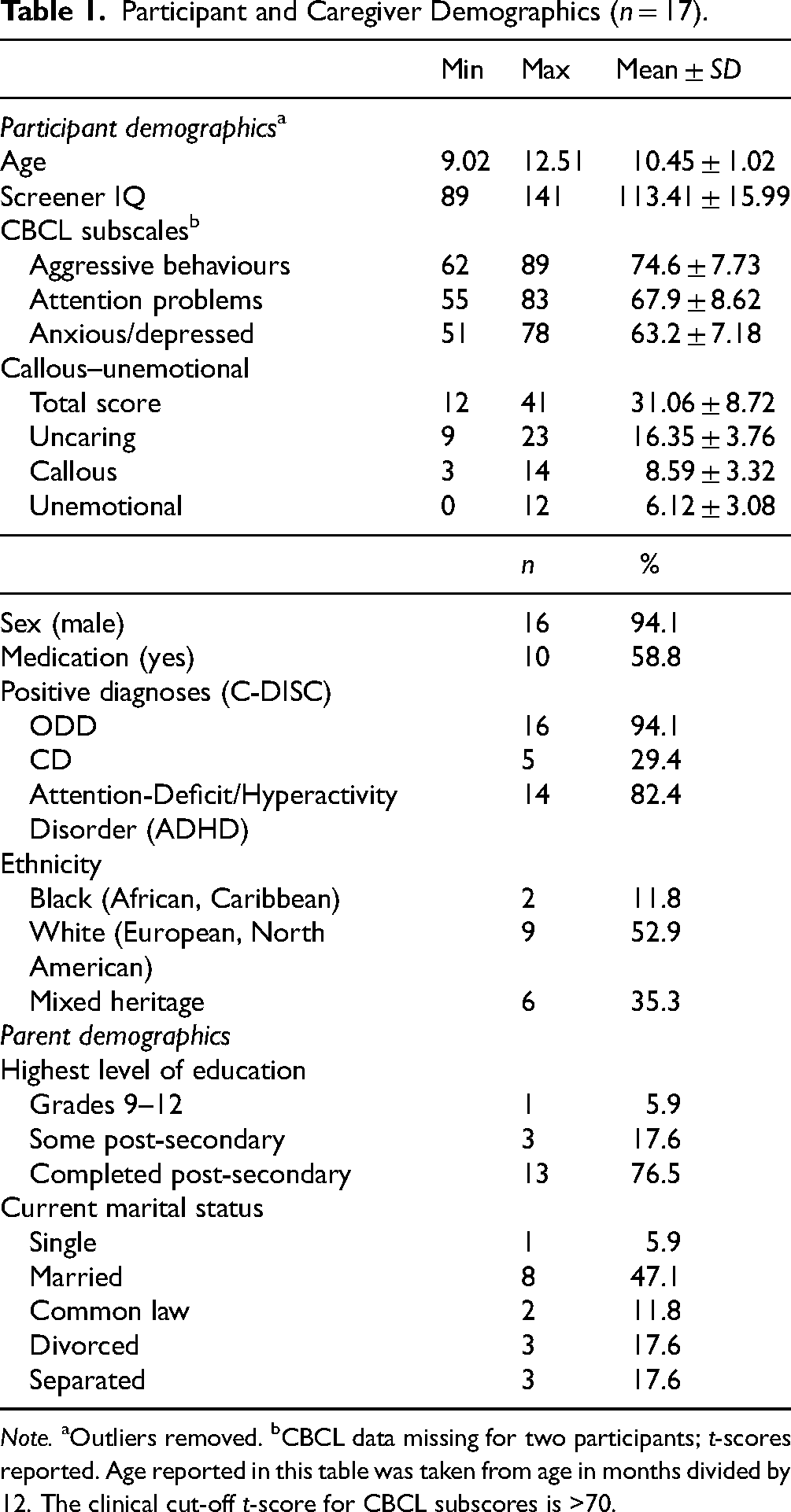
Note. aOutliers removed. bCBCL data missing for two participants; t-scores reported. Age reported in this table was taken from age in months divided by 12. The clinical cut-off t-score for CBCL subscores is >70.
Cross-Sectional Brain–Behaviour Associations
Baseline emotion dysregulation, CU traits, and conduct problems showed negative associations with brain structure, such that higher CU and emotional dysregulation scores (greater impairment) were associated with decreased cortical thickness (Figure 1). Associations between CU traits and ROIs that met the pre-determined cut-off (r > .30) included right insula (r = −.408, p = .104), left insula (r = −.514, p = 0.035), right rostral ACC (r = −.609, p = .009), left rostral ACC (r = −.401, p = .110), and right caudal ACC (r = −.401, p = .110). Associations between emotion dysregulation and ROIs that met the pre-determined cut-off included the left amygdala (r = −.459, p = .085) and left insula (r = −.365, p = .180). As shown in Figure 1, the majority of ROIs showed a negative relationship with the externalizing psychopathology dimensions examined. Given the small pilot sample, the majority of 95% CI error bars cross zero suggest a high degree of imprecision in the correlation, although the relationship between CU traits and the right rostral ACC and left insula had CIs that did not cross zero.
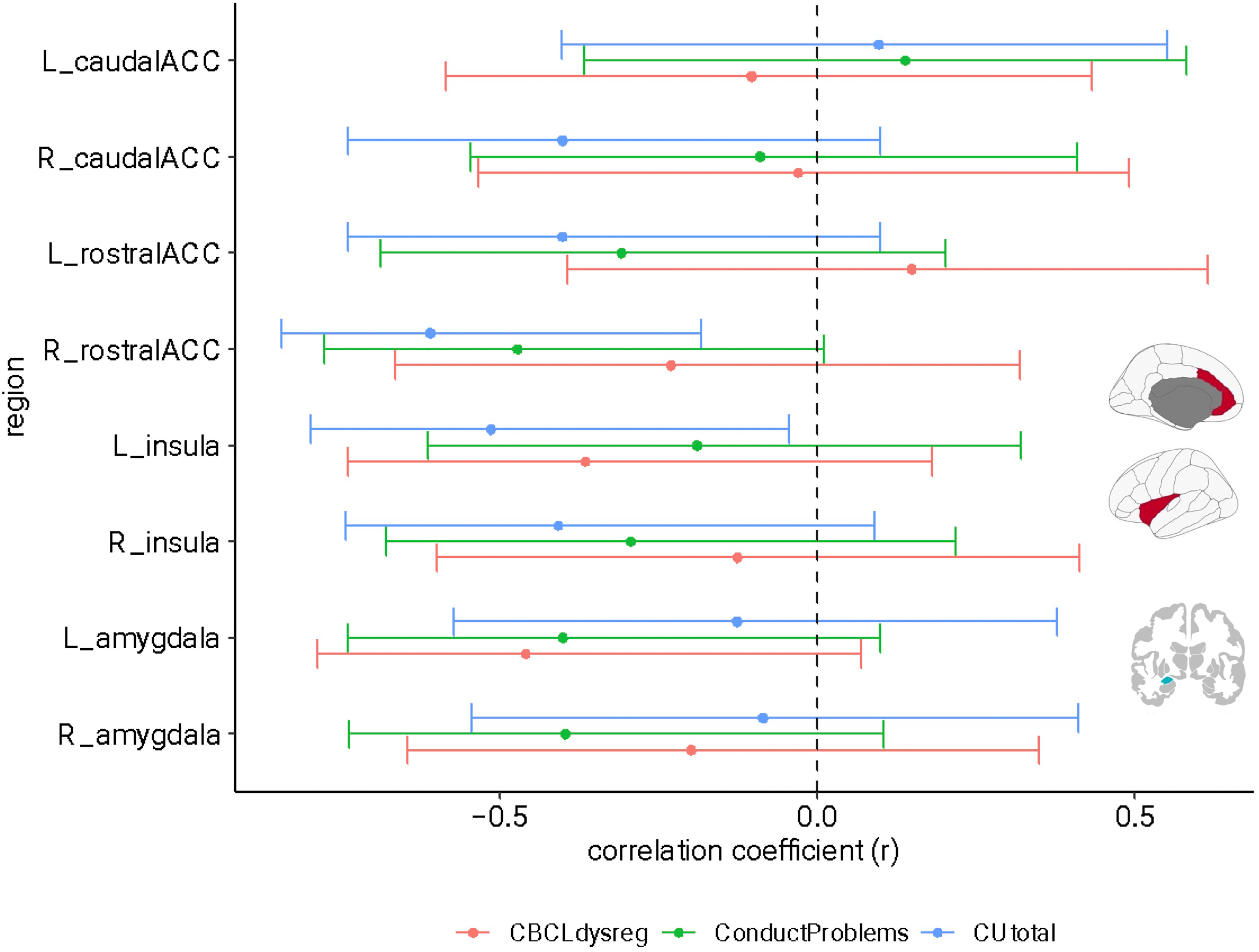
Correlation coefficients and confidence intervals derived from the initial cross-sectional analyses. Note. The red confidence interval line represents baseline emotion dysregulation scores, the green represents baseline conduct problems scores, and the blue represents baseline CU trait scores. The associations generally showed a negative pattern of association despite the wide confidence intervals (i.e., impaired behavioural indices were associated with reduced cortical thickness and amygdala volume). The brain regions depicted on the bottom right of the figure are the a priori ROIs analyzed in this study.
Linear Mixed Models Associated with Treatment Change in Conduct Problems
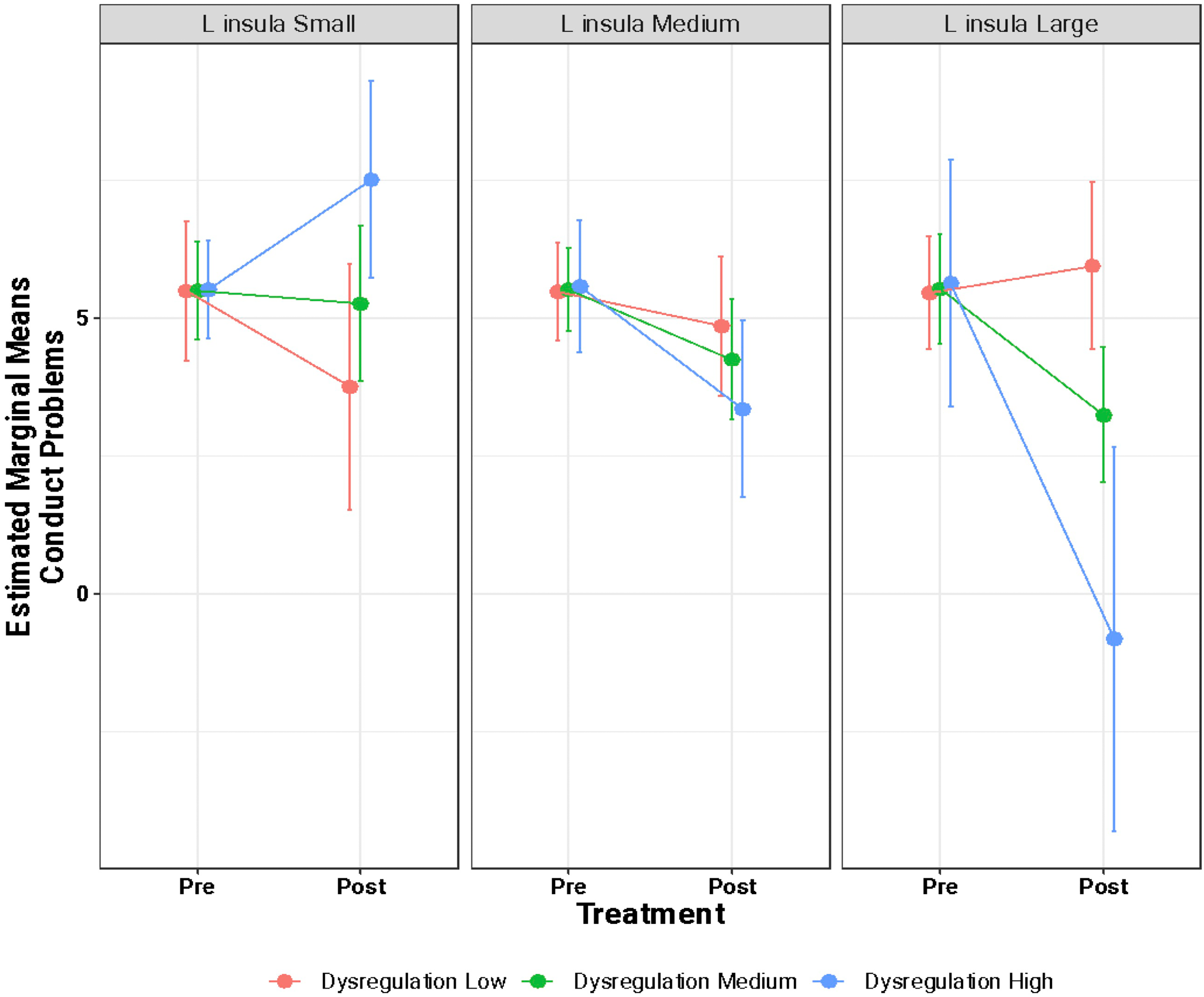
Using linear mixed-effects models, we did not find a main effect of brain structure or baseline CU or emotional dysregulation on change in conduct problems following treatment. However, an interaction effect (significance uncorrected) was found across three models: emotion dysregulation × left insula × time (β = −3.88, 95% CI = −6.17 to −1.60, t = −3.60, p = 0.003), CU traits × left insula × time (β = −1.25, 95% CI = −2.04 to −0.46, t = −3.38, p = 0.004), and CU traits × right rostral ACC × time (β = −1.01, 95% CI = −1.65 to −0.36, t = −3.30, p = 0.005). To visualize the three-way interactions, we divided the cortical thickness estimates of the significant regions and associated CU traits/emotion dysregulation into quartiles (i.e., first quartile, median, third quartile) to reflect low, medium and high baseline (pre-treatment) brain estimates and behavioural scores. We then estimated the pre- and post-treatment conduct score marginal means and compared those values between the brain and behavioural quartile groups (Figures 2–4). In Figure 2, participants in both the highest quartile of left insula thickness (greater thickness) and emotion dysregulation (greater impairment) pre-treatment showed the greatest decrease in conduct scores post-treatment. In Figure 3, participants in the highest quartile of left insula thickness pre-treatment showed decreases in conduct problems following treatment, regardless of whether baseline CU traits were low, medium, or high. This is in contrast with participants in the lowest quartile of left insula thickness at baseline which showed an increase in conduct problems following treatment, regardless of their baseline CU trait score. Similarly, in Figure 4, participants in the highest quartile of right rostral ACC thickness showed a decrease in conduct problems following treatment, regardless of baseline CU traits.
Estimated marginal means of conduct problems from pre- to post-treatment as a function of variation of left insula thickness and emotion dysregulation scores. This figure visualizes the three-way interaction between baseline emotion dysregulation × baseline left insular cortical thickness estimates × time (i.e., pre-/post-treatment). Both emotion dysregulation and cortical thickness were divided into quartiles such that “small/low” corresponds to the first quartile (25th percentile), “medium” corresponds to the median, and “large/high” corresponds to the third quartile (75th percentile). The y-axis shows the estimated marginal means of conduct problems as a function of treatment (pre- and post-treatment; x-axis).
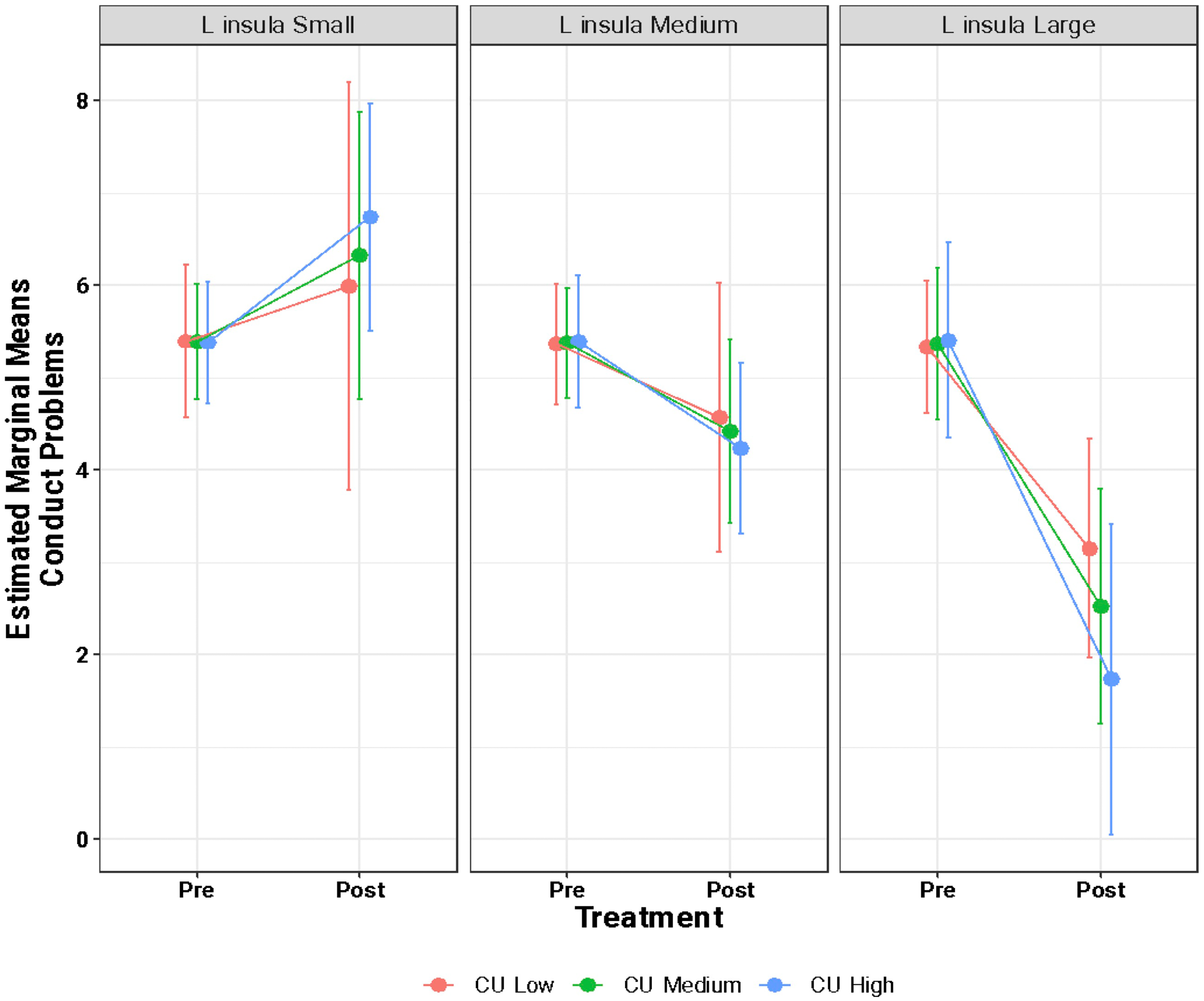
Estimated marginal means of conduct problems from pre- to post-treatment as a function of variation of left insula thickness and cu trait scores. This figure visualizes the three-way interaction between baseline CU trait scores × baseline left insular cortical thickness estimates × time (i.e., pre-/post-treatment). CU traits and cortical thickness were divided into quartiles such that “small/low” corresponds to the first quartile (25th percentile), “medium” corresponds to the median, and “large/high” corresponds to the third quartile (75th percentile). The y-axis shows the estimated marginal means of conduct problems as a function of treatment (pre- and post-treatment; x-axis).
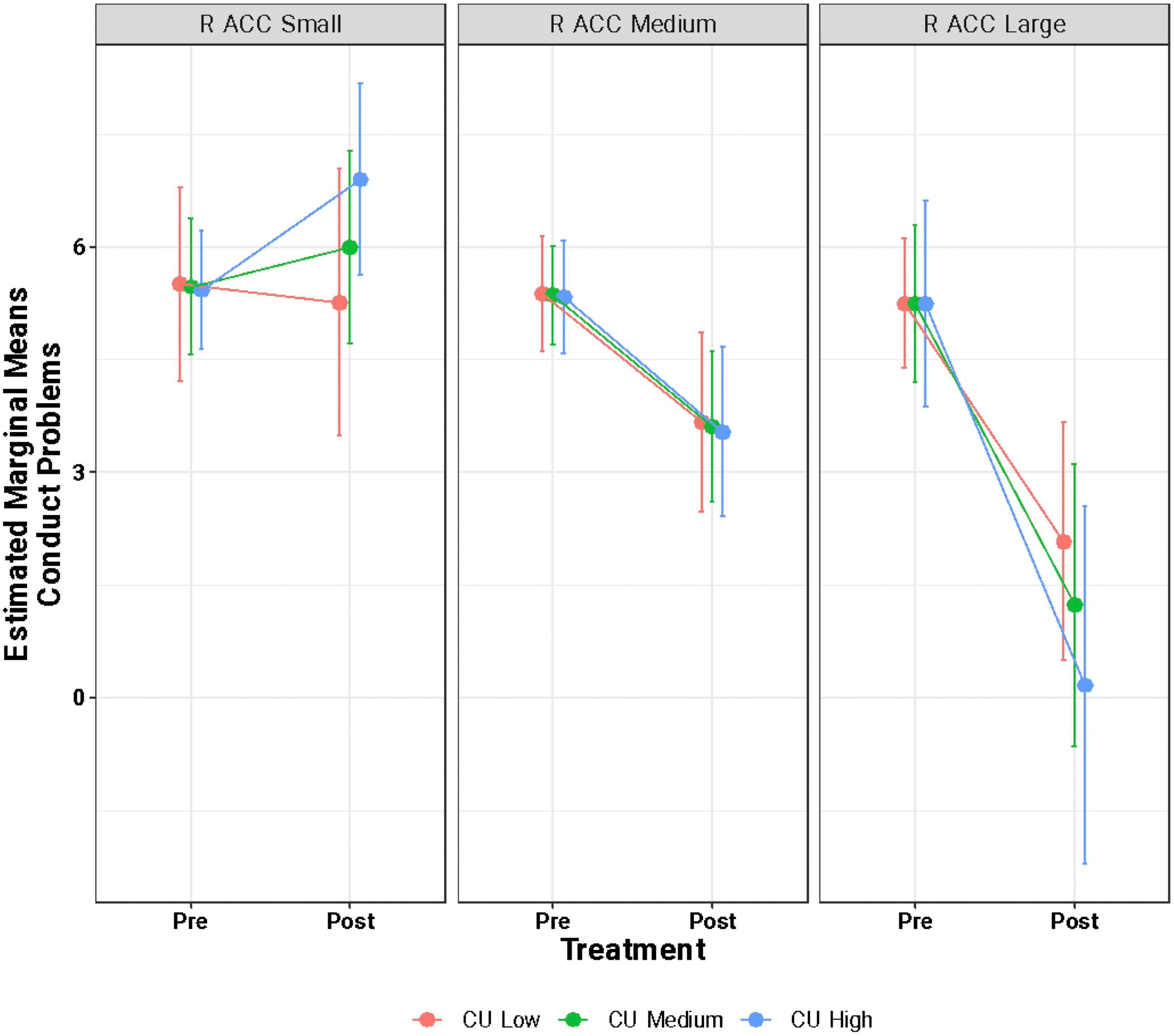
Estimated marginal means of conduct problems from pre- to post-treatment as a function of variation of right rostral ACC thickness and cu trait scores. This figure visualizes the three-way interaction between baseline CU trait scores × baseline right rostral ACC cortical thickness estimates × time (i.e., pre-/post-treatment). CU traits and cortical thickness were divided into quartiles such that “small/low” corresponds to the first quartile (25th percentile), “medium” corresponds to the median, and “large/high” corresponds to the third quartile (75th percentile). The y-axis shows the estimated marginal means of conduct problems as a function of treatment (pre- and post-treatment; x-axis).
Discussion
Understanding the neurobiology underlying emotion dysregulation and CU traits in children with externalizing disorders may lead to novel intervention strategies targeting externalizing psychopathology pathways. At baseline (pre-treatment), higher cortical thickness in the right and left insula, right and left rostral ACC, and right caudal ACC were moderately correlated with lower CU traits (less impairment; r = |0.4–0.61|). Higher cortical thickness in the left insula and left amygdala volume was also moderately correlated with lower pre-treatment emotion dysregulation (less impairment; r = |0.36–0.46|). The linear mixed modelling analyses found that overall, regardless of the severity of pre-treatment CU traits, increased thickness of the ACC and insula was associated with improvement in conduct problems following treatment.
While the results of the current study should be interpreted within the context and limitations of a preliminary pilot analysis, they are consistent with prior work. Lower insula and ACC volume have been associated with dimensions of emotion dysregulation, inclusive of CU traits, in children and adolescents with externalizing behaviours.18,20,22,58,59 Two previous studies have found that lower amygdala volume was associated with greater CU traits and emotion dysregulation in children with externalizing behaviours.21,60 Our previous work in a large population-based cohort of mostly typically developing children found that increased externalizing psychopathology symptoms (across different dimensions) was linked to structural alterations in frontolimbic and striatal regions. 8 The results from the current study, our prior work and others provide support that brain structure of the frontolimbic network is likely implicated in externalizing psychopathology, possibly encompassing both emotion dysregulation and CU traits.
The ACC and insula have been strongly implicated in emotional and behavioural regulation.27,29,61 Top-down modulations from the ACC and insula to limbic structures are thought to be implicated in regulatory processing of emotionally salient events.62,63 Altered maturation of the ACC and insula in childhood may be implicated in reduced abilities to identify one's internal emotional valence (e.g., anger or frustration) as well as a lower or altered threshold for emotional tolerance.61,64,65 This disruption in emotional tolerance may lead to impaired behavioural regulation, potentially supporting the observed pre-treatment (cross-sectional) brain–behaviour relationships. Psychosocial interventions, such as the Coping Power program used in the current study, targets conduct problems from a cognitive behavioural framework emphasizing the importance of children developing an awareness of both emotions and the physiological arousal that accompanies emotions. 33 The results of the linear mixed modelling analysis of the current study provide early evidence supporting a potential modulatory role of frontolimbic regions in externalizing psychopathology.
Limited studies have examined whether variation in both brain and behavioural metrics may be predictive of psychotherapeutic treatment outcomes. Prior work has typically examined whether baseline behavioural traits predict psychosocial treatment response.3,4,66,67 For example, higher baseline CU traits have been associated with poorer outcomes following treatment. 67 The results of the current study provide preliminary evidence to support future work assessing the viability of incorporating both brain and behavioural baseline metrics to improve predictive accuracy of treatment outcomes compared to using behavioural metrics alone. Given the limited efficacy of treatment to improve externalizing symptoms, 11 identification of neurobiological predictors of treatment response may inform hypotheses regarding mechanisms and opportunities for biologically informed treatment innovation. 68
Limitations
Some limitations of the present study should be considered when interpreting the results. First, the small sample size and the statistical estimation approach employed limit the conclusions and generalizability of findings. Replication in larger samples will be needed to make more definitive conclusions about these results. Moreover, five participants were missing post-treatment behavioural data and for this reason, we opted to run linear mixed effects models, rather than an analysis of covariance (ANCOVA) models, as they are considered more robust to missing data. 69 Second, participants were invited to opt-in to the imaging portion of the treatment study which may limit the generalizability of results due to potential bias linked to self-selection to participate in imaging. Notably, the full treatment intervention sample (n = 61) showed qualitatively lower conduct problem scores compared to the participants in the current study who opted into imaging (mean = 4.56 ± 1.85 full sample participating in coping power versus 5.3 ± 2.63 in the imaging sample; Supplementary Table S1). Third, this pilot sample is predominantly composed of participants assigned male sex at birth (n = 16/17), and therefore findings may not generalize adequately to females. Fourth, given the small sample size, we did not want to limit the power of the pilot analyses, thus, we did not include sensitivity analyses which covaried for medication status or sex. Similarly, we decided not to examine all the frontolimbic/striatal regions that have been previously linked to externalizing psychopathology to limit the number of models run given the small pilot sample. Lastly, due to the elevated probability of Type II errors (low power) and the exploratory nature of our analysis, we chose not to adjust for multiple comparisons.
Conclusion
The current study showed preliminary evidence that cortical thickness of the ACC and insula is negatively correlated with greater emotion dysregulation and CU traits in a small sample of children presenting to a tertiary care centre for clinically significant externalizing problems. Furthermore, we found evidence suggesting that the relationship between behavioural (emotion dysregulation and CU traits) and brain (ACC and insula thickness) metrics prior to treatment may be a predictor of psychotherapeutic treatment response. Future studies can expand on these results by exploring the interactions between cortical morphology and dimensions of psychopathology in larger samples as a first step towards developing targeted predictors of treatment response in children with externalizing psychopathological impairment.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437251315519 - Supplemental material for The Relationship Between Frontal Cortical Thickness and Externalizing Psychopathology is Associated with Treatment Outcomes in Children with Externalizing Problems: A Preliminary Pilot Study: La relation entre l’épaisseur du cortex frontal et les troubles extériorisés est associée aux résultats thérapeutiques chez les enfants ayant des problèmes extériorisés : une étude pilote préliminaire
Supplemental material, sj-docx-1-cpa-10.1177_07067437251315519 for The Relationship Between Frontal Cortical Thickness and Externalizing Psychopathology is Associated with Treatment Outcomes in Children with Externalizing Problems: A Preliminary Pilot Study: La relation entre l’épaisseur du cortex frontal et les troubles extériorisés est associée aux résultats thérapeutiques chez les enfants ayant des problèmes extériorisés : une étude pilote préliminaire by Lee Propp, Hajer Nakua, Anne-Claude V. Bedard, Marcos Sanches, Stephanie H. Ameis and Brendan F. Andrade in The Canadian Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: L.P. has received funding from a Canadian Institutes of Health Research (CIHR) Doctoral Award and Ontario Graduate Scholarship. H.N. has received funding from the Centre for Addiction and Mental Health (CAMH) Discovery Fund, the Ontario Graduate Scholarship, Fulbright Canada, and the CIHR Doctoral Award. S.H.A. currently receives funding from the National Institute of Mental Health, CIHR, the CAMH Foundation, and the Canada Research Chairs Program. B.F.A. currently receives funds from the CIHR, CAMH Discovery Fund, LesLois Shaw Foundation and Peter Gilgan Foundation. This study was funded by a grant from the American Psychological Foundation (principal investigator: B.F.A.). Other authors report no related funding support, financial or potential conflicts of interest.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.