
Abstract
Objective
Depression in later life is associated with a two-fold increased risk of dementia. It is not clear to what extent potentially modifiable risk factors account for this association.
Method
Older adults (age 50 + ) with objective health measures (n = 14,014) from the Canadian Longitudinal Study on Aging were followed for a mean duration of 35 months. Linear regression analyses were used to determine if clinically significant depression (Centre for Epidemiologic Studies Depression scale score (CESD) ≥ 10) was associated with global cognitive decline, assessed with a neuropsychological battery during follow-up, and if modifiable risk factors mediated this association.
Results
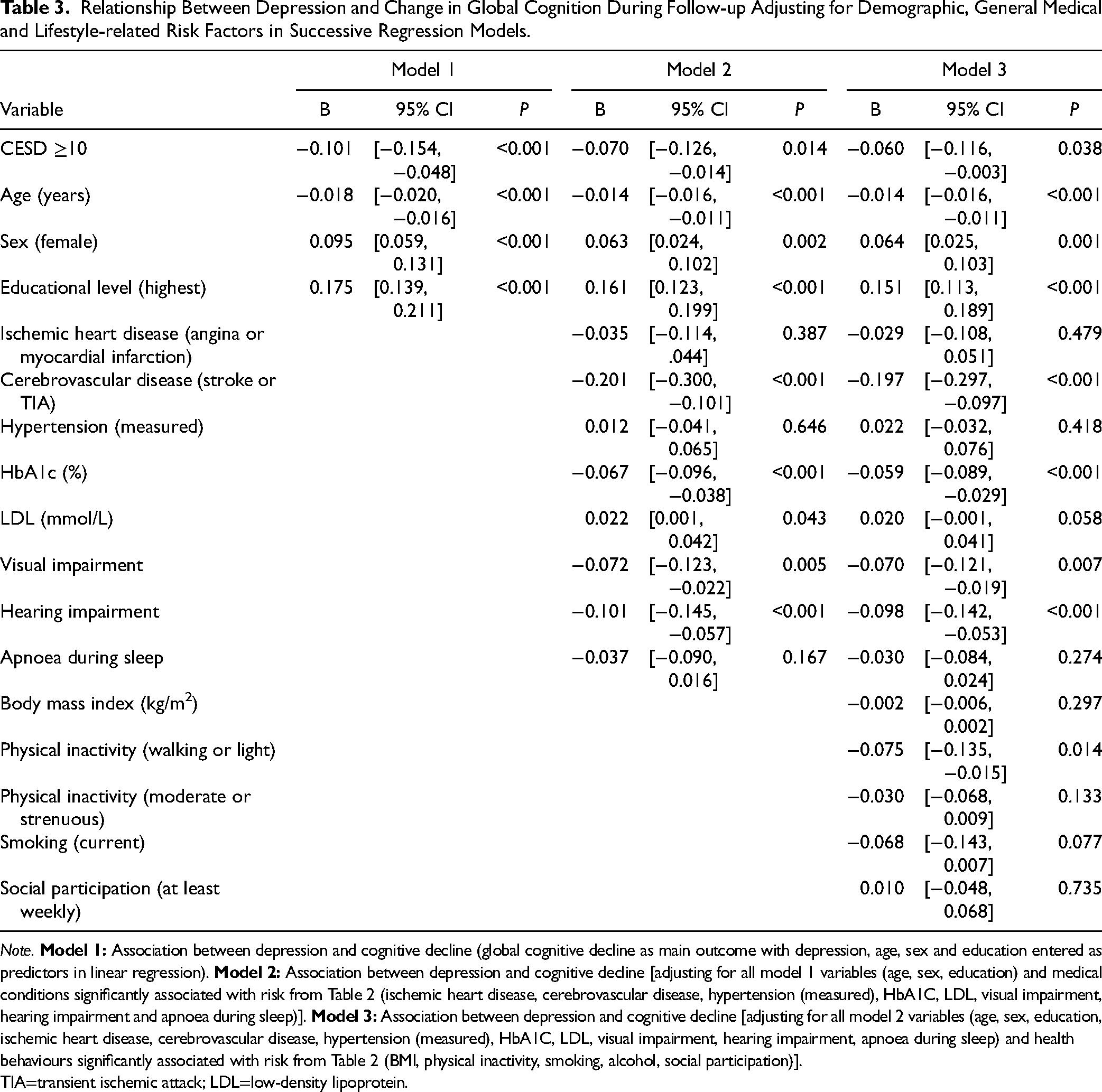
Depression was associated with an excess of risk factors for cognitive decline including: vascular disease, hypertension, diabetes, apnoea during sleep, higher body mass index, smoking, physical inactivity and lack of social participation. In regression analyses depression remained independently associated with cognitive decline over time (beta −0.060, P = 0.038) as did cerebrovascular disease (beta −0.197, P < 0.001), HbA1C (beta −0.059, P < 0.001), visual impairment (beta −0.070, P = 0.007), hearing impairment (beta −0.098, P < 0.001) and physical inactivity (beta −0.075, P = 0.014). In mediation analyses, we found that cerebrovascular disease (z = −3.525, P < 0.001), HbA1C (z = −4.976, P < 0.001) and physical inactivity (z = −3.998, P < 0.001) partially mediated the association between depression and cognitive decline.
Conclusions
In this large sample of Canadian older adults incorporating several objective health measures, older adults with depression were at increased risk of cognitive decline and had an excess of potentially modifiable risk factors. Clinicians should pay particular attention to control of diabetes, physical inactivity and risk factors for cerebrovascular disease in older adults presenting with depression as they can contribute to accelerated cognitive decline and may be addressed during routine clinical care.
Keywords
Introduction
Older adults with depression have a two-fold increased risk of dementia. A previous meta-analysis of 23 community based prospective cohort studies concluded that late life depression is associated with an approximate two-fold increased risk of Alzheimer's dementia and vascular dementia. 1 Clinically significant depression has a point prevalence of approximately 10% in community dwelling older adults representing one of the most common health disorders in later life. 2
The mechanisms that underpin the relationship between depression and increased risk of dementia remain incompletely understood. Depression has been associated with several vascular risk factors but has also been found to be a risk factor for cardiovascular disease, independently of these associations. 3 However, it remains unclear to what extent modifiable variables such as physical inactivity, hypertension and diabetes may mediate the association between depression and cognitive decline. While previous analyses have explored these relationships, many have relied on self-reported diagnosis of medical conditions rather than objective measures or have examined a limited number of risk factors in small study samples. 4 Reliance upon self-reported medical diagnoses potentially underestimates the prevalence of modifiable risk factors as depression has been associated with underdiagnosis and inadequate treatment of common conditions such as hypertension and diabetes.5,6
In an encouraging analysis, synthesizing data from several longitudinal population studies, the Lancet Commission on Prevention in Dementia concluded that 12 modifiable risk factors account for approximately 40% of cases of dementia worldwide which could theoretically be prevented or delayed. 7 Modifiable risk factors listed included: less education in early life, midlife hypertension, obesity, excessive alcohol intake, hearing loss, traumatic brain injury (TBI), late life smoking, depression, social isolation, physical inactivity, diabetes and air pollution. They acknowledge that these risk factors may be co-morbid or overlapping in many instances and have variable distribution among at risk groups. Older adults with depression are one such high risk group and no analysis to date using objective health measures (physical examination with blood testing) and incorporating a broad range of potentially modifiable risk factors has determined which risk factors are most relevant among older Canadians with depression. If we are to successfully reduce the high incidence of dementia among older adults with depression, increased understanding of potentially modifiable risk factors linking depression with cognitive decline will facilitate design of interventional strategies for those at greatest risk and will inform improved clinical care for older adults at risk of cognitive and functional decline.
We undertook a longitudinal analysis in a large dataset of community dwelling older adults incorporating a broad range of both objective and subjective health measures. We hypothesized that clinically significant depression would be associated with cognitive decline during follow-up and that depression would be associated with an excess of both self-reported and objectively measured modifiable risk factors for cognitive decline. We further hypothesized that potentially modifiable vascular risk factors such as physical inactivity, higher body mass index, having undertreated blood pressure or poorly controlled diabetes would partially mediate the association and present a therapeutic opportunity to reduce cognitive decline in this vulnerable population.
Methods
Sample
We used data from the Canadian Longitudinal Study on Aging Comprehensive cohort (baseline 2012–2015 and 3-year follow-up 2015–2018). The comprehensive cohort (n = 30,097) included community-dwelling individuals, aged 45–85 years, who were randomly selected from within a 25 to 50 km radius of 11 data collection sites in seven provinces across Canada using provincial health care registration databases and random digit dialling of landline telephones. 8 Data collection sites were located in small, medium and large cities, and several included large rural catchment areas. Individuals living in long-term care institutions or with cognitive impairment at baseline were excluded. Participants provided data through a computer-assisted in-person home interview. Additional questionnaires, tests, physical measurements and a blood test were collected at the data collection site. To participate in the comprehensive cohort, participants had to complete an in-home interview and visit a data collection site at baseline but provision of biological specimens was optional. Further details about study design and data collection have previously been published. 8 In this analysis, we included participants from the comprehensive cohort who (1) were age 50 + as we were primarily interested in older adults at risk of cognitive decline and wished to be consistent with similar longitudinal studies, (2) had completed the Centre for Epidemiologic Studies Depression Scale 10-item short form (CESD-10), (3) did not report that a doctor had previously diagnosed them with dementia or Alzheimer's disease at baseline, (4) had reported and objective measures of diabetes and hypertension (blood test and blood pressure measurement at baseline), and (5) had comprehensive neuropsychological testing available at baseline and follow-up. The research ethics board of Sunnybrook Health Sciences Centre provided approval for this analysis (project identification number 5663).
Measures
Sociodemographic data including age, sex and education were collected as part of a structured interview. Data regarding educational level was collected and dichotomized according to attainment of a bachelor's degree or above versus lower than a bachelor's degree.
Depression
Depressive symptoms were measured using the CESD-10 and a cut off of ≥ 10 was used to determine clinical significance in accordance with previous validation studies. 9
Chronic Medical Conditions
Study participants reported medical conditions previously diagnosed by a physician according to a structured interview. Objective measurement of blood pressure and a blood test were also used to help determine diagnoses of hypertension or diabetes. Previous diagnosis of hypertension or diabetes was confirmed if a participant reported that a doctor had previously diagnosed them with the condition or if the study participant reported taking a medication for blood pressure or diabetes. An objectively determined diagnosis of hypertension/blood pressure was based on repeated measurement of blood pressure (average systolic ≥ 140 or average diastolic ≥ 90 mmHg using an average of six readings with VSM BpTRU machine). Diabetes diagnosis was determined if HbA1C was ≥ 6.5%. Total low-density lipoprotein and trigycerides were also measured. Undiagnosed hypertension or diabetes was determined to be present when there was no reported diagnosis or medication for the condition, yet direct measurement demonstrated either raised blood pressure or raised HbA1C. History of cardiovascular disease was determined by reported history of either myocardial infarction or angina and cerebrovascular disease by reported history of either stroke or transient ischemic attack. The interview included a question regarding whether anyone had observed the study participant stop breathing during sleep. This was used as a possible surrogate marker for obstructive sleep apnoea which often co-occurs with depression in later life and is a risk factor for cognitive decline. 10
Sensory Loss
Using the standard Early Treatment Diabetic Retinopathy Study chart, 11 pinhole-corrected visual acuity (VA) was measured in both left and right eyes. If VA measurements for both eyes were available, the VA measurement from the better eye was used to determine visual impairment (defined as <0.3 logMAR) as per the World Health Organization (WHO). 12 The Tremetrics RA 300 + Digital Screening Audiometer was used to measure the pure-tone average (PTA) at 500, 1000, 2000, and 4000 Hz in each ear. If PTA measurements for both ears were available, the PTA measurement from the better ear was used to determine hearing impairment (defined as <26 dB) in accordance with WHO guidelines. 13 CLSA defined a positive screen for TBI as (1) having suffered a head injury from an accident (e.g., vehicular crash, fall, sport-related activity) and (2) that the head injury resulted in the individual being dazed, confused, “seeing stars,” not remembering the injury, or losing consciousness.
Physical Activity
This was assessed using a modified Physical Activity Scale for the Elderly (PASE). 14 Participants were asked whether they had engaged in either walking, light, moderate or strenuous sports or recreational activities during the past seven days. Walking and light activities were defined as those during which minimal effort was required, moderate activities were defined as those during which there was a moderate increase in breathing, while strenuous activities were defined as those during which it would be very difficult to hold a conversation. Reponses were categorized according to any engagement, within the past seven days, in walking outside or light sports/recreational activities. Participants were also asked if they had engaged in moderate or strenuous sports/recreational activities within the past seven days. Participants were dichotomized according to participation in (1) moderate or strenuous physical activity in the past week versus none, and (2) participation in light physical activity or walking outside in the past week versus none.
Smoking, Alcohol Intake & Social Participation
Participants were dichotomized based on smoking status (currently smoking versus never or in the past), and regular alcohol consumption over the past year (an alcohol intake of six or more drinks per week versus less than that per week). Social participation was defined as at least weekly participation in any community based social activity within the previous 12 months versus less than that.
Cognition
A comprehensive neuropsychological battery was conducted at baseline and follow-up and has previously been described in detail. 15 A summary of six tests scores was used to derive an index of global cognition that included memory and executive domains. Memory was assessed with a modified Rey Auditory Verbal Learning Test (REY) 16 (REYI measuring immediate memory recall; REYII measuring delayed recall). Tests of executive cognitive function included: Animal Fluency (AF) 17 measuring generative category verbal fluency, the Mental Alternation Test (MAT) 18 measuring speeded alternation of ascending letters and numbers, FAS 19 measuring generative phonemic fluency for the letters F, A and S (three scores summed to give a derived FAS total score), Stroop neurological screening test20,21 scores for speeded naming of coloured dots, speeded reading of words, and speeded naming of text colour of incongruently coloured words. Normed scores for each test were created adjusting for age, sex and education level. 15 Normed scores were expressed as standardized Z scores (number of standard deviations from the mean) and composite global cognition subscores were calculated from normed Z scores at baseline and follow-up. The main outcome of interest was change in Z score between baseline and follow-up.
Statistical Analyses
Descriptive analyses were initially conducted comparing frequency of sociodemographic and clinical characteristics between participants with and without clinically significant depression (CESD ≥ 10) at baseline. Continuous measures such as age were summarized using means and standard deviations whereas categorical measures were summarized using counts and percentages. We then conducted bivariate linear regression analyses with change in global cognition Z score between baseline and follow-up as the outcome variable to determine which variables were significantly associated with cognitive decline during follow-up. In further multivariable regression models we determined if clinically significant depression was associated with cognition at follow-up independently of other fixed and potentially modifiable risk factors associated with cognitive decline. In multivariable regression models we entered fixed sociodemographic variables, then clinical variables and finally lifestyle-related variables stepwise into the model in blocks to determine which potentially modifiable variables would remain independently associated with cognitive decline following adjustment for all other variables. In circumstances where there were both self-reported and objective measures for the same variable (e.g., hypertension, diabetes), we included the objective measure (e.g., measured blood pressure, HbA1C) to ensure undiagnosed cases were included. Multivariable models were checked for multicollinearity to ensure stability of models with all tolerance values ≥0.4. We then conducted mediation analyses to determine if risk factors independently associated with cognitive decline also partially mediated the observed association between depression and cognitive decline. Mediation is a hypothesized causal chain in which the first or predictor variable affects a second or mediating variable that, in turn, affects a third variable. The mediating variable may, either completely or partially, explain the association between the first variable (in this case depressive symptoms) and the third variable (cognitive decline). We tested for mediation using the method described by Baron and Kenny 22 in which it should first be demonstrated the predictor variable is significantly associated with the proposed mediating variable and both mediating and predictor variables must be significantly associated with the outcome. The coefficients for the mediation analyses were calculated with bivariate regressions in SPSS, and the significance of the mediated effects was assessed using the Sobel test. 23 All analyses were conducted with SPSS version 28. 24
Results
In total 14,014, study participants met inclusion criteria and were followed for a mean duration of 35 (±3.5) months. Participants had a mean age of 63.5 (±9), 49.3% were female and 47.6% had bachelor's degree or above. Demographic and clinical characteristics of study participants with and without clinically significant depression at baseline are outlined in Table 1. Older adults with depression had an excess of several risk factors significantly associated with cognitive decline including: ischemic heart disease, cerebrovascular disease, hypertension, diabetes, apnoea during sleep, higher body mass index, smoking, physical inactivity and lack of social participation. In unadjusted bivariate regression analyses with decline in global cognition over time as the main outcome, a number of sociodemographic, clinical and lifestyle-related risk factors were significantly associated with cognitive decline (Table 2).
Distribution of Sociodemographic, Clinical and Behavioural Characteristics Between Those With and Without Clinically Significant Depression (CESD ≥10) at Baseline.

Note. Diagnosis: self-reported clinical diagnosis or medication use for condition; measured: confirmed by objective measurement; undiagnosed: measured but no reported diagnosis or medication use for condition. TIA=transient ischemic attack; LDL=low-density lipoprotein.
Relationship Between Each Risk Factor and Change in Global Cognition During Follow-up in Unadjusted Bivariate Regression Analyses.

Note. TIA=transient ischemic attack; LDL=low-density lipoprotein.
* P-values that remain significant following application of stricter Bonferroni corrected P < 0.002.
Results from stepwise multivariable regression models to determine which modifiable variables remained independently associated with cognitive decline following adjustment for all other variables are presented in Table 3. In a final fully adjusted model, the following potentially modifiable variables remained independently associated with cognitive decline: depression, cerebrovascular disease, HbA1C, visual impairment, hearing impairment and physical inactivity (Table 3).
Relationship Between Depression and Change in Global Cognition During Follow-up Adjusting for Demographic, General Medical and Lifestyle-related Risk Factors in Successive Regression Models.
Note.
TIA=transient ischemic attack; LDL=low-density lipoprotein.
Finally, we conducted mediation analyses to determine if any of the variables independently associated with cognitive decline from Table 3 also partially mediated the association between depression and cognitive decline. We found that cerebrovascular disease (z = −3.525, P < 0.001), HbA1C (z = −4.976, P < 0.001) and physical inactivity (z = −3.998, P < 0.001) significantly partially mediated the association between depression and cognitive decline.
Discussion
In this large community dwelling sample of older adults, we found that several potentially modifiable risk factors including vascular risks (physical inactivity, HbA1C, history of cerebrovascular disease) and sensory loss (visual and hearing impairment) were independently associated with increased risk of cognitive decline. The association between vascular risks and cognitive decline is consistent with previous analyses and the association between sensory impairment and cognitive decline is also consistent with more recent analyses that have highlighted the importance of addressing visual and hearing loss to help prevent cognitive decline. 25 In addition, we found that depression was independently associated with increased risk of cognitive decline and this subgroup displayed an excess of several risk factors related to cognitive decline including medical (vascular disease, hypertension, diabetes, apnoea during sleep) and lifestyle-related (higher body mass index, smoking, physical inactivity, lack of social participation) risk factors. In multivariable stepwise regression analyses the strength of the association between depression and cognitive decline weakened but remained significant following adjustment for other risk factors. In mediation analyses we found that physical inactivity, HbA1C and cerebrovascular disease significantly partially mediated the relationship between depression and cognitive decline. Physical inactivity and poor control of diabetes have previously been associated with increased risk of cerebrovascular and Alzheimer's disease and are amenable to modification. 26
The association between depression and increased risk of cognitive decline has been described in previous analyses but there is less clarity regarding mechanisms and potential avenues for therapeutic intervention to reduce this risk. 1 It has been proposed that depression may behave as a true risk factor for cognitive decline (either directly via physiological changes associated with depression such as inflammatory activation and hypercortisolemia) or indirectly via associated medical comorbidities (hypertension, diabetes) and lifestyle-related risk factors (physical inactivity, smoking). 27 Previous longitudinal analyses conducted over decades have indicated a dose-related relationship between severity and frequency of depressive episodes with increased risk of dementia.28–30 There is also evidence that depression has a bi-directional relationship with cerebrovascular disease/beta-amyloid pathology and may frequently occur as part of prodrome of degenerative disease. This observation is supported by studies indicating a stronger relationship between depression and new onset dementia or cognitive impairment among those with recently active or late onset depression.31–33 These pathways are not necessarily mutually exclusive and may overlap or operate to varying degrees among different patient groups depending upon pattern of medical co-morbidities and personal history of depression. One interpretation of previously reported findings is that those who report a remote episode of depression, without persistent or recurrent symptoms are likely at the lowest level of depression-related risk while those with persistent recurrent, recently active or late onset depression are at greater risk. In this analysis we found supportive evidence for a relationship between depression and accelerated cognitive decline secondary to a number of common and potentially modifiable risk factors (HbA1C, physical inactivity). While these risk factors are of importance in the general population, our findings indicate that they are of particular relevance among older adults with depression where they occur more frequently and partially mediate the relationship between depression and increased risk of cognitive decline. We also note that depression remains independently associated with cognitive decline even following adjustment for all the risk factors listed here. This may be due to physiologic changes associated with the depressive state itself (hypercortisolemia, inflammatory activation and decreased trophic factors), other associated risk factors not accounted for here or may represent reverse causality with depression occurring as part of the behavioural prodrome of degenerative disease as discussed above. Findings from interventional studies do indicate partial improvement in cognitive test scores following treatment of depression with greater risk of cognitive decline attached to those with persistent symptoms.29,34 These findings support the importance of adequately treating depression itself to maintain both quality of life and improved functioning over the longer term.
In recognition of the variable distribution of common risk factors for cognitive decline among different patient groups, several studies have recently tested the utility of multicomponent interventions, tailored according to individual risk profiles, to reduce risk of cognitive decline. Those studies have generally focused upon some combination of vascular risk factor treatment, dietary change, cognitive stimulation or physical exercise to delay cognitive decline and have demonstrated some success in reducing cognitive decline among high-risk groups. 35 More recently, a European task force on brain health services has proposed that memory clinics and brain health services of the future should incorporate a greater focus upon risk factor reduction and that these interventions should be tailored according to the individual needs and risk profile of the patient. 36 Older adults with depression are one such high risk group and our findings support the need for an increased focus on treatment of common modifiable vascular risk factors in tandem with optimal treatment of depression to reduce risk of cognitive and functional decline over time.
This longitudinal analysis has a number of strengths and limitations. Strengths include the use of several objective health measures in a large population sample allowing for the assessment of multiple risk factors at once to determine which are most relevant to increased risk. We note that the findings here are observational in nature only, so causality cannot be definitively determined. In addition, not all measures were objective and there is potential for recall bias with self-reported measures or potential for loss of precision where measures were dichotomous rather than continuous. Although a large number of risk factors were examined, we note that other risk factors such as diet, isolation, loneliness, number and severity of past depressive episodes or measures of cognitive activity were not included. Participants in this study did not undergo subtyping to determine aetiology or clinical significance of cognitive decline and so it is possible that risk factors listed here may be differentially associated with decline in different cognitive domains associated with that aetiology. In addition, the sample under study represents a subsample of the larger CLSA cohort who attended data collection centres for examination and further testing. This subset of study participants has been found to have a generally higher level of education and better self-rated health than those who participated in the overall study. 8 Finally, we note that a proportion of participants were lost to follow-up or did not have follow-up data available potentially underestimating cognitive decline if those with more significant cognitive decline could not participate in follow-up assessments.
In conclusion, in this large sample of Canadian older adults incorporating several objective health measures we found that older adults with depression are at increased risk of cognitive decline over time and have several potentially modifiable risk factors that partially explain this association. Clinicians should pay particular attention to control of diabetes, physical inactivity and risk factors for cerebrovascular disease in older adults presenting with depression as they can contribute to accelerated cognitive decline and may be addressed during routine clinical care.
Footnotes
Acknowledgments
This research was made possible using the data/biospecimens collected by the Canadian Longitudinal Study on Aging (CLSA). Funding for the Canadian Longitudinal Study on Aging (CLSA) is provided by the Government of Canada through the Canadian Institutes of Health Research (CIHR) under grant reference: LSA 94473 and the Canada Foundation for Innovation, as well as the following provinces, Newfoundland, Nova Scotia, Quebec, Ontario, Manitoba, Alberta, and British Columbia. This analysis was supported by funding from Sunnybrook Health Sciences Centre Foundation and an academic scholars award from Sunnyrbook Health Science Centre. This research has been conducted using the CLSA dataset Baseline Comprehensive version 7.0 and Follow-up 1 Comprehensive version 5.0, under Application Number 2206001. The CLSA is led by Drs. Parminder Raina, Christina Wolfson and Susan Kirkland.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research, Sunnybrook Health Sciences Centre Foundation, Canada Foundation for Innovation (grant number LSA 94473).