
Abstract

Introduction
On March 17, 2021, the Canadian parliament passed Bill C-7, 1 an amendment to the Criminal Code exemptions relating to the provision of medical assistance in dying (MAiD) by medical practitioners. This bill established a separate set of procedural safeguards for individuals whose natural death is not reasonably foreseeable and made some amendments to the safeguards that apply in the case of individuals whose natural death is reasonably foreseeable. It also amended the eligibility criteria by temporarily disqualifying mental illness as an “illness, disease or disability” for the purpose of determining eligibility for MAiD. Under the revised legislation, the provision of informed consent to MAiD remains a key eligibility criterion. Additionally, the capacity to consent to health care decisions and voluntariness are eligibility criteria. Psychiatrists may be called upon to assess these aspects where there is a concurrent mental illness, and (after March 2024) where mental illness is the sole underlying condition.
The Canadian Psychiatric Association lias a position paper on informed consent to treatment 2 which articulates the ethical imperatives, clinical principles and legal issues related to informed consent to treatment in psychiatric practice. However, the highly consequential and irreversible nature of MAiD consent decisions, the ethical sensitivity and the perceived complexity of the clinical considerations therein have compelled the CPA to publish this paper.
The current paper addresses the evaluation of decisional capacity and voluntariness in those who are 18 years of age or older in the context of MAiD where there may be a concurrent or sole mental disorder underlying the request for MAiD.
The Canadian Context: Federal MAiD Legislation
On March 17, 2021 Bill C-7 An Act to amend the Criminal Code (Medical Assistance in Dying) 2 came into force in Canada. This law means that when a physician or nurse practitioner writes a lethal prescription that a patient can self-administer, or when they provide medications intravenously to end a patient’s life, they will not be criminally charged, providing the patient meets all the eligibility criteria as defined in the statute (see Table 1 for the relevant section of the Criminal Code of Canada). 3 Persons with mental illness as their sole underlying medical condition were temporarily excluded until March 17, 2023 to allow for further consultation by the federal government. This exclusion was then further extended until March 17, 2024. At that time, unless further extensions or amendments to the law occur, persons with mental illness as their sole underlying medical condition will be eligible to receive MAiD, assuming they meet all the eligibility criteria.
Eligibility for Medical Assistance in Dying.
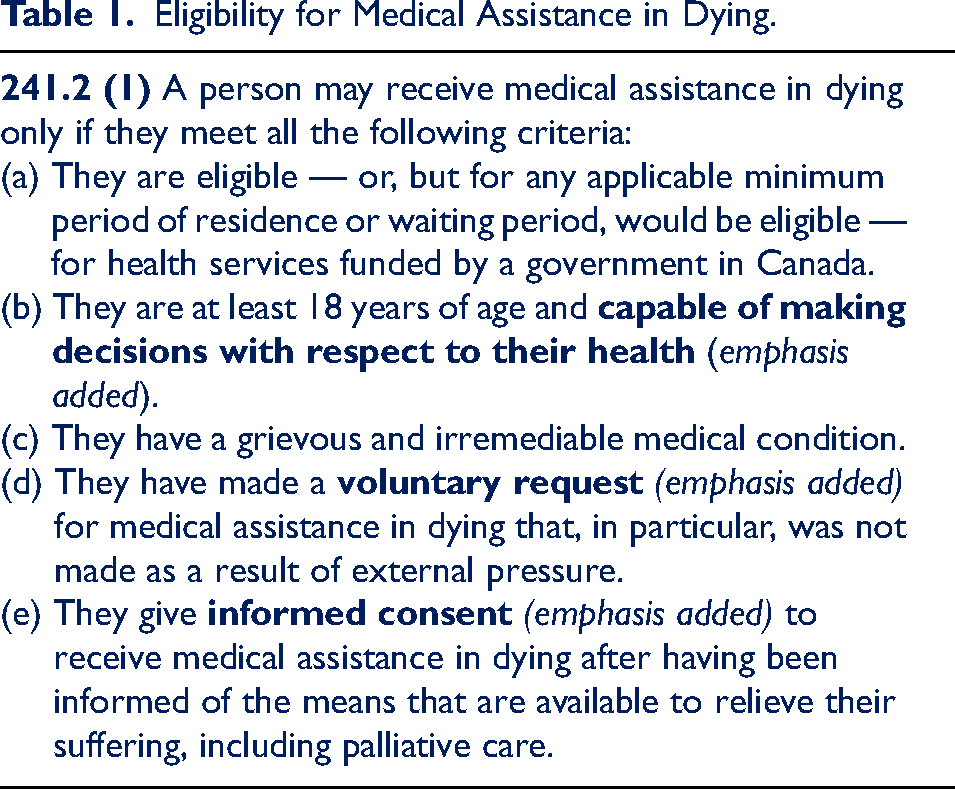
It is noteworthy that in addition to the decisional capacity element embedded within the informed consent to MAiD process, the MAiD eligibility criteria also specifically require that the adult be capable of making decisions with respect to their health. Similarly, voluntariness (which is also an element of consent) has also been singled out in the federal legislation as an element that requires special consideration. This underscores the clinical imperative for MAiD assessors and providers to formally turn their minds to the assessment of decisional capacity and voluntariness for every adult who seeks a MAiD procedure, as part of the assessment of the eligibility criteria.
The failure of a MAiD assessor or provider to properly assess the eligibility criteria could result in multifaceted liability, including, but not limited to criminal sanctions, claims of negligence by surviving relatives, professional discipline and/or revocation of hospital privileges. The appropriate assessment of the eligibility criteria for MAiD is not only a legal requirement but is also an ethical and clinical imperative. The assessment of decisional capacity and voluntariness are core features of any MAiD assessment.
The MAiD Eligibility Assessment and the Role of the Psychiatrist
Under the current federal legislation, two independent MAiD assessors (physician or nurse practitioner) must assess the legislated elements and confirm that the patient meets the eligibility requirements for MAiD. 4 If natural death is not reasonably foreseeable, one of the two practitioners confirming eligibility must have expertise in the condition that causes the patient’s suffering. 5 In cases where neither practitioner has sufficient expertise, one of the two assessors must consult with another practitioner with that expertise and share the results with the other assessor. 5 In this context, a psychiatrist may be asked to provide an opinion regarding the patient’s decisional capacity or voluntariness or aspects of irremediability that will be incorporated into the MAiD eligibility assessment. Unless the psychiatrist is also conducting the MAiD eligibility assessment, the position in law is that they are providing expert assistance to the primary MAiD assessor, similar to other medical consultations, and a duty of care is owed. This duty of care arises because the psychiatrist has expert knowledge of the patient and options for care and knows that the advice provided to the MAiD assessor will be relied upon to draw conclusions related to the eligibility criteria. Like with other independent third-party capacity assessments, the treating psychiatrist should avoid providing decisional capacity assessments for their own patients, due to the risk of bias. The requirement of independence of the two assessors is delineated in the federal MAiD statute. 6
It should be noted that “expertise” is not defined in the federal legislation, but the CPA’s position is that where the mental disorder is the sole underlying medical condition motivating the MAiD request, at least one of the two independent MAiD eligibility assessors should be a psychiatrist.
Psychiatrist-MAiD assessors and psychiatrists whose expertise is sought to supplement the MAiD eligibility assessment must use their clinical knowledge, skills, training, expertise and experience to evaluate the legislated criteria. At all times, they must be transparent about any medical uncertainty, particularly as it may relate to the limits of current scientific knowledge regarding assessment processes, treatment efficacy and prognosis. Indeed, this forms the basis of informed consent: capable patients have the right to decide what is, or is not, done to their own bodies, and they can only do this when they are fully and transparently informed about the prognosis for relief of their suffering, and the risks and benefits of MAiD in their individual health circumstances.
Elements of Consent
Health care and consent to medical procedures such as MAiD fall under provincial jurisdiction. Each province and territory has different legislation related to informed consent to treatment and the elements of consent may be slightly different from province to province, with most legal requirements being at a lower level than medical ethical standards. However, all provincial and territorial jurisdictions have in common the following minimal elements that are required for consent to be valid and legally binding; the consent must be:
given by a patient who has who has been
Thorough documentation of each of these elements indicates that they have been actively considered and appropriately weighed. The current paper addresses only the first and second elements: the assessment of decisional capacity to consent to MAiD, and voluntariness. The principles apply irrespective of whether the individual seeking MAiD has a concurrent or sole underlying mental condition.
Ethical Considerations
The ethics of MAiD are challenging because it sets in opposition fundamental values which are at the core of medical practice. However, the requirement that patients have decisional capacity and be able to act voluntarily and without influence has the same ethical underpinnings in the context of MAiD legislation as with other consent decisions. Ethically, the aim is to safeguard individual autonomy and to preserve freedom of choice, while at the same time protecting vulnerable individuals from making highly consequential and irreversible decisions when they are not capable to do so. Psychiatrists conducting MAiD eligibility assessments or those who provide consultations with respect to aspects of the consent process have an ethical (and legal) obligation to ensure that that the patient’s decision-making capacity and voluntariness with respect to their choice to pursue MAiD is not substantially impaired by their mental condition.
Psychiatric symptoms are not unexpected when individuals are facing terminal, life threatening or chronically debilitating conditions. 7 Symptoms of mental illness can impact decisional capacity and voluntariness in subtle and not-so-subtle ways.8,9–11 For this reason, a formal and thorough evaluation of these elements should be conducted in every case, but especially where mental illness is a sole or concurrent condition.
Psychiatrists who participate in MAiD assessments must carefully consider and document the impact of psychiatric symptoms, including the specific manner and degree to which they impact decisional capacity and voluntariness. They also have a duty to intervene where necessary and appropriate. For example, in the case of an individual under assessment whose desire to die is thought to be based on situational stressors or remediable aspects of illness, psychiatrist MAiD assessors are expected to follow relevant protocols to assure the person’s safety. However, in general terms, infringements on individual autonomy should be exercised with caution unless there are clear indicators of impairment in decisional capacity.
Psychiatrists should carefully consider the degree to which fulfillment of the legal elements of MAiD eligibility satisfactorily fulfills their medical ethical obligations. Each case will be unique, and some assessments may be nuanced and difficult both clinically and ethically. Here, seeking the advice of trusted colleagues who are independent of the case, yet knowledgeable about the clinical and ethical concerns, may lead to clarity.
Psychiatrists may face many ethical challenges related to the availability of MAiD in the context of mental illness, and they have the right to exercise conscientious objection to participating in MAiD eligibility assessments; however, they are expected to effectively facilitate referrals in the case of a request. Treating psychiatrists are expected to continue to provide ongoing care while the patient is undergoing a MAiD assessment by an independent psychiatrist assessor. Recognizing and addressing the potential for moral injury and psychological distress in colleagues who are involved in MAiD assessment/provision or whose patients choose MAiD is something that is an ethical imperative for the entire medical profession. Similarly, appropriate postvention support of those who are impacted by a MAiD death also requires the attention of the profession.
Part 1: Decisional Capacity
Decisional Capacity Defined
The dictionary definition of capacity is “the ability or power to do or to understand something.” 12 Decisional capacity is not a measure of the information that is actually held; it is a measure of the potential for holding information. While the difference between capacity to understand and appreciate and actual understanding or appreciation is easily stated, it may be less easy to apply in practice. Capacity is an abstract concept. The primary means of ascertaining capacity, in most contexts, is to look at what an individual in fact says and does, and how they make decisions in relation to a specific issue. 13
From a clinical perspective, decisional capacity is usually defined as an individual’s ability to receive, understand, hold, process and apply information to their situation that would enable them to make and communicate a decision relevant to a specific issue at a specific point in time. It involves a clinical assessment using the “understand/appreciate/communicate” clinical framework 8 which is outlined in more detail in the sections below.
From a legal perspective, all provinces and territories have legislation and regulations that relate to healthcare decisions, that apply equally to MAiD decisions. It is expected that psychiatrists involved in MAiD be thoroughly familiar, not only with MAiD legislation, but also with the provincial or territorial statutes that relate to health-care decisions.
Key Elements of Decisional Capacity
Presumption of Decisional Capacity, Capacity Thresholds and Causative Nexus
In the law as it relates to medical decision-making, the starting point is that all adults are presumed to be capable of making their own decisions. The onus is on the assessor to prove incapacity; it is not on the patient to prove capacity. 13 This presumption of capacity can only be displaced by medical evidence to the contrary. The standard of medical proof that must be achieved is “on the balance of probabilities.” Accordingly, it will always be for the assessor to prove that it is more likely than not that the person lacks capacity.
To date, no case law or government policy has set the legal threshold of capacity that is required to make a decision regarding MAiD (with or without a mental illness), and at the moment, it is the same threshold as for other medical decisions. However, it is generally agreed among psychiatrists that complex decisions require more sophisticated mental abilities to “understand” information relevant to the decision and to “appreciate” the implications of the decision. This is clearly the case in the decision to choose MAID, especially when death is not reasonably foreseeable. As such, from an ethical and medico-protective standpoint, the threshold of capacity for MAiD decisions may be higher than the current legal threshold. A clinically cautious and ethically dutiful approach is warranted.
The legal threshold of capacity to consent to psychiatric treatments in the context of provincial mental health legislation was outlined by the Supreme Court of Canada in the Starson 13 decision. This case did not address capacity to consent to medical treatments and interventions and should not be used as a reference point for MAiD consent decisions. There is, however, the requirement in the federal MAiD legislation that the person be “capable of making decisions with respect to their health,” which includes psychiatric treatments.
Finally, where capacity is in question, there must be a causal nexus between symptoms of mental disorder and one or more of the elements of decisional capacity. The assessor must be satisfied that the inability to make a decision is because of an impairment of the mind or brain and should be able to provide cogent medical evidence of the manner in which this disturbance impairs decision-making capacity.
Assessment of Decisional Capacity: Task, Context and Temporally Specific
The assessment of decisional capacity is task specific, context specific and temporally specific.
Task-specific refers to the kind of decision that needs to be made (in this case, the legislated task is the ability to make decisions related to the person’s health and decisions related to MAiD). It is important to remember that different decisions require different mental capabilities. For example, do not assume that a person who lacks the capacity to manage their own finances will also lack capacity to consent to MAiD. They are separate tasks, requiring separate but overlapping mental abilities, and must be assessed separately. Similarly, some patients may be capable of making decisions related to some aspects of their health (e.g., the treatment of cancer) but may lack capacity to consent to MAiD (e.g., by virtue of a delusion that death will not impact them).
Context specific refers to the situation within which the decision is being made. When a person’s situation changes, their capacity may change as well. For example, sedation may impair a person’s attention and ability to absorb information relevant to making a decision, whereas changing this context may improve their understanding.
Importantly, consideration of contextual factors is not limited to physical surroundings. A decisional capacity assessment should seek to understand and apply the patient’s value system as well as the degree to which the person’s structural and life circumstances may be impacting their decision-making. Here, linguistic and cultural barriers may be highly relevant. 14
In the assessment of capacity to consent to MAiD, it is very important to differentiate a decision that seems foolish or “wasteful of a life” from one that the patient does not have the capacity to take. There is a difference between an unwise decision and one in which an individual does not have the mental capacity to take, 13 and it is important to respect that space and to ensure that it is preserved, for it is within that space that an individual’s autonomy operates.
Contextual factors are not limited to the assessee: the experience, values and cultural competence of the assessor can also be contextual factors that can impact the assessment of decisional capacity. 15 Special care and attention should be paid when assessing people in historically marginalized groups, including monitoring one’s own implicit biases.
Temporally specific refers to the fact that capacity can fluctuate over time, depending on the underlying impairment that is affecting capacity; repeat evaluations may be required. For example, a person with “sundowning” related to dementia may have periods of fluctuating lucidity that may impact a capacity assessment. In the case of fluctuating capacity, “windows of lucidity” must be sufficiently large for the person to be able to make capable decisions throughout the entire timeframe that the MAiD consent decision is occurring.
Optimization of Assessment Setting
The patient should not be considered to lack decisional capacity unless all practical steps have been taken to help the patient demonstrate their capacity and have failed.
Communication should recognize diversity of culture, language, literacy and verbal skills present within the Canadian population. Interpreters may be necessary for non-English and/or non-French speakers, and a translator skilled in medical terminology is ideal for the purpose of transmitting accurate (verbatim) information. Translation should not be done by family members, as incomplete or misleading information may be transmitted. However, a patient’s desire to be accompanied by a support person and/or animal, family member or patient advocate during such a discussion should be accommodated but should never include allowing others to respond on the person’s behalf.
Considerations of optimal time of day and appropriately conducive examination settings should also be made. Avoiding the use of medical jargon and complicated explanations can sometimes facilitate understanding.
The Clinical Assessment of Decisional Capacity
The validity of unstructured determinations of capacity is problematic. Previous studies have shown that even the most skilled medical professionals may face difficulty when making capacity determinations, often leading to frequent disagreements and low inter-rater reliability. 16
Attempts have been made in academic circles to structure capacity assessments and identify specific criteria or standards for decisional capacity assessment. 17 Numerous standardized instruments have been developed for this purpose 18 (for example, the Aid to Capacity Evaluation 19 and the MacArthur Competence Assessment Tool—Treatment 20 ). Although informal MAiD consent tools are used in some hospitals 21 and organizations 22 to date, no standardized assessment tools have been validated (with basic psychometric properties such as inter-rater and test-retest reliability, as well as predictive or concurrent validity, error rates, etc.) specifically for the assessment of capacity to consent to MAiD. Currently, we do not recommend relying on this sort of tool or instrument as the sole contributor to determine decisional capacity. However, this is an area that is ripe for interested researcher-clinicians.
In the absence of validated standardized assessment tools, the CPA suggests that a structured clinical approach be adopted when assessing a patient’s decision-making capacity in the context of MAiD legislation. It can be conceptualized as consisting of two components.
First, there should be a medical (diagnostic) evaluation to rule out temporary or reversible impairments of, or disturbances in functioning of the mind or brain that may affect capacity. This could include medical conditions causing confusion (e.g., hypoxia, infection, electrolyte imbalance, medication adverse effects); drowsiness (e.g., the use of analgesics, psychotropic medications or sedatives); disorientation (e.g., sundowning in relation to dementing processes); diminished ability to think or concentrate (e.g., associated with acute or chronic depression). If any of these reversible impairments are present, they should be remediated and the assessment should be conducted on another day.
Second, a formal interview with the adult should be conducted using a cognitive and functional inquiry methodology to assess the capacities required of an adult in relation to health care decisions generally, and MAiD decisions specifically.
The basic elements to be assessed in relation to decisional capacity are:
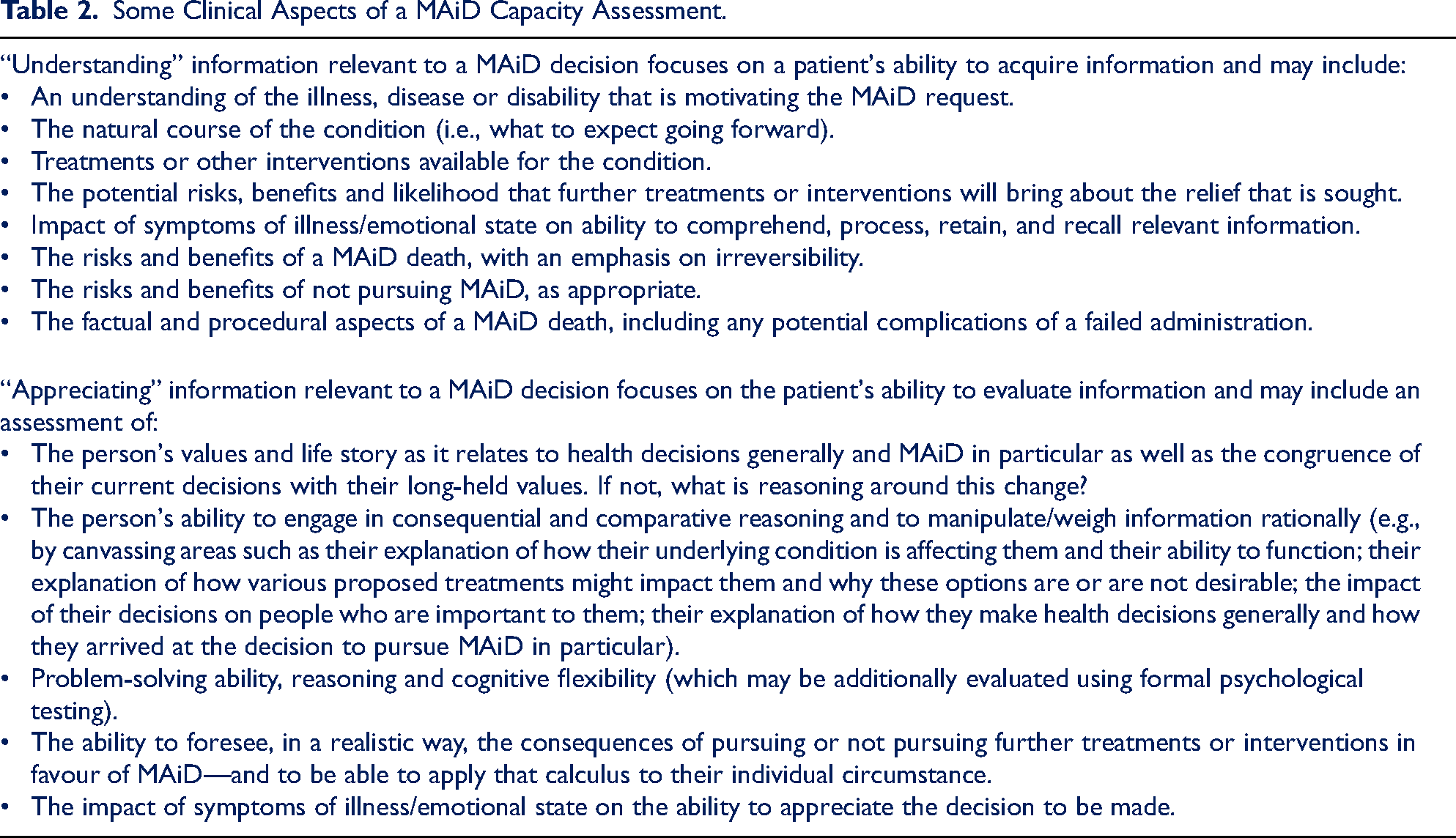
Any determination of incapacity must relate back to one of these three elements, which are reviewed in the sections that follow. Table 2 outlines some clinical aspects of a MAiD capacity assessment.
Some Clinical Aspects of a MAiD Capacity Assessment.
Understanding Information Relevant to a MAiD Decision
“Understanding” requires the cognitive ability to comprehend, retain and process relevant information and necessitates at least a working knowledge of one’s health circumstances, and of the MAiD procedure itself. Usually, the assessor is not starting with a “blank canvas.” Most individuals seeking MAiD will have been through a variety of treatment modalities and will likely have at least some understanding of their underlying diagnosis(es), the treatments they have attempted, the impact that this has had on their symptoms and overall functioning, and their prognosis for improvement. However, where this is lacking, the adult whose capacity is under scrutiny must be given “relevant information” about which available treatments or support options have not yet been provided, and the likely risks, benefits and prognosis associated therein, so that their capacity to weigh up those options can be fairly assessed.
It is entirely permissible for the assessor to provide relevant factual information to the patient, such that they have an accurate basis upon which to make a decision to pursue MAiD. The modified objective standard of disclosure of information (i.e., disclosure geared to what the average prudent person, the reasonable person in the patient’s particular position, would agree to or not agree to, if all material and special risks were made known to them) as articulated in Hopp v. Lepp 23 and Reibl v. Hughes, 24 continue to apply. In the case of treatment resistant conditions, this often requires specialized knowledge on the part of the assessor, therefore it is essential that the breadth of treatment options and interventions, as well as the likelihood of success, be canvassed with the appropriate specialist or subspecialist so this information can be conveyed to the patient under assessment.
The patient must also have a proper understanding of the MAiD procedure itself, the practical administration options (self-administered; physician administered) and venues, as well as possible complications in cases of failed administration, and finality of outcome. It goes without saying that this must be a reality-based understanding, unencumbered by beliefs that are not supported by medical evidence. Additionally, the person being assessed must be able to retain enough information for sufficient period to be able to make a decision at the time of the MAiD procedure. This is especially important when dealing with those who have fluctuating cognitive abilities.
The assessor must also consider the manner in which symptoms of illness impact the patient’s ability to understand information relevant to making a decision. Numerous cognitive symptoms such as indecisiveness, inability to think or concentrate, impaired memory and reduced processing speed may negatively impact a person’s ability to properly consider options for care. 8 Similarly, delusional misinterpretation of one’s circumstances or of the MAiD procedure itself may significantly impair the patient’s ability to understand information relevant to a decision. Psychological testing may help to elucidate the degree to which the person can comprehend, process, retain and recall information in a general sense, and can lend weight to clinical/ bedside cognitive testing, but is not routinely required to determine capacity.
Appreciation of Information Relevant to the Decision to Pursue MAiD
“Appreciation” is a broader concept than “understanding” and includes both a cognitive and affective component, 13 because our decisions are coloured by our emotions and psychological state. The “appreciation” aspect of the test is the capacity to rationally engage in the decision-making process itself—to be able to foresee, in a realistic way, the consequences of pursuing or not pursuing a particular treatment or intervention—and to be able to apply that calculus to one’s own circumstance.
The assessment of “appreciation” includes the assessment of reasoning. Rational thinking involves the ability to understand and evaluate alternatives, to make judgements that are relatively free of biases, and appropriately appraise the consequences of decisions.
Like the concept of “understanding,” “appreciation” does not require agreement with a particular conclusion, professional or otherwise. The assessor must be very careful to ensure that the way the patient applies their own values and outlook to their medical decisions is not conflated with a functional inability to use and weigh information. A patient may look at the pros and cons of treatment and arrive at a different conclusion than the medical experts. However, the way that they assess and weigh those pros and cons must be intact. In this regard, it is important to understand which pieces of information the patient is using to make their decision and the weight that they are applying to each piece. In some cases, it may be difficult to identify whether the patient is using a piece of relevant information and granting it no weight, or whether they are failing to use that piece of information at all.
Another aspect of the “appreciation” test is the degree to which the person’s emotions or psychological state impacts their decisions. As noted earlier, certain forms of mental illness may disturb the decision-making process in subtle and difficult-to-detect ways. Usually, these mental disorders tend to impact the person’s assessment and interpretation of risk and probabilities,25,8 yet leave cognition and communication intact, allowing the patient to express themselves in a seemingly logical, coherent and fluent manner, which can be convincing to inexperienced or careless capacity examiners.
For example, individuals with depression tend to seek out less information to help them with problem solving and make use of fewer resources, 26 possibly impacting their willingness to try certain treatments. They also have difficulty projecting themselves into the future related to their loss of hope, undermining their ability to make future oriented decisions.27,28 Similarly, cognitive distortions and other subtle symptoms such as hopelessness, helplessness, pessimism and apathy in patients with depression may distort the realistic appraisal of the likelihood of success of future treatments but may still allow the patient to be able to express their views in a coherent and logical manner. These symptoms could cause a person with depression to view the expenditure of further treatment efforts as futile, overly complex or too effortful, whereas this may not be the case. Although there is abundant research on the influence of cognitive distortions on decision-making capacity generally, 29 research about its specific influence in end-of-life decisions is needed. 30
Similarly, patients with longstanding eating disorders may be able to express clear and logical-sounding reasons for avoiding certain foods or rejecting certain treatments and for seeking MAiD to end their suffering, whereas their decisional incapacity may relate to the narrow area of their appreciation of food intake, nutritional requirements, exercise needs and body image. 31 A nuanced and clinically careful approach is required.
Another assessment challenge is when a person with impairments in executive functioning (e.g., an acquired brain injury, certain developmental disorders or dementia) can give superficially coherent answers to questions, but it is clear from their actions that they are unable to carry into effect the intentions expressed in those answers. Here a key question is whether the person is aware of their own deficits or the mismatch between their ability to respond to questions in the abstract and to act when faced with concrete situations.
Communication of the Decision
To have capacity, the person must be able to make and express a choice. This requires only a residual ability to communicate, providing the person can make themselves understood (e.g., by talking, writing, using sign language or any other means). A total inability to communicate precludes capacity. 8 This may be relevant when conducting capacity assessments on patients with chronic progressive neurological conditions.
The expression of the choice should be stable and enduring—that is, consistent and predictable over time, and declared in a definitive way.
Documentation of the Assessment of Decisional Capacity
In all cases, it is important to document that a robust assessment discussion that took place. This should include documentation of the patient’s understanding of the treatment options, interventions or supports and services available to the patient, the risks and benefits of those modalities, as well as their reasons for choosing MAiD over available alternatives. Some aspects that should be considered are presented in Table 2.
The causal link between the person’s mental disorder and the elements of capacity should be carefully documented. In other words, you must “show the math.” Psychiatrists must not assert an opinion about decisional capacity unless it is properly and logically supported by the medical evidence.
Disagreements over the relevance of psychiatric symptoms to decision-making are common, and may relate to the timing of the assessment, or even the psychiatrist’s understanding of the potential relevance of such symptoms. 8 To date, this is an area that has limited research. 8 Full transparency around the limitations of the assessment and degree of confidence of the psychiatric opinion is expected at all times.
A person who is psychiatrically assessed as lacking the capacity to consent to MAiD may request a second opinion from another capacity assessor. The legislative history giving rise to the Criminal Code amendments permitting MAiD reveals that Parliament considered, and rejected, a role for judges in the pre-approval or review of MAiD eligibility assessments. Parliament made clear that role rests with approved health-care assessors. 32 However, bereaved family members may later launch civil suits when they feel that the MAiD eligibility assessment was inadequate. It is in everyone’s interest to ensure that the assessment is robust, and that clinical documentation is sufficient to demonstrate that the appropriate issues were considered and examined.
Part 2: Voluntariness
Voluntariness, like decisional capacity, is an element of consent. 33 In addition, voluntariness is an eligibility requirement in its own right. In all circumstances, consent to MAiD decisions must be free from conditions, circumstances or external influences that may limit, influence or control choice. Psychiatrists who are MAiD assessors must consider the voluntariness of the MAiD request and must be cognizant of any limitations on voluntariness that may affect consent.
There are four potential barriers to voluntariness in the context of MAiD. Each must be actively considered and assessed.
Coercion
Coercion is the practice of persuading someone to do or to not do something by using force, pressure or threats, or by unjustly curtailing their options. In the context of MAiD, threats to involuntarily detain a patient in hospital or to change their decision-making capacity status based solely on their decision to pursue MAiD, are examples of coercion. However more subtle examples exist. For example, subtle pressures that relate to the cost of care or the burden of care may also come into play (e.g., family threat of placing the individual in nursing home or complaints of caregiver exhaustion actively figuring into the patient’s calculus).
We do not yet know whether patients feel unduly influenced when their own physician suggests MAiD as a treatment alternative, but this is not outside the realm of possibility. For example, suddenly suggesting MAiD to a patient who has not previously considered this intervention in the context of their care may be viewed as coercive, because the treating physician is in a fiduciary position of trust, authority and confidence (e.g., “If my psychiatrist thinks my case is hopeless, I guess it must be”). For this reason, raising MAiD as an alternative to ongoing psychiatric care is not recommended at this time.
Undue External Influence
Undue external influence is when a third party (e.g., family, friends, others) manipulates, pressures or uses excessive persuasion that causes the individual to act (or refrain from acting) in a manner that would benefit the influencer. The benefit is often financial but could also relate to other material or psychological gains, or to preserve the status quo. An obvious example is where a relative stands to benefit financially from the person’s death, and so actively encourages MAiD as an option. Less obvious examples are the active discouragement of MAiD to avoid perceived stigma of a threatened suicide, or in alignment with the personal and/or religious beliefs of the influencer.
The elderly, those who are dependent on others for care and companionship, and people whose mental functioning has declined because of their mental illness or addiction, can be particularly susceptible to undue external influence.
Undue Internal Influence
Undue internal influences are the psychological processes by which a person’s free will is constrained such that it causes the individual to act in a manner that is not consonant with their longstanding will and preferences. Symptoms of mental illness and addiction including hopelessness, self-loathing and an inability to envision a future may subtly constrain free choice, but whether they create an undue internal influence will depend on symptom severity. Various psychotic phenomena such as passivity phenomena, command hallucinations, or delusional misinterpretation of one’s circumstances or of the MAiD procedure itself may more obviously limit free choice. Addictions, eating disorders and obsessive- compulsive disorders can also create circumstances where the person’s choices are dictated by the illness, not by the person’s free will and preferences.
“No Choice” Situations
The lack of decent alternatives to accepting a particular avenue of treatment are the so-called “no choice” situations that can compel a person to choose MAiD over continuing to live in what they consider to be unacceptable life circumstances. For example, situations of inadequate housing, extreme poverty or social isolation, long term imprisonment, or no care available may cause the person to believe that there are no viable, available alternatives to MAiD, thereby undermining the voluntariness of the request. In perceived “no choice” situations, the assessor must carefully examine the impact of the social and systemic pressures to ensure that these aspects are not the driving force behind the decision. Careful gathering of collateral information through an interdisciplinary team will be essential.
Particular care and attention should be paid when assessing voluntariness in historically marginalized groups whose choices may be additionally constrained by a variety of structural and systemic inequities.
Assessment and Documentation of Voluntariness
There are currently no instruments or clinical guides available for the assessment of voluntariness in the context of MAiD (or any other treatment decisions, for that matter), but this is an area that psychiatrists consider routinely in all consent to treatment assessments. Psychiatrists should enquire about the specific factors that may have influenced the person’s decision to pursue MAiD, and actively consider the degree to which the person’s decision may or may not be impacted by barriers to voluntariness. This is another area that is ready for research.
Conclusion
The CPA affirms:
Psychiatrists have long been accepted as experts who can provide medical opinion to inform legal decision-makers dealing with the elements of informed consent, including decisional capacity and voluntariness. These are core skills of Canadian psychiatrists. Psychiatrists may be involved in the assessment of MAiD decisions in their role as MAiD assessors or as experts who are consulted about specific elements of the MAiD eligibility criteria, including the assessment of decision-making capacity and voluntariness. Psychiatrists have the right to exercise conscientious objection to participating in MAiD eligibility assessments; however, they are expected to effectively facilitate referrals or transfer care, as may be required by their medical licensing authority. Psychiatrists who choose to engage in MAiD assessments are expected to be thoroughly familiar with the legislated criteria related to MAiD, as well as applicable health care consent legislation in the jurisdiction in which they are practising. Psychiatrists who conduct MAiD assessments must carefully consider the way that psychopathology may result in functional deficits that are significant enough to prevent the person from meeting the demands of a MAiD decision-making situation, weighed in light of its serious and irreversible consequences. Clinical assessments and documentation of decisional capacity and voluntariness related to MAiD consent decisions should be robust and logically supported by medical evidence that meets a civil standard of proof (i.e., on the balance of probabilities, or more likely than not). At all times psychiatrists who are involved in MAiD assessments must be transparent about any medical uncertainty, particularly as it may relate to the limits of current scientific knowledge regarding assessment processes, treatment efficacy and prognosis. Although MAiD is now legal in Canada, this is a complex and complicated clinical and ethical area, and one that poses serious challenges. Psychiatrists should carefully consider the degree to which fulfillment of the legal elements of MAiD eligibility satisfactorily fulfills their medical ethical obligations. We also stress the importance of research in this area.