
Abstract
Objective
Tobacco smoking is the leading cause of preventable death among individuals with serious mental illness (SMI) but few persons with SMI are offered smoking cessation treatment. The purpose of this study was to pilot-test a multicomponent intervention to increase the delivery of evidence-based smoking cessation treatment in community mental health clinics (CMHCs).
Method
This study was carried out at five CMHCs in Maryland involving clinicians who participated in training in smoking cessation. Other implementation activities included the provision of a treatment protocol, coaching, expert consultation, and organizational strategy meetings. The primary outcome was a change in clinicians’ knowledge and self-efficacy about smoking cessation. Secondary outcomes included documentation of evidence-based smoking cessation practices including assessment of smoking status and readiness to quit, and provision of smoking cessation treatment over the course of the 12-month intervention period.
Results
A total of 91 clinicians participated in the study. Data were available on 6,011 clients. Clinicians’ scores on the knowledge and self-efficacy measures increased modestly over the course of the implementation period. Overall, 57% of clients had their smoking status assessed; 81% of current smokers were evaluated about their willingness to quit; 82% of those willing to quit within 90 days received behavioral counseling, and 36% were prescribed or given smoking cessation pharmacotherapy. Clinicians rated the smoking cessation program highly in terms of acceptability, appropriateness, and feasibility.
Conclusions
Clinicians at CMHCs were engaged by and participated in training and implementation activities around smoking cessation practices which they then delivered to a substantial portion of clients in their care. The results of this study provide important data for the future planning of testing implementation strategies to scale up tobacco cessation treatment in this population in outpatient mental health settings.
Plain Language Summary Title
Implementing Smoking Cessation Treatment in Community Mental Health Clinics.
Plain Language Summary
Tobacco smoking is the leading cause of preventable death among people who have serious mental illness such as schizophrenia or bipolar disorder. However, few people with these disorders are offered smoking cessation treatment. The purpose of this study was to implement smoking cessation treatment at 5 community mental health clinics. We trained staff at the clinics about smoking cessation treatment and then provided coaching sessions for the staff and met regularly with the clinic leaders over the 12 months of the study. We evaluated if staff increased their knowledge about smoking cessation and their confidence to deliver smoking cessation treatment over the study period. We also obtained information about whether staff delivered smoking cessation treatment to their clients including an assessment of smoking and interest in quitting smoking, behavioral counseling for smoking cessation, and medication to help with quitting. A total of 91 clinicians participated in the study. Data were available on 6,011 clients. Clinicians’ scores on the knowledge and self-confidence questionnaires increased some over the course of the study. Overall, 57% of clients had their smoking assessed; 81% of current smokers were evaluated about their willingness to quit; 82% of those willing to quit received behavioral counseling, and 36% received smoking cessation medication. Clinicians rated the smoking cessation program positively. This study may inform the implementation of smoking cessation treatment in other outpatient mental health settings.
Introduction
Tobacco smoking is the leading cause of preventable mortality in persons with serious mental illness (SMI).1–3 Smoking has declined dramatically in the US population since publication of the first Surgeon General's Report. 4 However, the percentage of persons with SMI who smoke remains alarmingly high, more than three times that in the general population, even though the majority of persons with SMI who smoke would like to quit. 5 Evidence-based treatment for smoking cessation, pharmacotherapy combined with behavioral counseling, is effective and safe for people with SMI,6–9 yet severely underutilized.7,10,11–13
Many people with SMI receive most of their healthcare from the specialty behavioral health sector such as at community mental health clinics (CMHCs).14–16 While these settings are well suited for the delivery of smoking cessation treatment, tobacco smoking is often not addressed. Clinicians often believe that persons with SMI are incapable of, or do not want to stop smoking, and that smoking cessation medications are not safe for this population. Some mental health clinicians perceive smoking cessation treatment as outside their scope of practice.17–21 In addition, clinics may lack procedures for systematically assessing and documenting smoking status. Few published studies have evaluated implementation strategies to increase mental health clinicians’ delivery of evidence-based smoking cessation treatment to people with SMI. 22
This study describes the results of a pilot implementation trial designed to increase the delivery of four evidence-based smoking cessation practices to persons with SMI served in CMHCs. 23 The primary outcome was a change in clinicians’ knowledge of and self-efficacy around supporting evidence-based smoking cessation treatments. Secondary outcomes included their delivery of evidence-based smoking cessation practices over the 12-month intervention period, completion of the training and implementation activities, and perceptions of the acceptability, feasibility, and appropriateness of the implementation strategies and the evidence-based practices.
Method
Settings and Sample
The study was conducted at five CMHCs in Maryland, USA. Study participants were recruited by study staff in partnership with clinic leadership and included prescribers (psychiatrists, nurse practitioners, and primary care physicians) and other clinicians who provided counseling services (licensed counselors, social workers, and nurses). All clinicians in designated roles during the study period were eligible, including new hires after intervention implementation.
The study was approved by the Johns Hopkins University School of Medicine Institutional Review Board (#IRB00231836). The study was approved for a waiver of documentation of informed consent; all clinician participants provided verbal consent after the study was explained to them. Limited datasets of client electronic health record data were provided under a waiver of consent. Clinician training was delivered in waves, and data were collected between January 22, 2021, and July 31, 2023.
Evidence-Based Practices
The intervention included four evidence-based practices for smoking cessation that were based on consensus guidelines, recommendations for persons with SMI, and recent clinical trials.6,7,9,24–26
Assessment of smoking status involved asking adult clients if they currently smoke tobacco and, assessing the severity of tobacco dependence for those who reported use of any combustible tobacco.
27
Assessment of willingness to quit used stage-of-change questions.
28
Clinicians classified clients who endorsed readiness to set a quit date within 12 weeks as ready for active cessation treatment.
29
Although previous work has often used willingness to quit within 30 days as an indication for smoking cessation treatment, a broader definition was used so that more clients would be offered smoking cessation treatment.
30
Behavioral counseling was delivered by clinicians who were trained to use motivational interviewing techniques. For clients not interested in quitting within 12 weeks, behavioral counseling entailed a brief session (<10 min) to explore the pros and cons of smoking, elicit client concerns about their smoking, and identify potential benefits of quitting.
31
The clinician also discussed resources for the client if they decided to work towards quitting, including the benefits of using smoking cessation medications. Those clients who expressed a willingness to quit were referred for ongoing smoking cessation behavioral counseling30,32 and pharmacotherapy. The counseling sessions addressed standard topics (e.g., identifying personal reasons to quit, addressing smoking triggers, preparing for the quit date).
33
The fourth evidence-based practice was pharmacotherapy in which a physician or nurse practitioner met with clients undergoing smoking cessation behavioral counseling to encourage the use of one of three FDA-approved treatments: varenicline +/- nicotine replacement therapy (NRT), bupropion SR +/- NRT, or NRT alone.
27
When NRT was used, combination NRT (transdermal patch + lozenge or gum) was recommended.
34
Medication choice was made by the prescriber in collaboration with the client, taking into account factors such as differential effectiveness and potential side effects. At one site, nurses offered NRT directly to interested clients. Therapists and prescribers were encouraged to communicate with each other about smoking cessation plans. Medication could continue for one year or longer as relapse rates are high without ongoing pharmacotherapy, particularly for those with SMI.
35
Those not willing to quit within 12 weeks were offered, and if interested referred for, a one-month trial of varenicline to increase readiness to quit.36,37
Implementation Strategies
To improve mental health clinicians’ knowledge, self-efficacy, and delivery of evidence-based practices, the study employed five implementation strategies:
1. Training 2. Tobacco smoking treatment protocol
Training was conducted by study staff. Clinician participants completed a one-hour online training module. They then used a videoconferencing platform to participate in real-time training on delivering smoking cessation behavioral counseling, prescribing smoking cessation pharmacotherapy, and using motivational interviewing skills for clients about smoking, supplemented with an online avatar practice module.
23
The research team developed a tobacco smoking treatment protocol to assist clinicians. Clients who reported being current smokers (i.e., smoked a tobacco product in the past 7 days) were assessed for willingness to quit. Based on client responses to this assessment, instructions were provided to help clinicians facilitate brief smoking cessation conversations. Clinicians were provided manuals for delivering the behavioral counseling sessions and prescribing pharmacotherapy.
The behavioral counseling manual included the outline for 13 session topics that could be delivered flexibly based on the client's current smoking status and the clinician's judgment. A smoking cessation session could be “stand alone” or part of a regularly scheduled therapy session and designed to be 10–15 min in duration. Each session was expected to include an assessment of the client's past week average cigarettes smoked per day, review of quit attempts since the previous visit, new session content, and collaborative identification of a smoking-related behavioral goal to focus on until the next therapy session.
3. Coaching 4. Expert consultation 5. Organizational Strategy Meetings
Coaching sessions were offered to clinicians monthly through a videoconferencing platform and were focused on skill development, overcoming barriers to providing smoking cessation treatment, discussion of specific client cases, and additional training as requested. To increase participation, coaching sessions were incorporated into regularly scheduled clinic meetings and clinicians were expected to attend at least quarterly.
Study team members who were experts in smoking cessation pharmacotherapy and behavioral counseling were available to prescribers and counselors during the intervention to conduct as-needed consultation.
Organizational strategy meetings were designed to improve engagement in practice change through identification of successful organizational-level processes, sharing implementation data, providing feedback, and problem-solving to overcome identified barriers to program delivery. These meetings were scheduled monthly at each site with study staff and a clinic leadership team.
Measures
The primary outcomes were changes in clinicians’ knowledge about and self-efficacy to deliver evidence-based smoking cessation treatment from baseline before training to 12 months, at the end of the implementation period. The knowledge measure was a 16-item scale developed by the investigators. The self-efficacy measure was based on one developed by Compeau and Higgins. 38
Secondary outcomes included the delivery of the four recommended evidence-based practices: (1) assessment of smoking status for all adult clinic clients; (2) assessment of willingness to quit for smokers; (3) receipt of behavioral counseling for smokers; and (4) receipt of pharmacotherapy for smokers as documented in the electronic medical record or study-specific forms. Secondary measures were changes in the acceptability, appropriateness, and feasibility of the intervention implementation strategies and of the evidence-based practices as assessed through the survey instrument immediately after training and again at the end of the 12-month implementation period.
In order to assess fidelity on the part of the clinicians providing behavioral counseling to the components of the evidence-based smoking cessation counseling, clinicians participated in interactions with standardized client actors, each of which was approximately 25 min, at the 12-month time point. Sessions were audio-recorded and rated on a 10-item, 3-point fidelity rating scale developed by the investigators.
Data Collection
Data were obtained from clinician surveys, online or paper-and-pencil, at baseline, either before or after the training depending on the measure, and at the 12-month endpoint. Data were also obtained about clinician participation in training. Participating clinicians were paid $20 for each set of surveys completed and $25 for participating in each standardized actor interview. The research team also received limited datasets of client electronic health record data or via study-specific forms about client receipt of each of the evidence-based practices during the 12-month implementation period. The study sites did not systematically document these client-based outcomes.
Data Analysis
Descriptive statistics were used to present the clinicians’ scores on the knowledge and self-efficacy measures, their perceptions of the implementation intervention strategies, delivery of the evidence-based practices, and clinician fidelity to smoking cessation counseling. A repeated-measure mixed-effects regression modeling approach was used for modeling each of the primary outcomes, the clinicians’ knowledge and self-efficacy outcomes, to study the change at 12 months from baseline (assessed before intervention training). All mean models included a binary variable representing the 12-month time point (with baseline as the reference), fixed effects for the five study sites, a binary variable for staff role (counseling provider vs. prescriber), a variable indicating years in profession, and corresponding study site by staff role interaction terms, except for the mean models used to evaluate self-efficacy to deliver smoking cessation pharmacotherapy and counseling, where the staff role variable and its interaction with study site were omitted as each of the staff roles only provided the corresponding role-specific evidence-based practices. An unstructured variance-covariance model was used for the repeatedly measured outcomes to allow different outcome variance at baseline and 12 months and address the within-subject correlation over time. Given the small number of sites, outcomes clustering within sites were addressed through the site-level fixed effects. No random effect was invoked. All available data for enrolled clinicians was included in the regression modeling, including data for participants who had missing data at either baseline or 12 months, with the other missing data indicated by the software designated missing indicator and analyzed under the assumption of missing at random. Estimates of mean change in outcome at 12 months from baseline and associated 95% confidence intervals were derived from the mixed-effects regression modeling results. All analyses were conducted using R version 4.1.1 (Vienna, Austria) with modeling using the mmrm package version 0.2.2. 39
Results
Settings and Sample
The study was conducted at five clinic sites, two of which were affiliated with an academic medical center. Geographically, two were in urban areas, two were in suburban areas, and one was in a rural location.
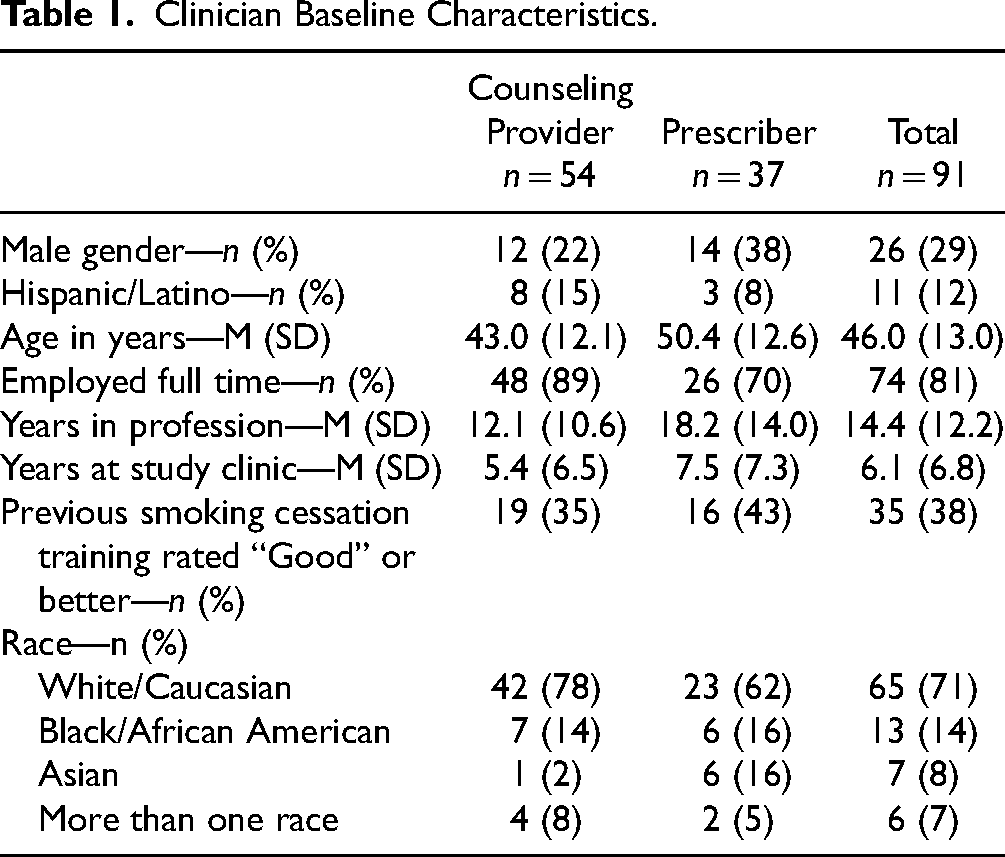
Across the five sites, a total of 81 out of 116 (70%) eligible clinicians enrolled at the start of the study, and an additional 10 of 28 (36%) joined over the course of the study period after they became eligible, yielding an overall enrollment yield of 63%. As shown in Table 1, clinician participants were predominantly white women with an average of more than 14 years of professional experience. The majority of clinician participants (59%) were nonprescribers who provided counseling and did not consider that the smoking cessation training they received prior to enrolling in this study was good.
Clinician Baseline Characteristics.
Completion of Training and Implementation Activities
As shown in Table 2, the majority of the clinician participants completed most training activities. The activity with the highest rate of participation was the real-time synchronous training. The rate of participation in the real-time motivational interview training was also high. Completion of the online avatar training was lower, especially among prescribers.
Clinician Training & Implementation Participation.
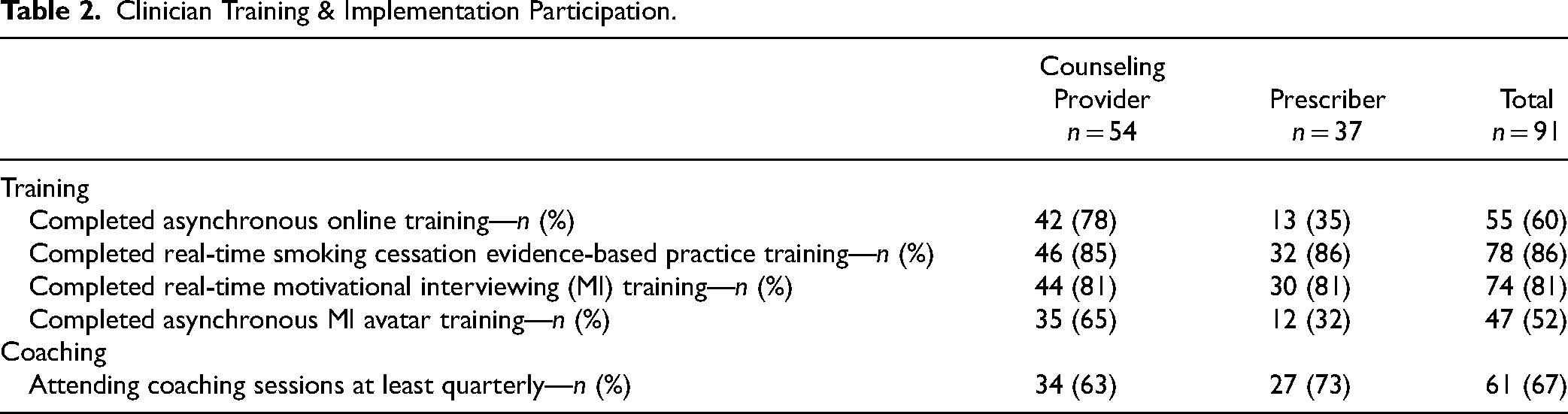
The majority of clinicians attended at least the minimum recommended number of coaching sessions (quarterly) led monthly by study staff. Expert consultation was provided to several clinicians. Organizational strategy meetings were routinely convened at each site monthly.
Clinicians’ Knowledge and Self-Efficacy About Smoking Cessation
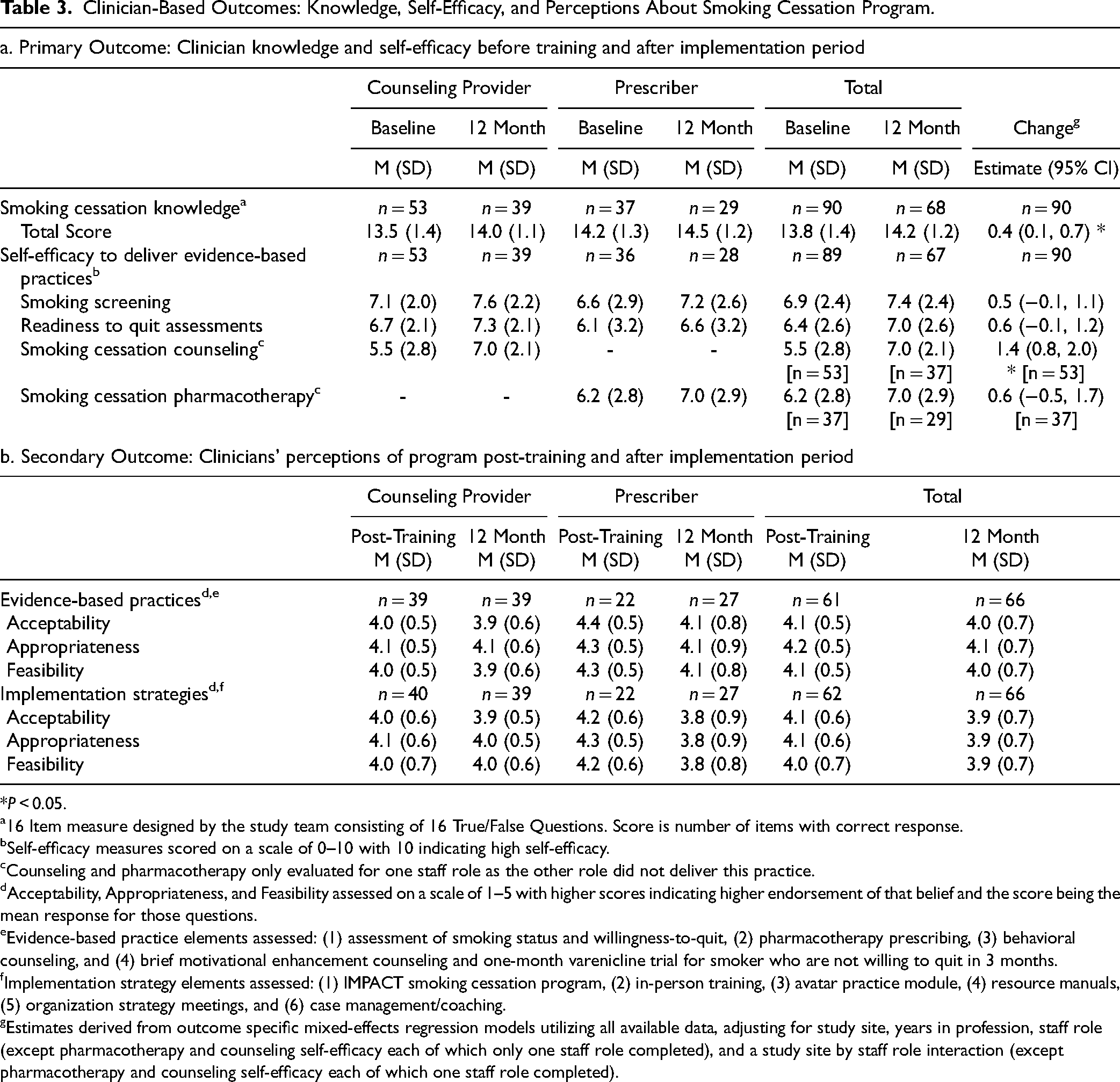
Participating clinicians were surveyed as to their knowledge about smoking cessation and their self-efficacy to deliver smoking cessation treatment before training and at the end of the implementation period. As shown in Table 3, clinicians had high levels of knowledge before training and their scores improved over the course of the implementation period with a significant increase in the total score. Clinicians also reported moderately high levels of self-efficacy to deliver evidence-based practices before training, the level of which increased for all groups over the course of the implementation period. Significant increases were found in the reported efficacy to deliver smoking cessation counseling.
Clinician-Based Outcomes: Knowledge, Self-Efficacy, and Perceptions About Smoking Cessation Program.
*P < 0.05.
a16 Item measure designed by the study team consisting of 16 True/False Questions. Score is number of items with correct response.
bSelf-efficacy measures scored on a scale of 0–10 with 10 indicating high self-efficacy.
cCounseling and pharmacotherapy only evaluated for one staff role as the other role did not deliver this practice.
dAcceptability, Appropriateness, and Feasibility assessed on a scale of 1–5 with higher scores indicating higher endorsement of that belief and the score being the mean response for those questions.
eEvidence-based practice elements assessed: (1) assessment of smoking status and willingness-to-quit, (2) pharmacotherapy prescribing, (3) behavioral counseling, and (4) brief motivational enhancement counseling and one-month varenicline trial for smoker who are not willing to quit in 3 months.
fImplementation strategy elements assessed: (1) IMPACT smoking cessation program, (2) in-person training, (3) avatar practice module, (4) resource manuals, (5) organization strategy meetings, and (6) case management/coaching.
gEstimates derived from outcome specific mixed-effects regression models utilizing all available data, adjusting for study site, years in profession, staff role (except pharmacotherapy and counseling self-efficacy each of which only one staff role completed), and a study site by staff role interaction (except pharmacotherapy and counseling self-efficacy each of which one staff role completed).
Perceptions About Training and Implementation Strategies
Ratings of acceptability, appropriateness, and feasibility were high (mean > 4 on 5-point scale) for the evidence-based practices and implementation strategies after training and slightly lower at the end of the implementation period.
Delivery of Evidence-Based Practices
Data were collected on the delivery of the evidence-based practices to all adult clients at each site except for site D where only data from clients of the participating clinicians were collected. Overall, data were collected on services provided to N = 6,011 clients.
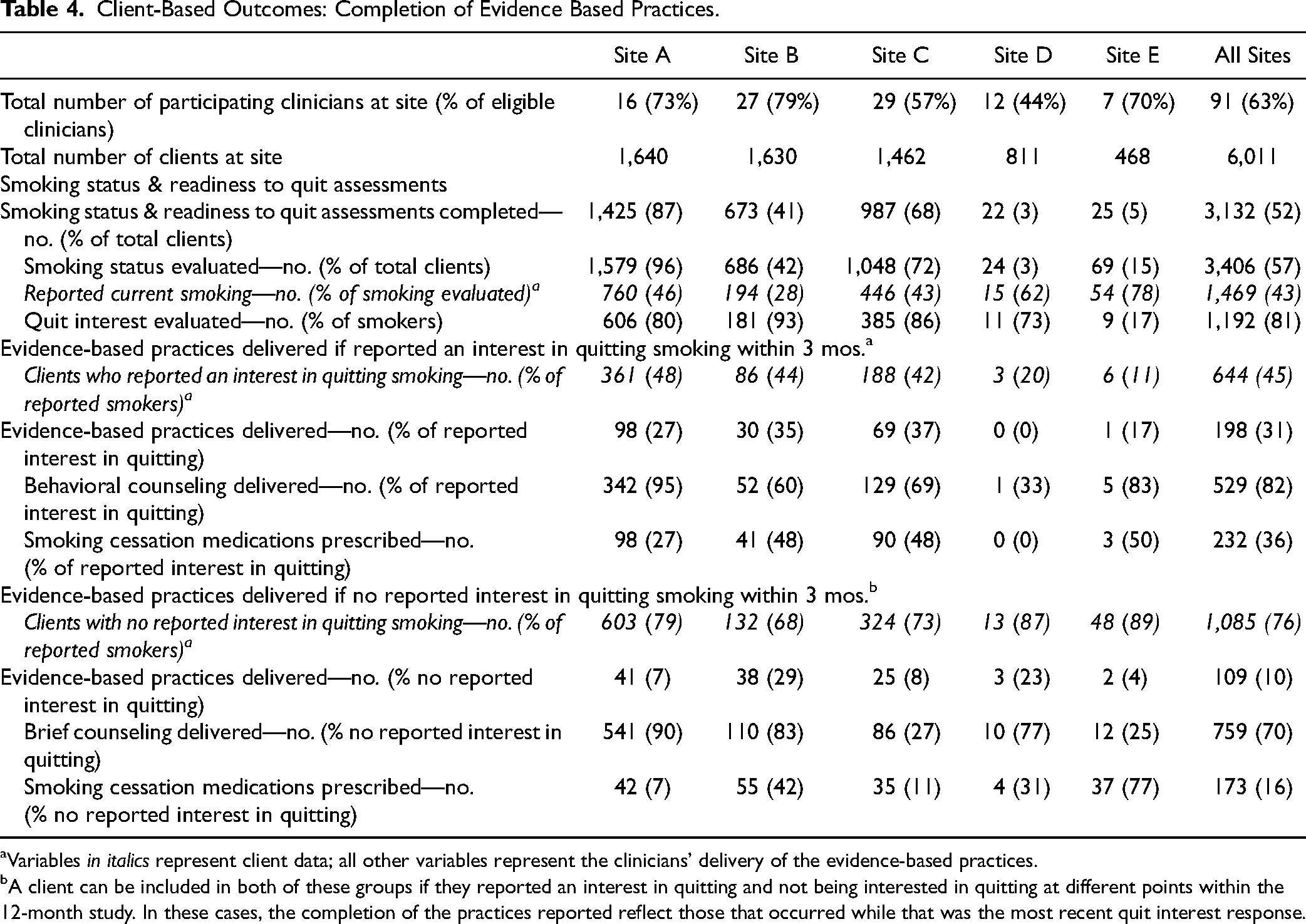
Of the 3,132 (52%) clients who were assessed as to their smoking status, 1,469 (43%) reported current smoking (Table 4). Of these smokers who also had their interest in quitting evaluated, a high percentage of clients (76%) expressed that they were not interested in quitting smoking at some point during the implementation phase. However, during the course of the implementation period close to half (n = 644, 45%) also expressed an interest in quitting within 12 weeks. Of these, the majority (82%) received some behavioral counseling, and more than a third (36%) were prescribed or given a smoking cessation medication during the course of the implementation phase. The delivery of evidence-based practices was less common to smokers who reported no interest in quitting within 12 weeks.
Client-Based Outcomes: Completion of Evidence Based Practices.
aVariables in italics represent client data; all other variables represent the clinicians’ delivery of the evidence-based practices.
bA client can be included in both of these groups if they reported an interest in quitting and not being interested in quitting at different points within the 12-month study. In these cases, the completion of the practices reported reflect those that occurred while that was the most recent quit interest response.
While the percentage of clients reporting that they were smokers was similar across three sites with the largest number of participants (28%–46%), there was considerable variability in the delivery of evidence-based practices. For example, as shown in Table 4, a majority of clients were assessed as to their smoking status but this ranged from 96% of clients at one site to 3% at another site. In general, the sites with the largest number of clients and participating clinicians had the highest percentage of clients to whom the evidence practices were delivered.
Fidelity Ratings
The average smoking cessation counseling fidelity score was 12.3 out of a possible score of 20. As seen in Table 5, a majority of clinicians were rated as demonstrating each behavior at least some of the time. Clinicians scored highest (best) on items related to assessing current smoking status and pharmacotherapy use and showing positive regard for the client. The average scores were lower for items related to actively exchanging information about smoking and smoking cessation treatment and assessing and recommending behavioral strategies to support smoking cessation
Fidelity of Behavioral Counseling on Part of Counseling Providers at 12 Months (n = 30)a.
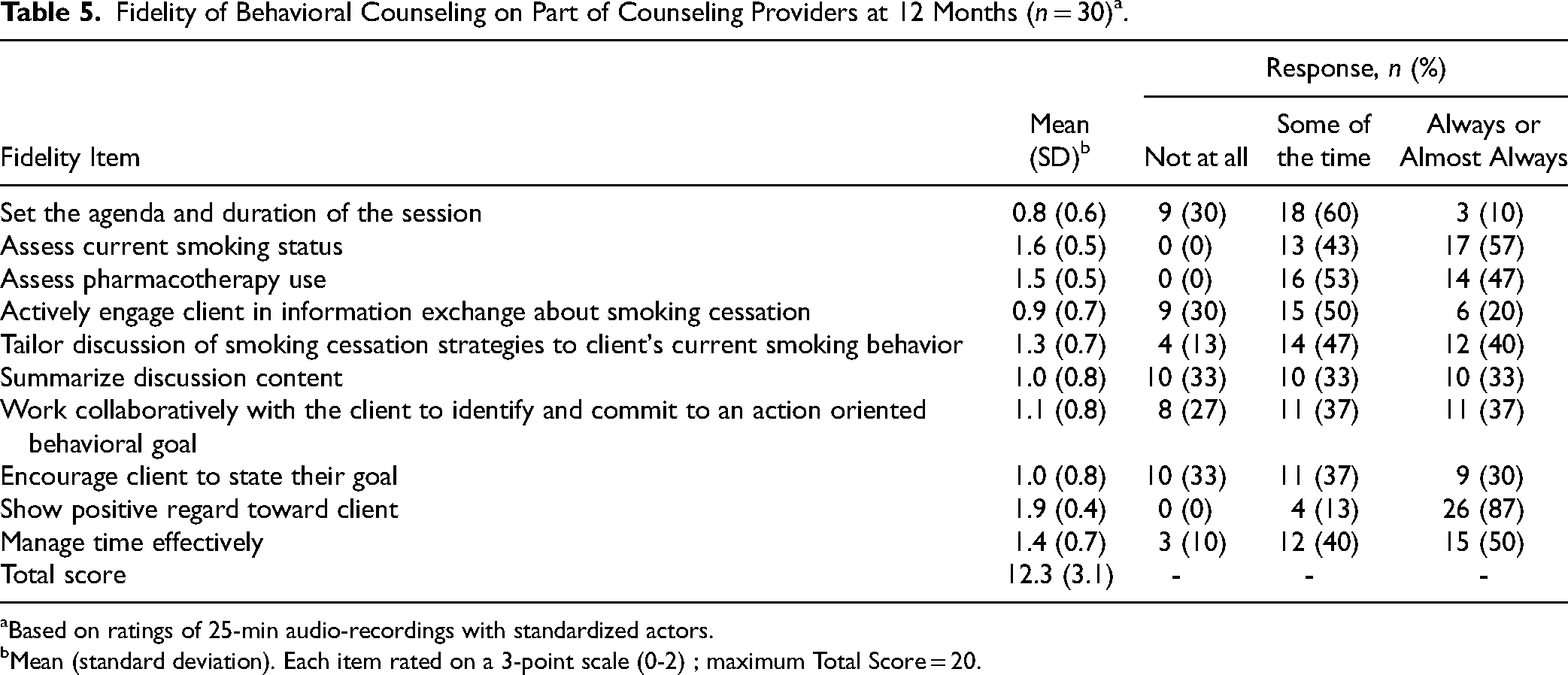
aBased on ratings of 25-min audio-recordings with standardized actors.
bMean (standard deviation). Each item rated on a 3-point scale (0-2) ; maximum Total Score = 20.
Discussion
In this pilot implementation study, we found a relatively high rate of participation on the part of CMHC clinicians in training and implementation activities focused on the delivery of smoking cessation practices. The level of clinicians’ knowledge about smoking cessation and their self-efficacy to deliver evidence-based practices increased modestly over the one-year implementation period. Clinicians rated the smoking cessation program highly in terms of acceptability, appropriateness, and feasibility both before and after the implementation period. Notably, at baseline only a minority of clinicians reported receiving previous training in smoking cessation practices which they would rate as “good” or better, suggesting that the training offered new learning opportunities.
In terms of the delivery of evidence-based practices, more than half of clients (52%) across the sites were assessed as to their tobacco smoking status and willingness to quit at least once during the 12-month implementation period. Impressively, 82% of smokers who expressed a willingness to quit received at least brief behavioral counseling though we do not know the content or duration of the counseling sessions. More than one-third (36%) of clients who expressed a willingness to quit were prescribed or given a smoking cessation medication. While ideally all smokers would receive counseling and medications for smoking cessation, tobacco smoking is typically not addressed in community mental health settings and so the increase in the reach of these evidence-based practices is meaningful.
There was variability in the delivery of evidence-based practices among the clinic sites likely due to resource issues, leadership priorities, staff turnover, and other circumstances beyond the purview of the study. We observed that sites with larger numbers of participating clinicians were more likely to have uptake of the evidence-based practices. There may have been more consistent expectations and support for delivering smoking cessation services at these sites.
The study had numerous challenges which underscore the success that was achieved. All of the implementation activities took place during the COVID pandemic when resources were strained, and clinics shifted rapidly to remote delivery for clinical services, as did the study procedures. Also, clinics did not have any billing structure for specific smoking cessation services posing a challenge to account for clinician time spent providing these services as clinicians were asked to add smoking and smoking cessation to the topics that they already addressed with clients including urgent mental health issues.
This pilot implementation study is one of few studies to examine a clinic-based approach to the implementation of smoking cessation treatment for persons with SMI in CMHCs. Previous studies have shown an increase in the delivery of smoking cessation after an implementation intervention but the focus has been on smoking cessation medication alone 40 or smoking along with other health behaviors. 41
The percentage of mental health clients across the sites who reported themselves to be tobacco smokers, 43%, is generally consistent with current reports in the United States of tobacco smoking among those with SMI,42,43 but a staggering prevalence in contrast to the US general population where smoking among adults declined to 11.5% in 2021, during the period when our study was conducted. 44 It is also noteworthy that close to half of smokers in the study who had their interest in quitting assessed did express an interest in quitting which counters previous myths that persons with mental illness are unwilling to quit and are immune from public health messaging about the hazards of smoking. 11 It is also of note that many of these same persons also reported they were not interested in quitting when assessed at other points during the one-year implementation period, reflecting the ambivalence about quitting, the need for routinely assessing willingness to quit, and the shifting motivation about smoking cessation found in other populations of smokers. 45
Clinicians self-reported relatively high ratings of knowledge about smoking cessation and self-efficacy to deliver smoking cessation practices both before and at the end of the implementation period. However, fidelity ratings of mock sessions conducted with actors suggested the possibility that counselors overestimated their skill level. Alternatively, the standardized actor interactions may not have accurately reflected encounters with actual clients which we did not evaluate due to privacy and feasibility concerns.
Our study had several strengths. We used multiple implementation strategies including online training, training in real time, a novel avatar skills practice module, monthly meetings with clinicians, expert consultation, and organizational strategy meetings. Also, we were able to study a relatively large number of clients for whom data about delivery of smoking cessation practices were available. In addition, the 12-month intervention period allowed adequate time for implementation. There was relatively high engagement on the part of clinicians despite challenges in the context of the pandemic and competing clinical issues.
Limitations of the study include that the intervention was effortful which may limit its easy transportability to mental health clinics at large. Sites were able to collect data about the evidence-based practices since implementation, but electronic medical records were not standardized across sites nor optimally configured to provide these data. Also, while we used multiple implementation strategies, we cannot be certain which ones were most effective. In addition, the duration and quality of behavioral counseling that was delivered was not assessed. We also did not collect data about clients’ quit attempts or their success with smoking cessation. Finally, because data were not available about practices at the clinics before implementation and this was not a randomized controlled trial, we cannot make causal inferences about the effectiveness of the program.
Conclusions
This study demonstrated that clinicians at CMHCs were engaged by and participated in training and implementation activities around smoking cessation practices which they then delivered to a substantial portion of their clients. While not without challenges, the training and implementation activities and evidence-based practices were reported to be feasible and acceptable. As a group, clinicians’ knowledge and self-reported self-efficacy about smoking cessation treatment increased over the implementation period. The results of this study provide important data for the future planning of testing implementation strategies to scale up tobacco cessation treatment in outpatient mental health settings.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437241309678 - Supplemental material for Promoting Evidence-Based Tobacco Cessation Treatment in Community Mental Health Clinics: Results of a Pilot Implementation Study: Promouvoir le traitement de sevrage tabagique fondé sur des données probantes dans les cliniques communautaires de santé mentale : résultats d’une étude pilote de mise en œuvre
Supplemental material, sj-docx-1-cpa-10.1177_07067437241309678 for Promoting Evidence-Based Tobacco Cessation Treatment in Community Mental Health Clinics: Results of a Pilot Implementation Study: Promouvoir le traitement de sevrage tabagique fondé sur des données probantes dans les cliniques communautaires de santé mentale : résultats d’une étude pilote de mise en œuvre by Faith Dickerson, Tyler Fink, Stacy Goldsholl, Arlene Dalcin, Benjamin Eidman, Christina T. Yuan, Joseph V. Gennusa, Corinne Cather, A. Eden Evins, Nae-Yuh Wang, Emma M. McGinty and Gail L. Daumit in The Canadian Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Center to Accelerate Translation of Interventions to Decreased Premature Mortality in SMI; P50MH115842; Daumit PI; National Institute of Mental Health, (grant number P50MH115842).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.