
Abstract
Objective
Co-occurring mental health and substance use disorders (concurrent disorders) lead to significant morbidity in children and youth. Programs for integrated treatment of concurrent disorders have been developed; however, there exists little guidance outlining their structure and activities. Our objective was to synthesize available information on outpatient child and youth concurrent disorders programs and produce a comprehensive framework detailing the components of such programs.
Methods
We used a four-stage critical interpretive synthesis design: (1) systematic review of published and grey literature, (2) data abstraction to identify program components and purposive sampling to fill identified gaps, (3) organization of components into a structured framework, (4) feedback from programs. We employed an iterative process by which programs reviewed data abstraction and framework development and provided feedback.
Results
Through systematic review (yielding 1,408 records total and 7 records eligible for inclusion) and outreach strategies (yielding an additional 7 eligible records), we identified 11 programs (4 American, 7 Canadian) and 2 theoretical models from which data could be abstracted. Program activities were categorized into 12 overarching constructs that make up the components of the framework: accessibility, engagement, family involvement, integrated assessment, psychotherapy for patients, psychotherapy for families, medication management, health promotion, case management, vocational support, recreation and social support, and transition services. Program components are informed by the philosophical orientation of the program and models of care. This framework considers health system factors, clinical service factors, program development, and community partnership that impact program structure and activities. Multidisciplinary teams provide care and include addiction medicine, psychiatry, psychology, nursing, social work, occupational therapy, recreation therapy, peer support, and program evaluation.
Conclusion
We developed a comprehensive framework describing components of child and youth outpatient concurrent disorders programs. This framework may assist programs currently operating, and those in development, to reflect on their structure and activities.
Introduction
Concurrent disorders, defined as co-occurring mental health and substance use disorders (SUDs), are often underrecognized, undertreated, 1 and lead to significant patient morbidity and mortality, and costs to the healthcare system.2,3 Children and youth aged 15–24 experience the highest rates of mental illness and substance use compared to any other age group, 4 as well as higher rates of concurrent disorders. 5 Previous studies suggest that more than 60% of children and youth with a SUD have a comorbid psychiatric disorder,6,7 such as attention deficit hyperactivity disorder, anxiety disorders, mood disorders, impulse control disorders, or psychotic disorders.7,8 It is estimated that while 15% of adolescents in the general population report symptoms of a substance use problem, less than 1% report receiving treatment in the past year. 9 Moreover, children and youth with concurrent disorders are less likely to access services than those without this comorbidity, due to difficulty connecting with the appropriate services, requirements of abstinence for receipt of services, and exposure to stigmatizing attitudes within the health care system.10,11 The risks of untreated concurrent disorders in young people are well established and include interpersonal difficulties, school drop-out, engagement in risky or illegal activities, hospitalization, and suicide.12-16 In contrast, treatment of concurrent disorders in children and youth has lasting effects and has been shown to reduce mental health and SUD diagnoses and emergency department visits up to three years later. 17
Parallel and sequential treatment remain the dominant models of care for concurrent disorders. In parallel treatment models, patients receive treatments for mental health and SUDs at the same time but separately and from different providers; in sequential treatment models, patients receive treatment for one disorder at a time. 10 Gaps in existing services have led to the development of integrated concurrent disorders programs in which patients receive care for both SUDs and other mental illnesses, by the same treatment teams and at the same time, providing coordinated care with consistent messaging. 18 There is evidence from randomized controlled trials that integrated treatment of major depression and SUDs in adolescents results in improvement in symptoms of both disorders.19-21 In contrast to studies of integrated interventions, studies of integrated treatment programs are limited. While integrated child and youth concurrent disorders programs exist in Canada and the United States, there are no guidelines, recommendations, or syntheses outlining the structure and activities of these programs. Using Critical Interpretive Synthesis (CIS) methodology, we aim to synthesize available information on the components of outpatient child and youth concurrent disorders programs and produce a comprehensive framework to guide programs and providers.
Methods
We employed CIS methodology to develop a framework describing components of outpatient clinical programs for children and youth with concurrent disorders. The protocol was preregistered with PROSPERO (ID CRD42021278816). Reporting of this study is in accordance with PRISMA 2020 guidelines for systematic reviews. 22 Our CIS involved four stages: (1) systematic review of published and grey literature, including outreach with existing clinical programs, (2) data abstraction to identify components across programs and purposive sampling to fill gaps identified during data abstraction, (3) organization of these components into a structured framework, and (4) feedback from programs to further develop the framework. 23
Knowledge synthesis approaches, such as the CIS, have been developed to address the limitations of traditional systematic reviews that are best suited for intervention studies. 24 These approaches have the ability to integrate rich contextual detail that is required to develop theories and frameworks that inform policy and practice. 25 A scoping review conducted by Tricco and colleagues in 2016 revealed nine knowledge synthesis methods developed for theory or framework generation. 25 As one such method, the CIS has been defined as a knowledge synthesis approach that facilitates dynamic analyses of quantitative and qualitative evidence to inform the development of new theoretical frameworks.23,26,27 Further guidance is becoming available on best practices for conducting and reporting CIS studies. 28 CIS methods allow for the flexibility required to synthesize knowledge derived from different study designs. This is exhibited through a flexible research question that can be refined throughout the research process and a flexible search strategy that is not entirely prespecified. 25 Data sources, including grey literature, are purposively sampled to fill gaps identified during the abstraction process until no new information is uncovered. 25 This is in contrast to the use of exhaustive sampling in systematic reviews to identify all possibly relevant literature. Finally, the CIS focuses on understanding reasons for differences in the literature, rather than attempting to adjust for or correct differences as seen in a traditional systematic review. 25
Search Strategy
We systematically searched MEDLINE, EMBASE, PsycINFO, Social Services Abstracts, and Social Work Abstracts from date of inception to October 5, 2021 (inclusive). To identify grey literature, we searched the Canadian Electronic Library and undertook searches on web-based search engines, and organizational websites (e.g., hospital websites). We worked with an Information Specialist at McMaster University to develop the search strategy (Supplemental Table 1). Search terms reflected the population of interest (youth, adolescent, child, pediatric, and word variations), the disorder of interest (substance use and mental health, concurrent disorders, dual diagnosis, and word variations), and the intervention of interest (service, program, clinic, model of care, and word variations). This search was restricted to English and French language publications.
We also conducted outreach with existing outpatient child and youth concurrent disorders programs in Canada to obtain grey literature (formal or informal) detailing program structure and activities. An initial web-based search was conducted to identify programs that appeared to meet our inclusion criteria, and this was followed up by electronic mail or telephone communication with program leadership. We held virtual meetings with program leadership (including clinical directors, psychiatrists, and multidisciplinary staff members) to learn more about the structure and activities of the programs and to inquire about program documents that would supplement our grey literature search. These outreach efforts led us to identify additional eligible programs that were not initially identified by web searches. In an attempt not to miss potentially eligible Canadian programs, we contacted Program Directors of Child and Adolescent Psychiatry training programs to inquire about programs in their respective provinces.
Study Selection
Inclusion criteria for this review included documents reporting on programs, clinics, and services providing care to children and youth up to 25 years of age with concurrent disorders. No minimum age limit was applied. To be eligible for inclusion, programs were required to provide access to diagnostic assessment, treatment, and follow up by a physician where required. Programs could be hospital-affiliated, academic, or community-based if they met the above criteria. Exclusion criteria included programs solely providing counseling services by mental health or addictions counsellors or programs that did not provide access to diagnostic assessment, medication treatment, and assessment or follow up by a physician where required.
All records from the search were imported into the Covidence platform 29 and duplicates were removed. Two reviewers (TR and EL) independently screened titles and abstracts for eligibility. Full-text documents were obtained for all abstracts deemed eligible and further assessed by two independent reviewers (TR and EL) in duplicate to determine final eligibility. Reasons for exclusion of full-text documents were documented in a PRISMA flow diagram (Figure 1). Disagreements were resolved through discussion or consultation with a third reviewer.
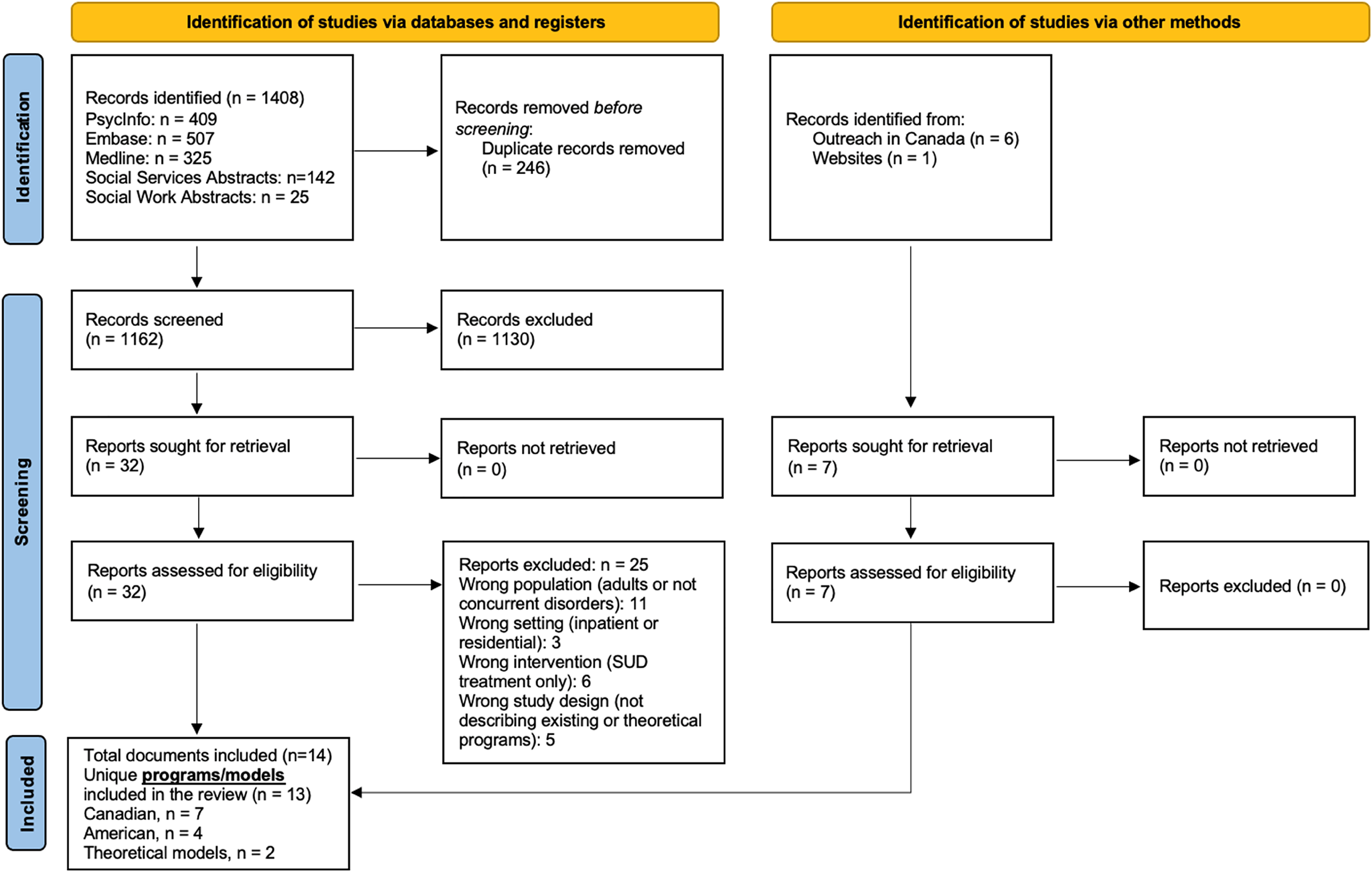
Study flow diagram.
Documents identified following systematic search and outreach were included if they proposed, described, or evaluated outpatient child and youth concurrent disorders programs. Documents were excluded from further analysis if they did not present details of program structure or if the program could not be contacted for additional information. Two attempts were made to contact identified programs, after which programs were excluded from analysis due to incomplete information.
Data Abstraction
A standardized data abstraction form was developed and piloted by two reviewers (TR and EL) using Microsoft Excel version 16.58 (Supplemental Table 2). One reviewer (TR) abstracted data from the included documents and a second reviewer (EL) independently reviewed all abstracted data. Information was abstracted on program characteristics, including description of population served, eligibility and exclusion criteria, referral process, clinical setting and funding, clinician composition, duration of follow up, assessment tools applied, and psychotherapies offered. Information was abstracted on program components based on their sequential description in available program documents. Components were defined as activities of a program that appeared to accomplish a task or contribute to its function, such as activities undertaken in the treatment of patients. Examples of components abstracted from documents included assessment processes, psychological therapy, and family engagement, among others.
General limitations of documents were noted; however, given the unique study designs and narrative nature of this review, the methodological quality and risk of bias was not formally assessed. To enhance the accuracy of our data abstraction process, we provided programs with the opportunity to review the characteristics and components abstracted from their program documents and share any feedback or additional information. If available, we reached out to the Clinical Director of the program for review and feedback; otherwise, we reached out to other members of the clinical team or program leadership. One clinical program did not have any written documents describing their program. In this case, we provided the program with our data abstraction form to populate with relevant details.
Development of a Conceptual Framework
Components abstracted from each program were assessed for their placement within a de novo, overarching, conceptual framework. When programs used different terms to describe conceptually similar components, we grouped these under a single construct. 22 We then synthesized constructs and presented them in a framework that maps the components of an outpatient child and youth concurrent disorders program. The framework development process was iterative. We iteratively presented drafts of the framework to programs to obtain feedback that helped us to refine and further develop the framework into its final form.
Results
Systematic Review Search Results
We identified 1,408 published documents of which 246 were duplicates (Figure 1; Study Flow Diagram). After title and abstract screening, 32 documents met our eligibility criteria; following full-text screening, 7 documents were included for data abstraction.30-36 We excluded full-text documents due to the following reasons: wrong patient population (e.g., adult population or not concurrent disorders; n = 11), wrong setting (e.g., inpatient settings; n = 3), wrong intervention (e.g., substance use treatment only; n = 6), and wrong study design (e.g., not describing programs; n = 5). From the seven documents included following full-text screening, four unique child and youth concurrent disorder programs30-34 and two theoretical models35,36 were identified. Through outreach with Canadian programs and websites, we identified seven additional programs from which formal and informal documents could be obtained describing program structure and components. In the end, the 11 programs and 2 theoretical models from which data could be abstracted to develop an integrated framework were as follows: Fraser Health Regional Youth Concurrent Disorders Program (Fraser Health Authority, British Columbia),37,38 Concurrent Addiction and Mental Health Program (Edmonton, Alberta),39,40 Youth Substance Use and Mental Health Services (Calgary, Alberta),41,42 Young Adult Substance Use Program (Hamilton, Ontario),43,44 Youth Addiction and Concurrent Disorders Service (Toronto, Ontario),45,46 Transitional Aged Youth Service (Ottawa, Ontario),30,31,47,48 IWK Concurrent Disorders Specific Care Clinic (Halifax, Nova Scotia), 49 Addiction Recovery Management Service (Boston, Massachusetts),50,51 East Tennessee Assertive Adolescent Family Treatment Program (Multisite, Tennessee), 32 Integrated Co-occurring Treatment Model (Multisite, Ohio),33,52-55 Sound Health (Multisite, Washington),34,56 and theoretical models proposed by Hulvershorn et al. 35 and Spencer et al. 36
Characteristics of Outpatient Youth Concurrent Disorders Programs Included in Framework Development
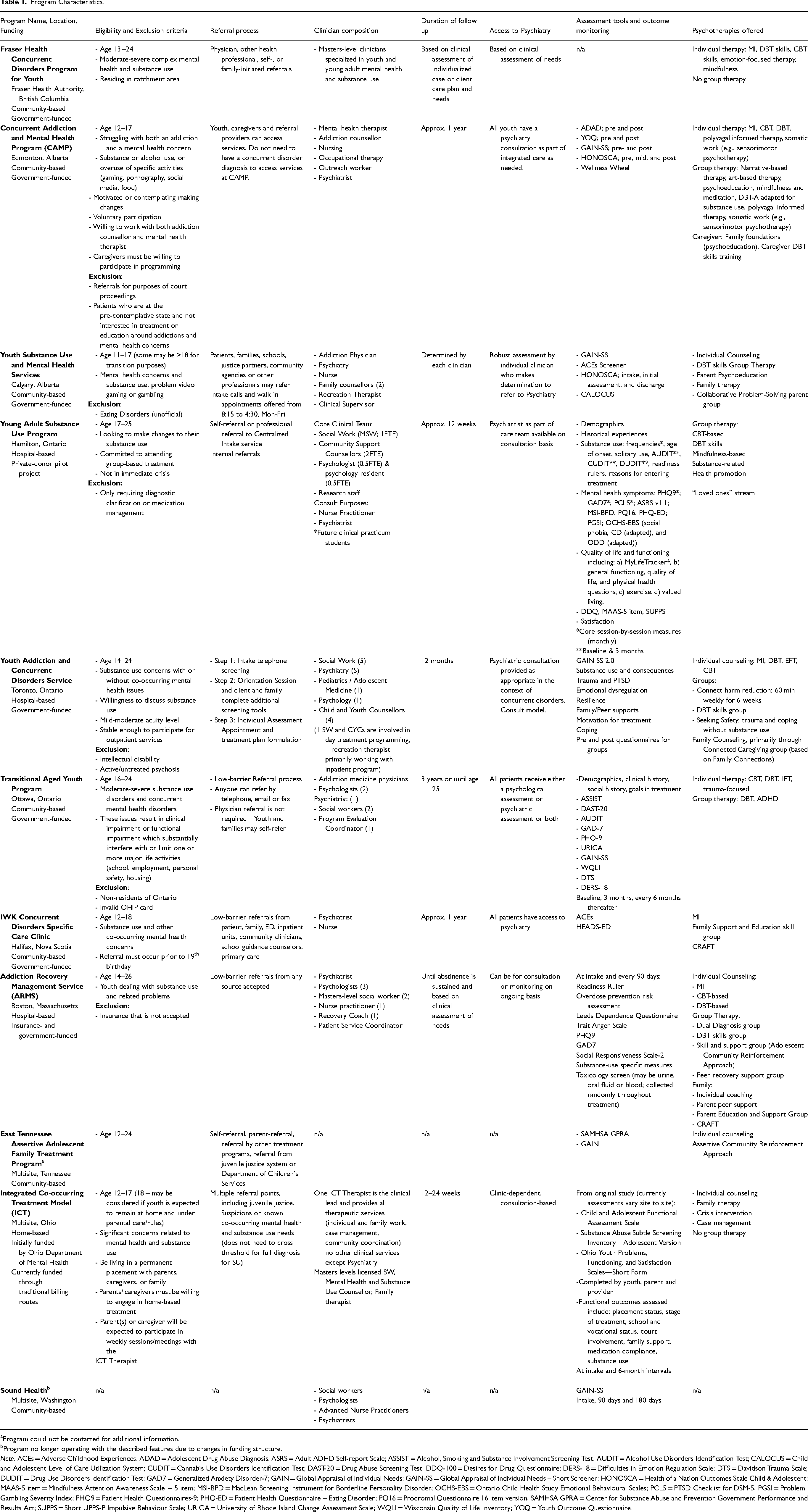
Characteristics of the programs included in our framework development process are detailed in Table 1. Among the programs, four exclusively served children younger than 19 years of age,39,41,49,52-54 two exclusively served youth (e.g., 16 or 17 to 25),43,47 and the remainder served both child and youth patients.32,37,45,50 Most programs specified in their inclusion criteria the requirement of both a mental health and substance use concern, although severity criteria ranged among programs. Two programs specified eligible severity criteria to be “moderate-severe,”37,47 another program accepted patients with “mild-moderate” 45 acuity level and other programs did not specify any severity criteria. In two programs, patients with overuse of specific activities such as problem video gaming and gambling could be eligible for services.39,41 Two programs required caregiver participation in programming for children and youth to be eligible for services39,52 while four programs provided services for caregivers or loved ones that were not predicated on child or youth participation.41,44,49,50
Program Characteristics.
Program could not be contacted for additional information.
Program no longer operating with the described features due to changes in funding structure.
Note. ACEs = Adverse Childhood Experiences; ADAD = Adolescent Drug Abuse Diagnosis; ASRS = Adult ADHD Self-report Scale; ASSIST = Alcohol, Smoking and Substance Involvement Screening Test; AUDIT = Alcohol Use Disorders Identification Test; CALOCUS = Child and Adolescent Level of Care Utilization System; CUDIT = Cannabis Use Disorders Identification Test; DAST-20 = Drug Abuse Screening Test; DDQ-100 = Desires for Drug Questionnaire; DERS-18 = Difficulties in Emotion Regulation Scale; DTS = Davidson Trauma Scale; DUDIT = Drug Use Disorders Identification Test; GAD7 = Generalized Anxiety Disorder-7; GAIN = Global Appraisal of Individual Needs; GAIN-SS = Global Appraisal of Individual Needs – Short Screener; HONOSCA = Health of a Nation Outcomes Scale Child & Adolescent; MAAS-5 item = Mindfulness Attention Awareness Scale − 5 item; MSI-BPD = MacLean Screening Instrument for Borderline Personality Disorder; OCHS-EBS = Ontario Child Health Study Emotional Behavioural Scales; PCL5 = PTSD Checklist for DSM-5; PGSI = Problem Gambling Severity Index; PHQ9 = Patient Health Questionnaires-9; PHQ-ED = Patient Health Questionnaire – Eating Disorder; PQ16 = Prodromal Questionnaire 16 item version; SAMHSA GPRA = Center for Substance Abuse and Prevention Government Performance and Results Act; SUPPS = Short UPPS-P Impulsive Behaviour Scale; URICA = University of Rhode Island Change Assessment Scale; WQLI = Wisconsin Quality of Life Inventory; YOQ = Youth Outcome Questionnaire.
Framework of the Components of an Outpatient Child and Youth Concurrent Disorders Program
In Figure 2, we present our integrated framework. Please refer to Supplementary Table 3 for complete details on the components abstracted from each program. The framework is comprised of a central core of 12 program components and 6 surrounding factors informing the program components. These factors include philosophical orientation, models of care, health system factors, clinical service factors, program development, and community partnerships.
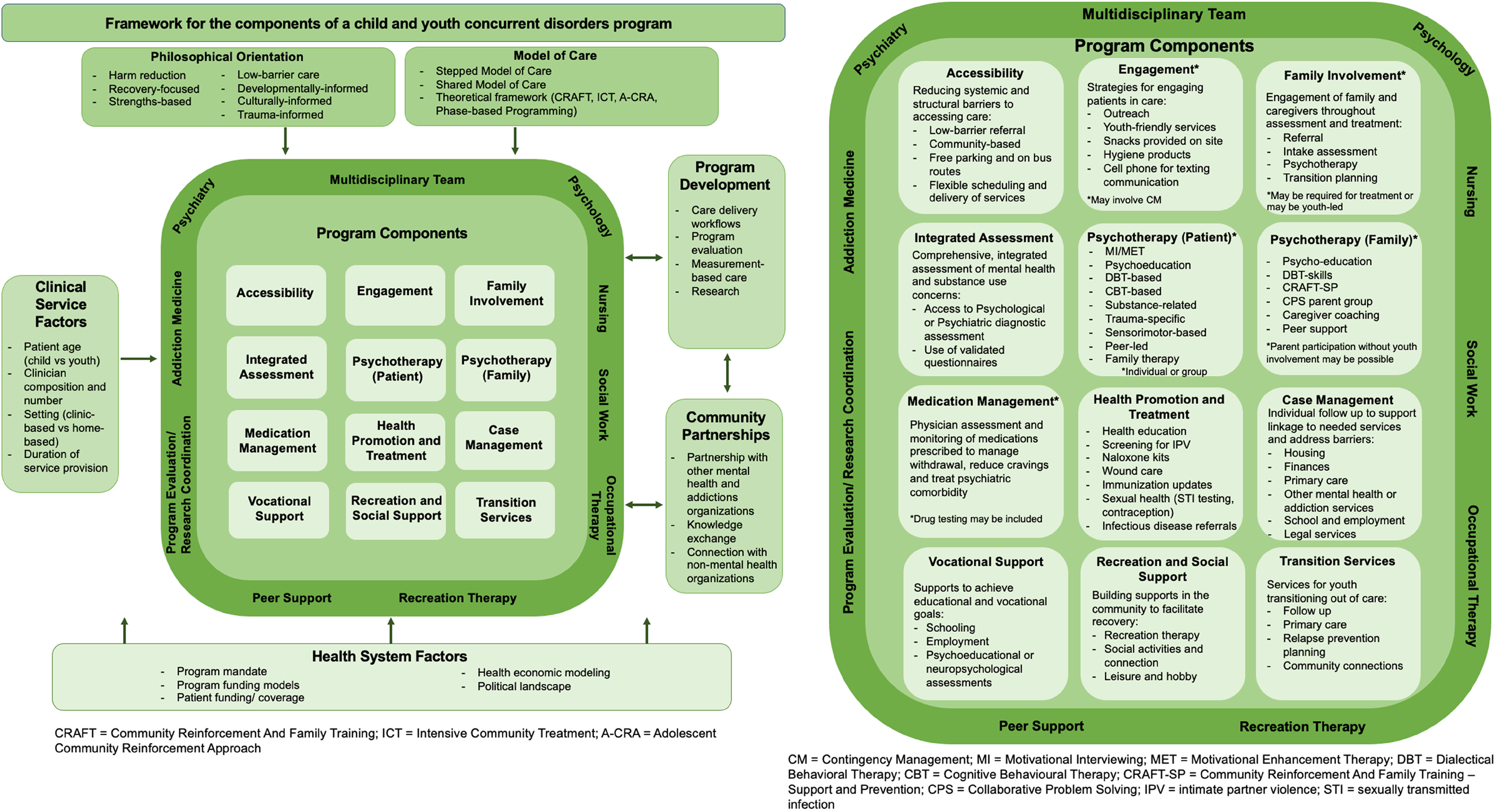
Framework for the components of child and youth concurrent disorders programs.
Across programs, components were informed by both the philosophical orientation of the program and the models of care applied. Programs frequently incorporated multiple philosophical orientations, which included: (1) Harm-reduction-oriented programs integrated strategies aimed to reduce negative consequences of substance use.38,39,45,48-50,52,55 Notably, none of the programs reported to have an abstinence-based orientation. (2) Recovery-focused programs described an emphasis on increasing knowledge about concurrent disorders, supporting more adaptive ways of coping,34,48,50 and one program included peer-led recovery groups. 50 (3) Strengths-based approaches focused efforts on building upon youth and family's strengths, resources, and informal supports.33,52 (4) Low-barrier care involved minimizing obstacles to accessing care; strategies ranged from not requiring a physician referral to accessible, youth-friendly, and community-based physical spaces.36,48 (5) Developmentally informed approaches considered developmental stages to inform assessment and intervention with respect to academic, vocational, family, and relationship domains. 39 (6) Culturally informed approaches involved efforts to provide culturally appropriate care for diverse groups and to include culturally diverse stakeholders in program planning and provision.36,37,43 For some programs, this included diversity training for clinicians, development of relationships with Indigenous community leaders, and creation of physical spaces to facilitate cultural practices. 39 (7) Trauma-informed care was described as both an organization structure and treatment framework that understands, recognizes, and responds to the effects of all types of traumas on patients.36,39,45 In one program, this was operationalized as including staff training in trauma-informed care (e.g., Brain Story Certification, Therapeutic Crisis Intervention).39,40 One theoretical model emphasized the importance of provider-initiated assessments of trauma and supports that reduce the risk of additional trauma exposure. 36
Models of care employed by the programs included stepped care, shared care, and models of care based on theoretical frameworks. In a stepped care model, the level of service intensity and resources is adjusted according to current needs; in many programs, this involved levels of care ranging from outpatient programming to day treatment to inpatient care or withdrawal management services.37,41,42,45,47-50 A shared care model allows patients followed by other community organizations to receive services delivered jointly with community partners with collaborative treatment planning, including case consultations and medication management. 48 Evidence-informed theoretical frameworks were employed in some programs, such as Community Reinforcement and Family Training (CRAFT),43,44,49,50 Intensive Community Treatment, 32 and Adolescent Community Reinforcement Approach.32,50 Phase-based or stage-wise programming was described in one program39,40 and in one theoretical model 35 as progression through different defined phases of treatment based upon patient's therapeutic progress and stages of change.
Health system factors, including program mandates and funding, influenced the structure and activities of the program. Indeed, Canadian and American programs differed in their structures of both program and patient funding, related to underlying differences in the funding of the health system in each country. Broad health system factors influenced not only the program components but also the clinical service structure, program development methods and community partnerships that each further informed the program components. Clinical service factors influencing program activities included clinician number and composition, clinical setting (hospital-based,43,45,50 community-based,32,38,40,42,46,49,56 or home-based33,52), duration of funded service provision (ranging from approximately three months43,44,52-55 or one year,39,40,44,46,49 to several years or until aging out48,51), and patient age (pediatric programs versus older adolescent and young adult programs).
Procedures related to program development also informed program components. One theoretical model emphasized the importance of care delivery workflows and establishing clear care pathways for patients presenting in different clinical environments (inpatient, outpatient, and emergency department) to be connected to concurrent disorders services. 36 Several programs described robust approaches to program evaluation, research, and measurement-based care.32,44-46,48 Nearly all programs incorporated the use of validated tools and questionnaires in their intake assessments and for outcome monitoring thereafter. Some of the most employed measures were the Global Appraisal of Individual Needs – Short Screener, Health of a Nation Outcomes Scale Child & Adolescent, Adverse Childhood Experience Questionnaire, Alcohol Use Disorders Identification Test, Generalized Anxiety Disorder-7, and Patient Health Questionnaire-9 (Table 1). Opportunities for patients to participate in research were available in at least three programs43,45,48 and two programs43,48 described program evaluation and research staff as members of the multidisciplinary team.
Finally, community partnerships additionally shaped program activities. Partnerships with other mental health and addictions organizations allowed for the use of shared care models 48 and facilitated indirect care and knowledge exchange activities that were described by three programs (e.g., providing consultations, clinical case reviews, presentations, and educational sessions for capacity building).37,39,47,48 Connection with nonmental health organizations facilitated for one program the opportunity to offer patients recreational programing within the community.50,51
All but two programs33,37 described multidisciplinary teams in which multiple providers worked together to provide care to patients. Disciplines included psychology, nursing, social work, psychiatry and/or addiction medicine (Table 1). Less commonly included disciplines were occupational therapy, recreation therapy, peer support and recovery coaching, and program evaluation and research staff.
Program activities could be organized into 12 overarching constructs that make up the components of the framework (Figure 2). In Figure 3, we present the number of programs describing their inclusion of each component.
Accessibility: Reducing barriers and optimizing access to care. Examples from programs included low-barrier referrals accepted from multiple referral sources, community-based locations situated on bus routes or with access to free parking, and flexibility around scheduling of appointments.47,48,52 Engagement: Strategies for engaging patients in care including use of assertive outreach36,37,39 (including home-based outreach). Two programs incorporated the use of youth-friendly services supporting basic needs (e.g., food and hygiene)39,40 and youth-friendly methods of communication (e.g., texting communication).
49
One theoretical model endorsed the use of contingency management to reinforce attendance and abstinence from substance use;
35
however, this was not employed by any of the clinical programs included in the study. Family Involvement: Many programs identified family as playing a critical role in treatment and eight programs31,39,41,43,45,49,50,52 and both theoretical models35,36 described methods of involving family in various stages of assessment and treatment. Approaches ranged from requiring family involvement for treatment,39,52 to being youth-led, such that youth decided on the role of family in their care. Integrated Assessment: All programs described comprehensive diagnostic assessment of both mental health and substance use conducted typically by psychology or psychiatry (less commonly by social work) and use of validated questionnaires. Psychotherapy (for Patients): All programs incorporated psychotherapy for patients using many evidenced-based modalities including Motivational Interviewing,37,39,45,48-50 psychoeducation, Dialectical Behavioral-based therapy,37,39,41,43,45,47,50 and Cognitive Behavioural-based therapy.37,39,43,45,47,50 Psychotherapy was generally provided both in individual and group formats, although some programs provided one or the other exclusively (Table 1). In addition to Motivational Interviewing, many programs offered psychotherapies focused on substance use and harm reduction, including CRAFT, Self-Management, and Recovery Training.32,43,45,49,50 One theoretical model recommended trauma-specific psychotherapy,
36
which was implemented by two programs in the form of individual therapy
48
and Seeking Safety
45
group therapy. Other psychotherapies described by programs included mindfulness-based therapy,37-39,43 art-based therapy,
39
and narrative-based therapy,
39
and three programs offered family therapy.42,45,46,52 Several programs reported using or piloting more unique approaches to psychotherapy. One program described an emphasis on integrating “top-down” and “bottom-up” approaches to psychotherapy and incorporated sensorimotor-based therapy involving somatic interventions for stabilization and skill building.
40
Another program described piloting an interpersonal therapy group and group therapy for attention deficit hyperactivity disorder.
48
A third program described more frequently employing acceptance and commitment-based psychotherapy.
49
Finally, one program utilized peer-led therapy in the form of a peer-led recovery group facilitated by a certified Recovery Coach who has lived experience and is a member of the clinical team.50,51 Psychotherapy (for Caregivers/Families): Seven programs39,41,43,45,49,50,52 and both theoretical models35,36 described psychotherapies designed for caregivers and families, including psychoeducation groups, DBT skills groups, CRAFT-Support and Prevention group, Collaborative Problem Solving parent group, caregiver coaching, and caregiver peer support. Some programs offer the opportunity for caregivers to participate even without child or youth involvement in the program.41,44,49,50 Medication Management: All programs described opportunities for physician assessment and monitoring of medications as required, including for treatment of SUDs (e.g., withdrawal and cravings) and psychiatric comorbidities. Two programs50,52 and one theoretical model
35
described the use of random drug testing to facilitate treatment. Health Promotion and Treatment: Activities promoting and maintaining physical health and well-being (including health education, screening for intimate partner violence and sexual exploitation,
49
and harm reduction management) and provision of medical treatments as required (including immunizations, sexual health care, and infectious disease testing and referrals).39,43,49 Case Management: Individual supports, follow up, and advocacy to ensure linkage to social services and to address barriers to service access. Case management focused on basic needs such as housing and finances, healthcare needs, and other supports around schooling, employment, and legal services.32,45,49,52 Vocational Support: Supports to achieve educational and vocational goals.45,46,48 Program activities ranged from supports around completing secondary or post-secondary schooling, to connections with employment agencies,
48
and one program45,46 was able to offer psychoeducational assessments for youth who required them. Recreation and Social Support: Building connections and supports within the community to assist recovery. Although only one program
42
included a recreation therapist within their outpatient clinical team, a number of programs emphasized the importance of incorporating leisure, recreation, and play activities into the therapeutic process.36,42,50,52 Another program
50
operationalized this by fostering connections with community organizations invested in supporting individuals affected by SUDs and developed partnerships allowing patients to access physical fitness and other recreational activities. Transition Services: Supports specifically implemented for youth transitioning out of clinical care. These included supports to obtain further follow up, connection with primary care, and relapse prevention planning.
39
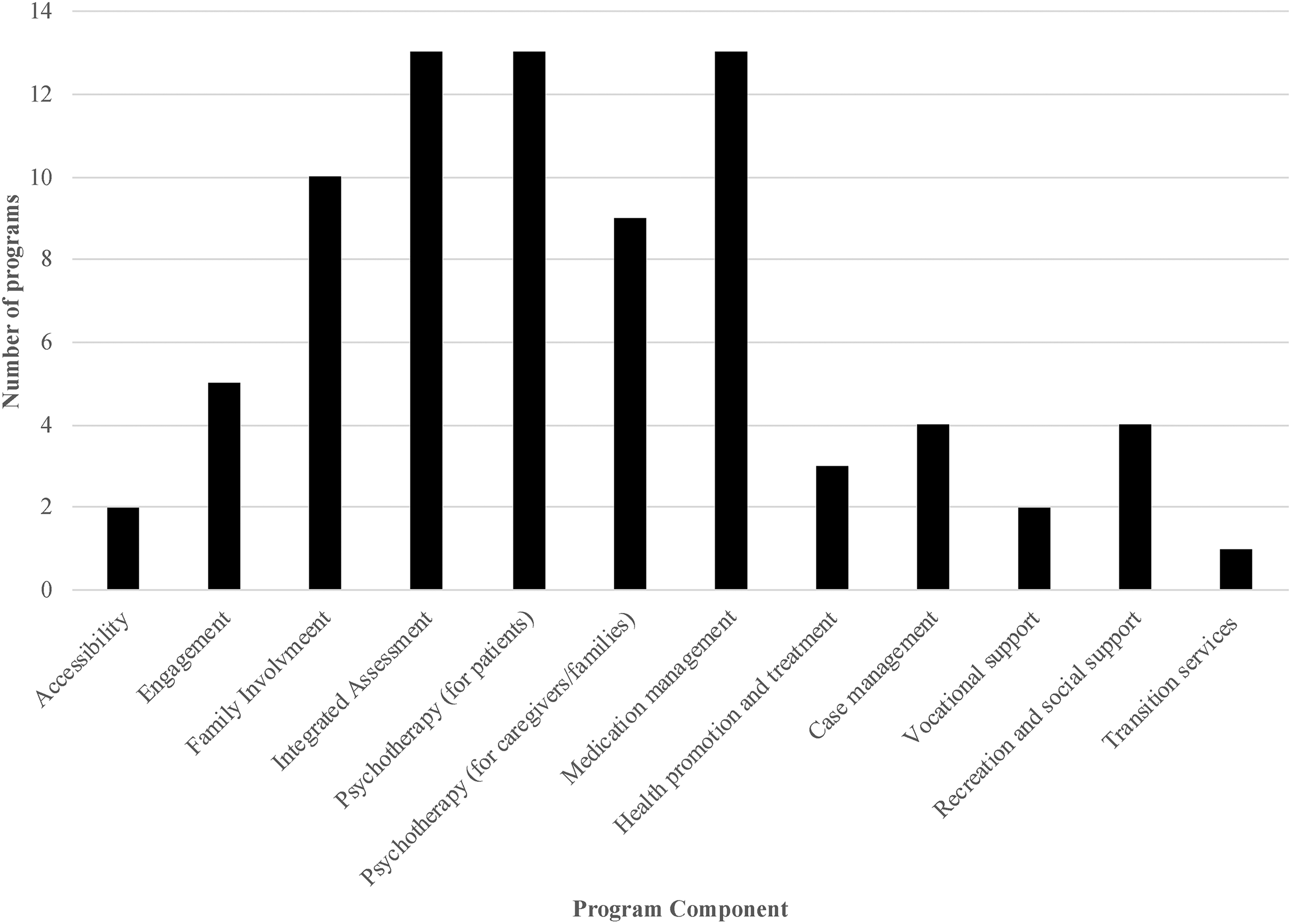
Number of programs describing the inclusion of each program component (N = 13).
Discussion
We developed a comprehensive framework describing components of child and youth outpatient concurrent disorders programs, drawing from 11 clinical programs and 2 theoretical models. These components included accessibility, engagement, family involvement, integrated assessment, psychotherapy (for patients), psychotherapy (for caregivers and families), medication management, health promotion and treatment, case management, vocational support, recreation and social support, and transition services. We identified factors influencing program components including the program's philosophical orientation and model of care, clinical service factors, program development, community partnerships, and health system factors. The final integrated framework may assist programs, both those currently operating and those in development, to reflect on their structure and activities. Organizing current or future activities into these components may reduce redundancy in activities resulting in streamlined resources. The framework may also serve to support advocacy for resource allocation for existing or future programs.
Our framework is designed to be comprehensive, and it is not the case that every clinical program included in our study incorporates every component that is identified in the integrated framework. Rather, the framework represents an amalgam of what different programs provide. Some of the most distinct differences existed between programs that primarily served pediatric patients and those that primarily served youth patients, particularly around family involvement and services provided to caregivers. There also existed significant variability in the duration of follow up provided by programs. American and Canadian programs differed considerably in their funding, reflecting fundamental differences in the funding of their health systems.
Many programs were structured in a way reminiscent of the service “hub” model of care that has been successfully implemented and researched in mental health and primary care.57-60 Hub-based services provide comprehensive health and social services in a single setting with the aim of reducing barriers to care and service fragmentation. 60
Limitations and Strengths
The interpretive nature of CIS is inherently subjective and creates inevitable limitations to the replicability of the framework developed. Additionally, the information obtained from programs included in this review reflects a snapshot in time; programs are continually developing and evolving and thus a framework and its components, too, should continue to evolve. This study does not examine the evidence base behind different components of treatment and cannot make evidence-guided recommendations about program structure or treatment. Although specific psychotherapies offered by different programs could be identified, the details of medication treatments offered were not available.
This study is strengthened by our use of both rigorous systematic review methods and outreach strategies to identify relevant programs and models ultimately used in the development of the final framework. This is the first time CIS methods have been applied to explore this topic and advance our understanding of structures of child and youth concurrent disorders care. The framework was developed by one researcher (TR), with input from a second researcher (EL), and with review and further input from the participating programs. Altogether, 8 of the 11 included programs provided feedback that was incorporated during the development of the final framework. Our iterative approach to obtaining feedback directly from the programs involved in this study improves the construct validity of the framework.
Future Directions
Next steps for this work include determining the applicability of this framework beyond the programs included in the present study. This may include seeking perceptions of providers working in the field about the face validity of the framework, to assess the applicability of the proposed components and to identify additional components that may be missing. Assessing challenges or barriers to the implementation of various framework components will be important. Although inclusion within the study was not limited to Canadian and American programs, we did not identify any programs from other countries through our systematic review search, nor did we conduct outreach in other countries. Further testing of the framework to assess applicability in other contexts worldwide would be valuable.
Additionally, the usefulness of this framework in evaluating outpatient child and youth concurrent disorders programs warrants assessment. Although not developed specifically as a framework for evaluation, an extension of this work may be to synthesize data from primary studies that evaluate individual program structure or components and to develop tools by which to assess the effectiveness of different components of care. Finally, future research may aim to examine the evidence base behind each individual proposed component of care. Although there exist studies and knowledge syntheses evaluating some proposed components (e.g., psychotherapies), for other components there is little or no evidence available in the literature to demonstrate effectiveness. Comparing the outcomes of different clinical programs may also help to inform the growing body of evidence about the effectiveness of different components.
Conclusions
Using a CIS approach to identify and synthesize rich detail from clinical programs and theoretical models, we developed a comprehensive framework describing components of child and youth outpatient concurrent disorders programs. This framework may assist programs, both those currently operating and those in development, to reflect on their structure and activities. Future research may include an assessment of this framework for applicability in different healthcare settings and contexts worldwide.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437231212037 - Supplemental material for Components of Outpatient Child and Youth Concurrent Disorders Programs: A Critical Interpretive Synthesis
Supplemental material, sj-docx-1-cpa-10.1177_07067437231212037 for Components of Outpatient Child and Youth Concurrent Disorders Programs: A Critical Interpretive Synthesis by Tea Rosic, Elizabeth Lovell, Harriet MacMillan, Zainab Samaan and Rebecca L Morgan in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
The authors would like to acknowledge the contributions of the following individuals for their time and valuable assistance in providing information about their clinical programs and feedback throughout the study process: Gretchen L. Conrad, PhD, CPsych, Amanda Davis, MSW, RSW, Selene Etches, MD, FRCPC, Michael Fox, MA, LPCC-S, LCDC III, Melissa Griffin, PhD, C.Psych, Jillian Halladay, RN, PhD, Cindy Nguyet Van Hoang, MA, Sharon Ling, MScOT, OT Reg (AB), Dennis Marceron, LMHC, CDP, CMHS, James McKowen, PhD, Richard Shepler, PhD, LPCC-S, and Susie Winston, MSW, LICSW, MHP.
Declaration of Conflicting Interests
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Harriet MacMillan is supported by the Chedoke Health Chair in Child Psychiatry.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.