
Abstract
Capacity to consent to treatment of substance use disorders at Ontario's Consent and Capacity Board: A review of past reported decisions
Plain Language Summary Title
An Ontario review of legal cases which have considered patients' ability to consent to substance use treatments
Plain Language Summary
In general, prescribers must consider whether informed consent was provided prior to starting a treatment. A patient is presumed to be capable to consent to a proposed treatment but could be incapable with respect to any medical treatment. While incapacity is often considered for psychiatric treatments, it could be relevant to substance use treatment like methadone or suboxone, which are also called “Opioid Agonist Therapies” or OAT. OAT is lifesaving and prevents relapse and overdose when a person has an opioid use disorder. If a patient is found incapable of consenting to a treatment, a Substitute Decisions Maker would become the decision maker. In such cases, the patient has the ability to contest or disagree with the finding, and this results in a tribunal hearing at the Consent and Capacity Board in Ontario (CCB). In certain circumstances, the CCB publishes what are known as its Reasons for Decision (RDs), which explain the tribunal's reasoning in coming to a decision in favour of the physician or the person found incapable. This information is publicly searchable. Our methods involved a search of all available CCB RDs in Ontario for search terms related to substance use treatment, such as "methadone”. We found that between June 1, 2003 (the date on reporting of RDs began) and June 27, 2023, only 71 RDs involved substance use search terms, out of a total of 10,463 reported RDs. Only one case involved the CCB upholding a finding of incapacity with respect to methadone treatment. These results imply that there are few cases in which the CCB has considered incapacity with respect to substance use treatment, although it is possible that these cases are reported at a lower frequency than other cases.
Introduction
Capacity is defined in Ontario's Health Care Consent Act (“HCCA”) as being able to understand the information that is relevant to making a treatment decision, and able to appreciate the reasonably foreseeable consequences of a decision or lack of decision. 1 The provider proposing the treatment must obtain consent from a capable patient, or make a finding that the person does not have capacity (and obtain consent from the person's substitute decision-maker). Any Ontario patient who has been found incapable may challenge that finding every six months with an application to the Consent and Capacity Board (CCB), a tribunal operating under the authority of the HCCA. 2
There are many reasons why a patient may not be capable with respect to substance use disorder (SUD) treatment such as opioid agonist treatment (OAT) for opioid use disorder or medications for alcohol use disorder (AUD). These reasons include psychosis from co-occurring schizophrenia, methamphetamine-induced psychosis, anoxic brain injury from overdose, traumatic brain injury, or neurocognitive disorder, several of which could be directly related to the SUD itself. The goal of this study is to identify publicly available CCB Reasons for Decision (RDs) in which incapacity findings with respect to OAT or AUD treatment have been considered.
Methods
We searched all published RDs of the Ontario CCB on the Canadian Legal Information Institute (CanLII) website, which has published RDs between 1 June 2003 (and previous 154 decisions) and the most recent update at the time of our search, 27 June 2023. 3 When the CCB conducts a hearing and makes a decision, a document confirming that decision is sent to the parties. However, RDs are only prepared by the CCB, and published on CanLII, if one of the parties to the hearing requests that the CCB provide RD within 30 days of the hearing. The CCB's Annual Report for the 2020/2021 fiscal year indicates it conducted 6300 CCB hearings in that fiscal year, 4 but only a minority of 785 RDs (12.4%) are available on CanLII.
The following keywords were searched: “methadone,” “buprenorphine,” “Suboxone,” “Sublocade,” “opioid agonist,” “opioid replacement,” “acamprosate,” and “naltrexone” to examine SUD treatment, and “surgery,” “schizophrenia,” “antipsychotic,” and “anti-psychotics” for comparison to common treatments contested before the CCB. Research Ethics Board review was not required as this information is in the public domain. All reported CCB Reasons for Decision containing any of the SUD key words were independently read by two authors (TSH and RG).
Results
Of 10,463 RDs reported on CanLII in this twenty-year period, 71 included the terms, “methadone,” “buprenorphine,” “Suboxone,” “opioid agonist,” “opioid replacement,” or “naltrexone.” Comparatively, 5016 included “schizophrenia,” 7148 included “antipsychotic” or “anti-psychotic” and 525 included “surgery.” None included “Sublocade” or “acamprosate.” Table 1 summarizes the results. In total, only six RDs considered the person's capacity to consent to SUD treatment. In 30 of the 71 RDs which contained the SUD treatment terms, treatment incapacity was an issue considered as part of the hearing, but incapacity specifically with respect to SUD treatment or OAT was not considered. Supplemental Table 1 contains a description of all cases.
Summary of Included Consent and Capacity Board Hearings (n = 71).
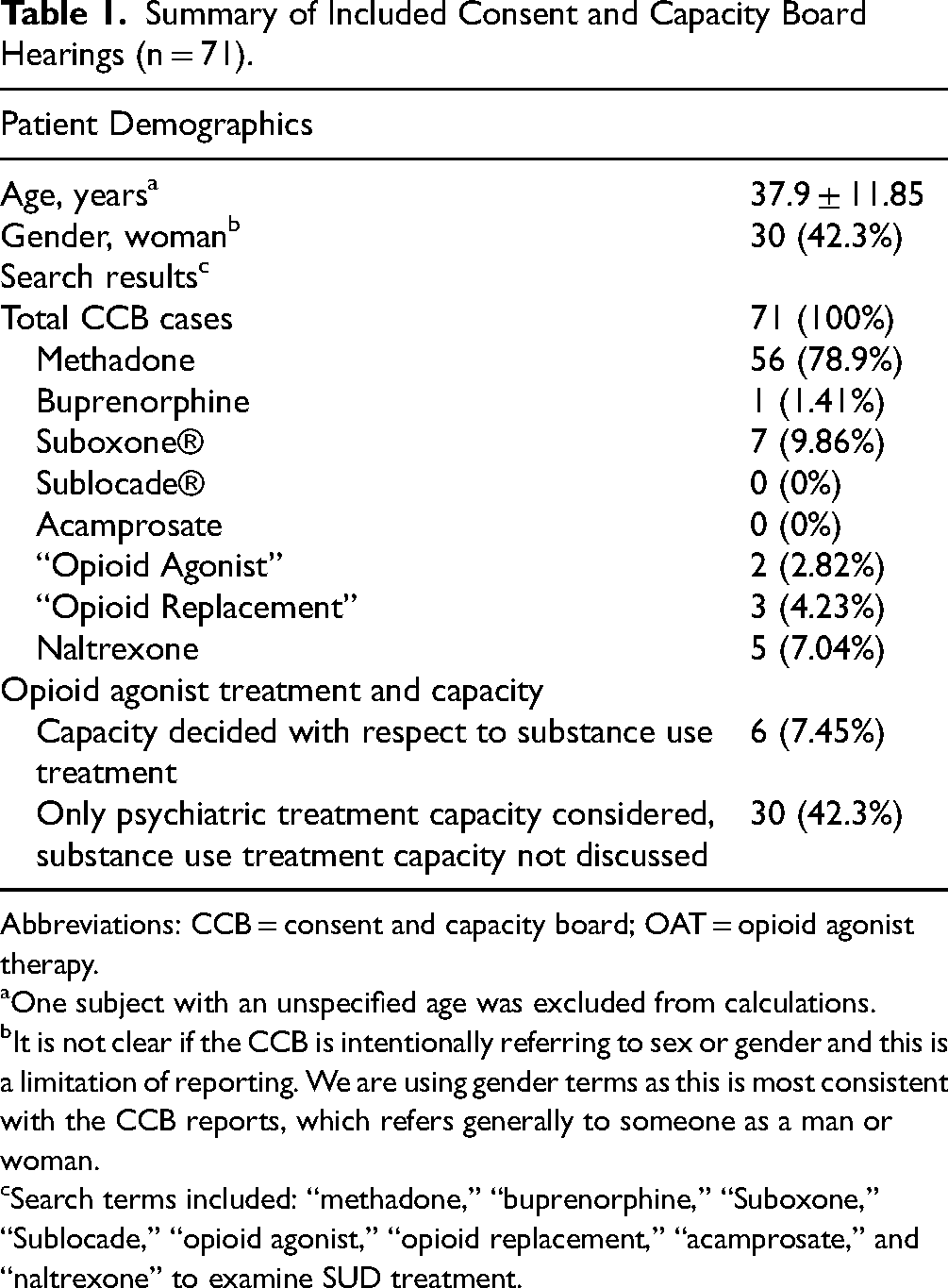
Abbreviations: CCB = consent and capacity board; OAT = opioid agonist therapy.
One subject with an unspecified age was excluded from calculations.
It is not clear if the CCB is intentionally referring to sex or gender and this is a limitation of reporting. We are using gender terms as this is most consistent with the CCB reports, which refers generally to someone as a man or woman.
Search terms included: “methadone,” “buprenorphine,” “Suboxone,” “Sublocade,” “opioid agonist,” “opioid replacement,” “acamprosate,” and “naltrexone” to examine SUD treatment.
In only one RD did the CCB make an incapacity finding with respect to OAT (Re AM, 2019). 5 This case involved a man in his 40s hospitalized since 2016 under the Ontario Review Board. He had diagnoses of schizophrenia, polysubstance abuse, opioid use disorder and antisocial personality disorder. At the 2019 hearing, he sought to review the finding that he was incapable of making decisions regarding treatment with antipsychotic medications, anti-anxiety medications, and opioid agonist therapy. The CCB discussed his inability to appreciate the purpose of methadone, and the fact that he did not believe he had a SUD, and upheld the incapacity finding. Although he was agreeable to taking methadone, he was considered incapable as he “continued to request higher doses then was clinically necessary” 5 and lacked insight into having a SUD.
Discussion
There are a few RDs issued by the CCB that consider the issue of incapacity with respect to SUD treatment. These results may suggest that clinicians infrequently make findings of incapacity with respect to SUD treatment, or it is possible that such findings are less likely to result in a hearing or a request for RDs.
Individuals may be unable to consent to life-saving OAT, and discontinuation of (or failure to start) OAT, particularly in a controlled hospital environment, may represent the greatest immediate threat to these patients’ morbidity and mortality with an extremely toxic unregulated drug supply. AUD represents a major source of morbidity and mortality, and individuals should be offered appropriate treatment with consideration of their capacity to consent to it. The CCB has indicated SUD treatments are the same as other medications. In the community and within psychiatric hospitals, the capacity to consent to or refuse SUD treatments should be considered part of psychiatric and medical care, particularly with methadone or buprenorphine.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437241261488 - Supplemental material for Capacity to Consent to Treatment of Substance Use Disorders at Ontario's Consent and Capacity Board: A Review of Past Reported Decisions
Supplemental material, sj-docx-1-cpa-10.1177_07067437241261488 for Capacity to Consent to Treatment of Substance Use Disorders at Ontario's Consent and Capacity Board: A Review of Past Reported Decisions by Tanya S. Hauck, Rachel Goud, Michele Warner, Susan Franchuk, Juveria Zaheer, Vicky Stergiopoulos, Victor M. Tang and Leslie Buckley in The Canadian Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.