
Abstract
Objective:
To qualitatively and quantitatively synthesize the literature on the efficacy and safety of magnetic seizure therapy (MST) in psychiatric disorders.
Methods:
A literature search was conducted of the OVID Medline, OVID EMBASE, PsychINFO, CINAHL, Web of Science and Cochrane databases from inception to 14 January 2024, using subject headings and key words for “magnetic seizure therapy.” Randomized controlled trials (RCTs), post-hoc analyses of RCTs, open-label trials, or case series investigating MST in adults with a verified psychiatric diagnosis and reporting on two possible primary outcomes (1) psychiatric symptom reduction (as measured by validated rating scale) or (2) neurocognitive outcomes (as measured by standardized testing), were included. Abstracts, individual case reports, reviews and editorials were excluded. Extracted data included: (1) basic study details; (2) study design; (3) sample size; (4) baseline demographics; (5) outcome data (including secondary outcomes of suicidal ideation and adverse events); and (6) stimulation parameters. Cochrane's risk of bias tool was applied. A quantitative analysis was conducted for the depression studies, using Hedge's g effect sizes.
Results:
A total of 24 studies (n = 377) were eligible for inclusion. Seventeen studies in depression (including three RCTs), four studies in schizophrenia (including one RCT), one study in bipolar disorder, one study in obsessive-compulsive disorder and one study in borderline personality disorder were summarized. We found no significant difference in depressive symptom reduction between MST and electroconvulsive therapy (ECT) in randomized, controlled trials (g = 0.207 towards ECT, 95% confidence interval (CI) −0.132 to 0.545, P = 0.232). We found a significant reduction in depressive symptoms overall with MST in the pooled RCT and open-label analysis (g = 1.749, CI 1.219 to 2.279, P < 0.005). It is suggested that MST has modest cognitive side effects.
Conclusions:
Large-scale RCTs are necessary to confirm early signals of MST as an effective intervention in psychiatric disorders with a cognitive profile that is potentially more favourable than ECT.
Introduction
First-line and second-line treatments do not produce meaningful improvement in an important subset of patients. Even with multiple medication trials and non-invasive neurostimulation approaches, there are significant proportions of patients that do not respond. For example, up to 30% of patients with depression do not respond to pharmacotherapy or psychotherapy 1 and response rates for interventions like repetitive transcranial magnetic stimulation (rTMS) range from 40% to 50%. 2 In patients with bipolar depression, up to 48% 3 do not respond to first-line interventions, and many patients with schizophrenia struggle with persistent symptoms despite adequate antipsychotic treatment. 4
The spectrum of brain stimulation treatments has expanded in recent years with proliferation of non-invasive neurostimulation approaches that include rTMS, transcranial direct current stimulation, transcranial alternating current stimulation, and others. 5 As an example, rTMS could be useful after one or more failed antidepressant trials and offers specific benefits: an office-based treatment without anesthesia, limited side effects and potentially rapid response. 6 Yet, we see that there are those with definite non-response to rTMS or modest improvement failing to meet remission—particularly patients with more severe baseline depressive symptoms or comorbidities. 7 Directing non-responders towards electroconvulsive therapy (ECT) is an effective next step in depression treatment, yielding a 60–80% response rate.8–10 Despite its clear benefits, there are some drawbacks to the use of this invasive treatment. Contemporary studies of patients with treatment-resistant depression (TRD) are showing somewhat lower response rates to ECT compared to earlier studies.11,12 ECT continues to have lower patient acceptance due to negative perceptions and concern over adverse cognitive effects. 13 The cognitive side effects can be impairing and are well-described: prolonged post-treatment disorientation, anterograde amnesia and possible retrograde amnesia.14–16
Thus, there is the need for new interventional treatments, which maintain efficacy with a more favourable side effect profile. First described in 2000, magnetic seizure therapy (MST) is emerging as a promising candidate treatment. MST uses repetitive transcranial magnetic stimulation instead of direct electrical current to induce a generalized seizure. 17 The promise of lower side effects is attributed to a more controlled and focal seizure onset and spread. 18
In the 2016 CANMAT guidelines, MST was listed as an investigational treatment, with level three evidence for acute efficacy and tolerability. This was based primarily on the results of smaller randomized controlled trials (RCTs) or non-randomized, controlled prospective trials or case series. 19 Since that time, there has been several studies exploring different aspects of this treatment in patients with depression and also other disorders.
Despite growing interest, there have been only four systematic reviews published on MST.20–23 Those published tend to be narrow in focus, for example, concentrating solely on unipolar depression or schizophrenia. They also tend to have restrictive inclusion criteria, excluding smaller research reports other than RCTs. As such, the aims of this study were to: (1) conduct a systematic review of the efficacy (reduction in psychiatric symptoms and suicidality) and safety of MST (neurocognitive and adverse effects) in all psychiatric disorders (2) conduct a quantitative analysis of these outcomes where sufficient data exists and a qualitative analysis where the data are insufficient.
Methods
A systematic search was conducted of the OVID Medline, OVID EMBASE, PsychINFO, CINAHL, Web of Science, and Cochrane Database of Systematic Reviews, from inception to 14 January 2024. This study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting checklist 24 (included in Supplemental Materials). It was further registered in PROSPERO (PROSPERO identifier: CRD42024502157).
Search Strategy
The search strategy was first designed, tested and revised in OVID MEDLINE in collaboration with a health sciences librarian. It was then translated and run in the remaining databases.
The search strategies utilized database-specific subject headings and keywords to capture the central concept of MST. The search terms (magnetic seizure therapy) OR (seizure therap*) OR (magnetic convulsive therap*) OR (magnetic neurostimulat*) OR (magnetic brain stimulation*) OR (magnetic seizure induc*) OR (magnetic neuromodulation) OR (magnetic seizure treatment) OR (Transcranial Magnetic Stimulation/ and seizure) were entered. Specific psychiatric disorders were not added as conjunctive search terms, as MST is an emerging field and limited in use at this time. No study type or language limits were applied. Unpublished studies were not sought as part of this systematic review. Please see Supplemental Materials for full details of the search strategies.
Inclusion Criteria
Selected studies were required to meet the following inclusion criteria:
RCTs, open-label trials, retrospective analyses of larger RCTs, or case series. In adults (age >18 years old) with a valid diagnosis of a psychiatric disorder according to a recognized diagnostic manual (i.e., The Diagnostic and Statistical Manual of Mental Disorders, Fourth or Fifth edition, or the International Classification of Diseases- Eleventh edition) or according to a clinician. Reporting the effects of MST on two possible main outcomes, either symptom improvement (as measured by a validated rating scale) AND/OR cognitive impairment (as measured by change in standardized cognitive measures). If an RCT format, with the main comparators being placebo or sham MST, ECT, other interventional treatments (eg. rTMS), or first-line pharmacotherapy. The full text was available in English.
Our systematic review was meant to provide a more comprehensive overview of the literature. Studies were not limited by the inclusion of comorbid disorders. Only abstracts, individual case reports, reviews and editorials (including letters to the editor) were excluded. Non-traditional treatment schedules (e.g., accelerated) and continuation MST formats were excluded from analyses.
Outcomes
The primary outcomes of interest for this systematic review were symptomatic improvement on a validated symptom rating scale and cognitive adverse effects as measured by a validated cognitive rating scale. Additional outcomes included reduction in suicidal ideation (as measured by validated suicide rating scale) and other adverse effects.
Screening and Data Extraction
All titles and abstracts identified by the literature search were independently reviewed for study inclusion by two authors, JP and LZ. Any disagreements were resolved through discussions with a senior author, DMB. If the study details were unclear from the abstract, the full text was retrieved for more in-depth assessment. The same process detailed above was applied for the next round of full text review.
The data was extracted and managed using the Covidence software program. Data was independently extracted by two authors, JP and LZ. The extracted data highlighted: (1) basic study details (e.g., authors, year published, country published); (2) study design; (3) sample size; (4) baseline demographics (age, sex, treatment setting); (5) outcome data (symptom scale reduction, neurocognitive measures, adverse events); and (6) treatment number and stimulation parameters. For missing data, authors were contacted once by email; if no response, only available data was analyzed. Cross-referencing clinical trial investigation numbers identified studies derived from a single sample; in these cases, the study with the largest available dataset was used.
Meta-Analysis
The meta-analysis compared the differences in primary outcomes between MST and ECT in RCTs. The focus on RCTs was chosen for the most rigorous comparison between the two treatments. A sensitivity analysis of study design was then conducted to include non-RCT (e.g., open-label) studies comparing MST to ECT. Finally, all studies—regardless of study design and with or without ECT comparator—were pooled for analysis of primary outcomes of MST alone. There were no planned subgroup analyses. For those studies not eligible for meta-analysis, we completed a narrative synthesis of study findings.
R version 4.3.2 25 was used for basic data proceeding, and the meta-analyses were performed using the Comprehensive Meta-Analysis version 4 software. 26
Hedge's g
Given that most studies have small sample sizes, we used Hedge's g to estimate the effect size for continuous data. The effect size was calculated based on the mean difference between the baseline and endpoint scores in the primary scale, standardized by the pooled standard deviation (within group if no comparator in study or between-groups if comparator). This standardization allows comparison across different study scales and also computes study weights to include in the analysis. 27 Within the standard error, an estimate of the pre-post correlation coefficient was based on calculation from data of two of the included studies.28,29 The correlation coefficient used in this study was the average of the two estimates. A random effects model was used considering study heterogeneity would be considerable. This model assumes that true effect size could vary between studies, as they represent random samples within a larger population.
Test of Heterogeneity
Heterogeneity between studies was assessed using the I2 statistic and was interpreted as suggested by the Cochrane Handbook: 0–30% uncertain, 30–50% moderate and >50% substantial heterogeneity. 27 A funnel plot was generated to examine publication bias for each analysis (please see Supplemental Materials).
Risk of Bias Assessment
The quality of studies included was assessed by two independent authors (JP, LZ) using the Cochrane Risk of Bias tools. More specifically, for RCTs, six domains were assessed: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, selective outcome reporting and missing data. An overall score divided studies into low, moderate (some concerns) or high risk. 30 For non-controlled studies, potential for confounding, selection of participants, classification of interventions, deviation from intended intervention, measure of outcomes, missing data and selective reporting were the domains assessed. The resulting score placed studies in low, moderate, serious or critical risk of bias. 31
Results
Our search yielded 3444 studies to be screened, supplemented by one additional article 32 from a journal not-yet-indexed. Full texts of 61 studies were reviewed (see PRISMA flow diagram—Figure 1). A total of 24 studies (n = 377 MST patients) were included in the qualitative analysis. This was divided into 17 studies in depression (n = 273), four in schizophrenia (n = 59), one in bipolar depression (BD) (n = 26), one in obsessive-compulsive disorder (OCD) (n = 10), and one in borderline personality disorder (BPD) (n = 9). Within depression, there were three RCTs comparing MST with ECT,28,33,34 one post-hoc analysis of an RCT, 35 four non-randomized, open-label comparison with ECT studies,36–39 eight open-label single arm studies,29,40–46 and one case series. 47 In schizophrenia, there was one randomized, double-blind comparison with ECT, 48 as well as one post-hoc secondary analysis of the RCT, 49 one open-label study 50 and one case series. 51 Bipolar disorder had one open-label trial, 52 though it should be noted that there were often small subgroups of participants with bipolar depression included in some of the depression studies. At this time, there was a single open-label pilot study examining MST in OCD. 53 Finally, there was one open-label feasibility trial 32 of conjoint MST and dialectical behavioral therapy (DBT) in suicidal patients with BPD comorbid with TRD. Full study characteristics are summarized in Table 1.
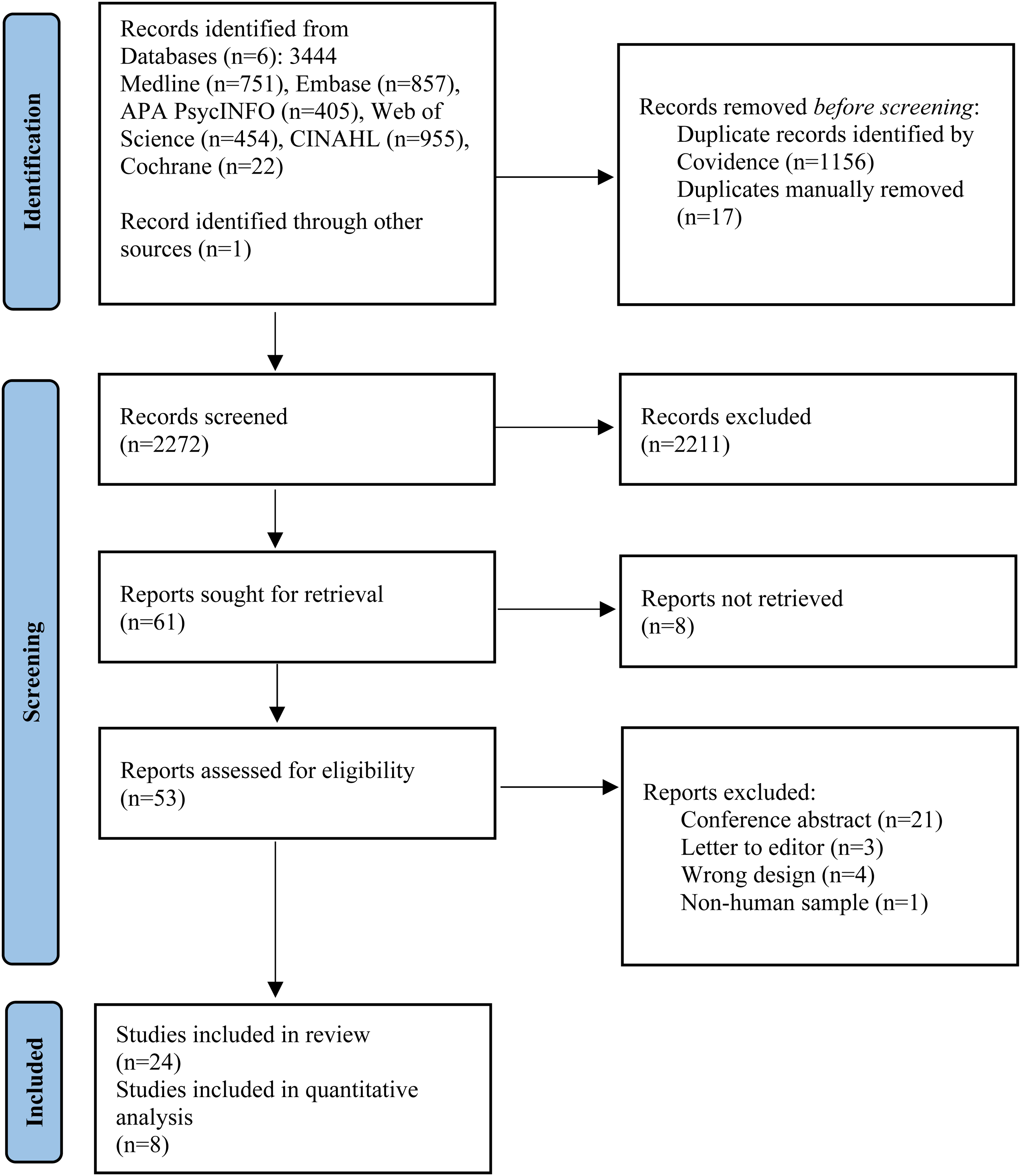
PRISMA flow diagram.
Study Design and Demographic-Clinical Characteristics of Subjects Included in Analysis.
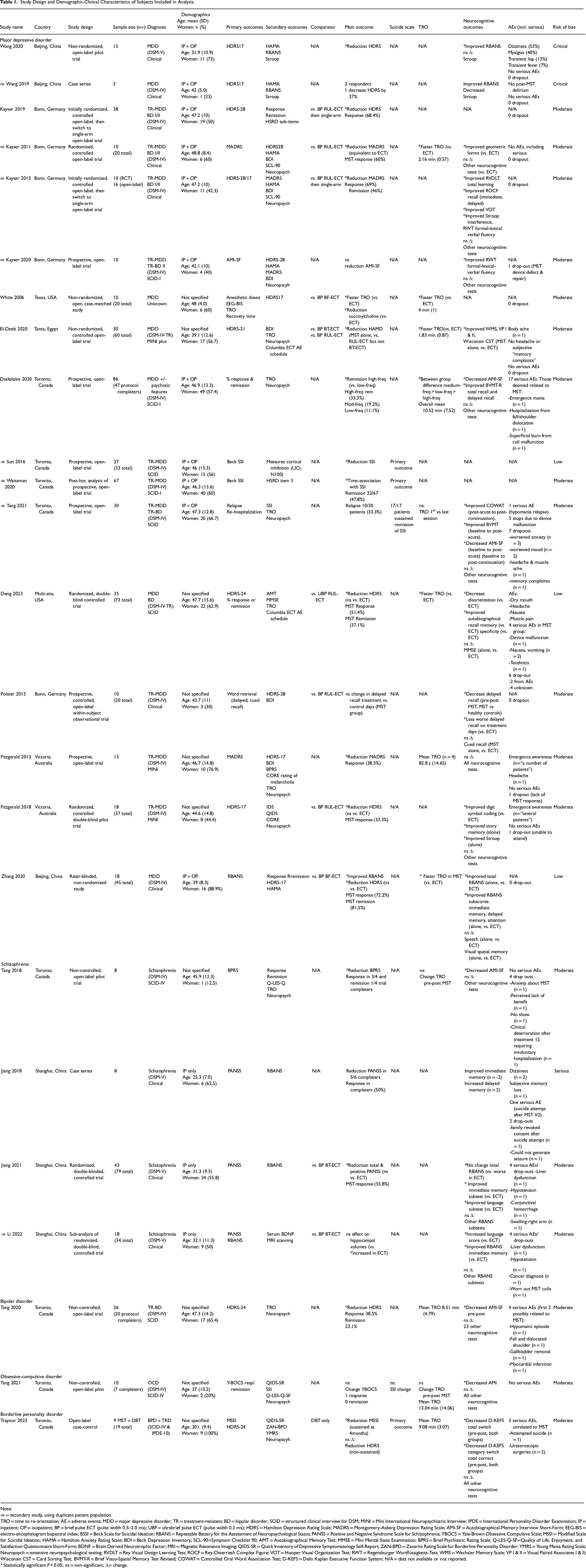
Note:
⇒ = secondary study, using duplicate patient population.
TRO = time to re-orientation; AE = adverse events; MDD = major depressive disorder; TR = treatment-resistant; BD = bipolar disorder; SCID = structured clinical interview for DSM; MINI = Mini International Neuropsychiatric Interview; IPDE = International Personality Disorder Examination; IP = inpatient; OP = outpatient; BP = brief pulse ECT (pulse width 0.5–2.0 ms); UBP = ultrabrief pulse ECT (pulse width 0.3 ms); HDRS = Hamilton Depression Rating Scale; MADRS = Montgomery-Asberg Depression Rating Scale; AMI-SF = Autobiographical-Memory Interview Short-Form; EEG-BIS = electro-encephalogram bispectral index; BSSI = Beck Scale for Suicidal Ideation; RBANS = Repeatable Battery for the Assessment of Neuropsychological Status; PANSS = Positive and Negative Syndrome Scale for Schizophrenia; YBOCS = Yale-Brown Obsessive Compulsive Scale; MSSI = Modified Scale for Suicidal Ideation; HAMA = Hamilton Anxiety Rating Scale; BDI = Beck Depression Inventory; SCL-90=Symptom Checklist 90; AMT = Autobiographical Memory Test; MMSE = Mini Mental State Examination; BPRS = Brief Psychiatric Rating Scale; Q-LES-Q-SF=Quality of Life, Enjoyment, and Satisfaction Questionnaire Short-Form; BDNF = Brain Derived Neurotrophic Factor; MRI = Magnetic Resonance Imaging; QIDS-SR = Quick Inventory of Depressive Symptomatology Self-Report; ZAN-BPD = Zanarini Rating Scale for Borderline Personality Disorder; YMRS = Young Mania Rating Scale; Neuropsych = extensive neuropsychological testing; RVDLT = Rey Visual Design Learning Test; ROCF = Rey-Osterrieth Complex Figure; VOT = Hooper Visual Organization Test; RWT = Regensburger Wortflüssigkeits-Test; WMS = Wechsler Memory Scale; VP I & II = Visual Paired Associates I & II; Wisconsin CST = Card Sorting Test, BVMT-R = Brief Visuo-Spatial Memory Test Revised; COWAT = Controlled Oral Word Association Test; D-KEFS = Delis Kaplan Executive Function System; N/A = data not available or not reported.
Statistically significant P < 0.05; ns = non-significant; Δ= change.
Table 2 provides an overview of the MST parameters used in retrieved studies. Earlier studies chose between low-, medium- and high-frequency stimulation. More recent studies have largely adopted a high-frequency stimulation of 100 Hertz (Hz). There are two commonly used positions in most studies, the vertex and frontal cortex at midline. For ECT, right unilateral (RUL) ECT has been the most common comparator in depression, followed by bifrontal and then bitemporal. Schizophrenia studies have only compared MST to bitemporal ECT.
Detailed Treatment and Stimulation Parameters of Included Studies.
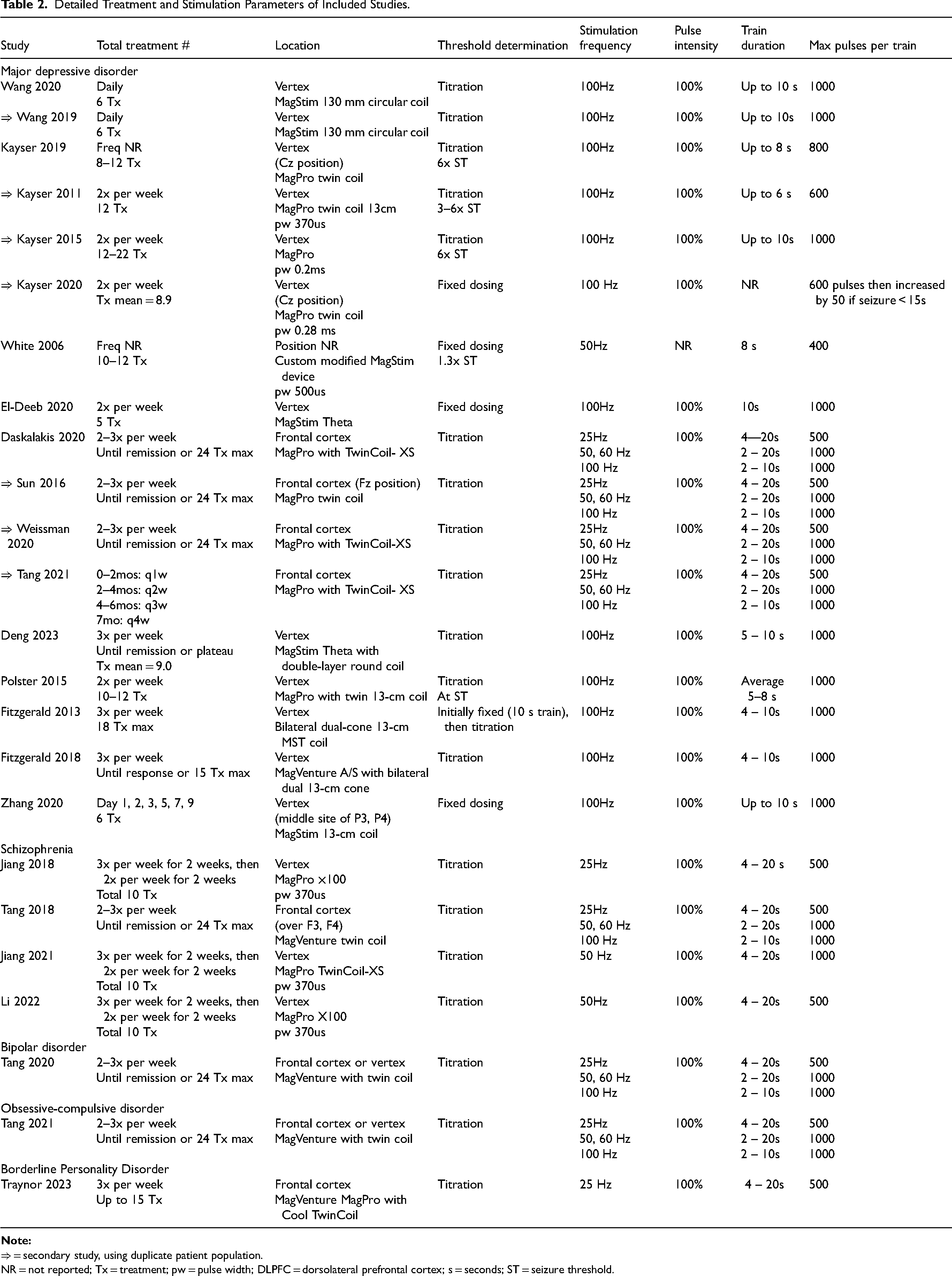
⇒ = secondary study, using duplicate patient population.
NR = not reported; Tx = treatment; pw = pulse width; DLPFC = dorsolateral prefrontal cortex; s = seconds; ST = seizure threshold.
The quantitative analysis was limited to patients with depression as the number of studies allowed this analysis to be conducted. The first analysis of three RCTs comparing antidepressant efficacy of MST versus ECT comprised a total 130 patients. A sensitivity analysis was conducted of both RCTs and open-label studies comparing MST versus ECT, totaling 255 patients. Finally, we examined antidepressant efficacy of MST alone by including all possible studies. After removing secondary studies, five open-label studies (with or without ECT comparator) were combined with the three active MST arms of the RCTs to form the pooled all-studies analysis of 248 MST patients.
MST in MDD
Symptom Improvement
Meta-Analysis of MST Versus ECT on Depressive Symptoms in RCTs
Trials included in this analysis employed a randomized, controlled design, comparing MST to ECT. All three studies measured depressive symptoms via the Hamilton Depression Rating Scale (HDRS), 54 a widely-used, clinician-administered scale for depression. However, they employed slightly different versions: the 17-item, 24-item and 28-item versions.
In the three trials analyzed, the cumulative effect size was 0.207 in favour of ECT (95% CI −0.132 to 0.545, Z-value = 1.194) (Figure 2(a)). The change in depressive symptoms for MST was not significantly different than for ECT (P = 0.232). It should be noted that all three confidence intervals cross zero, signifying likely no difference between groups. Further, one RCT 33 was weighted at 54.9%, meaning it contributes much more importantly to pooled results than the other studies. The test for heterogeneity showed no inconsistency (I2 = 0%, Q-value = 0.667). It is not likely to be a reliable measure due to lack of power and potential for bias with only three studies. Both fixed and random effects models were computed with no statistical difference in the results.
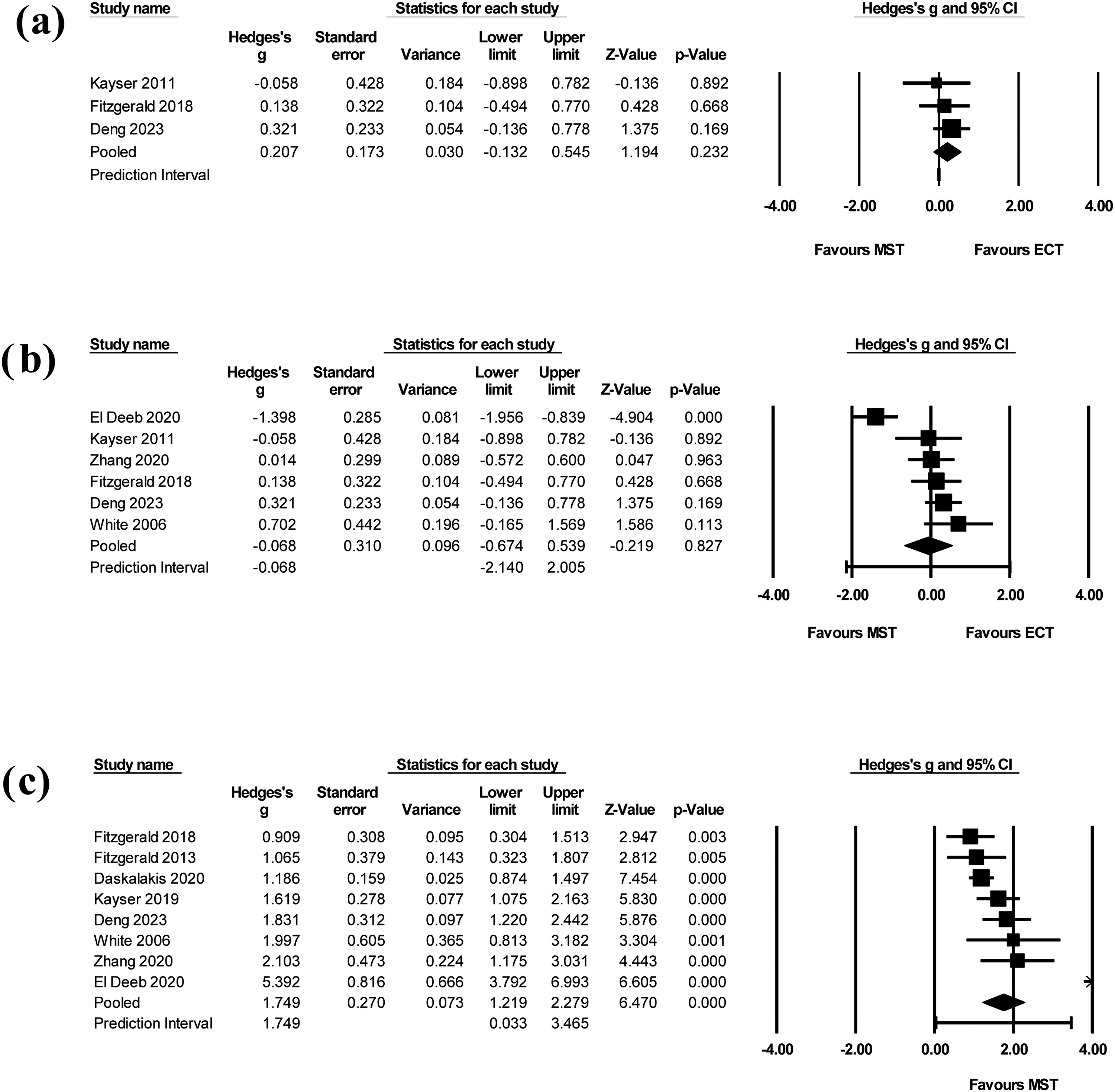
(a) Forest plot of MST versus ECT on depressive symptoms in RCTs. The cumulative effect size across three studies was 0.207 in favour of ECT (95% CI −0.132 to 0.545, Z-value = 1.194, P = 0.232). (b) Forest plot of MST versus ECT on depressive symptoms across RCTs and open-label trials. The cumulative effect size across six studies was −0.068 in favour of MST (95% CI −0.674 to 0.539, Z-value = −0.219, P = 0.827). (c) Forest plot of MST on depressive symptoms across all studies. The pooled effect size across eight studies included was 1.749 (95% CI 1.219 to 2.279, Z-value = 6.740, P < 0.005).
Meta-Analysis of MST Versus ECT on Depressive Symptoms Across RCTs and Open-Label Studies
A sensitivity analysis involved all studies comparing MST to ECT, using either randomized or open-label designs. Six studies were included. One open-label study only reported the baseline HDRS, not endpoint, and was thus excluded. 38
In the six studies, the cumulative effect size was −0.068 in favour of MST (95% CI −0.674 to 0.539, Z-value = -0.219) (Figure 2(b)). Again, the change in depressive symptoms was not significantly different than for ECT (P = 0.827). All but one study's confidence interval crossed zero. All studies contributed a similar weight between 14% and 19% in the analysis. Of note, when the main outlier study was removed, 37 the cumulative effect size resembled that of the previous analysis: a cumulative effect size of 0.214 in favor of ECT (95% CI −0.064 to 0.492). There was again no significant difference in depressive symptom reduction between MST and ECT (P = 0.131). The I2 statistic was 82% (Q-value = 27.968), indicating substantial heterogeneity. It should again be highlighted that this analysis contained less than 10 studies, affecting the interpretability of this measure. There was no significant difference between fixed and random effects models.
Meta-Analysis of MST on Depressive Symptoms Across all Studies
The final analysis combined the active MST arms of RCTs with all possible open-label studies with or without ECT comparator. Amongst the open-label studies, three studies40,44,47 were not included as they investigated MST in alternative formats, and five secondary studies28,35,41,42,45 were excluded. The pooled effect size across eight studies included was 1.749 (95% CI 1.219 to 2.279, Z-value = 6.740) (Figure 2(c)). The change in depressive symptoms after MST treatment was significant (P < 0.005). Most studies contributed similar weight or importance to the analysis, between 6% and 17%. The test for heterogeneity was substantial (I2 = 80%, Q-value = 34.729). Both fixed and random effects models were employed, with no significant difference in results.
Qualitative Analysis of MST on Suicidality
Only three studies35,44,45 reported on suicidality. However, these studies used the same sample of patients. The main clinical analysis by Weissman et al. was a post-hoc analysis of an open-label, prospective trial of 67 patients with TRD and baseline suicidality. MST treatment occurred until remission (0 on Beck Scale for Suicidal Ideation (SSI)) or a maximum of 24 sessions. Thirty-two patients achieved remission (47.8%), with a mean decrease in Beck SSI from 10.9 (4.9) to 6.0 (6.6) (P < 0.001). Tang et al. followed a subset of the remitters into continuation MST (decreasing frequency of MST sessions, with additional boosters as needed), totaling 17 patients. By study end, all 17 patients (100%) had continued remission of their suicidality.
Cognitive and Other Adverse Effects of MST
Fourteen studies examined a minimum of one neurocognitive measure before and after MST. Excluding those with alternative MST formats40,44,47 and secondary studies, 42 the ten remaining studies utilized different measures, such as time to reorientation, Folstein Mini Mental Status Exam (MMSE), the autobiographical memory test (AMT), the short-form autobiographical memory interview (AMI-SF), and the repeatable battery for neuropsychological status (RBANS). Seven studies reported either non-significant pre-post changes or improvement in all cognitive measures, two reported worsening of certain pre-post cognitive measures (namely autobiographical memory, delayed recall), and one study provided insufficient information. The mean time to orientation in reported studies is 3.99 min (0.65).
In addition, there were seven studies that examined the cognitive effects of MST versus ECT specifically. All seven report more favorable neurocognitive outcomes in MST than ECT in varied domains. The time to re-orientation was unanimously shorter in MST compared to ECT in the reported studies.28,33,34,36–39 If limited to randomized, controlled trials, MST carried less impairment in the AMT, 33 neglect (geometric forms) 28 and digit symbol coding. 34
Only six studies reported on adverse effects beyond cognition after those with alternative MST formats and duplicate data were removed. The commonly reported adverse effects amongst studies were: dizziness, headache, muscle ache and nausea. Two studies34,46 from the same research group reported emergence awareness in MST, despite using identical doses of succinylcholine and propofol to ECT. Three of the four studies28,33,34,37 with an ECT comparator reported higher adverse effects in ECT compared to MST. Regarding serious adverse events, the majority (83%) of studies reported no serious adverse events with MST. The one exception 29 reported a high absolute number, but only 3.4% of the serious adverse events were determined to be related to MST. The four studies with ECT comparator showed no serious adverse events in the MST arms.
Please refer to Table 1 for full details about the neurocognitive and other adverse effects of MST.
MST in Schizophrenia
Four studies examined the effects of MST in patients with schizophrenia. In general, the four studies showed antipsychotic efficacy, with improved or only slightly worsened cognition. The two early studies50,51 were smaller, open-label pilot trials, first assessing feasibility and acceptability in this population. The third study 48 by Jiang et al. is a randomized, controlled, double-blind study, comparing the effects of MST versus bitemporal ECT. The final study 49 was a secondary sub-analysis of the same RCT, with a specific focus on the serum brain-derived neurotrophic factor (BDNF) biomarker and hippocampus structural changes.
Symptom Improvement (Including Suicidality)
All four studies reported a reduction in psychiatric symptoms following treatment with MST. In the first study, 50 eight TR-schizophrenia patients underwent up to 24 sessions of MST. All subjects had a significant reduction in Brief Psychiatric Rating Scale (BPRS) from 42.6 at baseline to 32.4 after MST (P = 0.018). In the second pilot, 51 eight inpatients with schizophrenia received up to 10 sessions of add-on MST over four weeks. Only six patients received five or more sessions. Within this group, there were mean reductions of 27.3 and 11.2 in the Positive and Negative Syndrome Scale (PANSS) total score and PANSS positive score (P = 0.009) respectively. In the sole RCT, 48 79 inpatients were randomized to receive either 10 sessions of MST (n = 43) or ECT (n = 34) over four weeks. The per-protocol analysis (those receiving five or more sessions) of 37 patients treated with MST showed a significant reduction of 10 (7.5) in PANNS general score (P < 0.001). There was no significant difference in symptom reduction or response rates between the MST and ECT groups.
There was no systematic reporting of suicidality, via scale or other means, in the four studies. One pilot study 51 did report one suicide attempt in a patient after the second MST treatment, but deemed it unlikely to be related to MST treatment.
Cognitive and Other Adverse Effects
All four trials examined the neurocognitive effects of MST in patients with schizophrenia. Excluding the post-hoc analysis, the remaining studies used either the RBANS or other neuropsychological testing. In the first pilot study, 50 a worsening in the AMI-SF after MST was reported, though all other measures did not change significantly. In the second, 51 only three of eight patients could complete the RBANS, and the post-treatment scores were either stable or improved. Finally, the RCT demonstrated minimal RBANS changes in the 43 MST patients of the intention-to-treat analysis, while there was a worsening the ECT group (P < 0.05). There was significantly greater impairment in patients treated with ECT in the immediate memory and language subtests specifically. In summary, all studies in patients with schizophrenia demonstrated stable or improved cognitive testing following MST treatment, except for worsened autobiographical memory in one pilot study. The one trial comparing MST versus ECT noted significantly less impairment in patients with schizophrenia treated with MST.
Most studies did not report on common adverse effects. The main serious adverse events were either thought to be related to MST (e.g., conjunctival hemorrhage) or not related to MST (suicide attempt mentioned above, liver dysfunction secondary to anesthesia and hypotension secondary to anesthesia).
MST in Bipolar Disorder
One study 52 examined specifically the effects of MST in patients with treatment-resistant bipolar depression. Twenty-six patients were treated with up to 24 sessions of MST of varied orientations: low-, medium- or high-frequency prefrontal MST or high-frequency vertex MST. These 26 adequate-trial completers (received eight or more MST sessions) had a statistically significant reduction (P < 0.001) in HDRS-24 from baseline scores of 28.1 (4.4) to end of treatment scores of 17.8 (8.5). The corresponding effect size was large (d = 1.25, 95% CI 0.42–1.57) and slightly larger for the per-protocol completers. There was no specific data reported on suicidality.
This study also assessed 24 different neurocognitive measures at baseline and after MST. There was a statistically significant mean decrease of 18.9% (P < 0.001) on the AMI-SF, while the remaining 23 measures of cognition remained stable. Time to reorientation was 8.5 min (4.8). Otherwise, there were two serious adverse events reported, thought to be related to MST. The first was the emergence of hypomania days after protocol completion in a patient, while the second was a fall and shoulder dislocation in another patient.
As mentioned, six studies investigating MST in depression included a small proportion of patients with BD. However, there were no subgroup analyses performed and thus it was not possible to disentangle them from the larger unipolar depression cohort.
MST in OCD
One study 53 examined the effects of MST in patients with OCD. Ten patients with moderate-severe OCD, resistant to SSRI-medications, were treated with up to 24 MST treatments. Seven patients underwent an adequate trial (8 or more MST treatments), and only one achieved response. There was further no significant change in Yale-Brown Obsessive Compulsive Scale (Y-BOCS) score from baseline to endpoint in this group (Z = −0.08, P = 0.93). Similarly, there was a non-significant change in suicidality, as measured by the SSI (Z = −1.08, P = 0.28).
The mean time to reorientation for adequate trial completers was 13.0 (14.1) minutes, not significantly different than baseline (Z = −0.76, P = 0.45). A significant difference was found for the baseline-to-endpoint AMI-SF (Z = −2.21, P = 0.03), but no other neurocognitive outcomes. There were no serious adverse events reported amongst trial participants.
MST in BPD
One study 32 examined MST combined with psychotherapy in patients with BPD. Nineteen patients with moderate-severe suicidality and BPD comorbid with TRD were allocated to DBT alone (one hour of individual plus one hour of group therapy per week) versus MST (total of 15 treatments) combined with DBT. Only the MST-DBT group (n = 9) showed a significant reduction in suicidality as measured by Modified Scale for Suicidal Ideation (MSSI) (β = −12.03 CI −19.24 to −4.82, (SE) = 3.75; t[31] = −3.21; P < 0.01), sustained at four-month follow-up. Only the MST-DBT arm also showed improvement in HDRS and Zanarini Rating Scale for Borderline Personality Disorder (ZAN-BPD) after treatment.
The mean time to reorientation was 9.08 (3.07) minutes. A significant difference was found in the baseline-endpoint Delis-Kaplan Executive Function System (D-KEFS) category switch total correct (F[1,16] = 7.98; P = 0.01) and total switch (F[1,16] = 5.07; P = 0.04) for both groups. There were no other significant effects found in any of the other neurocognitive measures, including autobiographic memory. There were three serious adverse events unrelated to MST intervention.
Discussion
This study provides an up-to-date quantitative and qualitative synthesis of the efficacy and tolerability of MST in psychiatric disorders. We found 17 studies in depression (including three RCTs), four studies in schizophrenia (including one RCT), one study in bipolar disorder, one study in OCD and one study in BPD. A quantitative analysis of the patients with depression (n = 248) revealed a significant reduction in depressive symptoms with MST, without significant difference to ECT in the smaller RCT analysis (n = 130). A sensitivity analysis of RCTs and non-randomized studies comparing MST versus ECT (n = 255) then confirmed no significant difference in efficacy between the two treatments.
The antidepressant effects of MST found in this review are reinforced by recent studies. Chen et al. 21 performed a meta-analysis of 285 patients with depression from 10 non-randomized studies comparing MST with ECT. The results showed similar antidepressant efficacy, with shorter reorientation and less impaired recall in MST. Similarly, Cai et al. 22 did not find significant differences in study-defined remission and depressive symptom improvement between ECT and MST in four RCTs (n = 86). Taken together, evidence for the similarity in clinical efficacy of MST is continuing to mount and would now likely meet the threshold for level 2 evidence from depression guidelines. 19
That said, the preliminary evidence for MST's antidepressant effects requires careful consideration of the context. To start, the comparison to ECT is likely somewhat premature, as existing studies are too small and under-powered to detect true differences. Larger, multi-site RCTs will be necessary to confirm these initial signals, and a large, multi-centre trial is now nearing completion. 55 Furthermore, the existing studies examined MST versus ECT with RUL, bifrontal and bitemporal modalities— demonstrating an uncertainty about the most apt comparator to MST. The largest RCT to date 33 compared MST to ultrabrief pulse RUL-ECT, which may be appropriate, though bilateral ECT is widely considered the most effective form treatment. 56 It is most likely that research groups are simply following historical and institutional norms concerning pulse width, electrode placement, number of treatments and anesthetics. Yet some coherence in research will be necessary in order to truly understand MST's place in the therapeutic continuum and compared to ECT. Lastly, independent of its antidepressant effects, ECT has repeatedly demonstrated unique anti-suicidal properties.57,58 The investigation of MST's potential to reduce suicidality is promising, yet the evidence is still very limited.
Of note, the studies included also demonstrate the wide variation of MST practice in the literature. At this point, the optimal coil type, placement, frequency, pulses per train and treatment course length have yet to be fully determined. One of the included studies compared different stimulation frequencies in 86 patients; the findings indicated that high-frequency stimulation produced the most important antidepressant effects, with less time to orientation. 29 Indeed, the majority of MST trials in depression in the literature have employed a high-frequency stimulation over the vertex. This leaves the alternative treatment modalities open for further exploration. This is not dissimilar from ECT practice, which typically differs based on patient-related factors, treatment factors and institutional-geographic factors.59,60
In general, it is suggested that MST has a more benign cognitive side effect profile. The studies included showed more rapid orientation time and mostly preserved cognitive abilities (even some gains) after MST. For example, the time to reorientation across all reported MST studies was 5.93 min (1.59), while estimates in ECT range from 10 to 30 min.61,62 The anterograde and retrograde amnesia characteristic of ECT14–16 seems to be modest in MST. This is congruent with pre-clinical evidence, in both virtual conducting spheres and non-human primates, suggesting that MST seizure expression is less intense, more focal and more superficial, potentially sparing the deeper hippocampus.63,64 However, the strength of these conclusions is again limited by the low number of studies (typically under-powered due to small sample sizes) and heterogeneous neurocognitive testing across studies. In the future, it will be necessary to synthesize the neuropsychological measures between studies, ensuring common multi-domain testing that accounts for practice effects.
Outside of depressive disorders, there are still very limited conclusions to be drawn about the efficacy and safety of MST. Studies have started to accumulate in schizophrenia, followed by bipolar disorder, and these are likely the next major areas of exploration. There were no MST studies found for other indications of ECT (e.g., catatonia, Parkinson's disease, neurocognitive disorders). A search of the clinical trials online database reveals two upcoming non-inferiority trials between ECT and MST in patients with depression and two upcoming trials between ECT and MST in patients with bipolar depression. 65
Study Limitations
This study had multiple limitations. There is a small number of studies published to date on MST, from a small group of investigators and health centers. The majority of these studies are characterized by small sample sizes and open-label designs, with only a few medium-sized RCTs. As such, the quantitative analysis should be interpreted with caution. Furthermore, the studies also utilized different MST parameters, number of treatment sessions and outcome measures. There are also differences in ECT comparators. While this is indicative of the “real-world” clinical setting, it makes pooling effect sizes across studies more challenging. Finally, most studies had a short follow-up period of around 1–2 months. Given the high rates of relapse after a successful course of ECT in the first six months, 66 it is essential to determine the durability of MST effects.
Conclusion
MST is evolving as an alternative to ECT in treating severe and refractory psychiatric disorders. There is accumulating literature in depression, followed by bipolar disorder and schizophrenia. The potentially safer cognitive profile, with less post-ictal disorientation and amnesia, makes MST a particularly attractive alternative. Larger-scale, RCTs focusing on severe, treatment-refractory illness are needed. They should further make a concerted effort to harmonize neurocognitive outcomes with other studies, as well as include validated suicidality scales. The discrete effects of MST on suicidality have not yet been well characterized in comparison to ECT. Moreover, despite characterizing seizure induction, there are fewer studies exploring neurophysiological correlates in MST. This exploration is essential to uncovering the underlying mechanisms of action of MST. In sum, future research is necessary to reinforce MST as an effective, yet more cognitively-safe, convulsive therapy in our psychiatric armamentarium.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437241301005 - Supplemental material for Magnetic Seizure Therapy in Refractory Psychiatric Disorders: A Systematic Review and Meta-Analysis: La thérapie par convulsions magnétiques pour la prise en charge des troubles psychiatriques réfractaires : revue systématique et méta-analyse
Supplemental material, sj-docx-1-cpa-10.1177_07067437241301005 for Magnetic Seizure Therapy in Refractory Psychiatric Disorders: A Systematic Review and Meta-Analysis: La thérapie par convulsions magnétiques pour la prise en charge des troubles psychiatriques réfractaires : revue systématique et méta-analyse by Jake Prillo, Lorina Zapf, Caroline W. Espinola, Zafiris J. Daskalakis and Daniel M. Blumberger in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
The authors would like to thank Reena Besa, information specialist, Centre for Addiction and Mental Health, Toronto, Ontario, Canada, for their help in generating the search strategy.
Data Availability
The datasets used and/or analyzed for this meta-analysis are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LZ receives a stipend/salary from CAMH as a visiting graduate student. ZJD has received research and equipment in-kind support for an investigator-initiated study through Brainsway Inc and Magventure Inc and industry-initiated trials through Magnus Inc. He also currently serves on the scientific advisory board for Brainsway Inc. His work has been supported by the National Institutes of Mental Health (NIMH), the Canadian Institutes of Health Research (CIHR), Brain Canada and the Temerty Family, Grant and Kreutzcamp Family Foundations. DMB receives research support from CIHR, NIH, Brain Canada and the Temerty Family through the CAMH Foundation and the Campbell Family Research Institute. He received research support and in-kind equipment support for an investigator-initiated study from Brainsway Ltd. He was the site principal investigator for three sponsor-initiated studies for Brainsway Ltd. He also received in-kind equipment support from Magventure for two investigator-initiated studies. He received medication supplies for an investigator-initiated trial from Indivior. He is a scientific advisor for Sooma Medical. He is the Co-Chair of the Clinical Standards Committee of the Clinical TMS Society (unpaid). JP and CWE have no personal conflicts of interest to disclose.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.