
Abstract
Objective
This lived experience-engaged study aims to understand patient and family perspectives on the relationship between suicidality and medical assistance in dying when the sole underlying medical condition is mental illness (MAiD MI-SUMC).
Method
Thirty individuals with mental illness (age M = 41.8 years, SD = 14.2) and 25 family members (age M = 47.5 years, SD = 16.0) participated in qualitative interviews examining perspectives on MAiD MI-SUMC and its relationship with suicide. Audio recordings were transcribed and analysed using reflexive thematic analysis. People with lived experience were engaged in the research process as team members.
Results
Four main themes were developed, which were consistent across individuals with mental illness and family members: (a) deciding to die is an individual choice to end the ongoing intolerable suffering of people with mental illness; (b) MAiD MI-SUMC is the same as suicide because the end result is death, although suicide can be more impulsive; (c) MAiD MI-SUMC is a humane, dignified, safe, nonstigmatized alternative to suicide; and (4) suicidality should be considered when MAiD MI-SUMC is requested, but suicidality's role is multifaceted given its diverse manifestations.
Conclusion
For patient-oriented mental health policy and treatment, it is critical that the voices of people with lived experience be heard on the issue of MAiD MI-SUMC. Given the important intersections between MAiD MI-SUMC and suicidality and the context of suicide prevention, the role that suicidality should play in MAiD MI-SUMC is multifaceted. Future research and policy development are required to ensure that patient and family perspectives guide the development and implementation of MAiD MI-SUMC policy and practice.
Introduction
Assisted dying is legally permitted in a number of jurisdictions, such as Canada, the Netherlands, Belgium, Luxemburg, Switzerland, and several American states. 1 To be eligible for medical assistance in dying (MAiD) in Canada, the requester has to be aged 18+, eligible for government-funded health services, capable of making healthcare decisions, make a voluntary request, have a “grievous and irremediable” medical condition, give informed consent, and have been informed of the means available to relieve their suffering. 2 If natural death is reasonably foreseeable, 3 the patient must undergo two independent assessments; if not reasonably foreseeable, there must also be a consultation with a healthcare professional with expertise in the condition leading to the MAiD request if one of the assessors does not have this expertise; a minimum 90-day period should lapse between the start of the first assessment and the provision of MAiD; the provider, assessor, and patient must all agree that serious consideration has been given to any treatments and services available for the patient's condition. 3 Mental illness cannot be considered a serious or incurable illness, disease, or disability for the purposes of MAiD eligibility, until March 2024. 4 These changes and potential future legislative changes will open MAiD eligibility to a new population and raise questions requiring reflection and deliberation.
A number of countries allow MAiD when mental illness is the sole underlying medical condition (MAiD MI-SUMC). The Netherlands conducted 115 such procedures in 2021, 5 out of 7,666 MAiD procedures as a whole. 1 Belgium conducted 26 MAiD MI-SUMC procedures in 2022, out of 2,966 assisted deaths. 6 Though reasonable to expect that MAiD MI-SUMC in Canada will account for a small minority of cases, the implications are real for those who consider applying.
Public support for assistance in dying, across medical conditions, has increased in the past few decades. However, for many, it is difficult to identify fundamental differences between MAiD and suicide. 7 Both involve the decision to end one's life. However, across illnesses, differences between MAiD and suicide are said to relate to the acceptability of the decision (where MAiD is more socially accepted), impulsiveness, decision-making capacity, 7 the involvement of a medical professional, 8 and the existence of legislated criteria and safeguards guiding MAiD processes. However, these features do not distinguish suicidality from assisted dying because not all suicidality is impulsive, 9 not all people with mental illness lack decisional capacity, 10 not all those who help someone die have always been medical professionals, 8 and debates about safeguards remain ongoing.
Across mental health disciplines, suicidality is targeted as a preventable outcome using suicide prevention initiatives and interventions addressing suicidal ideation or behaviours. About 9% of the population has experienced lifetime suicidal ideation, and about one-third of those will at some point make a suicide plan. 11 Having a mental illness is a major risk factor for suicidal ideation and behaviours. 11 Elevated rates of suicidal ideation and completed suicide are associated with depressive disorders, bipolar disorders, psychotic disorders, posttraumatic stress disorder, substance use disorders, personality disorders, and other mental illnesses.12–16 When suicide is completed, in addition to the life lost, those who are left behind can face considerable burden, including substantial stigma, trauma, and complicated grief.17,18
As Canada's debates about MAiD MI-SUMC evolve, it is important that we reflect on the implications for patients and families.19,20 Historically, the perspectives of people with mental illness have not always been heard in service design and delivery, leading to interventions that they have ultimately deemed to be unethical or inappropriate, and with unintended consequences.21,22 Evidence-based policymaking and patient-oriented service planning require that the perspectives of people with mental illness and their families contribute to discussions and decisions about MAiD MI-SUMC. To date, a large portion of the literature emerging on MAiD reports on the perspectives of psychiatrists and other health professionals,23,24 not patients and family members.
Method
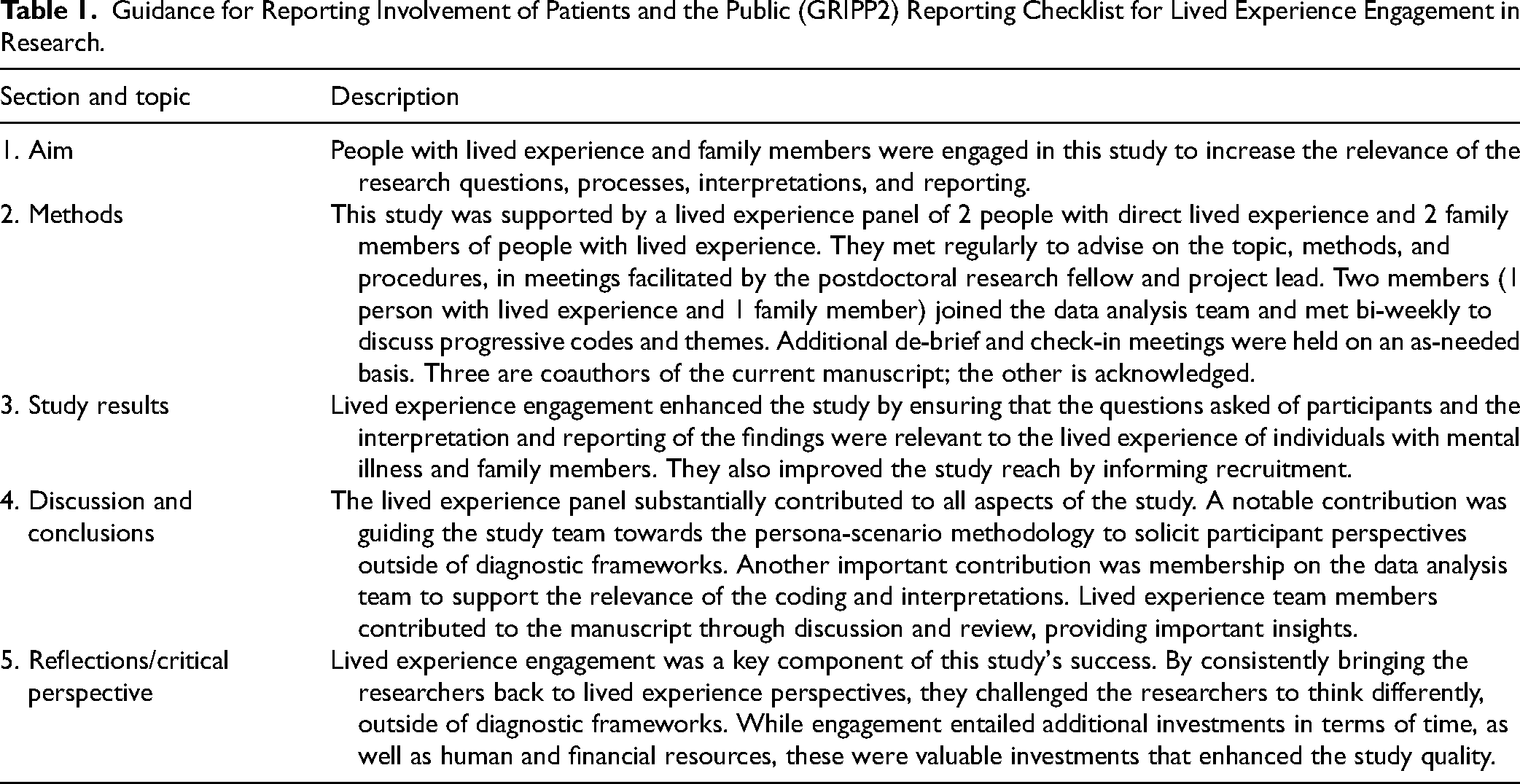
This qualitative study uses reflexive thematic analysis25,26 and is grounded in a contextualist epistemology26,27 to highlight the diversity of knowledge that patients and families create through their situated actions in lived experience contexts. This study engaged individuals and families with lived experience, in accordance with CIHR's Strategy for Patient-Oriented Research. 28 Results are reported following the Standards for Reporting Qualitative Research guidelines. The Guidance for Reporting Involvement of Patients and the Public (GRIPP2) checklist was used to describe engagement (Table 1). 29
Guidance for Reporting Involvement of Patients and the Public (GRIPP2) Reporting Checklist for Lived Experience Engagement in Research.
The semistructured interview guide was developed by interdisciplinary team members, including lived experience and family partners. It contained open-ended questions exploring participants’ perspectives on MAiD and suicide. To enhance the reflections and provide participants with the opportunity to externalize their views on this sensitive topic, we used a persona-scenario approach, 32 that is, participants imagined a fictional person in MAiD MI-SUMC request scenarios. Intersections between MAiD MI-SUMC and suicide were a consistent probe. Notes were taken during interviews to support interview processes. Interviews were audio recorded and transcribed by research staff or a transcription agency and then proofread by a second research staff. Transcripts were managed using NVivo 12 Pro. 33
Results
The characteristics of the patient and family participants are described in Table 2. The average age of patient participants was 41.8 (SD = 14.2, 21–67), and for family members, 47.5 years (SD = 16.0, 20–78). Patient participants reported an average of 2.7 mental illness diagnostic categories as defined in Table 1 (SD = 1.1, range from 1 to 4).
Participant Characteristics.
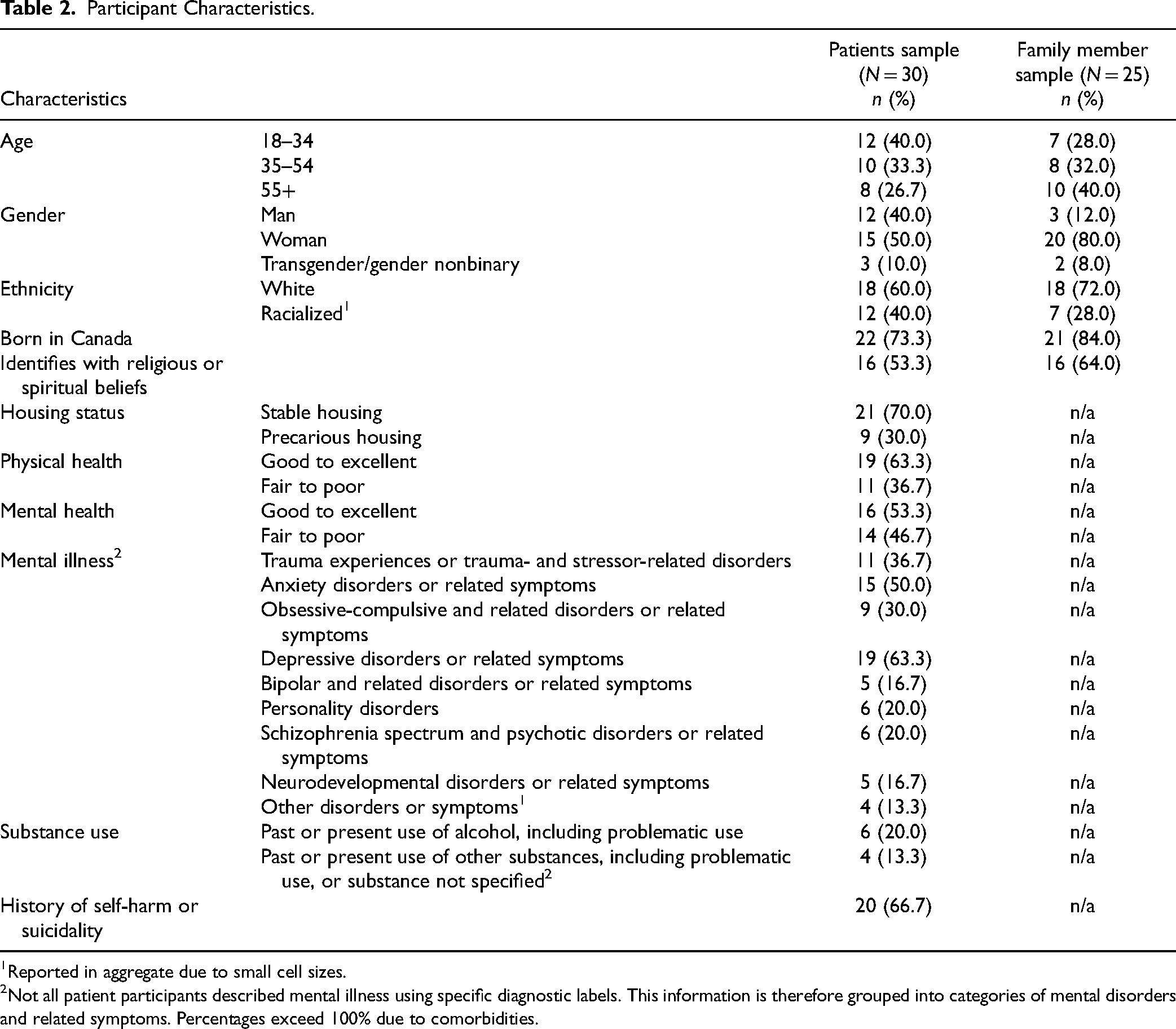
Reported in aggregate due to small cell sizes.
Not all patient participants described mental illness using specific diagnostic labels. This information is therefore grouped into categories of mental disorders and related symptoms. Percentages exceed 100% due to comorbidities.
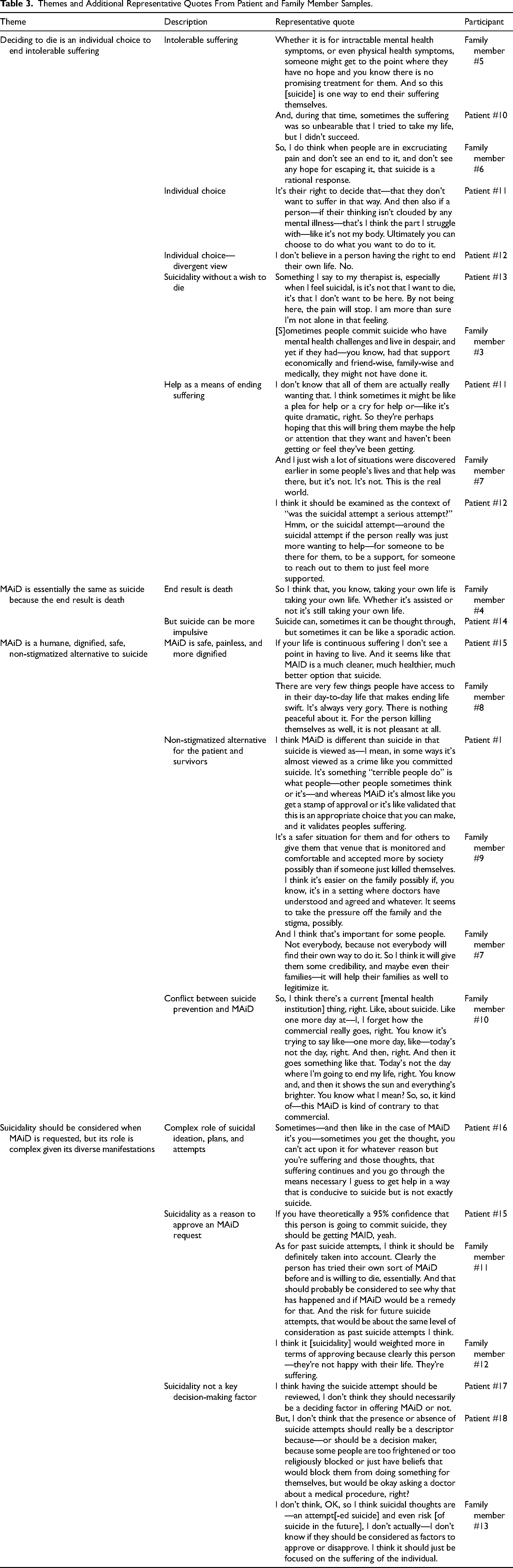
Four main themes were developed: (a) deciding to die is an individual choice to end ongoing intolerable suffering; (2) MAiD MI-SUMC is the same as suicide because the end result is death, although suicide can be more impulsive; (3) MAiD MI-SUMC is a humane, dignified, safe, nonstigmatized alternative to suicide; and (4) suicidality should be considered when MAiD MI-SUMC is requested, but suicidality's role is multifaceted given its diverse manifestations. Themes and divergent perspectives are reported below. For additional representative quotes, see Table 3.
Themes and Additional Representative Quotes From Patient and Family Member Samples.
There are things that are worse than death, I think, and for some people, living and suffering indefinitely is worse than dying, even though they may not know for certain that things could not have improved in the future. Patient #1
Among patients, in particular, it was mentioned that dying to end suffering is a choice that individuals can make for themselves: I think somebody's wishes should be respected if they truly are committed to ending their life. Patient #2
However, this belief in freedom of choice was not universal: Actually, from what I can see, is that you don’t say “it's my own life, I decide when to leave.” No, you don’t actually choose how—when and how to be born. And I think it's the two sides of one thing: then you don’t decide when to leave. You are sent into the world for some reason, and then you exit at the appropriate time, rather than, “I quit, I'm going.” Patient #3
Participants described that in suicide, the decision to die sometimes occurs without truly wishing to die, even in the presence of suffering. They emphasized that people who are suicidal want and need help to relieve their suffering, that is, that death is not the only possible way of relieving suffering. Help might be provided through treatments, informal support, or friends and families. Appropriate and effective help is not always available, which leads to ongoing suffering and sometimes the decision to die: I think that, if you are going to attempt suicide, I don’t think you necessarily want to be successful in it, and it's a release of your inner pain. Family Member #1
So I definitely believe that MAiD and suicide are one and the same, because it is somebody who is in this case intentionally seeking out a procedure to end their own life. Patient #4
However, participants noted that suicide can be more impulsive. Usually, less planning and time goes into preparation for suicide compared to MAiD MI-SUMC: We think about people who actually die by suicide or attempt suicide, yes, there is that kind of random kind of spur of the moment. You’re in that moment of deep anguish and you feel like it's your only way out. You’re kind of clouded in that moment. Family Member #2
There's more dignity to MAID, I think, than suicide for sure, and the chance to, you know, go with your loved ones around you. Family Member #3
And suicide can be painful before you die, which MAID wouldn't be. And you can also botch it and end up with more reasons to want to kill yourself after. Because your life sucks worse. Patient #5
Participants felt that MAiD MI-SUMC does not carry the stigma of suicide. They considered this a benefit of MAiD over suicide, for the individual and for family members left behind: It feels like maybe [MAiD] would be more acceptable to other people, for whatever that's worth. Suicide seems to have, well… it obviously does have a lot of stigma, and MAiD kind of less so, or very less so. Patient #6
Some participants struggled to reconcile suicide and suicide prevention or intervention in the context of the availability of MAiD MI-SUMC: [E]veryone knows that if you actually seriously express suicidal thoughts, people are legally obligated to do something. But, you can fill in an application and you can get—you know (…). So, it just strikes me as odd that, on one hand, the government says I can't kill myself but, on the other hand, they're telling me that I can. Patient #7
I think that, for sure, if there's suicide, you know, lots of… more than ideation is the attempts—if there's been a lot of attempts and coming close, because this person has put plans in place in the past. Ideation–I think people can have ideation and not want to die, but think about dying. And so, I think it would be more around the attempts and an actual having plans in place. I think that that would be something that would be important to consider. Just ideation, I would say no. Family Member #4
Some participants argued that the presence of suicidality points to the need for a MAiD MI-SUMC request to be approved, while others felt that it should not be a key factor in the outcome of an MAiD MI-SUMC request: I guess if he’d made one or more unsuccessful suicide attempts, that's harming him physically—if that was the case, then it's probably better to die in a peaceful controlled situation. Patient #8
Again, I think that the standard of eligibility should always be, “does the person requesting MAiD perceive that their suffering and anguish is intolerable to the point where they no longer want to live?,” whether or not suicide comes into play. Family Member #2
One participant felt that an MAiD MI-SUMC request should be denied in the presence of suicidal ideation: So, there should be a suicidal risk assessment. And if they are at the higher risk [of suicide], they should be denied for MAID. Patient #9
Discussion
This qualitative study examined patient and family perspectives on suicidality and MAiD MI-SUMC. Participants constructed the decision to die as a means of ending the ongoing suffering associated with mental illness. Some believe a decision to die to end suffering is an individual choice, while some expressed that access to effective help would be another way to end suffering. While participants largely equated MAiD MI-SUMC to suicide, since both resulted in death, MAiD MI-SUMC was seen as a more dignified alternative. They also noted less impulsivity and less stigma associated with MAiD MI-SUMC compared to suicide. Most participants believed that the presence of suicidality either suggests that an MAiD MI-SUMC request should be approved or that it should not influence the outcome, but they recognized that the relationship between the suicidality and a MAiD MI-SUMC assessment is complex and multifaceted.
Despite published opinions and perspectives on MAiD, including MAiD MI-SUMC, there is a lack of research that explores the experiences and opinions of patients and families. 34 Additionally, while there is a growing body of literature presenting arguments for or against MAiD MI-SUMC,35,36 there is a scarcity of research objectively examining real-world perspectives without having a predetermined stance. This paper provides some of these missing insights. It does not attempt to address whether MAiD MI-SUMC should or should not be legalized. Instead, it explores the perspectives of patients and family members to gain an in-depth understanding of how they view MAiD MI-SUMC in relation to suicidality, in the context of a tension between MAiD, suicidality, and suicide prevention or intervention in the field of mental health.
The American Association of Suicidology issued a statement opining that MAiD and suicide are different. 37 However, it has also been argued that there is overlap38,39 and attempting to distinguish between MAiD and suicide may not be fruitful. Instead of focusing on the similarities or differences between MAiD and suicide, opening a dialogue about the wish to die might provide more dividends by emphasizing individual control and destigmatization. 7 This reflects the current study's findings regarding the similarities and differences between MAiD MI-SUMC and suicide. For example, despite the shared outcome of death, suicide entails considerable stigma, 38 which participants felt that MAiD MI-SUMC does not. Many participants further supported the notion of individual control via the right to choose, although this was not universal.
The existing research shows a number of areas of overlap with our findings and areas for further reflection. A Dutch study reported that MAiD was considered important to people with mental illness as a means of ending suffering in a dignified manner, through self-determination. 40 Participants in that study argued that suicide could happen at a time of acute crisis as part of their mental illness, while an MAiD request entails a slower, more deliberate planning process than suicide. 40 It might therefore be important to distinguish between acute suicidality in the response to circumscribed suffering versus chronic suffering despite treatment access and longer reflection. Another study showed that marginalized populations prefer MAiD to suicide, due to a more certain, painless, and accepting process. 38 Research has identified unbearable suffering as a key contributor to MAiD requests in physical and mental illness, with continuous unbearable suffering being particularly associated with mental illness. 41 Unbearable suffering in MAiD requests can be complex and attributable to various factors. These include medical aspects of health, inter- and intrapersonal components, functioning, and existential distress. 42 Mental aspects may play a particular role in the unbearable suffering associated with MAiD requests.41,42
A qualitative study of partners of individuals who died by MAiD or suicide due to mental illness revealed differences in the grieving process. Participants connected to someone who had died by MAiD reported better emotional outcomes than those connected to someone who died by suicide. This difference was attributed to factors such as more planning, increased support, and less violence associated with the manner of death. 43 Similar results have been found among family survivors of MAiD for physical illnesses. 44 As research on patient perspectives advances, these notions that have emerged across studies and jurisdictions should be further explored.
Psychological theories of suicidality can help understand the findings. The stress-diathesis model suggests that stress plays a key role in triggering suicidality. 45 In contrast, the interpersonal–psychological theory proposes that suicidality arises from feeling like a burden on society and a lack of sense of belonging. 46 However, when we explored MAiD MI-SUMC with participants, they spoke of wanting to alleviate long-standing suffering. This may be more related to a loss of hope than a specific triggering event during a crisis. Hope is a key construct in suicidality, as in MAiD requests.34,41 For individuals with terminal physical illness, the desire for MAiD is often associated with the loss of hope for recovery, unlike suicide, where hope of recovery may still exist. 7 Indeed, some argue that offering MAiD MI-SUMC means conveying a loss of hope for the individual's recovery. 7 The interpersonal–psychological theory suggests that suicidality occurs when both the desire and ability to die are present. 46 MAiD MI-SUMC provides a new avenue that, for some individuals, will provide the opportunity for hastened death. In contrast, it has been argued that the availability of MAiD MI-SUMC might offer hope of relieving suffering for some, 34 potentially increasing the will to continue to live in some cases.34,47
These findings should be interpreted in the context of several limitations. Despite efforts to maximize diversity, some perspectives may have been missed. Ethnic/cultural differences have been found in public views of MAiD. 48 Research should examine perspectives among racialized groups, Indigenous peoples, LGBT2SQ+ individuals, immigrant populations, and people experiencing a range of social determinants of health. The use of self-reported diagnostic information is a further limitation.
Conclusions
MAiD MI-SUMC has intersections with suicidality that should be considered. Understanding patient and family perspectives about MAiD MI-SUMC is essential to guide practice and policy decisions. Participants acknowledge the intersections between MAiD MI-SUMC and suicidality and the benefits of MAiD MI-SUMC as a more dignified way of ending suffering, but also the inherent complexity of considering MAiD MI-SUMC requests in the context of suicidality. Future research is required with diverse populations to ensure that patient and family perspectives guide the development and implementation of MAiD MI-SUMC policy and practice.
Footnotes
Acknowledgments
The MAiD MI-SUMC Study Team at the Centre for Addiction and Mental Health includes Lisa D. Hawke, Hamer Bastidas-Bilbao, Vicky Stergiopoulos, Mary Rose van Kesteren, Vivien Cappe, Michael Dawthorne, Bartholemew H. Campbell, Donna E. Stewart, Mona Gupta, David Castle, Daniel Z. Buchman, Tarek K. Rajji, Alexander I. F. Simpson, Roslyn Shields, and Alison Freeland.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Lisa D. Hawke, Hamer Bastidas-Bilbao, Vivien Cappe, Mary Rose van Kesteren, Alexander I. F. Simpson, Bartholemew H. Campbell, and Vicky Stergiopoulos declare that there is no conflict of interest. Donna Eileen Stewart declares that she has served in the Expert Panel on MAID and Mental Illness and the Canadian Psychiatric Association Working Group on MAID and as a reviewer of the Canadian Association of MAiD Assessors and Providers curriculum on MAID. Mona Gupta declares that she has received funding related to this subject from CIHR; she was the Chair of Health Canada's Task Group on MAID Practice Standards, the Chair of the Federal Expert Panel on MAID and Mental Illness, and the Chair of the AMPQ ad hoc committee on MAID. David Castle has received grant monies for research from NHMRC (Australia), Barbara Dicker Research Fund, Milken Institute, Canadian Institutes of Health Research, and Psyche Foundation; consulting fees from Seqirus; honoraria for talks from Seqirus, Servier, and Mindcafe Forum; honoraria as advisory board member from Seqirus and Lundbeck; he is a founder of the Optimal Health Program (OHP) and holds 50% of the IP for OHP, is part owner and board member of Clarity Healthcare, is unpaid board chair of the Psyche Institute, and does not knowingly have stocks or shares in any pharmaceutical company.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by a grant (332964) awarded to Vicky Stergiopoulos by the Canadian Institutes of Health Research and a grant awarded to Lisa D. Hawke by the University of Toronto's Department of Psychiatry Suicide Studies Fund.