
Abstract

Introduction
This position paper addresses the need for psychiatrists to increase their understanding of the mental health needs of people who identify themselves as two spirit, lesbian, gay, bisexual, transgender, queer and other minority sexual orientations and gender identities (2SLGBTQ+) with a particular focus on the need for a more comprehensive approach to care for transgender and gender diverse individuals. While the Canadian Psychiatric Association (CPA) has taken a strong position in advocating for decreasing stigma and discrimination, the focus of antistigma advocacy has centred most significantly on people with mental illness. While doing so, however, the CPA has recognized the ongoing stigma and discrimination in society based on several factors, including sex, gender, race, sexual orientation and religion. 1 Psychiatry has a history of conflating 2SLGBTQ+ identities with mental illness and has, therefore, historically contributed to the stigma and discrimination faced by people who identify as 2SLGBTQ+, affecting not only their mental health but also their access to appropriate mental health care. 2
Background
In 1973, after much debate, deliberation and political and societal pressure, the American Psychiatric Association (APA) removed the diagnosis of homosexuality from the Diagnostic and Statistical Manual of Mental Disorders (DSM), Second Edition,3,4 and issued a position statement in support of gay and lesbian civil rights. 5 Since that time, all major professional mental health organizations have gone on record to affirm that homosexuality is not a mental disorder. However, controversy remains surrounding the continued inclusion of gender dysphoria6,7 within the DSM-5 (previously gender identity disorder8–10 in the DSM-IV). Many health-care professionals who work with people who identify as transgender argue that this diagnosis should also be removed from the DSM because the diagnosis pathologizes transgender identities, while others believe it should remain in the DSM to ensure continued access to appropriate medical treatment (access to hormones and [or] gender-confirming surgeries) for transgender people.6,7,8,10 The “Position Statement on Discrimination Against Transgender and Gender Diverse Individuals,” released by the APA in July 2012 and reapproved in 2018, states that “being transgender or gender variant implies no impairment in judgment, stability, reliability, or general social or vocational capabilities; however, these individuals often experience discrimination due to a lack of civil rights protections for their gender identity or expression.” 11 (p.1)
While the DSM-5 still includes gender dysphoria in its list of mental disorders, the Manual of International Statistical Classification of Diseases and Related Health Problems (ICD-11) removed the term “transsexualism” (previously included in the chapter on mental disorders), replacing it with the term “gender incongruence” (in a newly created chapter called “conditions related to sexual health”). 12 Most people who identify as transgender see this change in the ICD-11 as a great advance, ensuring access to medical transition treatments if desired, while depathologizing transgender identities by placing “gender incongruence” outside of the chapter on mental disorders. 13
Discussion
The demographic statistics regarding 2SLGBTQ+ identities vary according to the definition used. Most studies worldwide estimate that between two to 14 per cent of the population identify as 2SLGBTQ+.14,15 Within this heterogeneous population, the experience of each individual member of the 2SLGBTQ+ community varies widely depending on numerous potentially intersectional factors, including ability, age, sex, gender, ethnoracial group, nationality, religion, socioeconomic status, geographical location and other factors. However, what is common to sexual and gender minorities is that experiences of individual and systemic oppression (minority stress) can often threaten their health and well-being. 2 The history of discrimination and the associated shame concerning 2SLGBTQ+ identities has meant that many health professionals, including mental health professionals, are poorly informed about 2SLGBTQ+ issues and are unfamiliar with appropriate terminology and acceptable language.2,16
Both sexual orientation and gender identity may be most usefully understood as existing along a continuum. 17 Sexual orientation refers to how one thinks of oneself in terms of one's emotional, romantic or sexual attraction, desire or affection for another person. 17 It is very important to note, however, that sexual behaviour is not always congruent with sexual orientation or identity. For example, a person who has sexual relations with men and women may not identify as bisexual. Gender identity is one's internal and psychological sense of oneself as male, female, both or neither. 18 It is also important to note that one's gender identity is totally independent of one's sexual orientation. For example, regardless of whether someone identifies as cisgender, transgender, nonbinary (or any other gender identity), they can identify as having any sexual orientation. A glossary at the end of this document provides additional information about terms used in this position paper and other important terms related to 2SLGBTQ+ issues.18,19
Stigma and discrimination based on sexual orientation and/or gender identity have a tremendous negative impact on the mental health of 2SLGBTQ+ people.20,21 Sexual and physical assault are also risk factors for mental health issues, as is bullying for youth. 22 Risks for 2SLGBTQ+ youth can be reduced by family acceptance and connection with other 2SLGBTQ+ youth.22–25 In fact, lesbian, gay, bisexual and transgender (LGBT) youth who come from highly rejecting families are more than three times as likely to have attempted suicide than LGBT peers who reported no or low levels of family rejection. 24 In an Ontario-based study, a staggering 77 per cent of people who identified as transgender reported having seriously considered suicide at some time in their lives, 43 per cent reported attempting suicide at some point in their lives and 10 per cent reported attempting suicide in the past year.26,27 In a Canada-wide study of 2873 trans and nonbinary people aged 14 and over, one in three participants reported having considered suicide in the past year and one in 20 participants reported attempting suicide in the past year. 28 In the largest survey to date of gender variant and transgender people (N = 6,450), 41 per cent reported attempting suicide at some point in their lives. 29 A recent meta-analysis 30 demonstrated that people who identified as lesbian, gay or bisexual had a higher risk for mental disorders than people who identified as heterosexual in all investigated diagnostic categories (i.e., depression, alcohol use disorder, anxiety disorders and suicidality). The risk for depression and suicidality was higher in people who identified as bisexual compared with lesbians and gay people. 30
The marginalization and discrimination experienced by 2SLGBTQ+ people also contribute to barriers to accessing health and support services.20,31,32 These barriers are compounded by health-care providers often lacking the appropriate knowledge and skills around 2SLGBTQ+ health.33–37 Many 2SLGBTQ+ people fear and avoid traditional health-care settings to protect themselves from mental or physical harm from potentially homophobic health-care providers.38,39 Negative experiences with health-care professionals after disclosing sexual orientation such as the provider being visibly uncomfortable, harsh or abusive language, physically rough or abusive exams and actually being refused care, shape the future use of health services.
39
“Reparative” or “conversion therapy,” a range of pseudo-scientific treatments that aim to change a person's sexual orientation from homosexual to heterosexual or gender identity from transgender to cisgender, is a source of worldwide controversy. In 2000, the APA
40
condemned: psychiatric treatment, such as reparative or conversion therapy which is based upon the assumption that homosexuality per se is a mental disorder or based upon the a priori assumption that the patient should change his/her sexual homosexual orientation . . . Ethical practitioners refrain from attempts to change individuals’ sexual orientation.
40
(p. 1 and 4) APA condemns any practice that aims to change one's sexual orientation or gender expression in the form of conversion therapy, or any other similar type of therapy, as ethically and morally wrong and, additionally, these practices represent a significant risk of harm by subjecting individuals to forms of treatment that have not been scientifically validated.
41
(p. 1)
Changing Directions, Changing Lives: The Mental Health Strategy for Canada 51 and the Mental Health Strategy for Canada: A Youth Perspective 52 both discuss the importance of addressing specific mental health needs related to gender and sexual orientation. These documents specifically recommend increased understanding by professionals and the public about mental health differences related to gender and sexual orientation. They also specifically recommend improving the capacity of 2SLGBTQ+ organizations to address the stigma of mental illness and to work with local mental health services to support their community.
Stereotypes of all kinds can have an impact on the way 2SLGBTQ+ people living with mental health issues are treated, both within the 2SLGBTQ+ community and within the mental health system. People who identify as 2SLGBTQ+ who also happen to have mental health issues often experience a double stigma or dual alienation in which they feel they are not accepted within the mental health community because of their 2SLGBTQ+ identities and are also not accepted within the 2SLGBTQ+ community because of their mental health issues. 53
Recommendations
The CPA affirms the following:
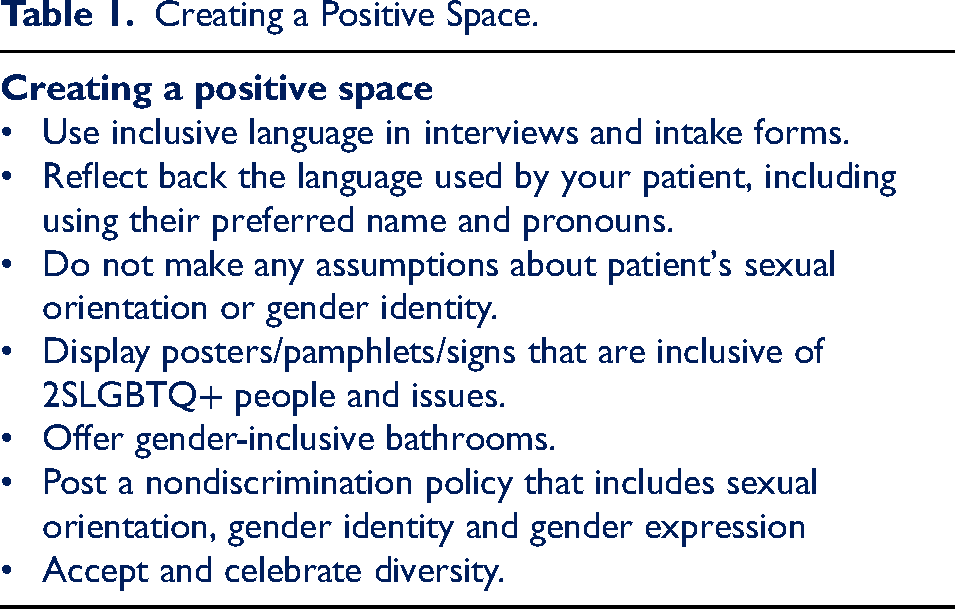
The CPA opposes all public and private discrimination based on sexual orientation, gender identity and gender expression and supports the repeal of discriminatory laws and policies. The CPA supports the passage of laws and policies protecting the rights, legal benefits and privileges of all people regardless of their sexual orientation, gender identity or gender expression. The CPA supports the provision of high-quality mental and medical health-care treatment for all people and, therefore, expects all psychiatrists to provide appropriate, nondiscriminatory treatment to all people, regardless of their sexual orientation, gender identity or gender expression. The CPA supports efforts to provide appropriate and safe environments for people who identify as transgender or who are gender variant or gender nonconforming in institutional settings, such as supportive living environments, long-term care facilities, nursing homes, treatment facilities, shelters and prisons. The CPA also supports access to appropriate treatment in institutional settings for people of all gender identities and expressions, including gender-affirming and transition-related therapies. The CPA supports efforts to provide safe and secure educational environments at all levels of education, as well as foster care environments and juvenile justice programs, that promote an understanding and acceptance of all youth, regardless of their sexual orientation, gender identity or gender expression. The CPA recognizes the efficacy, benefit and medical necessity of gender transition treatments for appropriately evaluated people and calls upon provincial health insurance plans to cover these medically necessary treatments, including travel expenses associated with required appointments and surgeries.44,54 The CPA supports educating psychiatric residents and psychiatrists about how to explore patients’ perceptions of their sexual orientation, gender identity and gender expression using 2SLGBTQ+-inclusive questions and gender-inclusive language. The CPA also supports educating all psychiatric residents and psychiatrists about the potential for mental health-care disparities in 2SLGBTQ+ communities and about some of the specific issues that can apply when working with people who identify as 2SLGBTQ+ (e.g., homophobia and transphobia, family rejection and the coming out process). The CPA supports psychiatrists assessing and addressing social determinants of health with all of their clients/patients, including those who identify as 2SLGBTQ+, given that gaps in these domains disproportionately affect this population's health outcomes and access to care.44,54,55 The CPA opposes the use of reparative or conversion therapy, given that such therapy is based on the assumption that 2SLGBTQ+ identities indicate a mental disorder and/or the assumption that the person could and should change their sexual orientation and/or their gender identity/expression. The CPA calls upon all levels of government to legislate against such “therapies” given they are harmful and unethical. The CPA encourages physician practices, medical schools, hospitals and clinics to broaden any nondiscrimination policies or statements to include sexual orientation, gender identity and gender expression. The CPA encourages the use of respectful and appropriate language with all 2SLGBTQ+ patients and specifically encourages using the patient's preferred name and pronouns. The CPA encourages the creation of a welcoming and affirming environment for 2SLGBTQ+ people by creating an office space and/or hospital unit that affirms people's identity (e.g., using gender-inclusive language on forms and providing gender-inclusive washrooms when possible). Please see Table 1 for further suggestions for creating a positive space.
Creating a Positive Space.
Glossary of Terms
The following terms and definitions may be used differently by different people in different regions and are not standardized. They are compiled from several sources,19,56,57 with the acknowledgement that they will change over time as the thinking, attitudes and discourses around 2SLGBTQ+ issues continue to evolve.