
Abstract

Keywords
The Canadian Network for Mood and Anxiety Treatments (CANMAT) guidelines remain one of the eminent guidelines influencing clinical care worldwide, and these revisions thoughtfully update the literature influencing clinical care. 1 The guideline effectively uses gradation of evidence that conveys to the reader the level of evidence for each intervention at various stages of treatment. This strength of evidence-based taxonomy provides the practitioner with a simple metric to weigh recommendations. One of the major changes in these updated guidelines reflects the increasing prioritization of patient experience and needs in designing care, with these new guidelines focusing much more on personalized care for individuals with major depressive disorder, considering their unique needs and preferences. This aligns with the notion of shared decision-making, which facilitates psychoeducation, reinforces the therapeutic alliance, promotes autonomy, and hence has increased prominence in these guidelines.
It is understood that the likelihood of response to depression treatment declines with each sequential treatment step. The STAR-D study found that remission rates for participants after four treatment steps were 67%. However, several recent papers have provided renewed optimism. Firstly, Harris and colleagues, using data from the world mental health surveys, showed that 93.9% of those who persisted through 10 treatment professionals found significant benefits (with the caveat that only 21.5% persisted). 2 And a re-analysis of the STAR-D study by Furukawa and colleagues, accounting for the substantial group of people enrolled in that study who already had received treatment and accounting for dropouts, found a more optimistic overall response rate than was originally reported. The cumulative remission rate was 87.5% a year after the initiation of treatment. 3 In sum, persistence seems to be the key to depression treatment, especially for those with difficult-to-treat profiles, as with many other domains of life. As such, rather more optimistic messaging appears to be evidence-based.
In this context, tricyclic antidepressants and especially monoamine oxidase inhibitors, which are rarely used in routine practice, remain valuable and neglected elements in the therapeutic armamentarium. While correctly listed as a third line due to tolerability concerns, they are not a third line in horsepower, and they retain valuable utility in people not benefitting from other alternatives and could be used more widely in such circumstances—the motivational text box in the guideline paper supports this. The same applies to lithium, which is valuable in many individuals with recurrent unipolar depression but rarely used in practice. Lack of clinician experience with these agents is a self-reinforcing barrier to use and, like clozapine for schizophrenia, these agents should be used far more widely in people who have not responded to other alternatives. The role of neuromodulation such as electroconvulsive therapy or transcranial magnetic stimulation appears early in the algorithm and these are recommended to be considered after one of the switch or adjunctive medication options. This is always hard to generalize, and there are scenarios for example of severely ill, psychotic and/or suicidal people where such placement might be appropriate, but for more routine cases this might be considered early.
Depression is acknowledged as a highly heterogeneous phenotype, and together with an equally heterogeneous and large menu of potential therapies, it is very difficult to assign treatment priorities or sequences according to Diagnostic and Statistical Manual (DSM) categories alone. In theory, at least, a plethora of pharmacotherapies, psychotherapies, lifestyle, nutraceutical interventions, and neurostimulation modalities are effective, with a microtome difference in effect sizes separating the various trial data sources. This is a major challenge for guidelines. In practice, individuals with the same depression scale scores might be advised to take a selective serotonin reuptake inhibitor, engage in psychotherapy, or even commence trauma counselling or cease drinking. Notwithstanding the eloquent promise of biomarkers for precision psychiatry, the clinical larder of such approaches with sufficient practicality, sensitivity and specificity for clinical care remains bare. 4
Clinicians, however, have the advantage of using a clinical formulation that extends beyond differential and DSM/International Classification of Diseases diagnosis to determine the individual patient characteristics and variances in risk features, phenomenology, personal characteristics, life events, etc., to aid treatment selection. Formulation is arguably of particular importance in difficult-to-treat depression, where the likelihood of confounding variables of large effects such as psychosocial stressors is greater, and consequently where a linear algorithm from psychotherapy to medication to neurostimulation, ignoring such factors, would be less appropriate. It is very hard to operationalize this kind of individual formulation-based decision-making in clinical practice because of the sheer vastness and diversity of variables that are dominant in an individual's circumstances. However, it forms the backbone of insightful clinical care. Guidelines need to acknowledge this critical element of the art of decision-making complementing the science of guidance algorithms. Within this formulation framework, it is imperative that the social determinants of depression be integrated as these are often a key driver of mental ill health. A challenge is that randomized controlled trial data regarding psychosocial determinants and treatment pathways is lacking, limiting what guidelines can say in this regard. It should be noted that there has been a large increase in antidepressant prescriptions over the past four decades, without a commensurate decrease in the period prevalence of depression. 5 This reinforces the importance of holistic case formulation (which facilitates targeted multilevel interventions) rather than the reflexive prescription of antidepressants as monotherapy.
One of the major drivers of heterogeneity in the construct of depression is the presence of clinically significant personality and psychological schema issues. It is likely that in many systems of care, the presence and impact of personality are underestimated. It is indeed normative for the index presentation of personality disorders to be that of depression and anxiety symptoms, and checklist approaches run a high risk of misdiagnosing personality disorders as depression. This has several adverse clinical consequences including misaligned expectations of care and the risk of inappropriate pharmacological therapies. Indeed, these updates note that in people presenting with depression and comorbid personality disorders, response rates to antidepressants are poorer than for people without comorbid personality disorders, and psychotherapy approaches might be more effective in this specific population. In this regard, screening for depression remains a contentious issue with risks largely around false positives driven by other disorders such as personality disorders that may lead to the application of misaligned algorithms, from which the benefit is uncertain.
The other major change is the incorporation of lifestyle interventions such as exercise, light therapy, improved dietary habits, tobacco (and other substances) cessation, and sleep hygiene into treatment plans. This is broadly concordant with other recent guidelines such as the RANZCP guidelines, which now place lifestyle modification as a foundational element of care. Furthermore, other lifestyle interventions, such as activity scheduling, volunteering, yoga, or tai chi, might also be effective in selected populations. 6 Diet is given a third-line recommendation in these guidelines, based on only 1 identified trial. However, there are now several trials, and a 2019 meta-analysis of 15 clinical trials mostly in nonclinical populations, showing an aggregate positive effect on depressive symptoms with dietary interventions. 7 A more recent meta-analysis of clinical populations using a Mediterranean diet also showed beneficial effects. 8 The ketogenic dietary pattern is attracting significant interest, but data are to date inadequate to make any clinical recommendations. Nevertheless, based on potential utility for commonly comorbid medical conditions and the precautionary principle, lifestyle modification should arguably not be considered as an alternative step but rather as a normative practice alongside other therapies, providing a platform on which other therapies can be—potentially more successfully—employed. This integration can help reduce the high burden of depression and depression treatments in long-term general health outcomes. 9 Similarly, the guidelines acknowledge the benefit of the combination of biological and psychological therapies. Rather than seeing these as alternative or sequential steps, it might be clinically prudent, in some cases, to conceptualize 3 axes of treatment proceeding independently, biological, psychological, and lifestyle, with choices and weightings between these guided by clinical formulation (Figure 1). This is especially true in the maintenance phase and to improve long-term outcomes beyond the use of pharmacotherapy ad aeternum.
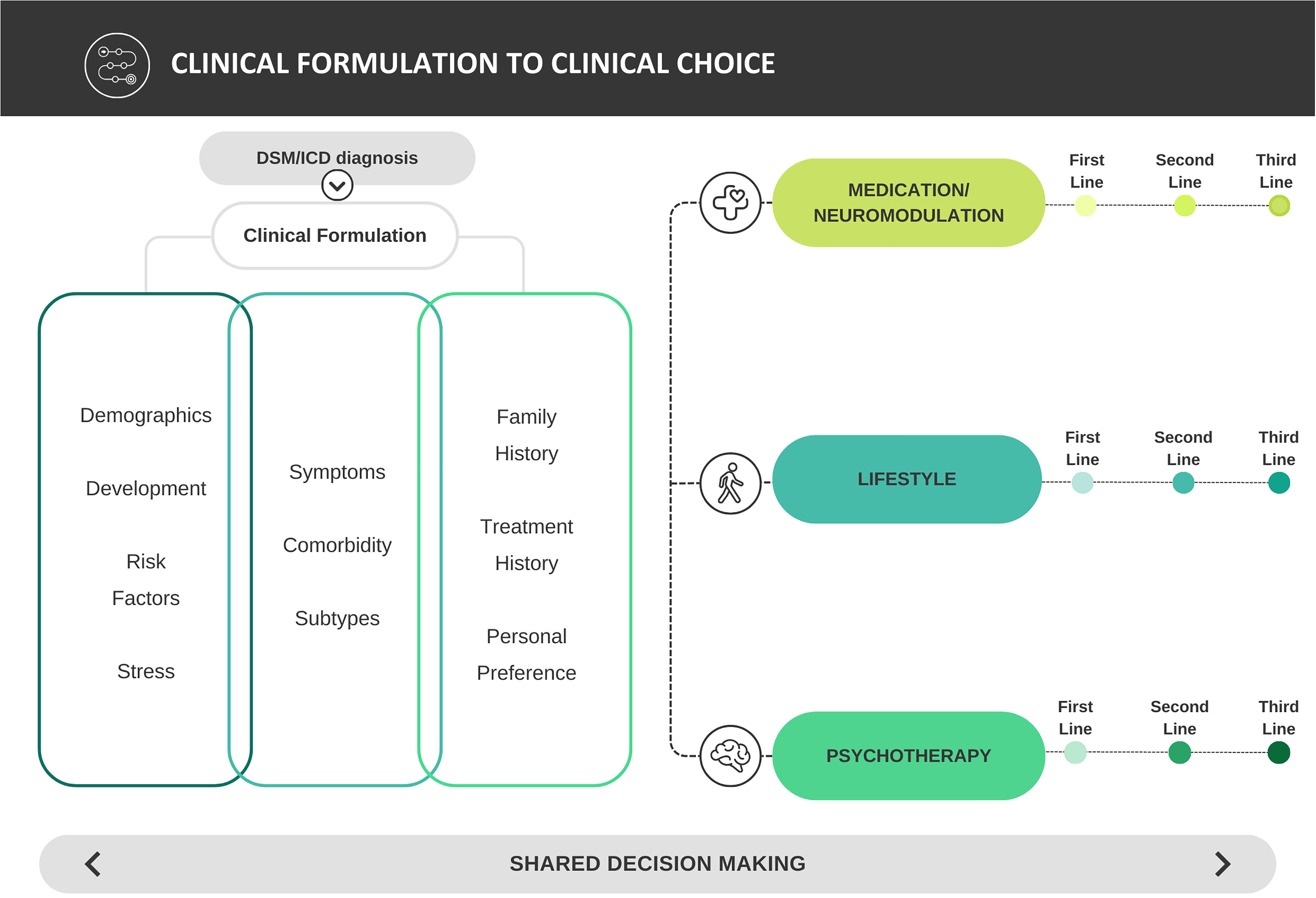
From formulation informed guidelines to clinical choice.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.