
Abstract

Introduction
Training in the management of substance use disorders (SUDs) in psychiatry remains disproportionately limited in psychiatric residency training programs, compared with other major psychiatric disorders, despite SUDs becoming increasingly common in all psychiatric care settings.1,2 Given the high prevalence of SUDs in psychiatric practice and unmet treatment needs for persons with comorbid psychiatric and SUD,3–6 it is imperative that all psychiatry residents develop the requisite knowledge, skills and attitudes for managing persons with SUD.
A shortage of experienced faculty, negative attitudes toward patients with SUD, lack of adequate curriculum and poorly defined educational goals and requirements have been identified as factors leading to limited training in SUD.7,8 The original Curriculum Guidelines for Residency Training of Psychiatrists in Substance-Related Disorders, 9 published by the Canadian Psychiatric Association (CPA) as a position paper in 1997, aimed to define curriculum and educational goals, but without Royal College of Physicians and Surgeons of Canada (RCPSC) requirements, little changed. On July 1, 2009, proficiencies in SUD became required by the RCPSC for all new Canadian psychiatry residents, to be realized during the five years of residency training. Requirements called for training programs to have a minimum one-month discrete rotation that was separate from other rotations focusing on the supervised experience in the treatment of patients with SUDs in various settings, the availability of a postgraduate year (PGY)-4 to -5 selective rotation in the management of SUD of at least three months, specific proficiencies in SUDs and introductory knowledge of motivational interviewing (MI). To help guide Canadian psychiatric residency training programs meet the requirements, national consensus was garnered resulting in the publication of two position papers by the CPA in 2015.1,10 It was recognized then, that a one-month rotation experience was unlikely to allow the resident to fully realize the expected proficiencies. However, it represented a significant step forward. When combined with seminars, the requirements began to lay an adequate foundation for residents in SUD, one that could be augmented by additional training experiences and ongoing continuing medical education (CME) to help more fully meet the requirements.
In 2020, Canadian psychiatry training programs began the transition from a traditional time-based training model to Competence by Design (CBD), with promotion in the program linked to successfully completing entrustable professional activities (EPAs). The publication of the new psychiatry competencies 11 and training experiences 12 ended the requirement of the one-month rotation in SUD, and instead, SUD case types are required, with multiple EPAs occurring during the foundations of discipline (FoD) and core of discipline (CoD) stages of training. 13 In FoD, additional clinical training experiences are required in at least three of the following eight areas, occurring in any care setting: addictions, community psychiatry, consultation liaison psychiatry, family medicine, general internal medicine or other medical subspecialty, geriatric medicine, palliative care and pediatrics. Formal instruction needs to occur in the “etiology, diagnosis, treatment and natural course of major psychiatric disorders, including substance use and withdrawal.” In the CoD stage, a required training experience is the care of special populations (integrated into other experiences or as discrete experiences), including patients with addictions and concurrent psychiatric diagnoses. For the “one other evidence-based psychotherapy” part of the required training experiences in the delivery of psychotherapeutic treatments, MI is one of the five recommended training experiences in addition to dialectical behaviour therapy, family or group therapy, interpersonal therapy and long-term psychodynamic psychotherapy (if not the modality of the required experience). In this context, the prior training guidelines have become outdated, necessitating this update to help programs recognize the psychiatry competencies as they apply to SUD, the EPAs related to SUD, and the nature of adequate entrustment when an EPA is being evaluated to best guide coaching and competence development.
To address the new psychiatry competencies and training experiences with CBD, a working group with national representation and expertise in addictions was reconstituted to update the position papers on education in addiction psychiatry and offer updated curriculum guidelines for psychiatric residency training in SUD. Part one of this two-part position paper describes current knowledge, skills and attitudes that practicing psychiatrists require to be able to provide evidence-based competent care, as well as to be able to appropriately evaluate and coach psychiatry residents in the EPAs on SUD. The core goals and objectives of this second part of the position paper are to review and describe the psychiatric competencies as they apply to SUDs, and to identify the EPAs related to SUD with a rubric for their evaluation to promote more uniform knowledge, skill and attitude development for residents nationally. The recommendations for EPA evaluation are based on the prior CPA position papers,1,10 practice guidelines,14–18 research papers and book chapters published on medical and postgraduate education in addictions2,8,18–21 and major textbooks.8,22,23 This position paper aims to provide guidance to residency training programs in Canada to facilitate the training of general psychiatrists to competently manage patients with concurrent or primary SUD in psychiatric practice using evidence-based practices with appropriate optimism for improvement.
Recommendations
The recommendations are divided into three sections. The first section details the clinical content based on the RCPSC psychiatry competencies delineating areas of knowledge in SUD that residents need to acquire, including substance effects, biopsychosocial understanding of SUD and the overlap with major mental disorders, addiction epidemiology, assessment and diagnostic skills for SUD and concurrent disorders, pharmacotherapy of SUD and concurrent disorders, recognition of stage of change, choice of most appropriate treatment setting, skills in treatment delivery including use of evidence-based psychotherapies, awareness of community resources, the role of the family in recovery and attitudinal components. The second section on detailed seminar content describes the content and means to develop a skill-based interactive curriculum, including suggested timing or sequencing. The third section on clinical rotations and EPAs describes the EPAs applicable to SUD and the means to evaluate them.
Detailed Clinical Content for SUD Curriculum
Canadian psychiatric residents are expected to develop proficient clinical knowledge, skills and attitudes appropriate to their practice to assess, manage, and if necessary, appropriately refer patients who present with a primary or comorbid SUD. Knowledge, skills and attitudes need to reflect appreciation of the continuum of substance use and behaviours associated with SUD, ranging from abstinence and limited use to at-risk use to the different severities of substance use and behavioural addictions. The recommended SUD curriculum content based on the 2020 competencies is organized by domain rather than CanMEDS roles for ease of implementation (Tables 1 and 2).
Royal College of Physicians and Surgeons of Canada (RCPSC) knowledge and skills definitions.36,*
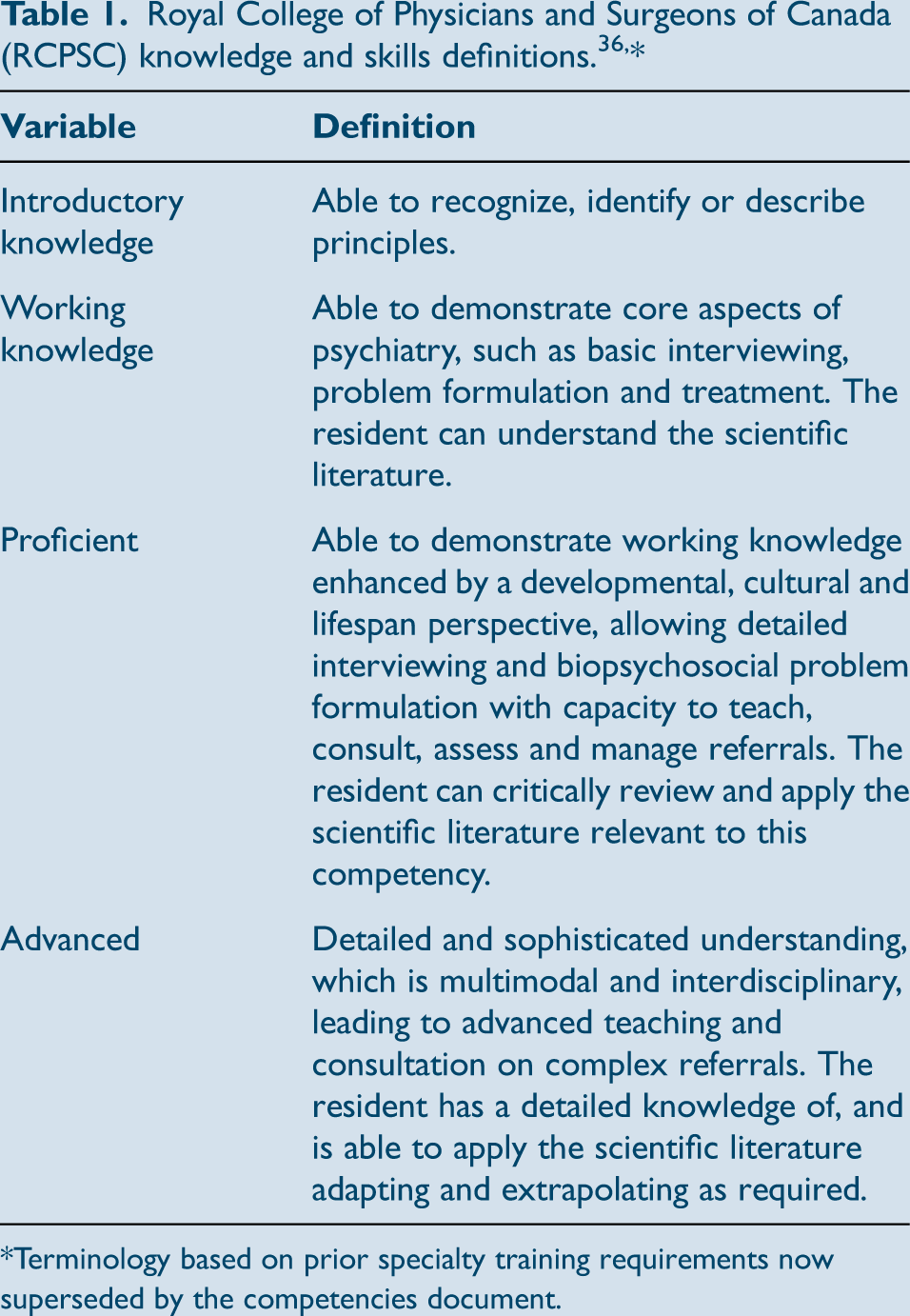
*Terminology based on prior specialty training requirements now superseded by the competencies document.
Proposed stage-specific competencies in SUD.
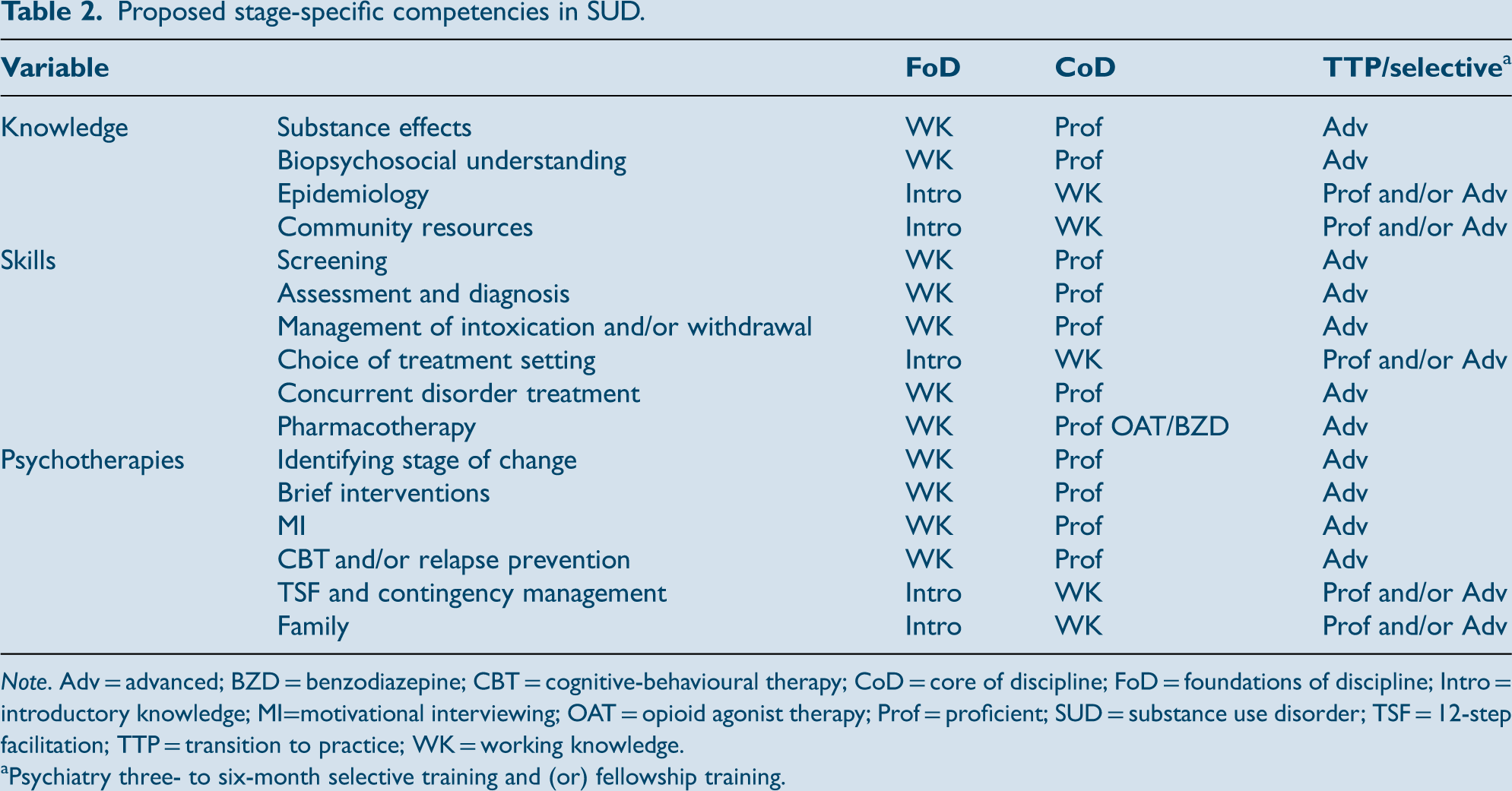
Note. Adv = advanced; BZD = benzodiazepine; CBT = cognitive-behavioural therapy; CoD = core of discipline; FoD = foundations of discipline; Intro = introductory knowledge; MI=motivational interviewing; OAT = opioid agonist therapy; Prof = proficient; SUD = substance use disorder; TSF = 12-step facilitation; TTP = transition to practice; WK = working knowledge.
Psychiatry three- to six-month selective training and (or) fellowship training.
Proficient knowledge of the mechanism of action for the primary substances encountered in clinical practice, including alcohol, nicotine and tobacco, caffeine, cannabis, sedative–hypnotics (benzodiazepines, z-drugs, barbiturates and gamma-hydroxybutyric acid), stimulants (cocaine, amphetamines and so-called designer stimulants), opioids, N-methy-D-aspartate receptor (NMDA) antagonists (phencyclidine and ketamine), inhalants, steroids and hallucinogens/psychedelics (classical and designer hallucinogens). This provides a foundation for understanding how addiction develops and the basis for different intoxication and/or withdrawal syndromes. Proficient knowledge of substance intoxication and withdrawal syndromes enabling their identification and management, whether in an acute setting or in the community. This requires the skills to complete a safety assessment to recommend the most appropriate withdrawal management setting and the most appropriate medication management. Working knowledge of the effects of chronic
substance use on the development and perpetuation of medical complications (e.g., hepatitis and human immunodeficiency virus) and comorbid mental disorders. Working knowledge of the similarities and differences between behavioural and substance-related addictions (using DSM-5 TR criteria for SUD).
24
Proficient knowledge of the critical role of the brain's extended dopamine reward pathway as the key mediator of the neurobiological basis for how a SUD develops incentive salience for future behaviour choices, compared with natural rewards. Proficient knowledge of other biopsychosocial factors contributing to risk and resilience, including drug type, delivery method, dosing, age of exposure, genetics and genomics, underlying psychiatric disorders and personality traits, expectancies from use, environment, history of trauma, abuse or neglect, peer use, availability, cultural and/or religious and/or spiritual factors and economics. Working knowledge of how psychosocial and cultural risk factors may contribute to the initial use of addictive substances and behaviours and progression to SUDs and behavioural addictions, understanding the interaction with biological risk and protective factors. This knowledge would help frame an understanding of different interventions to address the continuum of substance use, from at-risk use to the most severe forms of SUDs, as well as the recovery process. Working knowledge of the models proposed to
understand the development of concurrent psychiatric and SUD, including overlapping biopsychosocial components. Working knowledge of the prevalence of each of the SUDs and behavioural addictions (e.g., gambling disorder and internet gaming disorder), including appreciation of different rates based on age, gender, location and ethnicity. Proficient knowledge of SUD comorbidity with the major psychiatric and medical disorders. Working knowledge of current trends in SUD prevalence related to the availability of substances, perceptions of risk, fatality rates and other factors that promote and protect from the development of SUD. Working knowledge of the different trajectories and predictors for the course of SUD. Understanding how access to evidence-based treatments can change outcomes and an awareness of the phenomenon of natural recovery. Proficient knowledge and skills in the identification of SUD and behavioural addictions:
Be able to screen for use of alcohol, cannabis, opioids, sedative-hypnotics and other substances (both illicit and licit), including tobacco and e-cigarette use, prescription drugs, over-the-counter medications and behavioural addictions. Recognize typical signs and symptoms that would prompt more in-depth assessment for a SUD. Assess for potential at-risk use and factors that can predispose to problematic use and a SUD. Elicit a history indicative of a SUD and/or a behavioural addiction leading to a comprehensive diagnostic assessment using DSM-5 TR criteria for SUDs, gambling disorder and any comorbid psychiatric disorders. Perform a mental status examination, including recognition of intoxication or withdrawal status, longer-term cognitive effects of substances and physical signs of SUD. Differentiate as best as possible substance-induced psychiatric symptoms from independent psychiatric disorders and understand their clinical relevance. Working knowledge of screening instruments for SUD and behavioural addictions. This includes the Alcohol Use Disorders Identification Test (AUDIT),
25
Cannabis Use Disorder Identification Test-revised (CUDIT-R),
26
and their minimum cut-off values. Introductory knowledge of other screening instruments, such as the Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST)
27
and more comprehensive instruments to thoroughly evaluate the impact of addictive behaviours (e.g., Addiction Severity Index).
28
Proficient knowledge in the use of objective tools to assess withdrawal, especially the Clinical Institute Withdrawal Assessment for Alcohol, revised (CIWA-Ar)
29
and the Clinical Opiate Withdrawal Scale (COWS).
30
Working knowledge of the role of laboratory screening, urine drug screening and other forms of drug screening with their potential limitations. Working knowledge of common comorbid conditions when a SUD is present (e.g., psychosis with cannabis and stimulant use disorders; endocarditis and communicable diseases with intravenous drug use; anxiety, depressive, and sleep disorders with alcohol and sedative–hypnotic use disorders; and sexual disinhibition with stimulant use disorders, etc.). Proficient knowledge of the different stages of change reflective of the transtheoretical model
31
and how it is assessed. Proficient knowledge of how stage of change can evolve and may be different for each psychiatric and/or substance use disorder. Proficient knowledge and skills in how to alter treatment approaches based on the stage of change. Proficient knowledge and skills in MI approaches and brief interventions to help facilitate change.23,32–34 Working knowledge (but preferably proficient knowledge and skills) in cognitive-behavioural therapy (CBT)/relapse prevention for SUDs and/or 12-step facilitation. Working knowledge of contingency management as a method to create short-term incentives toward drug use reduction and abstinence. Proficient skills in using a trauma-informed and chronic disorder approach incorporating harm reduction, including disease prevention, health promotion and health surveillance in interactions with individual patients with SUD. Working knowledge in determining the most appropriate treatment setting for a person's SUD and/or comorbid psychiatric disorder (e.g., outpatient, residential and inpatient), minimum durations of treatment and types of providers required. Working knowledge of how to select best treatments and modify this based on response (e.g., use of the American Society of Addiction Medicine Patient Placement Criteria [ASAM PPC-2R]).
35
Proficient knowledge and skill to implement a patient-centred care plan that supports ongoing care, follow-up on investigations, response to treatment and further consultation. Hand over the care of a patient with SUD to another health-care professional to facilitate continuity of safe patient care and ensure treatment retention of adequate intensity and duration. Assess and manage safety risks for patients in all settings including non-suicidal self-injurious behaviour, suicidal behaviour and potential for violence/aggression. Assess and manage change in substance use, abstinence and treatment adherence in an ongoing manner. Proficient knowledge and skill in the use of pharmacotherapy for SUD, including medications for alcohol withdrawal, alcohol use disorder, opioid use disorder (OUD), including how to initiate and manage opioid agonist therapy (OAT), and nicotine/tobacco use disorder. Proficient knowledge and skill in the pros and cons of sedative–hypnotic prescriptions, recognizing patients at risk for developing problematic use, and strategies to safely taper and discontinue. Proficient knowledge and skill in the use of pharmacotherapy and psychotherapy for psychiatric disorders with comorbid SUD. Working knowledge of mutual help (e.g., Alcoholics Anonymous, other 12-step groups and recovery groups based on CBT or other models) and how to facilitate involvement in these recovery resources (e.g., 12-step facilitation). Working knowledge of community and hospital resources available to treat or to help manage SUD particular to their community, including evidence-based harm reduction approaches, withdrawal management facilities, outpatient treatment options, private counselling or clinics and residential treatment centres. Working knowledge of the impact of SUD on a person's family and community. Working knowledge and skills to support and involve the person's family and support network in the recovery process including psychoeducation, mutual support groups such as Al-Anon and couples and/or family therapy. Working knowledge and skills about tailoring or recommending treatments for special populations (e.g., Indigenous, LGBTQ+ and marginalized populations) and to different needs related to age, gender, socioeconomic and ethnocultural factors. Advocate for system-level changes in SUD care and resources by advocating for the needs of the communities or populations where they work in a socially accountable manner. Proficiency in personal awareness of one's own reactions and potential biases toward patients with SUD, with empathy for their condition and appropriate optimism for change and improvement over time. Proficient communication using a patient-centred approach that encourages patient trust and autonomy, characterized by empathy, respect and compassion. Proficient knowledge of factors influencing a patient's reactions to the physician, including cultural factors, trauma and the patient's previous health care experience(s). Proficient recognition of the impact of stigma and cultural factors on a patient's access to care and adoption of an attitude that is non-judgmental. Proficiency in responding to an individual patient's health needs by advocating for the patient within and beyond the clinical environment for treatment inclusion for persons with SUD. Incorporate opportunities for harm reduction.
Seminar Organization for SUD Curriculum
A skills-based curriculum that is interactive and experiential in nature should be emphasized to progressively increase knowledge, skills and attitudes toward patients with SUDs from mild to severe and behavioural addictions. The curriculum should recognize the lifelong process of learning, beginning with medical school and later reinforced through CME. The timing and content of the substance-related and addictive disorders curriculum can be incorporated into current seminars or could stand alone, depending on the needs of each individual program and the available resources. Incorporating SUD curriculum into current seminars (an integrated format) may facilitate greater teaching and discussion around comorbidities, where both teaching staff and residents may enhance their knowledge and skill sets in SUD, but may limit the time available for discussion of specific evidence-based SUD treatments and may come at the expense of consistency. Stand-alone seminars may better allow for in-depth discussion of SUD topics and the sequencing of education in addictions to better match trainees’ foundational knowledge, skills and attitudes as their training progresses, but potentially limit incorporation of practices with patients presenting with prominent psychiatric syndromes. It is suggested that for the curriculum in PGY-1 or PGY-2, a minimum of three hours of separate, or the equivalent of integrated seminar time, be dedicated to foundational knowledge in addiction psychiatry and introduce brief interventions. In PGY-2 to PGY-5, it is suggested that a minimum of six hours of separate, or the equivalent of integrated seminar time, be dedicated to advanced principles of addiction psychiatry. In PGY-2 to PGY-5, occurring separately, integrated into existing psychotherapy seminars, or part of the addiction lectures, it is suggested that an introductory seminar equivalent to a minimum of three hours introduce core concepts behind MI, relapse prevention, and 12-step facilitation that, ideally, incorporate case scenarios or real and/or simulated patients for the practice of techniques and feedback. More detailed descriptions of seminar content and CME are included in the supplemental materials section.
Clinical Rotations and EPAs
As the EPAs for SUD are in both the foundations of discipline (FoD) and Core of Discipline (CoD), a one-month rotation in SUD as previously required before the current psychiatric competencies are no longer sufficient. Specific rotations in SUD and concurrent disorders are still important to acquire competencies, but clinical experiences and training in SUD need to occur on a longitudinal basis. The concern is there may be a discontinuity between learning experiences, as many clinical preceptors may have relatively limited evidence-based knowledge, skills and attitudes for the management of SUD. As such, psychiatry residents need to work with clinical preceptors with expertise in SUD. Programs need to identify local psychiatric leaders to provide preceptorship and use family physicians or other physicians with expertise in SUD, especially if there is a limited number of psychiatrists with SUD expertise available. Longitudinal experiences, such as those for psychotherapy training, may be required for SUD. Programs also need to be able to offer elective/selective rotations in SUD. Training for clinical preceptors in the management of SUD will need to be prioritized by psychiatry departments to ensure appropriate evaluation of EPAs and teaching of evidence-based practices for appropriate feedback and coaching.
The current CBD plan for psychiatry as of 2020 specifically identifies the management of SUD in EPAs 1, 2, and 3 in the FoD and EPAs 1, 6, and 8 in the CoD. As residents need not complete EPA2 in FoD involving a SUD patient, or EPA6 in CoD for psychotherapy using MI, these EPAs are included under the supplemental materials section should a resident do so. In this regard, the required EPAs only cover some of the recommended curriculum elements, not all. Management of SUD in the FoD could occur during initial PGY-1 medical rotations, inpatient psychiatry and emergency psychiatry rotations, with those in CoD occurring during outpatients, chronic care, consultation-liaison, and longitudinal-based SUD or concurrent disorder rotations. Paralleling the scoring of objective structured clinical examinations (OSCEs) for the RCPSC certifying exams, a rubric is proposed for the knowledge, skills and attitudes for each EPA with the aim of improving evaluation consistency both within a program and nationally, as well as providing a basis for feedback and coaching.
Entrustable professional activities (EPAs)
Managing intoxication or withdrawal states commonly encountered in clinical psychiatric practice is a critical foundational competence. Alcohol withdrawal is common and is associated with significant medical and psychiatric morbidity, so should be evaluated. Identifying substance intoxication/overdose could be a specific substance or a mixed drug overdose. In all likelihood, these EPAs will be addressed in early training experiences during the psychiatry residency such as in emergency psychiatry, internal medicine or inpatient psychiatry.
For competence at the FoD level of training for alcohol withdrawal, the resident should demonstrate the following:
Identification of the patient in or at significant risk for alcohol withdrawal based on history (e.g., severity and duration of alcohol use and history of prior withdrawal) and physical manifestations (e.g., vital signs and stigmata). Communication that demonstrates a patient-centred approach, facilitating patient trust and autonomy, and characterized by empathy, respect and compassion. Recommendation of appropriate monitoring for alcohol withdrawal for persons at risk for significant withdrawal, including the initiation of the CIWA-Ar with triggers for benzodiazepine administration and discontinuation when appropriate. Recommendation of benzodiazepines pre-emptively to prevent development of severe withdrawal in a person with a known history of severe withdrawal, delirium tremens or seizures. Initiation of intramuscular or intravenous thiamine to prevent the development of Wernicke's encephalopathy. Recommendation of appropriate addiction treatment resources occurring after management of acute withdrawal as detoxification alone does not change alcohol use disorder outcomes. Application of clinical and medical sciences to manage the intoxication or overdose state with appropriate precautions for associated complications (e.g., airway/breathing risk, seizure potential and arrhythmia risk). If an opioid overdose, urgent use of naloxone. Communication demonstrates a patient-centred approach, facilitating patient trust and autonomy, and characterized by empathy, respect and compassion while maintaining the safety of the resident, patient and other personnel present. Demonstration of an appropriate medical assessment to determine the type of substance or substances causing the intoxication/overdose and any associated complications related to the substance use. Differentiate a stable from unstable intoxication or overdose state, the latter requiring pre-emptive approaches and appropriate assistance. Awareness of the limits of the resident's own professional expertise. Recommendation of appropriate addiction treatment resources occurring after management of acute intoxication/overdose.
For the observation of achievement for substance intoxication or overdose, the substance type need not be specific and maybe a mixed substance presentation. For competence at the FoD level of training for substance intoxication or overdose, the resident should demonstrate the following:
For competence at the FoD level of training, the resident should demonstrate the following:
Develop and implement a management plan that considers the severity of their SUD. Describe the setting that would be best to manage the patient's SUD considering the indications, contraindications, risks and alternatives to the SUD treatment plan. Communicate the plan using a patient-centred approach that facilitates patient trust and autonomy, characterized by empathy, respect and compassion. Prescribe or help coordinate prescription for first-line pharmacotherapy for alcohol, tobacco or OUD, if indicated. Develop a basic management and follow-up plan for the person's SUD.
Assessment and diagnostic practices are expanded from those demonstrated in the FoD EPA2 and EPA3, applied to a patient presenting with a more complicated psychiatric presentation, with greater depth to the assessment to better differentiate substance-induced symptoms from primary psychiatric disorders and a more comprehensive treatment plan. Sufficient competence includes the following:
Questioning about SUD with open-ended questions asked in a nonjudgmental manner that invites honest and full disclosure. Questioning about SUD should be tied to the context of the patient's presentation. All patients should be screened for substance use, covering the major classes of substances including alcohol, cigarettes/vaping, cannabis, stimulants, sedative-hypnotics, opioids, hallucinogens, prescription medications and over-the-counter medications, as appropriate. Screen for behavioural addictions when indicated, such as when mentioned by the patient or if they commonly occur with certain substances, co-morbid psychiatric states or other historical clues. If substance use is identified, the resident should determine when substance use started, when use became regular, when use became problematic, maximal amounts used, current use, consequences of use, whether criteria are met for a SUD and prior treatment history. This should be done for each substance, time permitting. A timeline of substance use should be identified correlating patterns of use with psychiatric symptoms to help differentiate substance-induced from primary psychiatric disorders. Stage of change should be identified for each substance meeting criteria for a substance use disorder (e.g., precontemplative, contemplative, preparatory, action and remission). The screening and assessment questions should enhance engagement in the interview and treatment process. Develop and implement a management plan that considers the patient's stage of change, severity of their substance use disorder(s), medical and psychiatric co-morbidity, state of intoxication and risk of withdrawal. Describe the settings that would be best to manage the patient's substance use disorder and recovery needs considering the least intensive treatment setting that meets the patient's needs and considers available treatment environments. Describe the indications, contraindications, risks and alternatives to the substance use disorder treatment plan, including potential barriers. Communicate the plan using a patient-centred approach that facilitates patient trust and autonomy, and is characterized by empathy, respect and compassion. Prescribe or help coordinate prescription for first-line pharmacotherapy for alcohol, tobacco or OUD, if indicated. Develop a management and follow-up plan for the patient's needs for SUD treatment.
Apply knowledge of pharmacodynamics and pharmacokinetics at various developmental stages. For benzodiazepines, this would particularly relate to half-lives of different benzodiazepines, dose equivalencies, changes with aging and drug–drug interactions. For OAT, familiarity with buprenorphine, naloxone and methadone, awareness of common drug interactions, half-lives and the effect on electrocardiogram QT interval would be of particular importance. Describe the indications, contraindications, risks and alternatives for a given treatment plan. For benzodiazepines, this would include the risk of problematic use and BUDs, cognitive impairment and falls as priorities. For OAT, this would include the presence of a moderate to severe OUD, awareness of different treatment options (predominantly buprenorphine/naloxone or methadone), factors to consider if continuing or switching a specific OAT medication, adverse effects and risk of overdose. Assess and monitor treatment adherence and response to pharmacotherapy. Assess potential interactions between pharmacotherapy for a SUD and common psychiatric medications. Establish plans for ongoing care. For benzodiazepines, this would emphasize a short duration of treatment, lowest possible dose, discontinuation if problematic use and approaches to deprescribing (e.g., gradual tapering, switching to agents with a longer half-life and use of other medications to facilitate the deprescribing of a benzodiazepine). For OAT, it requires ensuring appropriate ongoing follow-up care with no gaps in prescribing. Document prescriptions accurately in the patient's medical record including rationale for decisions. Facilitate access to appropriate medications (e.g., via an OUD treatment program).
This EPA focuses on pharmacological management and includes the prescription and monitoring of medications. Managing does not include starting and monitoring, where the focus is on reviewing, safe prescribing, deprescribing, switching, augmenting and/or discontinuation. It is suggested for benzodiazepines that the EPA focus on identifying problematic benzodiazepine use and limiting, tapering or deprescribing. Managing OAT is suggested to focus on the maintenance of OAT where the resident will be aware of the indications and evidence for OAT in the treatment of OUD, risks and benefits of OAT, typical medications used and their dosing, common adverse effects and interactions with common psychiatric medications. Exposure to problematic benzodiazepine use and benzodiazepine use disorders (BUDs) will likely be common during a variety of rotations, but exposure to OAT may likely be limited to a SUD-specific rotation or potentially on a consultation-liaison or inpatient rotation. If programs struggle with opportunities for residents to meet this EPA, use of simulation or OSCEs could be an option. Sufficient competence for this EPA should be demonstrated by the following:
Conclusions
Further development of training in SUD within psychiatric residency programs needs to be a priority given the high prevalence of SUD in Canada, comorbidity with major psychiatric disorders and shortage of SUD treatment providers. The new training requirements provide an opportunity for residency training programs to enhance the competence of our future psychiatrists in treating SUDs. It is hoped that these updated curriculum guidelines will facilitate the expanded knowledge, skills and attitudes in SUDs for psychiatry residents, begin to address the often-unmet needs of concurrent psychiatric and SUD patients and improve overall psychiatric care in Canada.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437241232456 - Supplemental material for Training in Substance Use Disorders, Part 2: Updated Curriculum Guidelines
Supplemental material, sj-docx-1-cpa-10.1177_07067437241232456 for Training in Substance Use Disorders, Part 2: Updated Curriculum Guidelines by David Crockford, MD, FRCPC; Anees Bahji, MD, FRCPC; Christian Schutz, MD, FRCPC; Jennifer Brasch, MD, FRCPC; Leslie Buckley, MD, FRCPC; Marlon Danilewitz, MD, FRCPC; Simon Dubreucq, MD, FRCPC, MSc; Michael Mak, MD, FRCPC; Tony P. George, MD, FRCPC in The Canadian Journal of Psychiatry
Supplemental Material
sj-docx-2-cpa-10.1177_07067437241232456 - Supplemental material for Training in Substance Use Disorders, Part 2: Updated Curriculum Guidelines
Supplemental material, sj-docx-2-cpa-10.1177_07067437241232456 for Training in Substance Use Disorders, Part 2: Updated Curriculum Guidelines by David Crockford, MD, FRCPC; Anees Bahji, MD, FRCPC; Christian Schutz, MD, FRCPC; Jennifer Brasch, MD, FRCPC; Leslie Buckley, MD, FRCPC; Marlon Danilewitz, MD, FRCPC; Simon Dubreucq, MD, FRCPC, MSc; Michael Mak, MD, FRCPC; Tony P. George, MD, FRCPC in The Canadian Journal of Psychiatry
Footnotes
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.