
Abstract
Objectives
Heavy alcohol and drug use is reported by a substantial number of Canadians; yet, only a minority of those experiencing substance use difficulties access specialized services. Computer-Based Training for Cognitive Behavioural Therapy (CBT4CBT) offers a low-cost method to deliver accessible and high-quality CBT for substance use difficulties. To date, CBT4CBT has primarily been evaluated in terms of quantitative outcomes within substance use disorder (SUD) samples in the United States. A comparison between CBT4CBT versus standard care for SUDs in a Canadian sample is critical to evaluate its potential for health services in Canada. We conducted a randomized controlled trial of CBT4CBT versus standard care for SUD.
Methods
Adults seeking outpatient treatment for SUD (N = 50) were randomly assigned to receive either CBT4CBT or treatment-as-usual (TAU) for 8 weeks. Measures of substance use and associated harms and quality of life were completed before and after treatment and at 6-month follow-up. Qualitative interviews were administered after treatment and at follow-up, and healthcare utilization and costs were extracted for the entire study period.
Results
Participants exhibited improvements on the primary outcome as well as several secondary outcomes; however, there were no differences between groups. A cost-effectiveness analysis found lower healthcare costs in CBT4CBT versus TAU in a subsample analysis, but more days of substance use in CBT4CBT. Qualitative analyses highlighted the benefits and challenges of CBT4CBT.
Discussion
Findings supported an overall improvement in clinical outcomes. Further investigation is warranted to identify opportunities for implementation of CBT4CBT in tertiary care settings.
Plain Language Summary Title
Evaluating a digital intervention targeting substance use difficulties
Plain Language Summary
Why was the study done?
Heavy alcohol and drug use is frequent in the Canadian population, although very few people have access to treatment. The digital intervention, Computer-Based Training for Cognitive Behavioural Therapy (CBT4CBT), may provide a low-cost, high-quality, and easily accessible method of treatment for substance use difficulties. Limited research on this digital intervention has been conducted in Canadian populations, and few studies thus far have evaluated participants’ subjective experience using the intervention, along with the cost on the Canadian healthcare system.
What did the researchers do?
The research team recruited participants and provided access to either CBT4CBT or to standard care at a mental health hospital for 8 weeks. Participants were asked questions about their substance use and related consequences, quality of life, and thoughts on the treatment they received. Information regarding healthcare use and the cost to the healthcare system was also gathered.
What did the researchers find?
Participants in both groups improved with regards to their substance use, some related consequences, and psychological quality of life. Participants provided insight on the benefits and challenges of both types of treatment. It was also found that the CBT4CBT intervention was less costly.
What do these findings mean?
These findings support that adults receiving CBT4CBT and standard care both improved to a similar degree in this sample. Participant feedback may inform future studies of how best to implement this intervention in clinical studies. Future studies with larger samples are needed to further examine whether CBT4CBT can increase access to supports and be beneficial in the Canadian healthcare system.
Introduction
Heavy alcohol and drug use is reported by a substantial number of Canadians, and accounts for 40 billion dollars to Canadian society each year. 1 However, only a minority of those experiencing substance use difficulties access specialized services, 2 highlighting the need for scalable treatment alternatives. Cognitive behavioural therapy (CBT) is empirically supported for the treatment of substance use disorders (SUDs); yet, this treatment is rarely implemented with high fidelity in clinical practice. 3 The components of CBT are adaptable, however, and have exhibited promise in reducing substance use. 4
Computer-Based Training for Cognitive Behavioural Therapy (CBT4CBT) is an online treatment program 5 that leverages the potential of this digital format, providing psychoeducation and skills building using an interactive form of delivery. CBT4CBT initially demonstrated efficacy as an adjunct to standard care in adults seeking addiction treatment5,6; effects were then replicated in an investigation of cocaine misuse. 7 Kiluk and colleagues 8 reported the first investigation of CBT4CBT as a stand-alone treatment in adults with alcohol use disorder (AUD), where CBT4CBT was comparable to standard care or standard care plus CBT4CBT. In a subsequent investigation, 9 CBT4CBT as a stand-alone treatment was superior to standard care in adults with a range of SUDs, but not different from clinician-delivered CBT. In this study, CBT4CBT was associated with better retention compared to standard care or in-person CBT.
The current investigation aims to extend this research to include qualitative outcomes and the first cost-effectiveness analysis of this innovative program in Canada. Economic investigations are required to support the implementation of novel treatment approaches into health services. 10 We compared the efficacy and cost-effectiveness of a stand-alone implementation of CBT4CBT to treatment-as-usual (TAU). The primary hypothesis was that CBT4CBT will be associated with greater decreases in substance use frequency compared to TAU. Secondary hypotheses were that CBT4CBT will be associated with (a) greater improvements in secondary outcomes such as SUD symptom severity and quality of life, and (b) lower healthcare costs and thus, cost-effectiveness, compared to TAU. Hypotheses were not specified for qualitative analyses, which aimed to elucidate the patient experience of this program in this clinical context.
Methods
Participants
The study included 50 participants, ranging in age from 22 to 73 years (Mage = 39.98, SD = 11.42). Participants were registered with outpatient services at a psychiatric hospital in Ontario, Canada. Participants were included if they met the following criteria: ≥ 18 years of age; fluency in English; understanding and willingness to comply with study requirements; meet DSM-5 criteria for current SUD according to the Structured Clinical Interview for DSM-5 (SCID-5); 11 have used substances in past 30 days according to the Timeline Follow-Back (TLFB); 12 seeking treatment for substance use. Exclusion criteria: untreated or unstable severe psychiatric or medical disorder that would impede participation; acute suicidal or homicidal ideation requiring immediate intervention; unable to read at a sixth-grade level. The institutional Research Ethics Board approved study procedures and all participants provided written informed consent.
Procedure
We conducted a parallel design randomized control trial with a 1:1 allocation ratio (ClinicalTrials.gov identifier: NCT03767907. See https://clinicaltrials.gov/ct2/show/NCT03767907; Figure 1). Participants were recruited from January 2019 to August 2020 following standard registration procedures. Prospective participants completed an initial telephone interview to assess basic demographic and clinical characteristics, and then a more in-depth in-person assessment to obtain fulsome demographic and health information. Notably, study assessments were switched to remote during the COVID-19 pandemic. Eligible participants were enrolled and randomized after the baseline “Week 0” assessment. Participants completed a post-treatment “Week 8” assessment including quantitative and qualitative measures. The same measures were administered at a 6-month follow-up (“Month 6”). Healthcare utilization and costs were extracted from the health record from baseline to Month 6. Randomization was stratified according to sex and diagnosis (AUD only vs. other) in randomly generated block sizes, without replacement. Randomization was conducted by an independent biostatistical consultant (sequences generated using R Studio), with allocation concealment ensured using sequentially numbered, opaque, sealed envelopes. Outcomes assessors blind to group assignment rated interview measures.
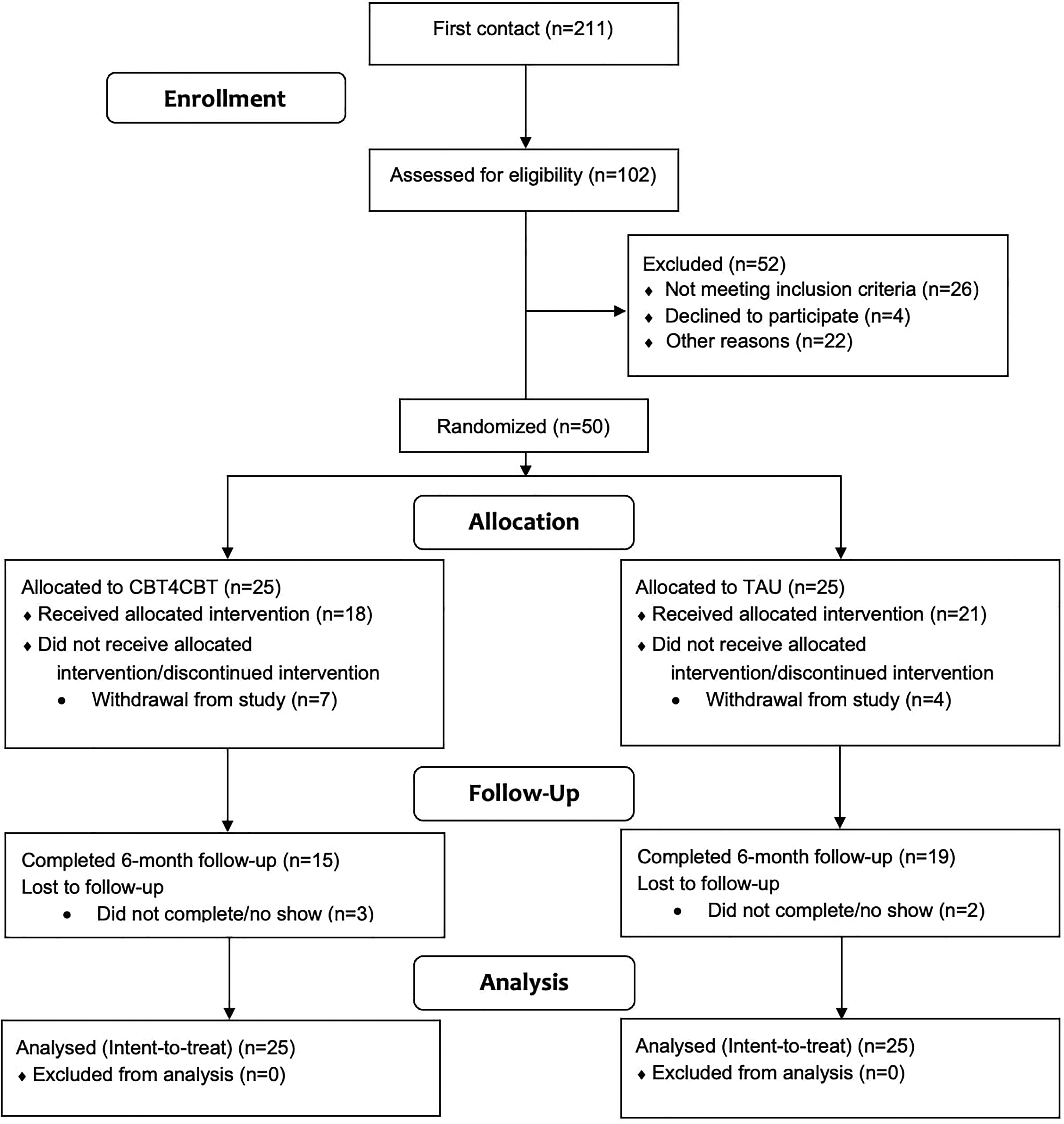
Consort diagram.
Interventions
CBT4CBT: CBT4CBT consisted of seven online modules, including interactive videos presenting characters portrayed by professional actors struggling with real-life situations. 5 These characters experience a common risky situation or problem and then, after the skill is presented and used, negotiate that situation without substance use. The program is user-friendly, requires minimal computer experience or reading, and includes interactive exercises to teach and model effective use of skills and strategies.
TAU: The active control intervention consisted of group therapy, supported by individual therapy as needed. Group therapy protocols ranged from 8 to 12 sessions. Models of therapy were primarily cognitive behavioural, with some groups including motivational enhancement, dialectical behavioural therapy concepts and mindfulness. Participants attended M = 3.58 (SD = 3.29) groups during the 8 weeks; no individual sessions were requested. All participants, regardless of their randomized condition, received psychiatric and emergency services as needed.
Measures
All quantitative measures were administered at Weeks 0, 8, and Month 6. The primary outcome was the number of days of use of the primary substance over the past 30 days, as measured by the TLFB. 12 Secondary outcomes were as follows: severity of the primary SUD, measured using the SCID-5 module E; 11 psychiatric functioning using the Psychiatric Composite score of the Addiction Severity Index (ASI);13,14 severity of drug dependence from the Severity of Dependence Scale (SDS) 15 (α=0.77); Global Severity Index (GSI) from the Brief Symptom Inventory (BSI)14,16 (α=0.97); and all 4 domains of the World Health Organization Quality of Life Assessment (WHOQOL-BREF)17,18 (physical α=0.82; psychological α=0.84; social relationships α=0.69, environment α=0.88).
Analyses
Efficacy Analysis: To evaluate efficacy, a generalized linear mixed model was conducted where the number of days the primary substance was used in the past 30 days was the level 1 primary outcome nested within participant. A Poisson distribution with a log link function was used. Time (pre-treatment, post-treatment) and group (CBT4CBT, TAU) were entered as fixed effects and individual subjects were specified as random effects.
To evaluate efficacy for secondary outcomes, mixed effect models were conducted, with each secondary outcome evaluated in separate models. Time was entered as a within-subject factor with two levels (pre-treatment, post-treatment), and group as a between-subject factor with two levels (CBT4CBT, TAU); individual subjects were specified as random effects. Mixed effect models handle missing values using maximum likelihood estimation. 19 We followed the intention-to-treat principle and analyzed all randomized participants. Models were run with and without covariates, including age, sex, primary diagnosis (AUD only vs. other), and the COVID-19 pandemic (acute treatment outcome assessed before vs. after onset). All models were also conducted with the inclusion of the 6-month time point to evaluate similarity of effects over time.
An a priori power calculation indicated that the sample size required to locate a small-to-medium effect size based on Kiluk et al., 9 a power of 80% (for main effects or interactions), and an alpha level of 0.05 is 54 participants or 27 per group.
Economic Evaluation: A cost-effectiveness analysis was undertaken for the primary outcome – the number of days used of the primary substance – in line with Canadian Agency for Drugs and Technologies in Health (CADTH) guidelines 20 and Consolidated Health Economic Evaluation Reporting Standards (CHEERS). 21 We adopted the perspective of the publicly funded healthcare payer.
CBT4CBT cost included the time per participant spent to show how to use the program ($10 for 15 min based on an hourly wage rate of $35.73) and the program fee ($140 per participant). Data on healthcare utilization and time spent by staff per service were extracted from the electronic health record. Staffing costs included physician visits and other OHIP-funded visits to allied health professionals. Three costing categories were identified: counselling, medical and administrative services. Total service cost was estimated by multiplying the hourly compensation for the service by the time spent providing the service.22,23 (see Supplemental Table S1 for more details). Although the cost-effectiveness analysis solely included the costs of services received at the study site, participants were also asked at each visit regarding their expenditures on healthcare outside of this site, using the Program and Client Costs Substance Abuse Treatment.24,25
Costs and outcomes were compared at follow-up, as mean values by arm with standard errors. An incremental cost-effectiveness ratio (ICER), defined as the mean difference in cost between groups divided by the mean difference in effect (i.e., the extra cost required to gain an additional unit of health), was calculated for the cost-effectiveness analysis. Of the participants randomized to treatment, 33 had the required follow-up outcome assessment (i.e., TLFB) to complete the cost-effectiveness analyses.
Qualitative Analysis: The qualitative component of the study was organized as a qualitative description design. 26 Semi-structured interviews were deployed with a focus on (1) what was and was not working for participants based on how they gave meaning to their experiences, and (2) “health work” 27 or practices surrounding health, including what individuals do to take care of themselves, and how they access and utilize health information and services. 28 All interviews were audio-taped and transcribed verbatim. Here, we contrast what did and did not work well for participants with a focus on CBT4CBT. The sample consisted of 21 participants at week 8 (CBT4CBT n = 11, TAU n = 10; 25 min on average) and 17 at month 6 (CBT4CBT n = 9, TAU n = 8; 12 min on average). Analyses were conducted on participants for whom COVID-19 did not impact acute treatment, until saturation was met.
Thematic analysis of the transcripts was conducted to offer a summative description based on how participants gave meaning to their experiences. Data analysis focused on identifying, analyzing and reporting patterns 29 and included a process that involved both open and focused coding. 30
Results
Participant Descriptives
The majority of participants (N = 50) were heterosexual (81.6%), identified as a man (69.4%), and were never married at the time of study (53.1%). The majority of the sample identified as White European and/or White North American (67.3%; see Table 1). Overall, 76% of individuals reported alcohol as their primary substance, 10% reported cannabis, 10% reported cocaine, 4% reported another substance as their primary substance of concern. 42.9% of the sample was diagnosed with AUD only, whereas 57.1% was diagnosed with either AUD plus another SUD, or another SUD without AUD. Co-occurring conditions were present in 58% (n = 29), including: persistent depressive disorder (36%, n = 18), major depressive disorder (30%, n = 15), generalized anxiety disorder (20%, n = 10), social anxiety disorder, panic disorder, agoraphobia or specific phobia (24%, n = 12), post-traumatic stress disorder (10%, n = 5), and other (6%, n = 3). 36% (n = 18) met criteria for more than one co-occurring diagnosis. Baseline demographic characteristics between groups were not significant.
Participant Descriptives.
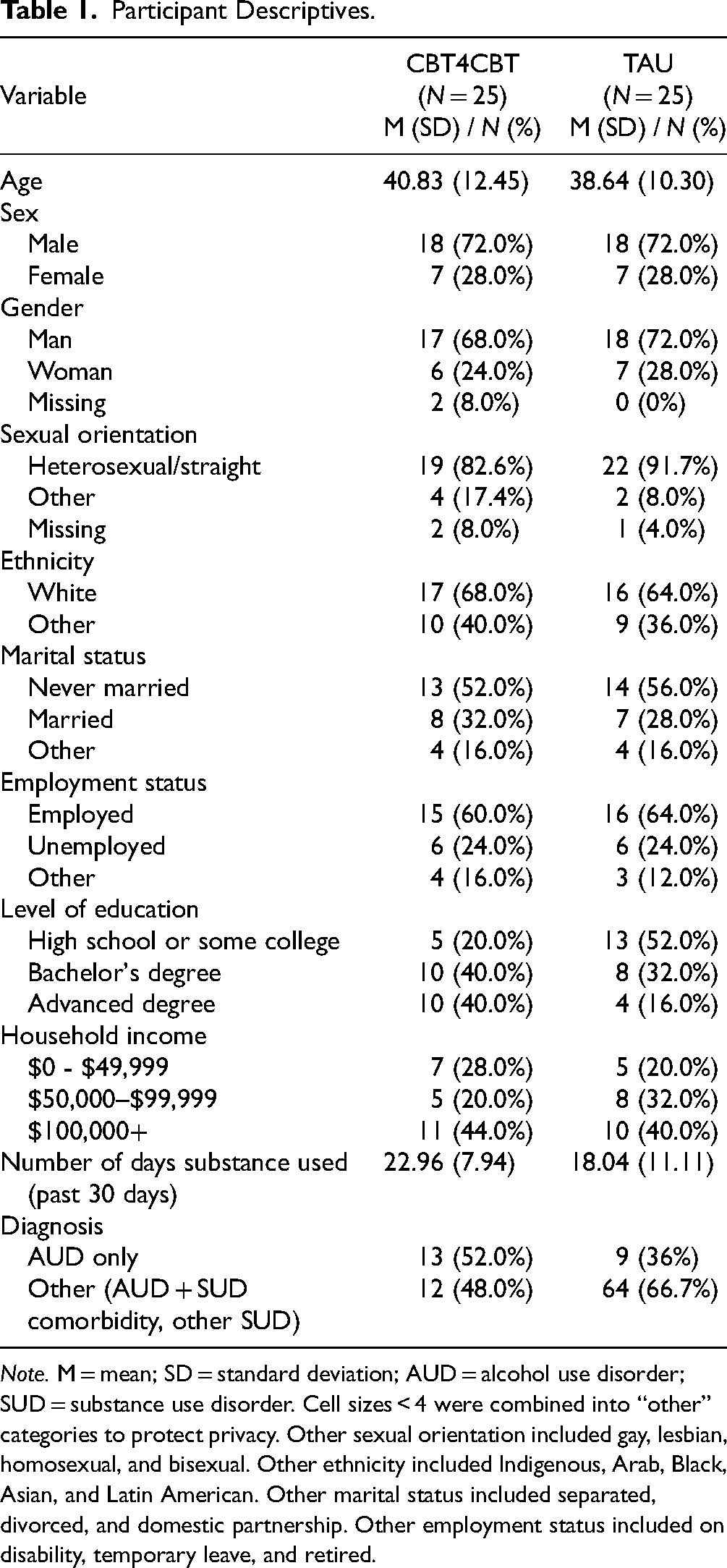
Note. M = mean; SD = standard deviation; AUD = alcohol use disorder; SUD = substance use disorder. Cell sizes < 4 were combined into “other” categories to protect privacy. Other sexual orientation included gay, lesbian, homosexual, and bisexual. Other ethnicity included Indigenous, Arab, Black, Asian, and Latin American. Other marital status included separated, divorced, and domestic partnership. Other employment status included on disability, temporary leave, and retired.
Efficacy Analyses
Primary Outcome: Generalized linear mixed effects models revealed a main effect of time (F = 6.90, P = 0.01), such that both groups improved from Week 0 (M = 16.70) to 8 (M = 14.49). There was also a main effect of group (F = 4.76, P = 0.03), such as that individuals in the CBT4CBT group had higher overall number of days used of the primary substance (M = 19.70) compared to the TAU group (M = 12.29).
Secondary Outcomes: Mixed effects models revealed main effects of time for multiple study outcomes, such that scores improved from Week 0 to 8 on SCID-5 Module E, BSI GSI, and WHOQOL-Bref Psychological domain scores (see Table 2a). There were no significant interactions between time and study group for any outcomes.
Efficacy Analyses.
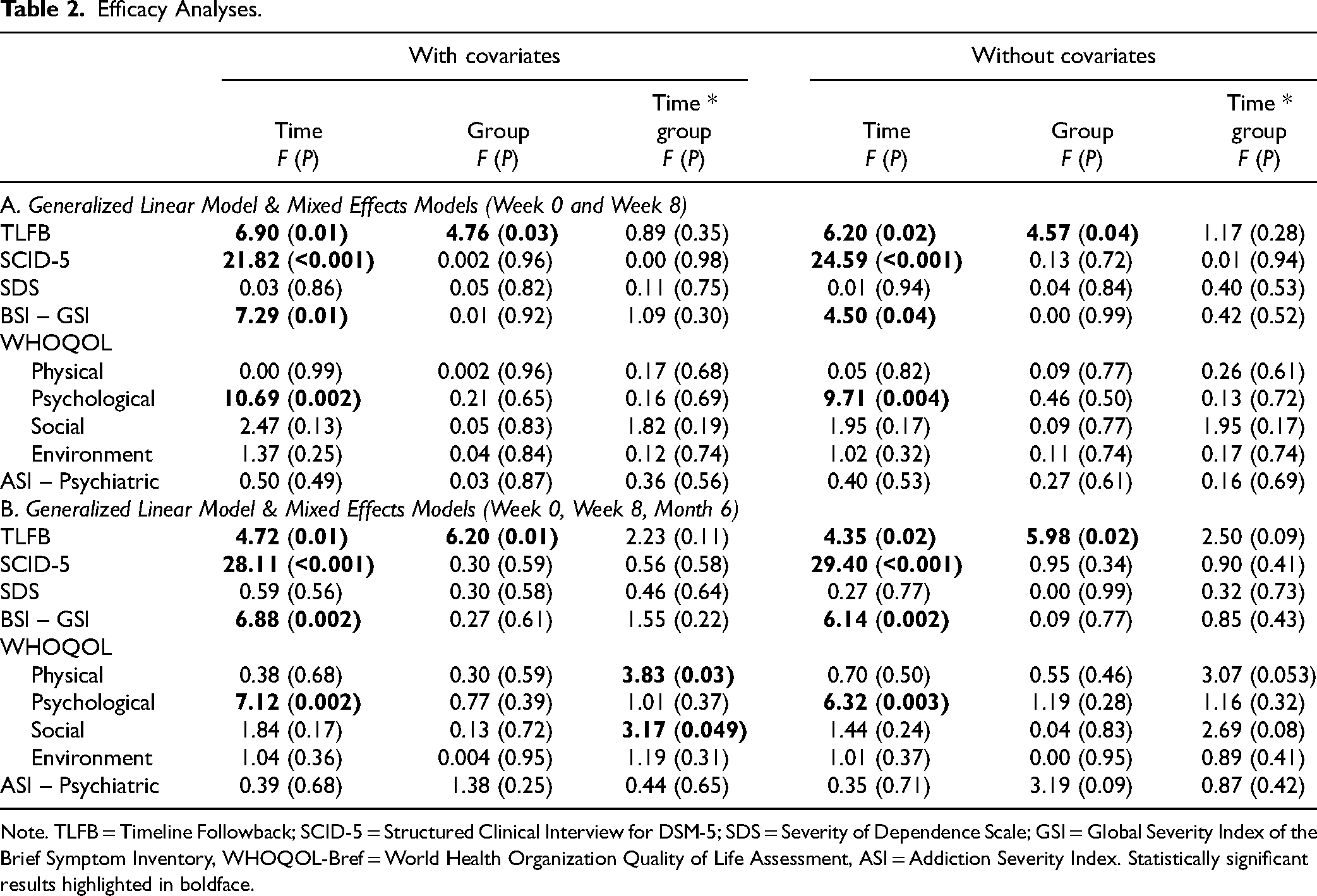
Note. TLFB = Timeline Followback; SCID-5 = Structured Clinical Interview for DSM-5; SDS = Severity of Dependence Scale; GSI = Global Severity Index of the Brief Symptom Inventory, WHOQOL-Bref = World Health Organization Quality of Life Assessment, ASI = Addiction Severity Index. Statistically significant results highlighted in boldface.
Analyses incorporating the 6-month follow-up assessment demonstrated the same pattern of effects (see Table 2b). Two time×group effects were located in these analyses for two domains of the WHOQOL; however, as these effects were not replicated across analyses with and without covariates, they are not interpreted substantively. See Supplemental Table S2 for marginal means for each outcome.
Cost-Effectiveness Analyses
Average and incremental healthcare resource utilization are reported in Table 3a for both groups. Compared to TAU, CBT4CBT had fewer counselling sessions on average per participant. The categories in percentage of total costs were medical care (CBT4CBT: 27%; TAU: 30%), administrative tasks (CBT4CBT: 7%; TAU: 7%) and counselling (CBT4CBT: 54%; TAU: 65%).
Average and Incremental Healthcare Utilization, Healthcare Costs and Health Outcomes.
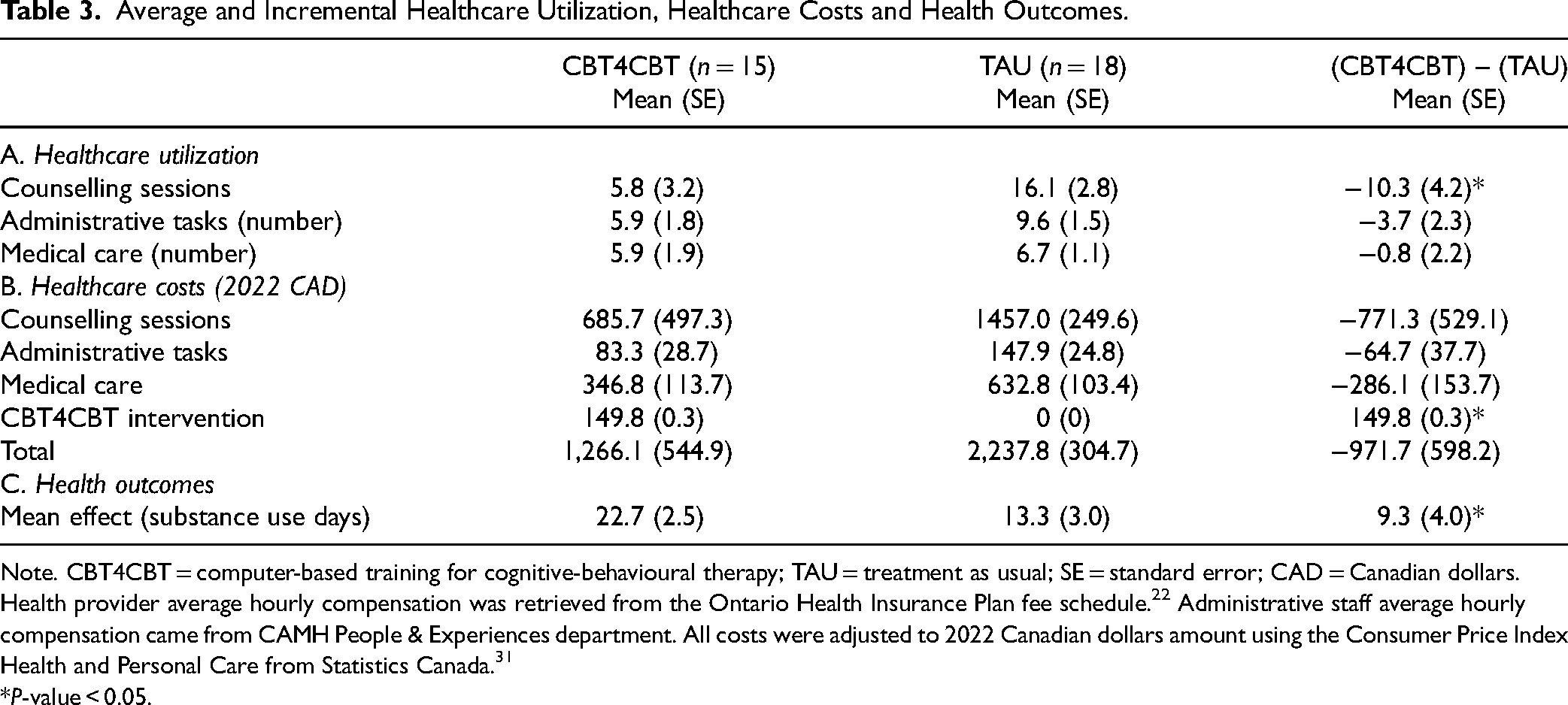
Note. CBT4CBT = computer-based training for cognitive-behavioural therapy; TAU = treatment as usual; SE = standard error; CAD = Canadian dollars.
Health provider average hourly compensation was retrieved from the Ontario Health Insurance Plan fee schedule. 22 Administrative staff average hourly compensation came from CAMH People & Experiences department. All costs were adjusted to 2022 Canadian dollars amount using the Consumer Price Index Health and Personal Care from Statistics Canada. 31
*P-value < 0.05.
Table 3b and Table 3c presents the two groups’ average and incremental costs and outcome differences. Although the average incremental total cost was not statistically significant, it indicated a lower average treatment cost of $972 per participant. Within this subsample analysis, CBT4CBT was associated with more substance use days compared to TAU. The ICER for the primary outcome was $104.2/substance use days, suggesting that CBT4CBT was less costly but was associated with more substance use days. Sensitivity analyses controlling for age, sex and baseline values of substance use days showed similar results. Notably, only one participant reported limited treatment expenditures during the study period.
Qualitative Analyses
CBT4CBT: Themes identified during the qualitative analysis are reviewed below, with illustrative quotes in Table 4. At Week 8, improved subjective well-being was reported by many participants as a benefit of CBT4CBT, although this was often described as small in size. As 109 summarized, “health-wise I feel a little better.” Some participants reported substantial changes in substance use, describing how they are “drinking less…I feel like my drinking has, um, reduced quite a bit. And that was my goal, to kind of get that more under control” (41).
Qualitative Analysis: Themes and Illustrative Quotes.
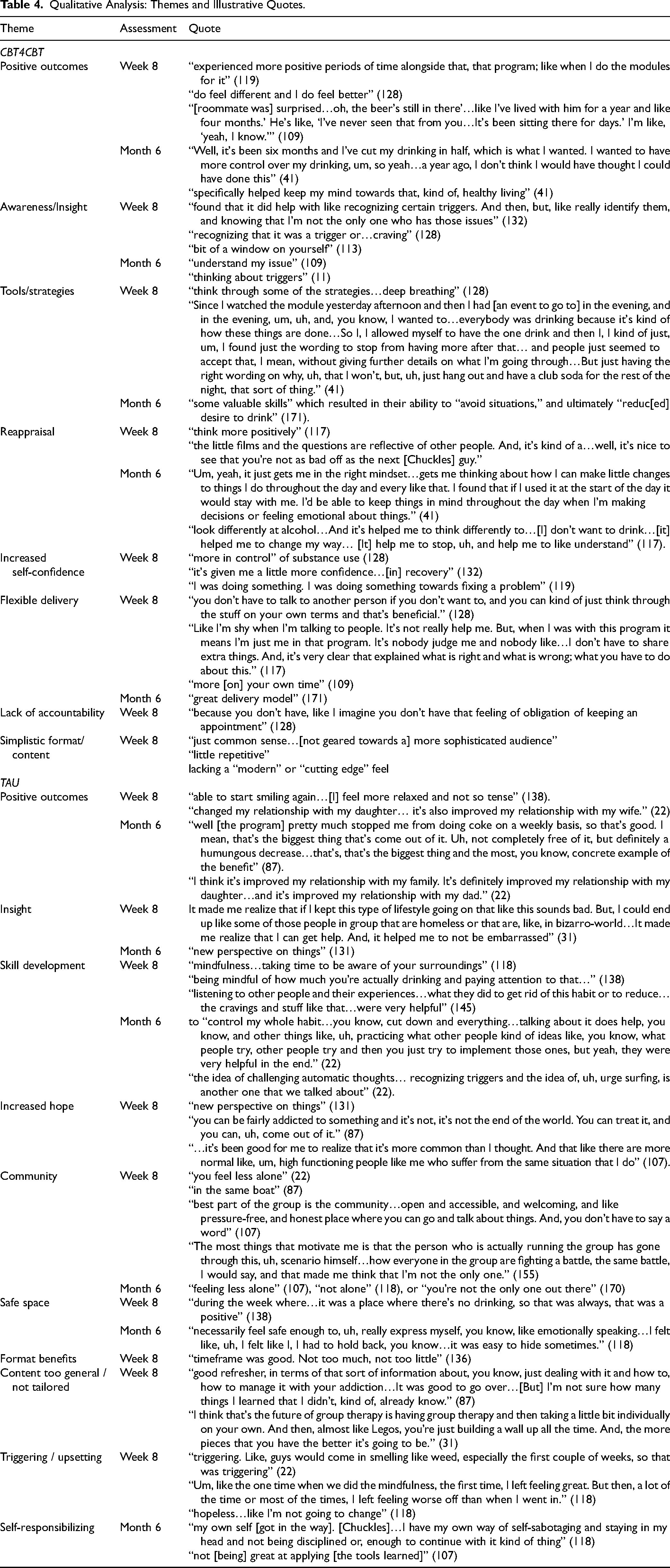
Participants who received CBT4CBT reported “small but positive” (128) and larger benefits from the intervention. Benefits included increased awareness and insight regarding triggers and cravings, and learning tools or strategies to meet substance use goals such as deep breathing and refusal skills. For example, CBT4CBT allowed many participants to recognize triggers and “choose something else to do,” facilitating healthier choices, and reducing harm associated with substance use – “like notice why I was going to drink, and remind me that I have an option to do something else” (141).
Participants reported that CBT4CBT videos supported skill development and cognitive reappraisal, helped them feel more confident, and know they are not alone in their struggles. The program's flexible format provided greater clarity: “I try one more CBT group actually with people; like with 10 people sitting. And uh, and like two workers … for me it doesn’t work. It's a lot of opinions. A lot of different, uh, experiences. And, it's a big mix for me in my head” (117). This format was also helpful for those with concerns about judgment from others.
Indeed, some described the program as a “brilliant delivery model … I think the convenience of delivery, the privacy of delivery to certain people. Like, I mean that's a big deal for me” (171). Others described that once they got used to the online format, “[it] actually did help…I felt it, it worked pretty good. It didn’t like fully stop me from drinking. But, it gave me ideas and ways to cope, and ways to look at things from a perspective that I didn’t really look at” (109). Furthermore, while some participants were “firm believer[s] in that….one-on-one…would work even better,” the online program met many participants where they were at and was a good “fit” for many (109).
While some participants described the online format as very positive due to how simple it was to use and its ability to reduce barriers, some participants described program format as a “blessing and a curse” (128) as they found it challenging to keep themselves accountable. Importantly, some participants were critical of the program for being “pretty simplistic” (113), a “little repetitive” (128), and thus less impactful – “I’ll say this again for the record, that like I think that it would be impactful for a lot of people. Uh, for myself I don’t think it's impacted me” (132).
Many of the benefits at Week 8 were still present at the Month 6 mark, such as tools to support better choices: “But, I think the value is that it took it to the front of mind, um, and reminded me of things that I maybe just wouldn’t have been thinking of … it helped me think” (119). Other participants described the maintenance of insight and skill development at Month 6, which resulted in behavioural change and decreased craving. Overall, many participants described that CBT4CBT “sticks with me” (132), ranging from descriptions of a profound effect – “…on the whole it was really useful for me” (125) – to a “change [in] my attitude towards mental health” (132) to, at the very least, being a “step” in the right direction – “a great starter” (109). For those who did not find the program useful at Month 6, a positive outcome was realizing what does work for them. [For a description of the qualitative results for TAU, please see Supplemental Results: TAU Qualitative Description.]
Discussion
The present study extends the literature by examining the effects of CBT4CBT versus TAU in a sample of diverse treatment-seeking individuals with SUDs. We examined not only quantitative outcomes of substance use and health, but also adopted a qualitative and economic evaluation lens to understand the impacts of CBT4CBT in a Canadian context. Findings regarding the number of days an individual's primary substance was used showed improvement for both groups; contrary to hypotheses, however, there were no differences in improvement across study groups. This contrasts with previous research examining CBT4CBT as a stand-alone compared to individual CBT and TAU, in which both CBT4CBT and individual CBT were associated with greater reduction in the frequency of substance use than TAU. 9 Notably, a main group effect was also exhibited for the primary outcome, suggesting that individuals from TAU had fewer days used compared to CBT4CBT. No other group effects were observed for SUD or mental health outcomes, suggesting that this difference was specifically related to use rather than harms or consequences related to use. Consistent with hypotheses, CBT4CBT was associated with lower healthcare use related to counselling in a subsample analysis. The economic evaluation suggested that CBT4CBT was associated with lower healthcare costs; however, higher substance use days in this group suggested that this cost reduction could be linked to reduced outcomes.
There were also no significant interactions of group and time observed in our secondary outcomes. Participants in both CBT4CBT and TAU exhibited improvements in the number of SUD symptoms endorsed, global severity of psychological symptoms, and psychological quality of life from pre-treatment to post-treatment. These results also differ from other studies of CBT4CBT as a stand-alone treatment versus standard care,8,9 which may suggest that differences across treatment conditions might vary across geographical regions and patient populations. However, evaluating other outcomes would be valuable.32,33
Exploring the impact of CBT4CBT from a qualitative perspective provides important insights into this digital intervention's potential. This qualitative analysis complements what the efficacy analysis and economics evaluation reported and brings to the fore what might have been left in abeyance in the quantitative analysis, mainly, how participants construct their social world 34 in relation to their participation in this study. As Hills argues, “Qualitative methods provide the means by which to explore and explain people's experiences in ways that cannot be captured by quantitative methods or reported by statistical data.” 35 Future research may extend this important analysis; for example, a discourse analysis may provide insights into participants’ language use and contribute to refining the CBT4CBT intervention.
Limitations: The recommended economic evaluation by CADTH is a cost-utility analysis; given the lack of utilities for the WHOQoL-BREF, undertaking a cost-utility analysis was not possible. Furthermore, the subsample used to undertake the cost-effectiveness analysis was small; this and overall group differences may have implications for the interpretation and generalizability of the findings. Additionally, the current sample size was less than anticipated due to the COVID-19 pandemic, which also impacted power and generalizability of efficacy analyses. Notably, qualitative research does not aim to be generalizable per se; rather, the aim is to shed light on participant's lived-experiences. With that said, qualitative findings are typically transferable to other contexts. 36 Finally, attrition over the follow-up was high, which may have biased estimates. The heterogeneity and complexity of the sample, and more accurate effect size estimates and power calculations, are critical considerations for future research.
Conclusions
CBT4CBT has demonstrated promise in improving access to treatment for those struggling with substance use. Although this investigation found that participants receiving CBT4CBT improved over acute treatment and longer-term follow-up on the primary and some secondary outcomes, they did not differ from those who received standard care. These results cannot be interpreted as support of equivalence between these treatments, however, as target accruals were not met due to the COVID-19 pandemic. Yet, the economic analysis supported that participants who received CBT4CBT had fewer healthcare costs than those who received TAU, and qualitative analyses identified areas of strength and growth for this digital health resource. Data from this investigation can inform continued evaluation and implementation of this program, incorporating unique and key information, including local estimates of clinical outcomes and costs and patient perspectives of treatment format and content. The current investigation is thus a crucial step to realizing this innovation in clinical care to innovation in clinical practice.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437241255100 - Supplemental material for Computer-Based Training for Cognitive Behavioural Therapy for Substance Use Disorder: A Randomized Controlled Trial Including Quantitative and Qualitative Health and Economic Outcomes: Formation informatisée pour la thérapie cognitivo-comportementale pour les troubles liés à l'usage de substances : un essai randomisé contrôlé y compris les résultats quantitatifs et qualitatifs en matière de santé et d’économie
Supplemental material, sj-docx-1-cpa-10.1177_07067437241255100 for Computer-Based Training for Cognitive Behavioural Therapy for Substance Use Disorder: A Randomized Controlled Trial Including Quantitative and Qualitative Health and Economic Outcomes: Formation informatisée pour la thérapie cognitivo-comportementale pour les troubles liés à l'usage de substances : un essai randomisé contrôlé y compris les résultats quantitatifs et qualitatifs en matière de santé et d’économie by Alina Patel, Michael Corman, Claire de Oliveira, Joyce Mason, Nibene Somé, Danielle Downie, Esha Jain, Michelle Patterson, John A. Cunningham, Tony P. George, Bernard Le Foll and Lena C. Quilty in The Canadian Journal of Psychiatry
Supplemental Material
sj-doc-2-cpa-10.1177_07067437241255100 - Supplemental material for Computer-Based Training for Cognitive Behavioural Therapy for Substance Use Disorder: A Randomized Controlled Trial Including Quantitative and Qualitative Health and Economic Outcomes: Formation informatisée pour la thérapie cognitivo-comportementale pour les troubles liés à l'usage de substances : un essai randomisé contrôlé y compris les résultats quantitatifs et qualitatifs en matière de santé et d’économie
Supplemental material, sj-doc-2-cpa-10.1177_07067437241255100 for Computer-Based Training for Cognitive Behavioural Therapy for Substance Use Disorder: A Randomized Controlled Trial Including Quantitative and Qualitative Health and Economic Outcomes: Formation informatisée pour la thérapie cognitivo-comportementale pour les troubles liés à l'usage de substances : un essai randomisé contrôlé y compris les résultats quantitatifs et qualitatifs en matière de santé et d’économie by Alina Patel, Michael Corman, Claire de Oliveira, Joyce Mason, Nibene Somé, Danielle Downie, Esha Jain, Michelle Patterson, John A. Cunningham, Tony P. George, Bernard Le Foll and Lena C. Quilty in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
We would like to thank Dr. Kathleen Carroll, who was Co-Principal Investigator of this seed grant and contributed substantially to project design; her inspiration and guidance cannot be overstated. We would also like to thank all participants for sharing their insights and experiences with us.
Abbreviations
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MC, CdO, MP, JC, TG, BL, KMC, LCQ were awarded a Centre for Addiction and Mental Health (CAMH) Foundation Discovery Fund Seed Grant for this project. BL is supported by CAMH, Waypoint Centre for Mental Health Care, a clinician-scientist award from the Department of Family and Community Medicine of the University of Toronto, and an Addiction Psychiatry Chair from the Department of Psychiatry of the University of Toronto. TPG is Co-Principal Editor of Neuropsychopharmacology (NPP), the Official Journal of the American College of Neuropsychopharmacology (ACNP). All other authors disclose no relevant conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the CAMH Foundation Discovery Fund. This funding agency was not involved in study design, analyses, results or conclusions.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.