
Abstract
Objective
Racial/ethnic disparities in the prevalence of psychiatric disorders have been reported, but have not accounted for the prevalence of the traits that underlie these disorders. Examining rates of diagnoses in relation to traits may yield a clearer understanding of the degree to which racial/ethnic minority youth in Canada differ in their access to care. We sought to examine differences in self/parent-reported rates of diagnoses for obsessive-compulsive disorder (OCD), attention-deficit/hyperactivity disorder (ADHD) and anxiety disorders after adjusting for differences in trait levels between youth from three racial/ethnic groups: White, South Asian and East Asian.
Method
We collected parent or self-reported ratings of OCD, ADHD and anxiety traits and diagnoses for 6- to 17-year-olds from a Canadian general population sample (Spit for Science). We examined racial/ethnic differences in trait levels and the odds of reporting a diagnosis using mixed-effects linear models and logistic regression models.
Results
East Asian (N = 1301) and South Asian (N = 730) youth reported significantly higher levels of OCD and anxiety traits than White youth (N = 6896). East Asian and South Asian youth had significantly lower odds of reporting a diagnosis for OCD (odds ratio [OR]East Asian = 0.08 [0.02, 0.41]; ORSouth Asian = 0.05 [0.00, 0.81]), ADHD (OREast Asian = 0.27 [0.16, 0.45]; ORSouth Asian = 0.09 [0.03, 0.30]) and anxiety (OREast Asian = 0.21 [0.11, 0.39]; ORSouth Asian = 0.12 [0.05, 0.32]) than White youth after accounting for psychiatric trait levels.
Conclusions
These results suggest a discrepancy between trait levels of OCD, ADHD and anxiety and rates of diagnoses for East Asian and South Asian youth. This discrepancy may be due to increased barriers for ethnically diverse youth to access mental health care. Efforts to understand and mitigate these barriers in Canada are needed.
Plain Language Summary
We know that there is there are differences in the prevalence of childhood mental illnesses by race/ethnic group, which may be related to disproportionate access to mental health care. What is unknown is whether there this difference in prevalence is related to differences in the presence of symptoms for mental illness or whether children and youth from marginalized racial/ethnic groups have symptoms but are not getting diagnosed. This information is needed to understand the degree to which children and youth from marginalized race/ethnicity groups are accessing mental health care in Canada. We tested the differences in reported symptoms and diagnosis of three common and impairing childhood-onset disorders (obsessive-compulsive disorder—OCD), attention-deficit/hyperactivity disorder—ADHD and anxiety disorders) in children and youth (6–17 years of age) living in Canada that were from three racial/ethnic groups: White, South Asian and East Asian. East Asian and South Asian youth reported significantly higher levels of OCD and anxiety traits than White youth. However, East Asian and South Asian youth were significantly less likely than White youth to have a reported diagnosis of OCD, ADHD or anxiety even after accounting for symptom levels for each disorder. Our findings suggest that East and South Asian children are less likely than White children to get a diagnosis for common mental illness even if they have symptoms of that mental illness. This gap in receiving a diagnosis might be because of more barriers to mental health care for children and youth from marginalized racial/ethnic groups but we need more research to pinpoint the cause.
Introduction
Ethnic and racial disparities in health status and access to care are present in many domains of health care. 1 These disparities are especially salient in the field of mental health2–5 warranting calls for increased scientific attention. 6 Some studies suggest that ethnic and racial minorities have a lower prevalence of several psychiatric disorders.5,7–9 However, other evidence suggests that ethnic and racial minorities have worse mental health8,10 but are more likely to face significant barriers to mental health assessment and care resulting in unmet needs.8,11 These mixed findings may be because previous large population-based studies examined rates of physician-diagnosed psychiatric disorders 12 without examining differences in the underlying prevalence of traits of a psychiatric disorder between different ethnic and racial groups.
Race and ethnicity are related social constructs that can act as a significant socio-political lens through which racism and inequality can be understood. 13 Though distinct, there is considerable overlap between the general use and understanding of the terms “ethnicity” and “race.” Ethnicity refers to a person's cultural identity (e.g., language, customs, religion) whereas race refers to broad categories of people that are divided arbitrarily based on ancestral origin and physical characteristics.13–15 There has been increasing concern about what has been deemed an arbitrary separation of ethnicity and race in equity-based research.13,15 Proposals have been put forth to treat race and ethnicity as non-mutually exclusive categories of a single concept. Henceforward, we refer to race/ethnicity as a single variable.
The mechanisms by which race/ethnicity affects mental health care remain largely unclear. Some studies suggest that race/ethnicity can affect access due to reduced willingness to engage in mental health services8,11 though the factors underlying this reduced willingness have not been established. Reduced willingness to engage in mental health services must be considered in concert with structural barriers to accessing care such as a lack of culturally competent, timely and affordable treatment options. Other explanations suggest that the quality of mental health services may differ by race/ethnicity 16 and that rates of psychiatric disorders can be affected by experiences of discrimination, exposure to discrimination and stigma17–19 and levels of social support within the community. 20 Ethnic/racial identity has also been shown to have both positive and negative associations with the prevalence of psychiatric traits and symptoms depending on the disorders and different racial/ethnic groups examined.21–23 It remains unclear whether differential rates of psychiatric diagnoses between ethnic groups reflect differences in the population prevalence of psychiatric symptoms.
Social, cultural and economic risk factors may also contribute to youth's mental health and youth access to mental health care by influencing the accessibility of services and the quality of services available. 24 In understanding access to treatment, prevalence rates and outcomes, it is important to consider socioeconomic variables to ensure that indicators such as unemployment, poverty and poor housing, which may be independently linked with poor mental health, are not the primary drivers for differences in rates. 25 This is particularly relevant as racially/ethnically diverse young people often have an increased prevalence of these social risk factors due to historical discrimination and racism. Without controlling for the contribution of economic adversity, adverse outcomes may be falsely attributed to race/ethnicity when in fact they are driven by structural factors.
Another limitation of the existing literature examining mental health disparities is that it is largely based on adult populations4,8,9,26 and samples based in the USA1,3,5,27,28 where health care is private. In Canada, the degree to which these disparities are present among youth within a largely publicly funded health-care system is unclear.
To better appreciate the landscape of mental health difficulties for racially/ethnically diverse Canadian young people, we must better understand the prevalence of psychiatric disorders within the population. In particular, given the hypothesized differential access to care, it is important to estimate prevalence using non-clinical samples which include individuals who may not otherwise have access to clinical care. This is a complex topic, and estimations must also take into account the multiple forces that affect mental health in racially/ethnically diverse youth (e.g., socioeconomic status). To answer this question, we sought to examine ethnic/racial differences in levels of self- and parent-reported psychiatric traits and the prevalence of reported psychiatric diagnoses (while adjusting for differences in trait levels), within a large Canadian community-based sample of children and youth. We tested the following primary research questions: (1) Do youth from specific racial/ethnic groups have different levels of anxiety, obsessive-compulsive disorder (OCD) and attention-deficit/hyperactivity disorder (ADHD) traits; and (2) Do youth from specific minority racial/ethnic groups have lower odds of reporting a psychiatric diagnosis and treatment for anxiety, OCD and ADHD than white youth, after adjusting for psychiatric traits. As a secondary aim, we examined whether social and economic factors accounted for reported differences in psychiatric trait levels and/or rates of diagnoses and treatment between racial/ethnic groups.
Methods
Participants
Participants were part of the Spit for Science study that were recruited while visiting a science museum (Ontario Science Centre) between 2008 and 2009. For the purposes of this study, we only included participants residing in Canada. A demographic breakdown of the entire sample is available in Table S1. Parents provided ratings for younger children (n = 13,162; mean age = 10.2 ± 2.2 years). Youths ages 12 and older who were able to provide informed consent, reported on their own trait levels and diagnoses (n = 2900; mean age = 15.3 ± 1.4 years). Further details about the study and study participants are available in the Supplemental Material.
Ethical Considerations
We obtained informed consent and verbal assent where applicable, for all participants as approved by the Hospital for Sick Children Research Ethics Board.
Measures
Race/Ethnicity
Race/ethnicity was measured by self- or parent-reported race/ethnicity of the participant's maternal and paternal grandparents. Race/ethnicity responses were coded in accordance with the Canadian Institute for Health's Proposed Standards for Race-Based and Indigenous Identity Data Collection and Health Reporting in Canada. 29 We used a threshold of all four grandparents of a given race/ethnicity for a participant to be classified as that given race/ethnicity. We only retained participants classified as White, East Asian and South Asian, as these were the only race/ethnic groups sufficiently large to be analyzed. We conducted additional sensitivity analyses to allow for some mixed race/ethnicity in these groups (see the Supplemental Material).
Trait Measures
Psychiatric traits are characteristics that are continuously distributed within the general population. There has been increasing evidence suggesting that ADHD, OCD and anxiety disorders are extremes of a continuous trait.30,31 Trait measures may act as a proxy for the underlying distribution of a given psychiatric disorder within a given population. ADHD, OCD and anxiety traits were measured, respectively, by the Strengths and Weaknesses of Attention-Deficit/Hyperactivity-symptoms and Normal-behaviours (SWAN) rating scale, 30 The Toronto Obsessive-Compulsive Scale (TOCS) 31 and the anxiety subscale within the child behaviour checklist (CBCL). 32 Measurement invariance between each racial/ethnic group included in this study was established at the scalar level enabling mean comparisons between groups for each measure. 33 We calculated t-scores for each symptom that were standardized for the respondent (parent/self), age and gender (when significantly associated with the raw scores). To examine the discrepancy between individuals with high trait levels likely warranting a diagnosis and the rates of reported diagnoses/treatment, we classified individuals as being “high-trait” based on the estimated population prevalence of a given psychiatric disorder. High traits for OCD, ADHD and anxiety were defined as having trait scores in the 99th, 95th and 97.5th percentile of the entire sample, respectively.34–36
Reported Diagnoses
Reported diagnoses for ADHD, OCD and anxiety were measured by participants’ responses to the question: “Have you had a diagnosis of, or treatment for any of the items listed below” with a list of psychiatric disorders to select from.
Socioeconomic Status and Neighbourhood Marginalization Indices
For a subgroup of participants residing in the Greater Toronto Area (GTA; the region around the Ontario Science Centre), herein labelled as the “urban subgroup,” we estimated socioeconomic status based on the first four digits of participants’ Postal Code by calculating the quintile of neighbourhood income per person equivalent, adjusted for household size, which is released by Statistics Canada. We further obtained established neighbourhood-level indices of marginalization including material deprivation, residential instability, dependency and ethnic concentration based on the participant's Postal Code (see the Supplemental Material for details). 37 We only estimated these indices within the subgroup of participants residing in the GTA to ensure data quality in terms of spatial variability and using four-digit Postal Codes for residential proxy is valid for those in urban areas.
Statistical Analyses
To examine differences in ADHD, OCD and anxiety trait levels between ethnic groups, we estimated multiple mixed-effects linear models where standardized t-scores for each symptom were the dependent variables. Race/Ethnicity was a categorical predictor, with White youth treated as the reference group given that it was the largest category. Sibling-relatedness was accounted for as a random effect in these models. 38 To examine the possibility that results differed by the respondent on the questionnaires (parent/self), we re-ran the models with the raw score (unadjusted for respondent) stratified by the respondent.
To examine racial/ethnic differences in rates of psychiatric diagnosis, we described the proportion of individuals who reported a diagnosis and/or treatment for the given psychiatric disorder. To examine differences in the rates of psychiatric diagnosis after adjusting for participant symptom levels between racial/ethnic groups, we fit Firth binomial logistic regression models accounting for rare events39,40 with ethnicity/race as a categorical predictor and reported diagnosis for a given psychiatric disorder as the dependent variable. We then use the model's regression coefficients to calculate adjusted odds ratios for each racial/ethnic group in comparison to White youth. Sibling-relatedness was accounted for in the logistic regression models by randomly retaining one participant per family. All models were covariate-adjusted for age, gender and respondent (parent/self). We fit subsequent models adjusting for covariates such as socioeconomic status, primary language spoken at home and additional indices of marginalization: residential instability, material deprivation, dependency and ethnic concentration in the subgroup of participants residing in GTA. We also compared the prevalence of individuals with “high traits” for a given disorder with the prevalence of reported diagnoses for each racial/ethnic group.
Results
Participant characteristics are described in Table 1.
Sample Characteristics.
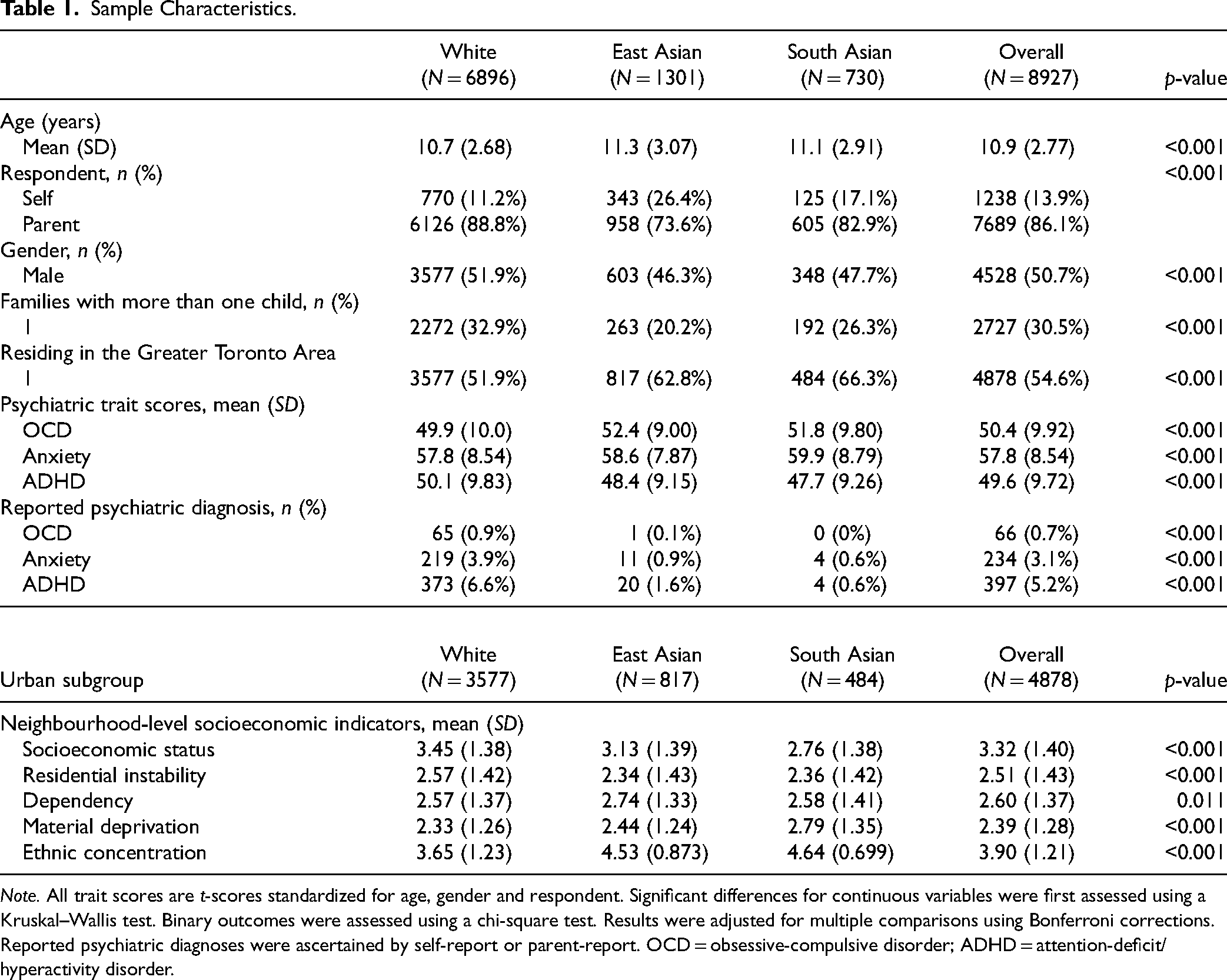
Note. All trait scores are t-scores standardized for age, gender and respondent. Significant differences for continuous variables were first assessed using a Kruskal–Wallis test. Binary outcomes were assessed using a chi-square test. Results were adjusted for multiple comparisons using Bonferroni corrections. Reported psychiatric diagnoses were ascertained by self-report or parent-report. OCD = obsessive-compulsive disorder; ADHD = attention-deficit/hyperactivity disorder.
Ethnic/Racial Differences in Neighbourhood Marginalization Levels
As shown in Table 1, within the subsample of participants residing in the GTA, East Asian and South Asian participants were of significantly lower socioeconomic status than White participants. South Asian and East Asian youth, on average, lived in neighbourhoods with significantly higher levels of ethnic concentration and material deprivation. On average, East Asian youth lived in neighbourhoods with higher levels of dependency than White youth. White youth tended to live in neighbourhoods with significantly higher levels of residential instability than East Asian and South Asian youth.
Ethnic/Racial Differences in Mental Health Trait Levels
East Asian and South Asian youth had significantly higher levels of OCD traits and anxiety traits compared to White youth (Table 2). However, East Asian and South Asian youth had significantly lower levels of ADHD traits. Results in the total sample were consistent in the urban subgroup even after adjustment for covariates. When we repeated the analysis stratifying by questionnaire respondent (parent or youth), the results did not change (data not shown).
Differences in Psychiatric Trait Levels between Ethnic/Racial Groups.
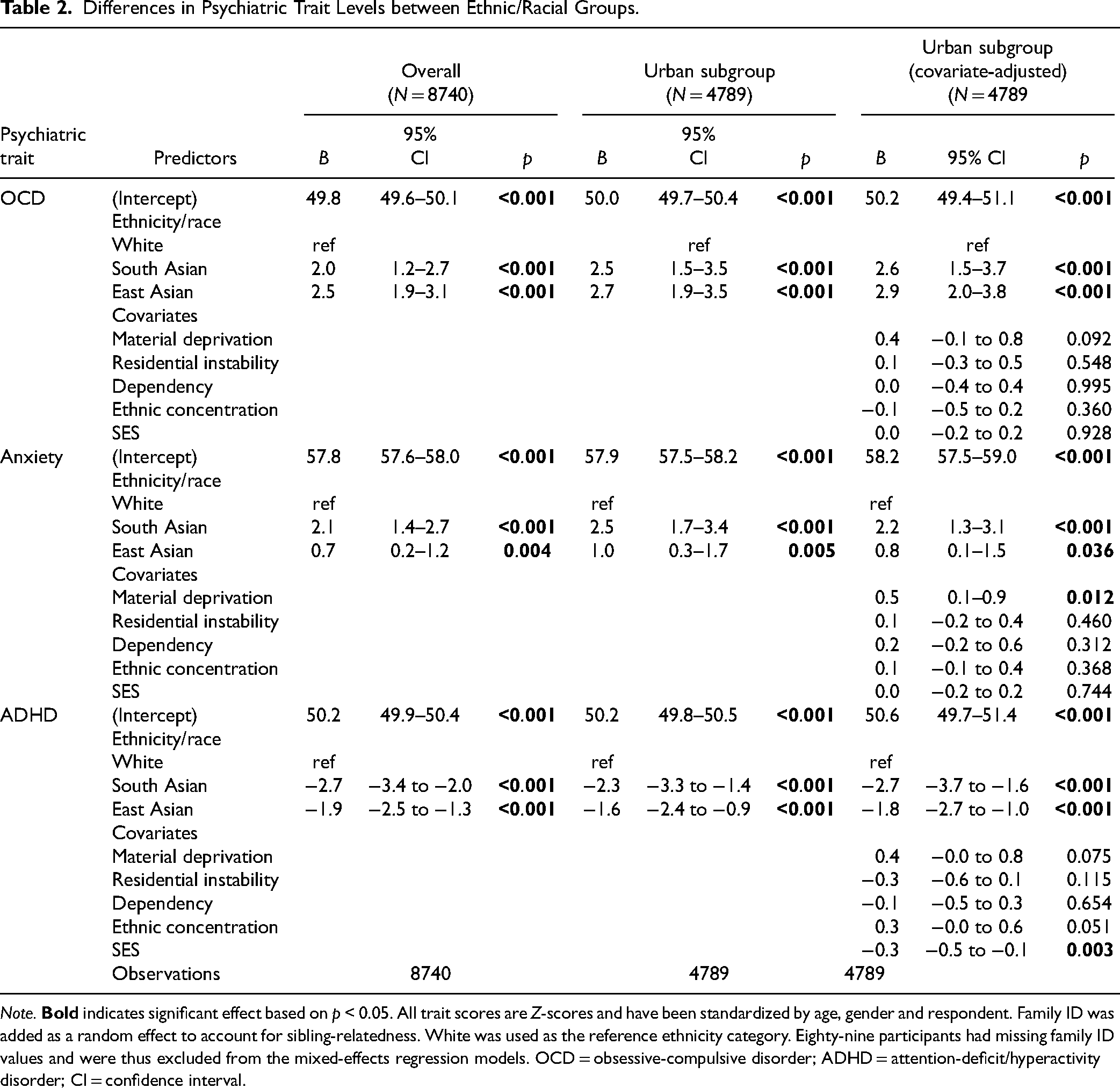
Note.
As shown in Table 2, results in the sample of participants residing in the urban subgroup, were consistent for OCD and ADHD, even after adjusting for covariates including age, gender, material deprivation, ethnic concentration, dependency, residential instability and socioeconomic status. We also observed that socioeconomic status was inversely associated with ADHD trait levels and that material deprivation was positively associated with ADHD traits.
Ethnic/Racial Differences in Odds of Reporting Diagnosis
As shown in Table 3, South Asian youth had 95% decreased odds of reporting a diagnosis and/or treatment for OCD compared to White youth after adjusting for OCD trait levels. Similarly, East Asian youth had 77% lower odds of reporting a diagnosis and/or treatment for OCD. South Asian and East Asian youth had 86% and 76% reduced odds, respectively, of reporting a diagnosis and/or treatment for anxiety compared to White youth. For ADHD, South Asian and East Asian youth had 88% and 75% lower odds of reporting a diagnosis or treatment for ADHD compared to White youth after adjusting for ADHD trait levels. All results showed no major differences in the urban subgroup, after adjusting for covariates with similar effect sizes and p-values. Increasing age was significantly associated with increased odds of reporting a diagnosis for each disorder examined. Females were significantly less likely to report a diagnosis/treatment for ADHD after accounting for trait levels, but no gender differences were found for anxiety and OCD. Having a non-English language primarily spoken at home was associated with reduced odds of reporting a diagnosis and/or treatment for anxiety. The odds of reporting a diagnosis for OCD, anxiety and ADHD, respectively, across a range of trait levels (t-scores) are illustrated in Figure 1.
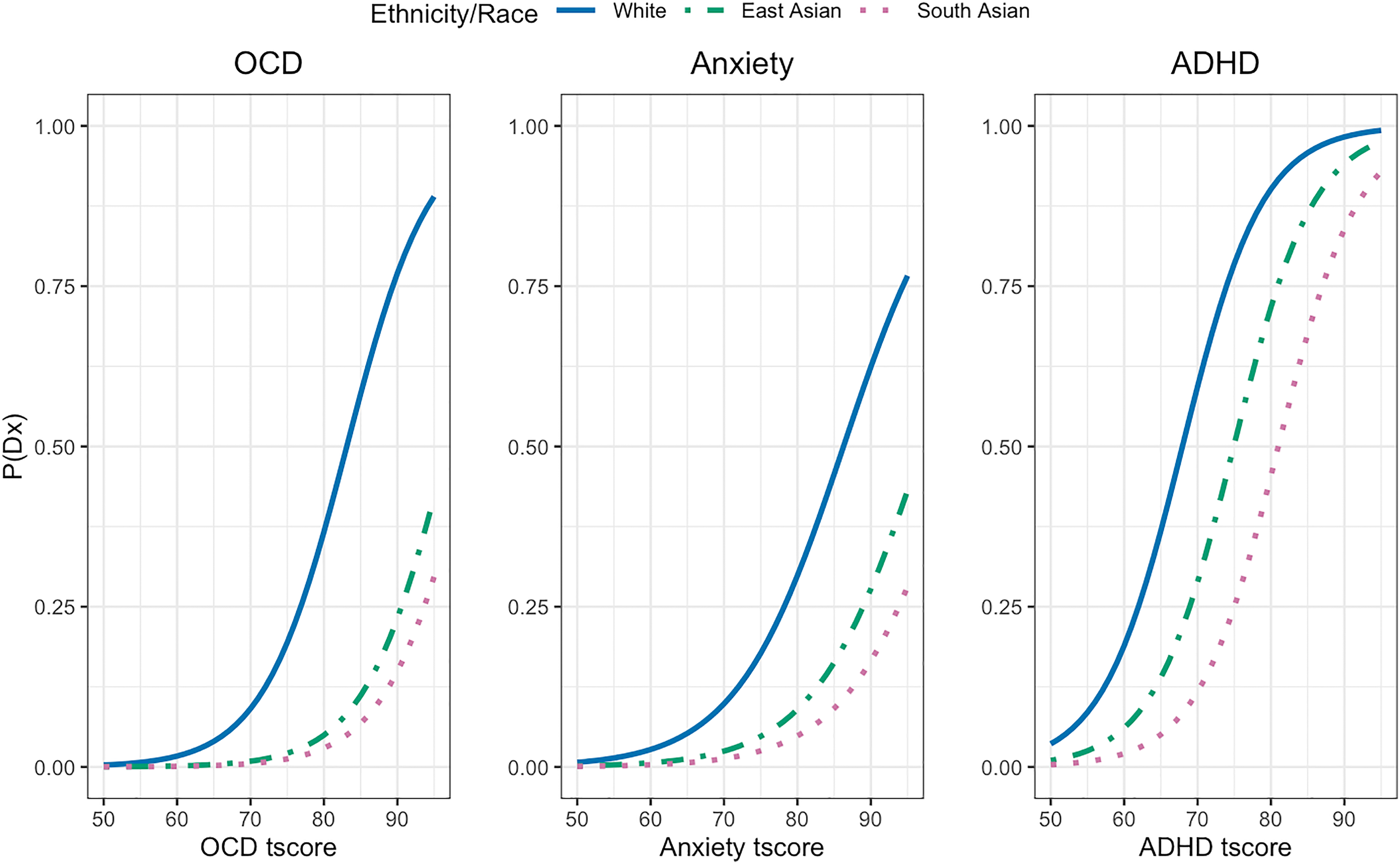
Probability of reporting OCD, ADHD and anxiety diagnoses across the spectrum of trait severity by ethnic/racial group. This figure illustrates the odds of reporting a given psychiatric diagnosis across the spectrum of trait severity between ethnic/racial groups. OCD traits were measured by the Toronto Obsessive-Compulsive Scale (TOCS). ADHD traits were measured by the Strengths and Weaknesses of ADHD scale (SWAN). Anxiety was measured using the Child Behaviour Checklist (CBCL) Anxiety subscale. t-scores were calculated accounting for effects of age, gender and respondent when significantly associated with raw scores. OCD = obsessive-compulsive disorder; ADHD = attention-deficit/hyperactivity disorder; Dx = parent/self-reported diagnoses.
Differences in the Probability of Reporting a Psychiatric Diagnosis between Ethnic/Racial Groups.
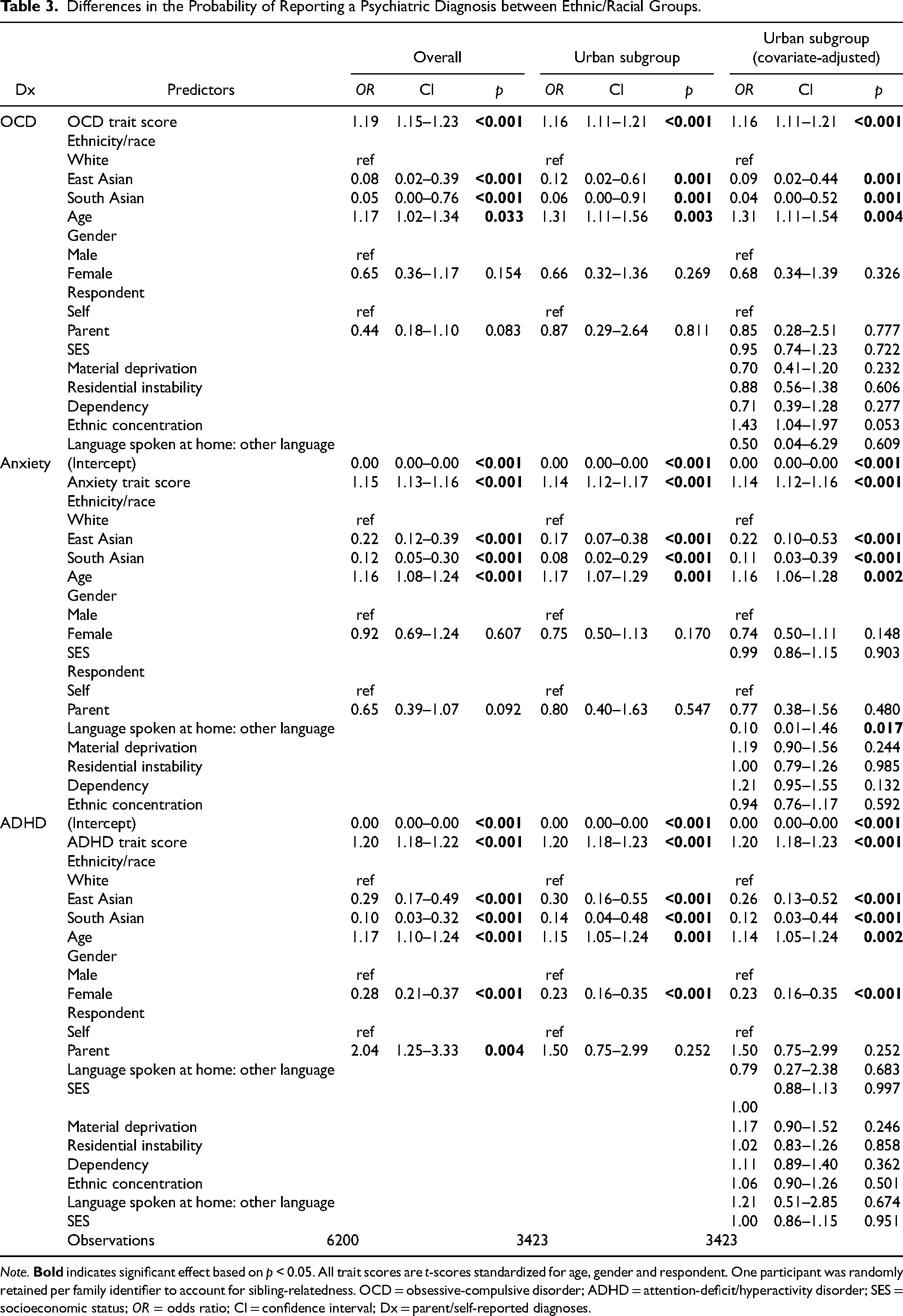
Note.
Examining the Prevalence of High Trait Levels Versus Reported Diagnosis Between Ethnic/Racial Groups
We further compared the proportion of individuals with high trait levels of a given condition with the proportion who had reported a diagnosis (Figure 2). For OCD, anxiety and ADHD, there was a discrepancy between the prevalence of high trait levels versus the prevalence of those who received a diagnosis within the South Asian group, especially when compared to the White group. There were similar trends for OCD and ADHD within the East Asian group (Figure 2).
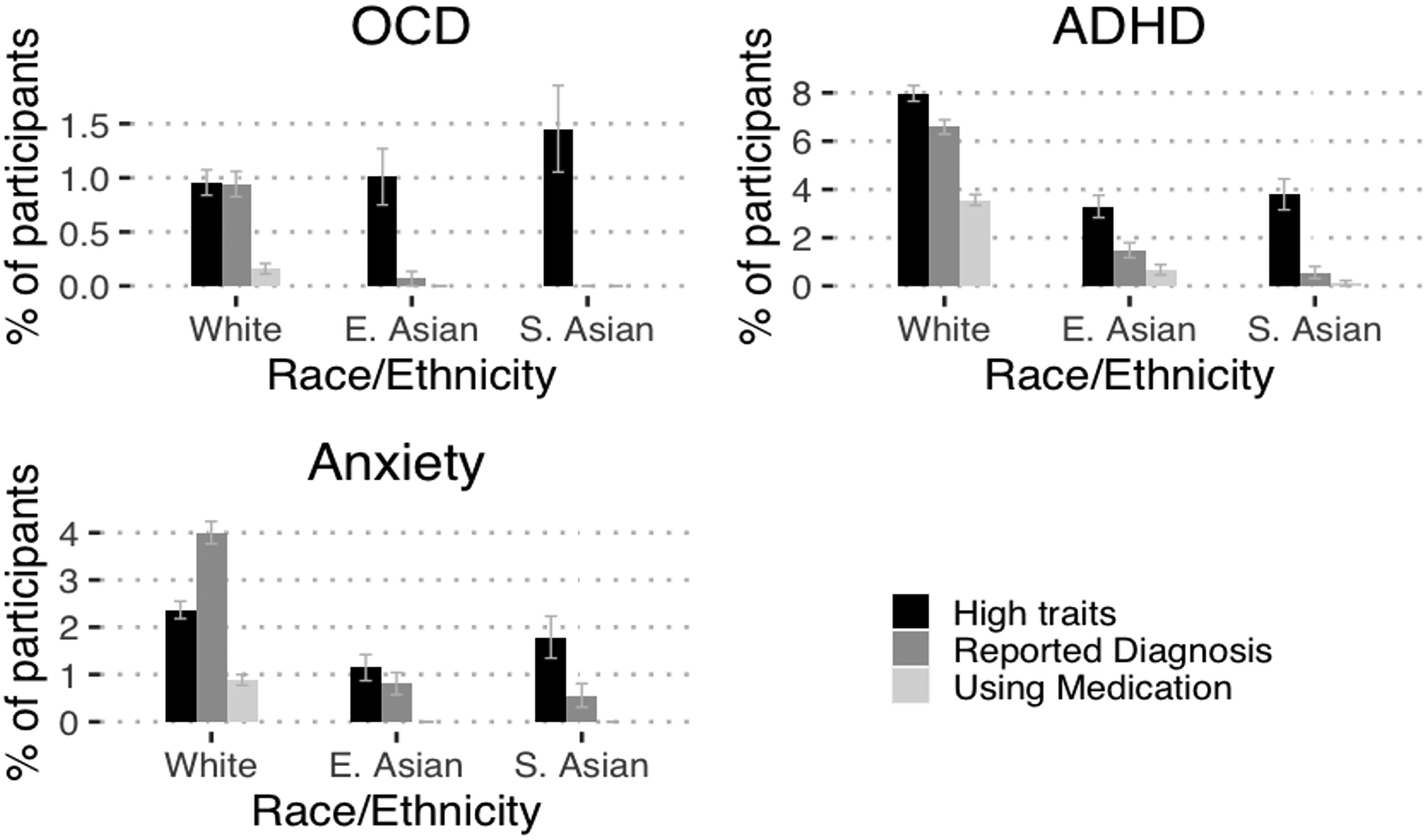
Discrepancies in psychiatric trait levels and rates of diagnoses by ethnic/racial group. This figure illustrates the prevalence of individuals with high traits and diagnoses for a given psychiatric disorder between ethnic/racial groups. High trait was defined based on the estimated population prevalence of a given psychiatric disorder. High trait for OCD was defined as having OCD trait scores in the 99th percentile of the population. ADHD high trait was defined as having ADHD trait scores 95th percentile or above for either inattentive, hyperactive or overall trait score. Anxiety high trait was defined as having trait scores greater than the 97.5th percentile within the population. Community diagnosis/treatment was ascertained based on parent or self-reported responses of whether the child had received a diagnosis for the given psychiatric disorder and/or received treatment for it. OCD = obsessive-compulsive disorder; ADHD = attention-deficit/hyperactivity disorder; E. Asian = East Asian; S. Asian = South Asian.
Discussion
This study examined whether there is a discrepancy between traits and rates of diagnoses for OCD, ADHD and anxiety disorders based on ethnicity/race and social factors in Canada.
Ethnic/Racial Group Differences in Psychiatric Trait Levels
We found that East Asian and South Asian youth reported having or were reported as having elevated levels of OCD traits compared to their white peers. This trend is similar to studies in adults that show an association between Asian ethnic identity and several OC symptom dimensions. 21 Some findings from clinical samples contradict our results suggesting that OCD symptom severity does not differ based on ethnicity; however, later age of OCD symptom onset, clinical diagnosis and treatment have been noted. 22 It is possible that the increased prevalence of OCD traits within our sample reflects more developed mental illness due to a lack of diagnosis and treatment within the East and South Asian communities. These differences in findings may also be due to the nature of the sample studied. Unlike clinical studies, the present community-based sample includes East and South Asian youth with high OCD traits but no OCD diagnosis potentially due to barriers in accessing care and assessment.41–43
We also found that East Asian and South Asian youth had significantly higher mean levels of anxiety. These results line up with studies within pediatric clinical populations within the USA.10,44 Experiences of racism 45 and familial/academic pressure and expectations 46 have been proposed as factors that underlie this difference. However, we also observed that increasing levels of anxiety were associated with living in a neighbourhood with increasing material deprivation. This finding suggests that socioeconomic factors may be related to risk for anxiety traits over and above the associations of ethnicity. Further work is needed to precisely elucidate the mechanisms behind these trends within Canadian youth.
We found that East Asian and South Asian youth had less reported ADHD trait levels than White youth. Additionally, East Asian and South Asian youth also were less likely to report a diagnosis of ADHD, even after adjusting for trait levels. This result suggests the lower reported diagnosis of ADHD in East and South Asian youth may be in part related to a reduced prevalence of the disorder in these racial/ethnic groups as reported previously,5,28,47,48 however, there are likely potential barriers to accessing care for Asian children. Further investigation into protective factors for ADHD traits within East Asian and South Asian youth would be beneficial. We also observed that increased levels of material deprivation and decreasing socioeconomic status were associated with an increased prevalence of ADHD traits. This finding was consistent with studies conducted in the UK 49 suggesting that financial insecurity may be a risk factor for ADHD in youth.
Ethnic/Racial Disparities in Reporting Diagnosis and Treatment
Critically, across all psychiatric disorders examined in this study, we found that South Asian and East Asian youth had substantially reduced odds of reporting a diagnosis and treatment than White youth at every level of trait severity. The magnitude of these effects emphasizes that there are significant barriers to accessing mental health care within these ethnic/racial groups. These trends are especially concerning in the context of OCD and anxiety, where South Asians had increased trait levels relative to White youth. There are many speculative reasons behind these trends. It is well understood in adult and US populations that Asian populations have some of the lowest rates of mental health service utilization.11,42 Community, family and self-stigma may contribute to this phenomenon. 43 One study conducted within South Asian populations residing in Ontario suggested that systemic-, family- and community-level barriers to mental health care exist, including a lack of South Asian representation within mental health professionals, long wait times, prohibitive fees for services not covered by government health-care coverage and culturally insensitive treatment. 50 For anxiety, we also observed that having a non-English language spoken as the primary language at home was associated with decreased odds of reporting a diagnosis and/or treatment. This trend suggests that language barriers at the individual or family level may be an additional barrier to receiving a psychiatric diagnosis for minority ethnic children. 51 Another potential mechanism behind these trends is differences in the way that psychiatric traits within minority youth are interpreted by family members, teachers, guidance counsellors, health-care professionals and youth themselves, all of whom play key roles in the recognition of psychiatric disorders. Mental health-care provider racial bias has also been demonstrated as a contributing factor in the misdiagnosis of ethnic and racial youth. 52 Cultural differences impacting the presentation of psychiatric traits in clinic may also be a contributing factor to the disparities in diagnoses, however, literature examining the relationship between cultural factors and psychiatric presentation in youth is scarce. We also observed that the disparities in OCD and anxiety diagnoses were greater than the disparities observed in ADHD. Several hypothetical factors could contribute to this discrepancy. ADHD is an externalizing disorder and teachers play a major role in symptom recognition, which could increase the likelihood of accessing care. Another contributor may be differential access to primary versus specialist health-care providers. Primary care providers may be more comfortable treating ADHD in youth and may be more likely to suggest specialist assessments for anxiety disorders, particularly OCD. Ethnic/racially minoritized youth may have less access to specialists, which further contributes to the greater disparities in OCD/anxiety versus ADHD diagnoses. It is also possible that OCD and anxiety may be more stigmatized conditions in certain ethnic/racial communities compared to ADHD prompting decreased help-seeking behaviours. Investigating the mechanisms behind these trends is complex because of the inter-relatedness of risk factors such as race/ethnicity and social deprivation and likely involves both structural and individual levels.
A few limitations should be considered within the current study. First, our main outcomes were established by self-/parent-reported diagnosis rather than clinician-verified diagnoses. Second, we utilized participants’ maternal and paternal grandparents’ ethnicity as a proxy for participants’ race/ethnicity because we were using data from an existing genetic study. That said, we underwent multiple sensitivity analyses to ensure that the threshold for altering the definition and measurement of race/ethnicity would not our conclusions. Third, we limited our analyses to White, East Asian and South Asian youth due to insufficient sample sizes for other racial/ethnic groups. It is critical that further work is conducted with larger data sets to understand mental health disparities in different marginalized ethnic groups within Canada. Fourth, our participants were recruited from a science museum, which has an admission fee for entry, which may have limited the representativeness of the sample. However, our rates of reported psychiatric diagnoses are overall similar to previous large epidemiological studies, suggesting the general representativeness of the sample. Fifth, we did not include depression in our analyses because depression trait data were not collected. However, these data are currently being collected to contribute to future work in this area. Finally, we did not have any participant-level socioeconomic measures which could have affected our results.
Conclusions and Implications
Within Canada, East Asian and South Asian children show large disparities in rates of psychiatric diagnoses and access to care compared to White youth, even after controlling for underlying psychiatric trait levels and socioeconomic factors. These findings highlight reasons for concern. Lower rates of psychiatric diagnoses and care may leave East Asian and South Asian youth in need of care with no access to treatment and worse eventual outcomes. Furthermore, psychiatry research largely focuses on cohorts of participants with diagnoses. Disparities in access to diagnoses may exclude certain ethnic/racial populations from research, further widening the research and treatment gap for historically marginalized communities. More work is critically needed to understand and mitigate barriers to equitable mental health care for racial/ethnic minoritized youth within Canada.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437241233936 - Supplemental material for Racial/Ethnic Disparities in Psychiatric Traits and Diagnoses within a Community-based Sample of Children and Youth
Supplemental material, sj-docx-1-cpa-10.1177_07067437241233936 for Racial/Ethnic Disparities in Psychiatric Traits and Diagnoses within a Community-based Sample of Children and Youth by Andrew Dissanayake, Annie Dupuis, Christie L. Burton, Noam Soreni, Paul Peters, Amy Gajaria, Paul D. Arnold, Russell Schachar and Jennifer Crosbie in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
The statistical expert on the manuscript is Dr. Annie Dupuis. The authors thank the families and participants of Spit for Science who made this study possible.
Data Access
The data that support the findings of this study are not openly available and are available from the corresponding author upon reasonable request (including a study outline), subject to review.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Andrew Dissanayake, Annie Dupuis, Christie L. Burton, Noam Soreni, Paul Peters, Jennifer Crosbie and Russell Schachar report no biomedical financial interests or potential conflicts of interest. Amy Gajari would like to disclose funding for research time by the O’Brien Fund at CAMH and by the Margaret and the Wallace McCain Centre for Child, Youth, and Family. She would also like to disclose a one-time speaking fee paid by Mathers, McHenry, and Co. for professional development training on working with clients with mental health difficulties. Paul D. Arnold would like to disclose grant support from Biohaven Pharmaceuticals unrelated to the topic of this manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Canadian Institutes of Health Research (Paul D. Arnold: MOP-106573; Russell Schachar: MOP-93696) and the Alberta Innovates Translational Health Chair in Child and Youth Mental Health (Paul D. Arnold).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.