
Abstract
Objective
Although the coronavirus disease 2019 (COVID-19) pandemic has had widespread negative impacts on the mental health of healthcare workers (HCWs), there has been little research on psychological interventions during the pandemic for this population. The current study examines whether a brief coping-focused treatment intervention delivered in a virtual individual format would be associated with positive changes in Canadian HCWs’ mental health during the pandemic.
Method
Three hundred and thirty-three HCWs receiving the intervention at 3 large specialty tertiary care hospitals in Ontario, Canada, completed measures of anxiety, depression, perceived stress, work/social impairment, insomnia and fear of COVID-19. After completing treatment, HCWs rated their satisfaction with the treatment.
Results
The intervention was associated with large effect size improvements in anxiety, depression, perceived stress, insomnia and fear of COVID-19, and moderate effect size improvements in work/social impairment. At treatment session 1, prior mental health diagnosis and treatment were both significantly correlated with depression, anxiety, and work/social impairment scores. Secondary analyses of data from one of the sites revealed that treatment-related changes in anxiety, depression, perceived stress and work/social impairment were independent of age, gender, occupational setting, profession and the presence of a previous mental health diagnosis or treatment, with the exception that nurses improved at a slightly greater rate than other professions in terms of work/social impairment. HCWs were highly satisfied with the treatment.
Conclusions
A large number of HCWs experiencing significant distress at baseline self-referred for assistance. Timely and flexible access to a brief virtual coping-focused intervention was associated with improvements in symptoms and impairment, and treatment response was largely unrelated to demographic or professional characteristics. Short-term psychological interventions for HCWs during a pandemic may have a highly positive impact given their association with improvement in various aspects of HCWs’ mental health improvement.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic had extensive negative mental health impacts. A systematic review across 19 countries revealed that 1 in 3 individuals in the general population reported psychological distress and a higher COVID-19 infection risk was a predictor of depression and anxiety symptoms. 1 Healthcare workers (HCWs) have been at the forefront of the COVID-19 response. Many HCWs were at an increased risk of developing COVID-19 due to their work with infected patients, particularly at the beginning of the pandemic, when many had inadequate access to personal protective equipment and vaccines were not yet available. HCWs worked long hours, experienced stigma/discrimination related to working with COVID patients, and social distancing restrictions and lockdowns interfered with HCWs’ typical coping strategies. 2 Not surprisingly, 84% of HCWs scored higher than the general population on psychological distress. 3
The most commonly studied mental health impacts on HCWs during COVID-19 were depression and anxiety. Thirty-three percent of HCWs reported depression symptoms in a recent systematic review, 4 with 1 study reporting that half of the HCWs showed moderate levels of depression symptoms. 5 Forty-two percent of HCWs reported anxiety symptoms in a systematic review 4 and 24% reported both anxiety and depression symptoms. 6
Stress, insomnia, and COVID-19 fears were also common. Half of the HCWs showed moderate levels of perceived stress in one study 5 and 42% reported insomnia in a systematic review. 4 Finally, almost 42% of HCWs reported feeling fearful about COVID-19 and had anxiety related to becoming infected themselves and/or infecting a loved one. 2 Predictors of HCWs’ mental health symptoms during COVID-19 included younger age,3,6,7 female gender,5,7–9 fear of COVID-19 transmission/family exposure,7,10 being at very high risk for COVID-19, 6 profession11,12 and a history of mental health disorders.13,14
Although calls for HCW mental health support arose following the severe acute respiratory syndrome global outbreak, 15 there is little consensus in the literature on how to best support HCWs’ mental health. A 2020 Cochrane systematic review concluded that there is insufficient evidence from research during/after disease outbreaks, epidemics or pandemics to inform the selection of interventions to assist the mental health of HCWs. 16 A systematic review of psychological support interventions for those exposed to mass infectious disease outbreaks reported positive effects on depression and anxiety but equivocal findings for stress. 17
Despite the widely established negative mental health effects of the pandemic on HCWs, little published work has examined mental health interventions for HCWs during the COVID-19 pandemic. In general, existing studies suggest that brief interventions focused on improving HCWs’ mental health during COVID-19 were associated with reductions in anxiety,18–23 depression,18–21 stress,22,24 and sleep disturbance, 19 while others found no changes in anxiety,25,26 depression, 25 stress,25–27 and insomnia.21,25 The interventions used included resilience enhancement,22–24,28 cognitive behaviour therapy (CBT),18,20,21 acceptance and commitment therapy, 27 and mindfulness.19,25–27 Many of the aforementioned studies had small sample sizes, were conducted outside of North America, and started months to over a year after the pandemic onset. Two Canadian psychotherapy studies were identified20,29; 1 measured 2 of the aforementioned symptoms. 20 Research is needed with Canadian HCWs, who face different circumstances related to the nature of their work, health-care systems (funding, universal health care, resources, etc.), and pandemic prevalence, than HCWs in other parts of the world. Evaluation in the Canadian context may help justify resource allocation, inform sustainability given the ongoing impacts of the pandemic, and provide guidance for future pandemics.
The current study examines government-funded brief therapy interventions developed in 3 Canadian academic hospitals, which were part of a larger provincial collaboration of 5 psychiatric hospitals providing HCW mental health support across Ontario during COVID-19. It is not a clinical trial with uniformity of measures and interventions; rather, it examines naturalistic programming delivered within weeks of the pandemic onset. This study examines 3 questions: 1. Does a brief coping-focused intervention delivered in an individual virtual therapy format decrease symptoms of depression, anxiety, functional impairment, stress, insomnia and fears related to COVID-19? 2. Are demographic variables, including age, gender, occupational setting, profession, prior diagnosis, and prior treatment, (a) correlated with symptom measures at treatment session 1; and (b) predictors of improvements in these variables? 3. Are HCWs satisfied with the treatment provided? Based on the research findings summarized above, we hypothesized that all primary outcomes would be associated with improvement with the treatment intervention; that younger age, female gender, inpatient setting, nursing profession, and presence of prior diagnosis and treatment would be correlated with symptom measures at treatment session 1 and be significant predictors of improvement in the primary outcome variables; and that HCWs would be satisfied with the treatment they received.
Method
Participants
HCWs (N = 333) seeking mental health treatment from 3 large hospitals in Ontario, the Centre for Addiction and Mental Health (CAMH, n = 254), St. Joseph's Healthcare Hamilton (SJHH, n = 35), and Royal Ottawa Mental Health Centre (Royal, n = 44) participated in the study. Participants self-referred for treatment, in response to a broadly internally (within a hospital) and externally (hospital and Ontario ministry websites, social media) advertised provincial initiative to support HCWs whose mental health had been negatively impacted by COVID-19. Each hospital site provided different treatment pathways for HCWs, ranging from low-intensity (e.g., internet-based CBT) to high-intensity (e.g., one-to-one individualized CBT) options, including the brief coping-based treatment intervention that is the focus of this study. The number of participants per site depended on the launch date, other types of mental health support available to HCWs, and the completion of questionnaires. CAMH, situated in Toronto, was the biggest hub, had the largest population to serve, was the first to launch, and had the most referrals. This initiative served HCWs more broadly and not necessarily HCWs from each site.
The overall sample was largely female (89.2%). Just over half the sample was White (58.9%), from the nursing profession (55.7%), and had an average age of 35.87 (SD = 9.87). Slightly less than half of the sample reported a previous mental health diagnosis (43.3%) and approximately half (51.2%) reported prior treatment for a mental health issue. Table 1 presents the demographic breakdown by hospital site.
Demographic, Diagnostic, and Professional Characteristics of the Healthcare Workers by Site.
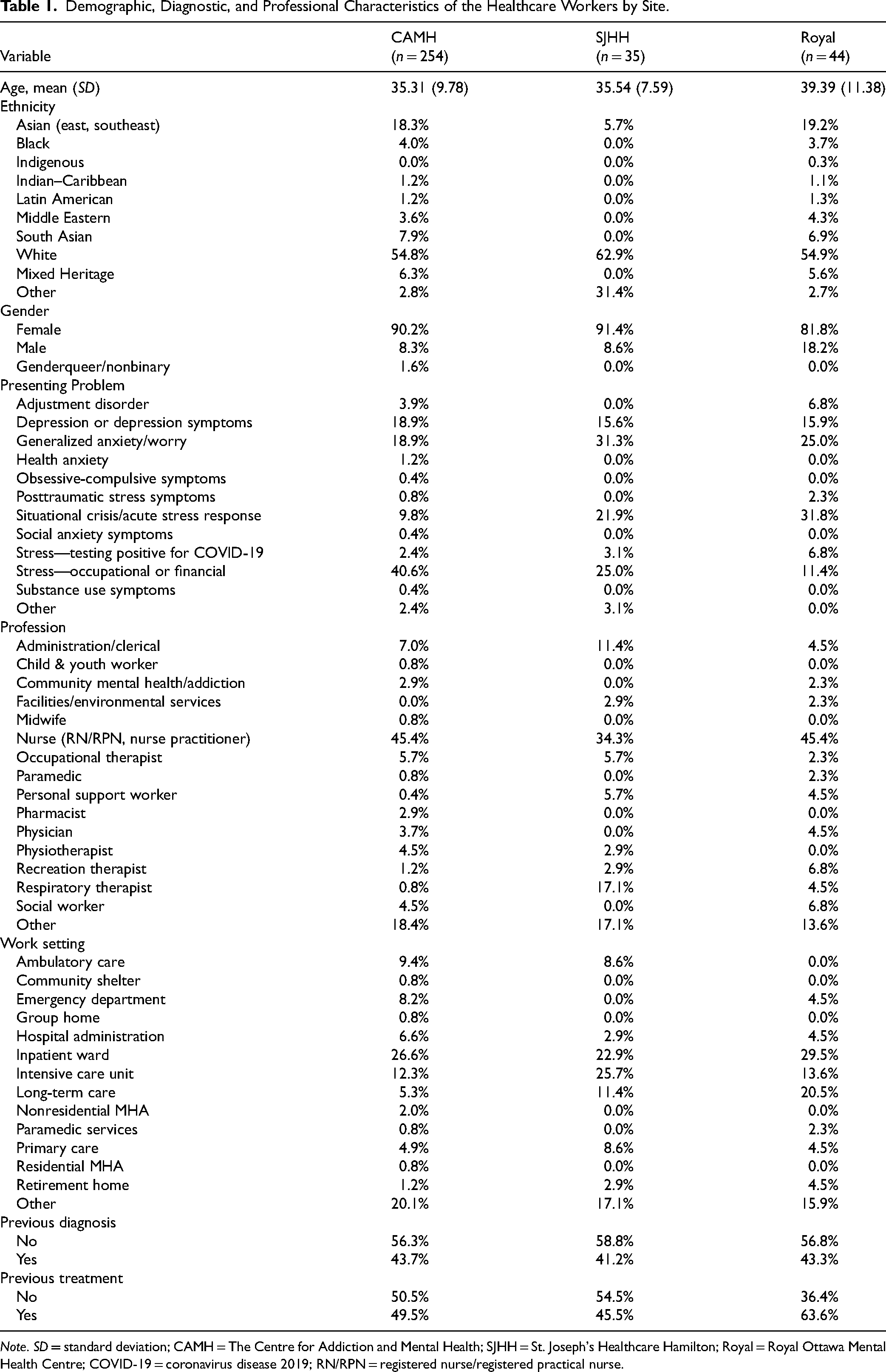
Note. SD = standard deviation; CAMH = The Centre for Addiction and Mental Health; SJHH = St. Joseph's Healthcare Hamilton; Royal = Royal Ottawa Mental Health Centre; COVID-19 = coronavirus disease 2019; RN/RPN = registered nurse/registered practical nurse.
Assessment
Participants completed a pretreatment semistructured clinical assessment (content varied by site), which identified the main presenting issue and informed treatment disposition (based on the nature and severity of symptoms, and HCW preferences). Demographic and professional characteristics collected included age, ethnicity, gender, profession, work setting and prior mental health diagnosis or treatment.
Measures
Patient Health Questionnaire 9 (PHQ-9). 30 Depression symptom severity was assessed with the PHQ-9, a 9-item measure rated on a scale of 0 = not at all to 3 = nearly every day. The PHQ-9 has demonstrated excellent reliability and validity.30,31 Reliability in the current study was high, preα = 0.86 and postα = 0.91.
Generalized Anxiety Questionnaire 7 (GAD-7). 32 Symptoms of anxiety were measured with the GAD-7, a 7-item measure rated on a scale of 0 = not at all to 3 = nearly every day. The reliability and validity of the GAD-7 are well established.32,33 Reliability in the current study was high, preα = 0.87 and postα = 0.89.
The Work Social Adjustment Scale (WSAS). 34 The WSAS assesses functional impairment with 5 items rating of how much mental health impairs one's ability to carry out various activities related to work, home management, social leisure activities, private leisure activities and close relationships, on a scale where 0 = not at all and 8 = very severely. Lower total scores reflect better adjustment, and the scale has established reliability and validity indices. 34 In the current study, reliability was high, preα = 0.82 and postα = 0.92.
The Perceived Stress Scale (PSS). 35 Individual stress levels were assessed with the PSS. Across 10 items, respondents rate how often they thought or felt a certain way, where 0 = never to 4 = very often. The timeframe for the scale was changed to the last week (instead of the month). Higher total scores correspond to higher perceived stress. The PSS has good reliability and validity. 35 The current study's reliability was high, preα = 0.85 and postα = 0.92. This measure was not used as a proxy for traumatic stress.
The Fear of COVID-19 Scale (FCS). 36 The FCS is a 7-item measure assessing fears of COVID-19 on a scale ranging from 1 = strongly agree to 5 = strongly disagree. Example items include “I am afraid of losing my life because of the coronavirus” and “It makes me uncomfortable to think about coronavirus.” It is valid and reliable in assessing the fear of COVID-19 in the general population. 36 In the current study, reliability was high, preα = 0.89 and postα = 0.89.
The Insomnia Severity Index (ISI). 37 With 7 items, the ISI assesses the impact and severity of insomnia symptoms. Respondents rate items on a 5-point scale, where 0 = no problem and 4 = very severe problem. The scale has good reliability and validity. 37 In the current study, reliability was very strong, preα = 0.90 and postα = 0.92. This measure was not used as a proxy for traumatic stress.
Satisfaction. Treatment satisfaction at CAMH was assessed with 8 items rated on a 4-point scale of agreement where 1 = strongly disagree and 4 = strongly agree: 1. “I think the services provided here are of high quality.” 2. “If a friend was in need of similar help I would recommend this service.” 3. “The number of treatment sessions provided was what I needed.” 4. “As a result of this individual service, I gained some new skills to help with my mood/anxiety/coping.” 5. “As a result of this individual service, I was able to reinforce skills that I knew already, to help with my mood/anxiety/coping.” 6. “I utilized time outside of the session to work on the skills being reviewed (e.g., completed the homework tasks).” 7. “The availability of a variety of appointment time slots was very helpful.” 8. “The services I have received have helped me deal more effectively with my life challenges.” SJHH asked “How satisfied are you with the COVID-19 Mental Health and Psychosocial Support Service,” on a scale of 0 (not at all) to 100 (fully satisfied).
Procedure
Treatment for HCWs was provided by a multidisciplinary team in anxiety and mood disorder clinics, consisting of psychologists, social workers, occupational therapists, registered psychotherapists, and nurses (composition varied by site). The initiatives were launched in early April 2020 (CAMH) and May 2020 (SJHH, Royal). The data presented were collected from the launch dates to December 2021. All sites provided the treatment intervention in a virtual format (infrequently via phone if needed), and each site focused the brief treatment intervention largely on coping; however, this was provided in slightly different ways across sites (see Table 2). The time between assessment and starting treatment was typically 1 to 2 weeks.
HCW Brief Treatment Intervention Details by Hospital Site.
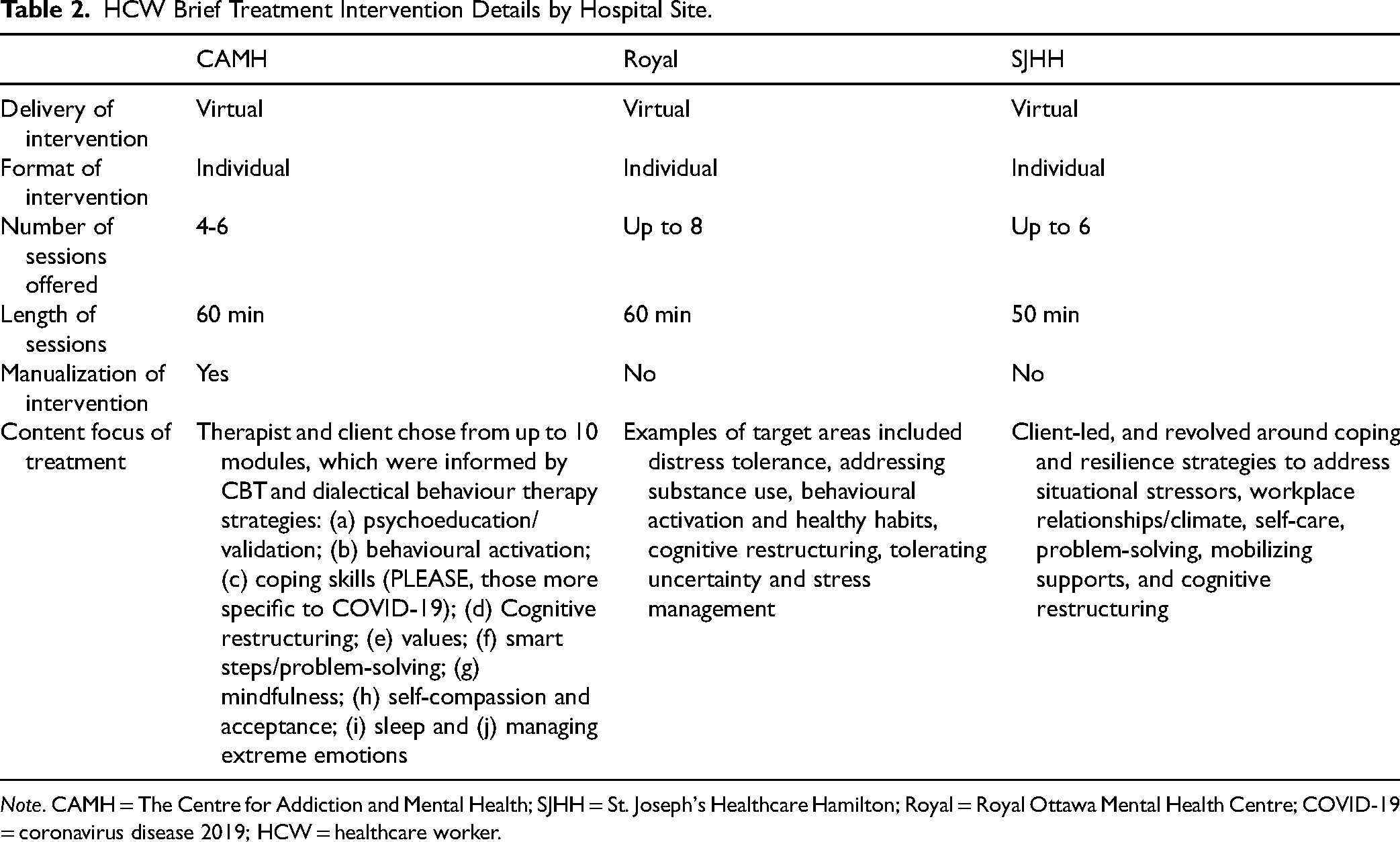
Note. CAMH = The Centre for Addiction and Mental Health; SJHH = St. Joseph's Healthcare Hamilton; Royal = Royal Ottawa Mental Health Centre; COVID-19 = coronavirus disease 2019; HCW = healthcare worker.
At all sites, participants completed self-report questionnaires pretreatment and posttreatment, and CAMH participants also completed them weekly. All sites used the PHQ-9 and GAD-7. CAMH and the Royal included the WSAS, whereas the PSS was only given at CAMH, and the ISI and FCS were only given at SJHH. The research was approved by the hospital Research Ethics Boards (CAMH REB No. 086/2020, consent form requirement waived; SJHH REB No. 12842, written consent obtained) or exemption was provided (Royal). At SJHH, 93% of HCWs consented; declines were largely due to their distress.
Data Analysis
Primary outcomes for the full sample across all sites (N = 333) with complete data for each measure at both time points were assessed by paired samples t-tests, and results are presented with Cohen's d as the effect size (small = 0.2, medium = 0.5, and large = 0.8). 38 All participants had complete data at both pretreatment and posttreatment; no missing data were accounted for in these primary analyses.
Due to the availability of weekly data at CAMH, a secondary analysis was performed within the CAMH sample (n = 254) to assess predictors of change across 6 time points, from treatment week 1 to week 6. To evaluate the impact of predictors on change in outcome variables over time, hierarchical linear modelling (HLM) was conducted. 39 HLM was used given its ability to evaluate individual differences in the trajectory of change over time, and because it can accommodate missing data at Level 1. Level 1 outcome variables included GAD-7, PHQ-9, PSS, and WSAS, and Level-2 predictors of change included age, gender, previous mental health diagnosis (yes/no), previous treatment for a mental health diagnosis (yes/no), occupational setting (inpatient unit vs. other), and profession (nurses vs. other). Levels of missing data were the same for each outcome variable (including PHQ-9, GAD-7, WSAS, and PSS), and data were missing at random, as indicated by Little's missing completely at random (MCAR) test (χ2 = 127.39, df = 112, p = .152).
Results
Primary Outcome Variables
There were no differences between the 3 sites at baseline for the PHQ-9, F(2, 226) = .02, p = .982, and the GAD-7, F(2, 225) = 2.82, p = .062, and there was no difference in WSAS between CAMH and Royal, t(190) = .75, p = .455, so data remained pooled. At the start of treatment, depression and anxiety scores were both in the moderate severity range. The average number of treatment sessions attended was 3.09 (CAMH), 3.0 (SJHH), and 6.66 (Royal).
Results of primary outcomes are summarized in Table 3. The GAD-7 and PHQ-9 both decreased significantly from pretreatment to posttreatment, indicating improvements in anxiety and depressive symptoms, respectively, with large treatment effect sizes. For both measures, participants moved from the moderate to mild severity range. The WSAS also decreased significantly, indicating a medium treatment effect size in an improved ability to carry out day-to-day tasks related to work and social settings. Perceived stress improved significantly within the moderate severity range from pretreatment to posttreatment, with a large effect size. Additionally, FCS and ISI scores had reduced significantly at posttreatment, indicating improvements in fears related to COVID-19 and severity of insomnia symptoms, with large effect sizes. Insomnia decreased from the top to bottom of the subthreshold insomnia severity range.
Change in Primary Outcome Variables From Pretreatment to Posttreatment.
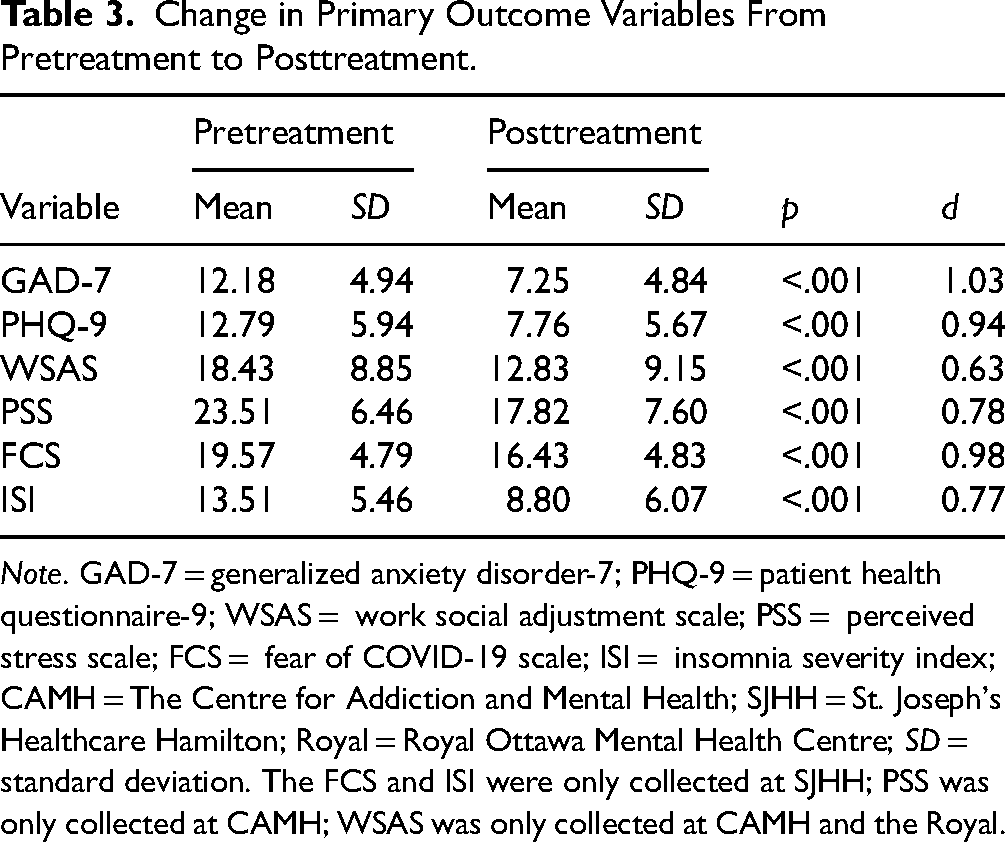
Note. GAD-7 = generalized anxiety disorder-7; PHQ-9 = patient health questionnaire-9; WSAS = work social adjustment scale; PSS = perceived stress scale; FCS = fear of COVID-19 scale; ISI = insomnia severity index; CAMH = The Centre for Addiction and Mental Health; SJHH = St. Joseph's Healthcare Hamilton; Royal = Royal Ottawa Mental Health Centre; SD = standard deviation. The FCS and ISI were only collected at SJHH; PSS was only collected at CAMH; WSAS was only collected at CAMH and the Royal.
Correlations between demographic predictors and session 1 symptom scores across all sites are presented in Table 4. Prior diagnosis was significantly correlated with depression, anxiety, and stress scores, and prior treatment was significantly correlated with depression, anxiety, stress, and work/social impairment. All other correlations were not significant.
Correlations Between Demographic Variables and Pretreatment Symptom Severity Measures Across All Sites.
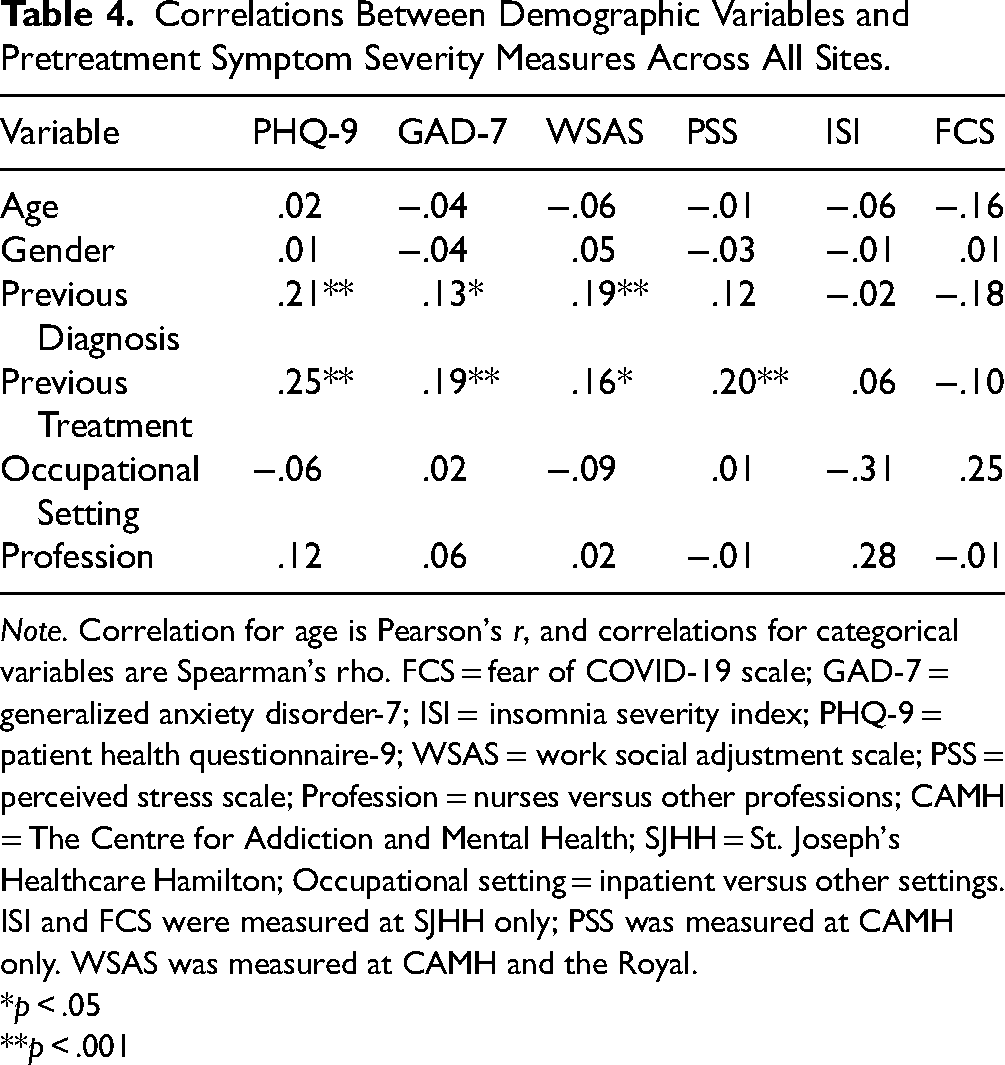
Note. Correlation for age is Pearson's r, and correlations for categorical variables are Spearman's rho. FCS = fear of COVID-19 scale; GAD-7 = generalized anxiety disorder-7; ISI = insomnia severity index; PHQ-9 = patient health questionnaire-9; WSAS = work social adjustment scale; PSS = perceived stress scale; Profession = nurses versus other professions; CAMH = The Centre for Addiction and Mental Health; SJHH = St. Joseph's Healthcare Hamilton; Occupational setting = inpatient versus other settings. ISI and FCS were measured at SJHH only; PSS was measured at CAMH only. WSAS was measured at CAMH and the Royal.
*p < .05
**p < .001
Secondary Analyses
Full results of the HLM analyses for the CAMH site weekly data are presented in Supplementary Table. Each outcome variable significantly improved over the course of treatment (ps < .001). However, only 1 of the Level-2 predictors demonstrated a significant effect on the trajectory of change in outcomes over the course of treatment. Specifically, nurses improved at a slightly greater rate on the WSAS as compared to others (b = .48, SE = .24, t = 2.04, p = .042, d = .013). The remainder were not significant (ps > .05), indicating that treatment effects are independent of age, gender, the presence of a previous diagnosis or previous treatment, or occupational setting.
Satisfaction Results
Overall, satisfaction ratings across the items were high; see Table 5.
Satisfaction Results.
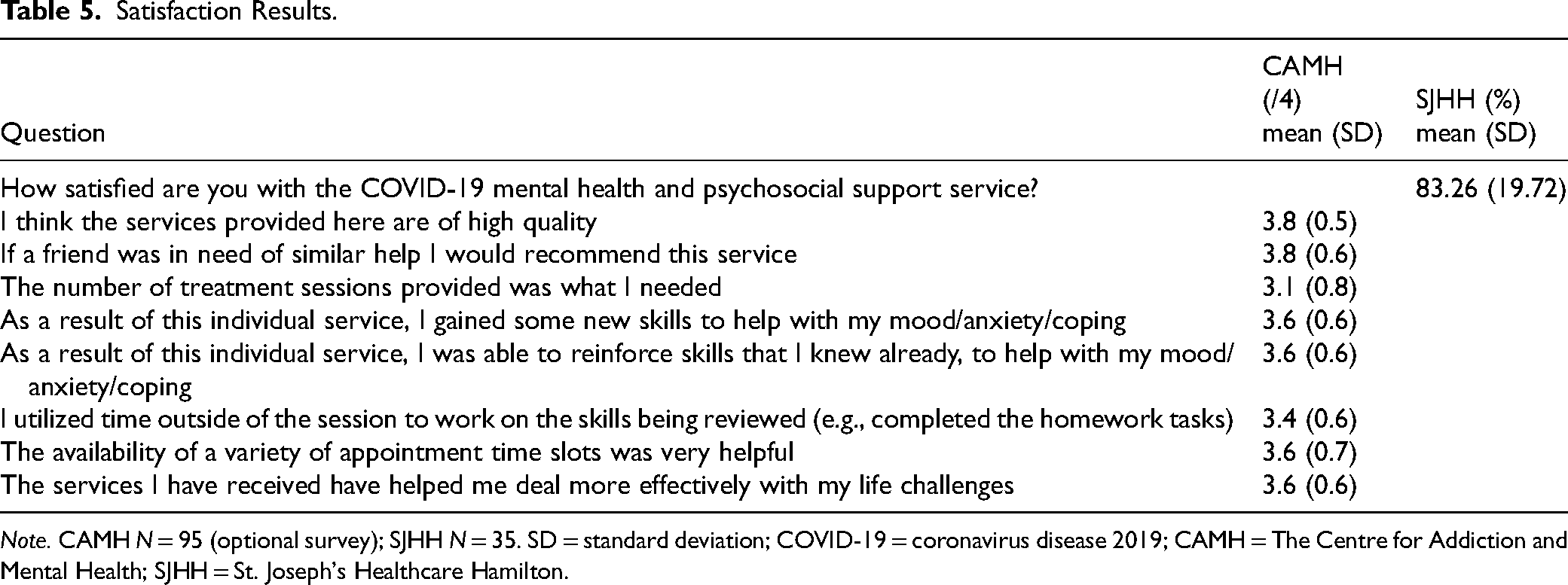
Note. CAMH N = 95 (optional survey); SJHH N = 35. SD = standard deviation; COVID-19 = coronavirus disease 2019; CAMH = The Centre for Addiction and Mental Health; SJHH = St. Joseph's Healthcare Hamilton.
Discussion
To address the limited research on supporting HCWs’ mental health during pandemics, the current study evaluated a brief psychotherapy intervention for HCWs during COVID-19, developed at 3 Ontario hospitals. Consistent with our hypotheses, the intervention was significantly associated with decreases in symptoms of anxiety, depression, perceived stress, insomnia and fear of COVID-19. It is noteworthy that all of these domains showed large effect size improvements, despite the short-term and virtual nature of the treatment. Virtual treatment was significantly associated with improvements in this population, likely in part due to the ease of access and the ability to seek assistance outside of their home institution. In addition, there were no differences between hospitals on shared measures. Work/social impairment also significantly decreased, albeit with moderate effect size changes. Consistent with existing evidence, 40 larger changes were seen in the symptom areas themselves than in the impairment from those symptoms, although the latter still improved significantly. Improvements in depression and anxiety symptoms replicate prior work on HCW treatment during COVID-19,18–23,41 with a larger and Canadian sample. The current study extends the literature to reveal positive changes associated with treatment in perceived stress,22,24 fear of COVID-19 and insomnia, all of which have been reported at high levels in HCWs during the pandemic.
In line with our hypotheses, at session 1, prior treatment was significantly positively correlated with depression, anxiety, work/social impairment scores, and perceived stress symptom scores; previous diagnosis showed the same pattern with the exception of no significant correlation with perceived stress. In contrast, none of the symptom variables were significantly related to age, gender, occupational setting or profession. The vast majority of HCWs who self-referred for treatment identified as female, which may have precluded the detection of gender effects. Contrary to our hypotheses, improvements in symptoms of anxiety, depression, perceived stress and work/social impairment were independent of gender, age, setting and the presence of prior mental health diagnoses or treatment. This speaks to the impact of the intervention provided, as it was found to be associated with large improvements for diverse HCWs, from various workplace settings, and for those who engage in various healthcare-related work tasks. One exception to this is that nurses improved at a slightly greater rate than other professions in the area of work/social impairment, although this is difficult to interpret given that nurses were compared to a wide variety of other professions. Future research exploring the impacts on different professions is warranted. Importantly, although prior mental health diagnoses or treatments were associated with more severe symptoms among HCWs at the start of treatment, prior mental health status was not associated with treatment response.
Of note, although 333 is by far the largest sample among HCW COVID-19 psychotherapy studies, this number also represents a low percentage of Ontario HCWs. The brief intervention was one of the several options available to HCWs who self-referred for assistance (e.g., iCBT, medication consultation, etc.). Nevertheless, not all distressed HCWs sought treatment, which may help explain the null results for gender and age. Furthermore, 89% of the sample was female; other studies had 100%.18,19 This is explained in part by the higher percentage of nurses who identify as female, females having higher prevalence of mood and anxiety-related disorders, 42 and being more likely to seek treatment for mental and physical health. 43 Additional research is required to understand who among distressed HCWs do not seek mental health assistance and why. Potential barriers include feeling too burnt out or time-strapped to engage in psychotherapy and stigma around treatment-seeking among HCWs. Anecdotally, several HCWs expressed guilt about burdening other HCWs by taking time to attend to their mental health, particularly if they took a medical leave.
Lastly, we sought to examine the degree to which HCWs were satisfied with their treatment experience. Among the 2 sites that assessed this, HCWs were highly satisfied with their treatment, with most average scores ranging from 83% to 95%. Acceptability of the treatment is crucial for HCWs, and these high ratings suggest that HCWs are receptive to this brief intervention, in addition to it being associated with positive improvements for them. The lowest-ranked item, at 78%, was the number of sessions was what was needed. Future directions involve collecting qualitative data to better understand which aspects were helpful, and the optimal number of sessions.
Several clinical aspects may have contributed to the positive improvements associated with these treatment interventions. HCWs self-referred and were rapidly assessed and offered treatment. One site included direct online booking. HCWs started treatment within 2 weeks of referral, meeting their mental health needs in a timely manner. Previous research shows that longer wait times negatively impact treatment outcomes, independent of the quality of treatment. 44 We were able to offer flexible scheduling by accommodating shiftwork and providing daytime and early evening sessions. Thus, offering service quickly, and with low barriers, may be equally important as treatment quality. Furthermore, treatment was delivered individually, which was valued by HCWs. 2 Live contact with a mental health professional was important. The findings of Fiol-DeRoque et al. 25 revealed that an app intervention led to no between-group changes (intervention vs. control group) for HCWs; however, those already receiving psychological treatment did improve, 25 suggesting that live contact is important. Anecdotally, it was important for some HCWs to have access to hospital-based clinicians, who might be more likely to understand the context and were highly experienced in treating anxiety, mood, and trauma symptoms. In addition, the treatment was publicly funded by the Ontario government, which removed financial barriers. Lastly, all treatments were delivered virtually, a necessity during the pandemic, which in turn likely improved access to the treatment (decreased travel time to receive treatment, accessible to HCWs in more rural areas in the province). The importance of readily accessible, high-quality treatment is underscored by the finding that psychological support for HCWs was associated with decreased morbidity. 14
The study findings are tempered by some limitations. Each hospital site offered a different number of sessions and slightly different treatments, although there was significant overlap in concepts and interventions. Despite this, no between-site differences emerged in the shared outcome measures. Given that we did not have sufficient resolution of data to factor differing treatment lengths into the analysis, the adoption of an intent-to-treat approach may have suppressed predictor effects. Not all sites included all of the same measures. The participants largely self-identified as female, which although consistent with the large proportion of nurses, restrict the generalizability of the findings. Many professions were underrepresented in the sample. The self-referral nature of the study precluded representative sampling of occupational settings and professions, so finer-grain analyses in these areas were not possible. Measures of posttraumatic stress and moral injury were not included. Finally, the lack of randomization to a control comparison limits the ability to rule out effects due to other factors, such as the passage of time, nonspecific factors and regression to the mean. A future research direction is to include weekly questionnaires at all sites. One site conducted double the average number of sessions with no significant difference in effect size, and weekly data may pinpoint an optimal ratio of sessions to symptom improvement. Furthermore, one could evaluate whether the intervention is helpful as a future prevention strategy, that is, to proactively prevent, as well as respond to, distressed HCWs.
Conclusion
A substantial number of HCWs in significant distress accessed a provincial mental health resource during the COVID-19 pandemic. Offering timely and flexible access to a brief virtual treatment intervention that largely focused on coping was associated with positive impacts on symptoms (anxiety, depression, stress, insomnia, and fears of COVID-19) and impairment related to symptom burden. The sample was heterogeneous, yet the response to treatment was largely unrelated to demographic or professional characteristics, supporting the robustness of the treatment outcomes. For the healthcare system to function effectively, it is crucial that HCWs receive rapid access to mental health support when needed. The current study provides an example of how a well-received brief treatment intervention was associated with several mental health improvements among HCWs during COVID-19, which may help inform the planning of supporting the mental health needs of HCWs in future pandemics or healthcare crises.
Data Access
Given the multisite format and varying forms of REB approval/waiver, data access is not available.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437231187462 - Supplemental material for A Rapid Access Brief Psychotherapy Intervention to Respond to Healthcare Workers in Ontario Whose Mental Health was Negatively Impacted During the COVID-19 Pandemic
Supplemental material, sj-docx-1-cpa-10.1177_07067437231187462 for A Rapid Access Brief Psychotherapy Intervention to Respond to Healthcare Workers in Ontario Whose Mental Health was Negatively Impacted During the COVID-19 Pandemic by Judith M. Laposa, Duncan Cameron, Kim Corace, Natalie Quick, Karen Rowa, Cary Kogan, Stephanie Carter, Irena Milosevic, Sara de la Salle, Vicky Stergiopoulos, Joseph Pellizzari, Erika Haber, Paul Kurdyak, and Randi E. McCabe in The Canadian Journal of Psychiatry
Footnotes
Acknowledgements
We would like to thank the HCW participants for their phenomenal service during the pandemic, as well as the treatment providers in the current study, who were themselves HCWs. Thanks also goes to the hospital administrations at the Centre for Addiction and Mental Health, St. Joseph's Healthcare Hamilton, and Royal Ottawa Mental Health Centre, who very quickly initiated mental health support for HCWs when the pandemic started, as well as to the Ontario government, for funding these important services for HCWs.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.