
Abstract
Aim
To assess the incremental cost-effectiveness ratio (ICER) of group transdiagnostic cognitive-behavioural therapy (tCBT) added to treatment as usual (TAU) for anxiety disorders compared to TAU only from the healthcare system perspective over a 1-year time horizon.
Methods
Data from a pragmatic multisite randomized controlled trial where adults (18–65 years) with an anxiety disorder were randomized to tCBT + TAU (n = 117) or TAU (n = 114). Group tCBT is a 12-week (2h weekly sessions) community-based intervention. Health service utilization and related costs were captured from medico-administrative data and included those for the intervention, ambulatory visits, hospitalizations and medications. Effectiveness was based on quality-adjusted life years (QALYs). The study included measures at baseline, 4, 8, and 12 months. Intention-to-treat and complete case analyses were carried out. Missing data were imputed using multiple imputation analyses. Seemingly unrelated regression analyses were used to assess the effect of the intervention on total costs and QALYs while also adjusting for baseline confounders. The probability of cost-effectiveness of the intervention was assessed according to different willingness-to-pay (WTP) thresholds using the net benefit regression method.
Results
The ICER of tCBT + TAU as compared to TAU in the intention-to-treat analysis was $6,581/QALY. Complete case analyses showed a similar ICER of $6,642/QALY. The probability at a WTP threshold of $20,000 and $40,000 that tCBT + TAU as compared to TAU is cost-effective is 93.0% and 99.9%.
Conclusion
tCBT added to TAU appears to be cost-effective from the healthcare system perspective for treating adult patients with anxiety disorders. Larger trials including young and older adults as well as a range of anxiety disorders are needed to further investigate the cost-effectiveness of tCBT in different patient populations.
Introduction
Anxiety disorders are the most prevalent common mental disorders with past-year prevalence in adults between 8.4% and 21.3%.1,2 Anxiety disorders are also associated with increased health care costs.3,4 Although the long-term effects of the pandemic on the chronicity of anxiety disorders remain to be studied, 5 the increase in anxiety symptoms and severity 6 and increased mental health service needs 7 will most likely add to the strain of limited human resources in the healthcare system.
In Canada, the majority of patients with anxiety disorders consult in primary care.8,9 Clinical recommendations for anxiety disorders include evidence-informed pharmacological options and psychotherapy such as cognitive-behavioural therapy (CBT) for generalized anxiety disorder, panic disorder, social phobia, and agoraphobia. 10 Although psychotherapy is preferred by patients, 11 pharmacological treatments are still the most prescribed option12,13 due to their wider coverage under public and private drug insurance plans. 14 Barriers to accessing psychotherapy in Canada include insufficient funding, long waiting lists in the public sector and high out-of-pocket costs in consulting in the private sector.15,16 Sustainable solutions for community-based primary mental health interventions include increasing access to psychotherapy in primary care,15,16 which has been shown to be cost-effective.17,18
Among individuals reporting a lifetime anxiety disorder, 56% and 20% will also report at least two and three comorbid anxiety disorders at one point in their lifetime. 19 Transdiagnostic CBT (tCBT) therapy is a promising intervention that can be offered to individuals with a range of anxiety disorders in group therapy. The option of creating groups consisting of individuals with different anxiety disorders can improve timely access to psychological treatment of anxiety disorders by reducing the human resources required for individual anxiety-specific treatment protocols.20-24 This evidence-based intervention has been developed based on common processes observed across a range of anxiety and depressive disorders and aims to treat multiple anxiety disorders simultaneously by targeting negative affectivity/neuroticism.20,24 The effectiveness of group tCBT for the treatment of anxiety disorders has been reported with findings showing improvements in anxiety symptoms, social functioning and quality of life as well as reductions in comorbid anxiety and depressive disorders.25-28 Although the benefits of this intervention have been studied, rare are the studies that have looked at its cost-effectiveness. 28
The aim of this study was to assess the cost-effectiveness of group tCBT with treatment as usual (tCBT + TAU) for anxiety disorders compared to TAU from the healthcare system perspective over a 1-year time horizon in community-based primary care settings using data from a pragmatic multisite randomized controlled trial (RCT). Findings from this trial showed improved self-reported and clinician-rated severity of anxiety disorders from baseline to 12 months postrandomization in individuals randomized to group tCBT + TAU as compared to TAU. 26 A cost-effectiveness study over an 8-month time horizon using self-reported data from the same trial showed a high probability that tCBT was cost-effective from a societal perspective. 29 An earlier study had shown a significant reduction in health service utilization and costs in individuals with anxiety disorders up to 1-year following CBT treatment. 30 By linking health survey and medico-administrative data on health service use, and therefore limiting information bias associated with recall and loss to follow-up and the control of a number of confounders, this study included an additional 4 months of follow-up and assesses over a 1-year period the costs and effects of receiving group tCBT + TAU compared to TAU in a community-based sample of adults with anxiety disorders. We expect that the additional follow-up will allow for more precise estimates of the long-term cost-effectiveness of the intervention and inform decision makers as to its cost-effectiveness in the context of a Canadian public healthcare system context.
Methods
The study design is a pragmatic, multicentre, 2-arm parallel, single-blind, superiority RCT conducted in 3 regions in Quebec, Canada (trial registration: https://clinicaltrials.gov/ct2/show/NCT02811458) and has been described elsewhere. 31 The RCT included 231 participants of which 117 were randomized to tCBT + TAU and 114 to TAU arm. Participants were recruited through advertisements in Google AdWords, Facebook, newspapers, and bulletin ads in the community. Interested adults were invited to complete an online survey on eligibility criteria. Eligible participants were then contacted for a short telephone interview. The final step of verifying participants’ eligibility was assessed with the Anxiety and Related Disorders Interview Schedule for DSM-5 (ADIS-5) 32 through a face-to-face interview (baseline, T0). Participants provided written informed consent.
The study was conducted among French-speaking adults aged 18 to 65 years with an anxiety disorder meeting DSM-5 criteria (social anxiety, panic disorder, agoraphobia, and generalized anxiety disorder) and a score of ≥4 on the clinical severity rating, indicating clinical threshold (disabling disorder) on the ADIS-5 (ranging from 0, no symptoms, to 8, severe symptoms). 32 Participants with the following conditions were excluded from the study: cognitive impairment, bipolar disorders, psychosis, substance-related and addictive disorders and active suicidal behaviour. Participants having consulted in the last 12 months with a psychiatrist were also excluded. These patients may reflect more complex clinical profiles that necessitate more specialized mental health care and active follow-up. Although it is common in clinical practice for psychiatrists to refer patients to psychotherapy in various settings (e.g., community, private practice, and hospital), these individuals had already received specialized care reflecting different health service use trajectories. Considering a stepped-care approach, the current study focused on individuals consulting in community and primary care settings with and without physician referrals. At each study site, patients meeting eligibility criteria were randomized (1:1) by blocks of 4 into the intervention (tCBT + TAU) or the control group (TAU).
Data collection and assessments for the tCBT + TAU arm included face-to-face assessments at baseline (T0) and at 4 months postrandomization, corresponding to posttreatment (T1), telephone interview at 8 months postrandomization (posttreatment + 4 months, T2) and face-to-face assessment at 12 months postrandomization (posttreatment + 8 months, T3). For individuals in the TAU arm, the study included prerandomization face-to-face assessments at baseline (T0), telephone interviews at 4 months (T1) and 8 months (T2), and face-to-face assessment at 12 months (T3). Information collected from the RCT was linked to provincial medico-administrative data on health and drug service utilization for the 12 months preceding and following baseline (T0). Of the 231 individuals randomized to either group, 218 participants gave consent to access their provincial medico-administrative data on health service utilization and the remaining 13 participants were considered to have missing information on medico-administrative data.
Measures
Intervention
The 12-week community-based transdiagnostic CBT (tCBT)31,33 in primary care settings consisted of a 2 h session on a weekly basis and included 4 components: (1) education and self-monitoring of symptoms, (2) specific and (3) generalized cognitive restructuring, and (4) response prevention and graduated exposure. Treatment components are delivered according to a set protocol: education and self-monitoring (session 1), specific cognitive restructuring (sessions 2 and 3), exposure and response prevention (sessions 4–9), and generalized cognitive restructuring (sessions 10 and 11), with the final 12th session focusing on termination and relapse prevention issues. The treatment groups were composed of 10 participants on average. Sessions were conducted by trained PhD-level psychologists assisted by psychologists and psychotherapists from the public health sector. PhD-level psychologists received a 2-day training workshop with the developer of the tCBT protocol (PJN) and a gratis copy of the published treatment manual. Psychotherapists joining the project after the workshop received individual training from a trained PhD-level psychologist (MDP). There were case discussions with all psychotherapists throughout the study period. 31
The comparator was TAU, which may have included consultations with physicians and mental health specialists in the private or public sector, psychotherapy or psychotropic drug use. A complete description of the intervention and study methods has been previously published.26,31,33 Additional information on the intervention is in the Supplemental Material.
Economic Evaluation
Health care Costs Related to Health Service Utilization
The economic evaluation was carried out from the healthcare system perspective over a 1-year time horizon. Health care costs were measured from the healthcare system perspective in the year preceding and following baseline (T0). Residents of Quebec are covered for the majority of their medical consultations under the province's public medical insurance plan. For residents not having private drug insurance coverage, the province's public drug plan will cover drug costs for medications on the provincial formulary. Costs included those incurred for health services during ambulatory visits (cost/visit), hospitalizations (per diem), medications covered under the public drug plan and physician fees paid for consultations and medical acts. Costs not covered by the health system are those incurred by the patient for receipt of services from health professionals in the private sector such as psychologists and medications for individuals covered under a private drug insurance plan.
Health care utilization for any health problem and related costs were ascertained from information found in provincial medical and pharmaceutical administrative databases (Supplemental Table S1). The cost related to the intervention for a training course also included professional training and supervision as well as time spent for intervention and preparation.
Cost estimation was based on previously published methods34-36 and economic evaluation guidelines37,38 using the direct allocation approach. The description of unit costs is presented in Supplemental Table S1. The detailed methodology used is described elsewhere. 36
Quality-Adjusted Life Years
The EQ-5D-5L was used to assess health-related quality of life on a 5-level rating scale ranging from no problem to extreme problems. 39 A summary health utility is calculated by applying Canadian weights to each response level to the 5 questions. 40 The total 1-year quality-adjusted life year (QALY; details in the Supplemental Material) is based on the EQ-5D-5L health utilities 40 measured at T0, T1, T2, and T3 and by calculating the area under the curve during the 1-year observation period [(((T0 + T1)/2) × 4months) + (((T1 + T2)/2) × 4months) + (((T2 + T3)/2) × 4months)/12months]. 38
Other Covariables
Study covariables included sociodemographic and clinical characteristics defined in the Supplemental Material.
Statistical Analysis
Nonparametric and parametric descriptive (Mann–Whitney test, Student's t-test and chi-square statistics) and bivariate analyses (generalized linear models with log link and gamma distribution) were conducted to assess the association between the intervention and health care costs, health care utilization, QALYs, and study variables.
The current economic evaluation included an intention-to-treat analysis and additional complete case analyses that considered individuals with complete follow-up information. Challenges in analyses of data and the valid conclusions in economic evaluations include the importance of accounting for differences in baseline characteristics and potential important confounders, missing data throughout follow-up, skewed distribution of costs and the correlation between costs and QALYs.41,42 It has been shown that seemingly unrelated regression analyses correcting for confounders with multiple imputations address all 4 challenges. 42
In order to estimate the cost-effectiveness of tCBT + TAU as compared to TAU, in the intent-to-treat analysis, we first carried out multiple imputations using chained equations for missing data on total healthcare system costs and QALYs and potential study confounders.43-45 There were 45 imputed datasets that corresponded to the percentage of individuals with incomplete data, 46 and the mean and standard error of the mean (SEM) of the means of each multiple imputation was estimated with Rubin's rule. 47
The total healthcare system costs and QALYs associated with the intervention were studied with seemingly unrelated regression analysis, to account for the correlation between the costs and QALYs, where 2 separate regression models are specified simultaneously, that is, one for total costs and QALYs.48,49 Total costs were adjusted for past-year total healthcare system costs and baseline primary diagnosis of anxiety disorder, depression symptom severity, and psychotropic drug use. QALYs were adjusted for baseline preference-based index value, primary diagnosis of anxiety disorder, depression symptom severity, and psychotropic drug use.
The incremental cost-effectiveness ratio (ICER) was calculated using the difference in mean point estimates in costs divided by the difference in mean QALYs, associated with tCBT + TAU as compared to TAU, with the following formula: ICER = ΔC/ΔE = (CtCBT+TAU − CTAU)/(QALYtCBT+TAU – QALYTAU). 38 The cost-effectiveness of tCBT + TAU as compared to TAU was assessed with the net benefit regression method50,51 across a range of willingness-to-pay (WTP) thresholds relevant to the Canadian context, 52 with uncertainty explored by cost-effectiveness acceptability curves (CEAC). 53 These are presented by plotting the probability (y-axis) that tCBT + TAU as compared to TAU is cost-effective for a range of WTP values ranging up to $140,000 (x-axis).53,54 For this, we calculated the net monetary benefit (NMB) for each individual, which combines economic and health outcomes such as the QALY in a dollar amount 55 with the following formula: [NMB = (WTP × QALY) – costs]. For different WTP thresholds, multiple regression analyses were carried out to study the NMB as a function of the intervention (tCBT + TAU versus TAU) controlling for baseline primary diagnosis of anxiety disorder, depression symptom severity, psychotropic drug use, health-related quality of life at baseline and past-year total healthcare system costs. Regression analyses were carried out on imputed data for intent-to-treat and complete case analyses. All analyses were carried out with SAS version 9.4.
Results
The flowchart of the study is presented in the Supplemental Material. Among the 231 participants randomized, 218 (94%) gave access to their medico-administrative data of which, n = 112 were randomized to the tCBT + TAU and n = 106 to the TAU groups had similar sociodemographic and clinical characteristics except for the primary diagnosis and comorbid diagnoses (Table 1). At the baseline, the 2 groups had similar scores on health-related quality of life (HRQOL) on the EQ-5D-5L and the EQ-Visual Analogue Scale. Retention rates at follow-up were 86% (T1), 74% (T2) and 72% (T3). In general, the tCBT + TAU group had on average better HRQOL than the TAU group at T1, T2, and T3 (p < 0.05) (Table 2). The difference in EQ-5D-5L index scores between tCBT + TAU and TAU at T1, T2, and T3 was 0.08 (p < 0.001), 0.04 (p = 0.057), and 0.04 (p = 0.032), respectively. The difference in visual analogue scores between tCBT + TAU and TAU at T1, T2, and T3 was 6.3 (p = 0.004), 5.8 (p = 0.004), and 5.4 (p = 0.025), respectively. The difference in patient healthcare questionnaire-9 scores between tCBT + TAU and TAU at T1, T2, and T3 was −3.4 (p < 0.001), −2.1 (p = 0.011), and −2.1 (p = 0.010), respectively. The difference in Beck anxiety inventory scores between tCBT + TAU and TAU at T1, T2, and T3 was −8.2 (p < 0.001), −7.9 (p < 0.001), and −6.3 (p < 0.001), respectively.
Characteristics of the Study Sample According to Treatment Group.
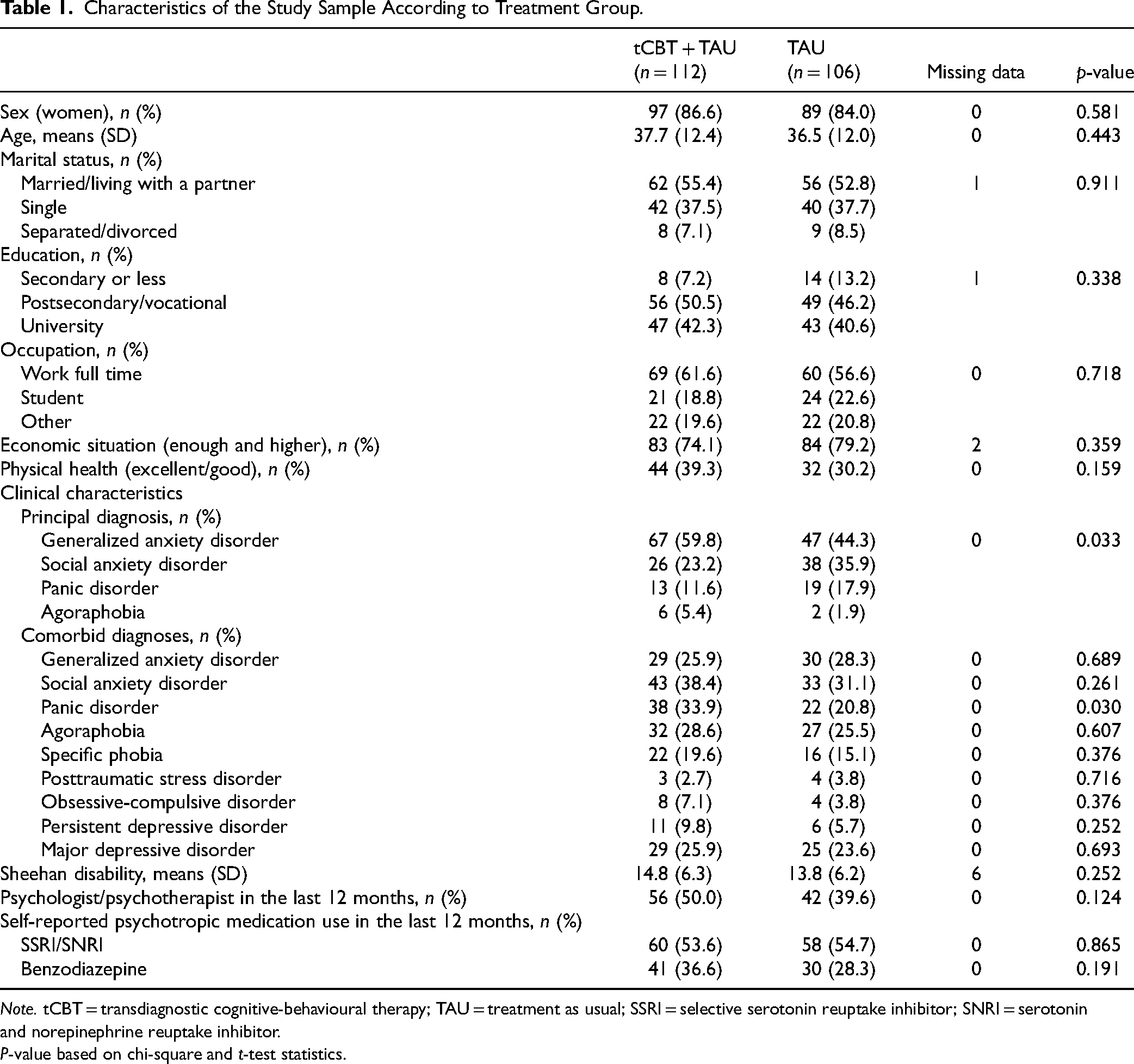
Note. tCBT = transdiagnostic cognitive-behavioural therapy; TAU = treatment as usual; SSRI = selective serotonin reuptake inhibitor; SNRI = serotonin and norepinephrine reuptake inhibitor.
P-value based on chi-square and t-test statistics.
Effects Associated With the Treatment Group.
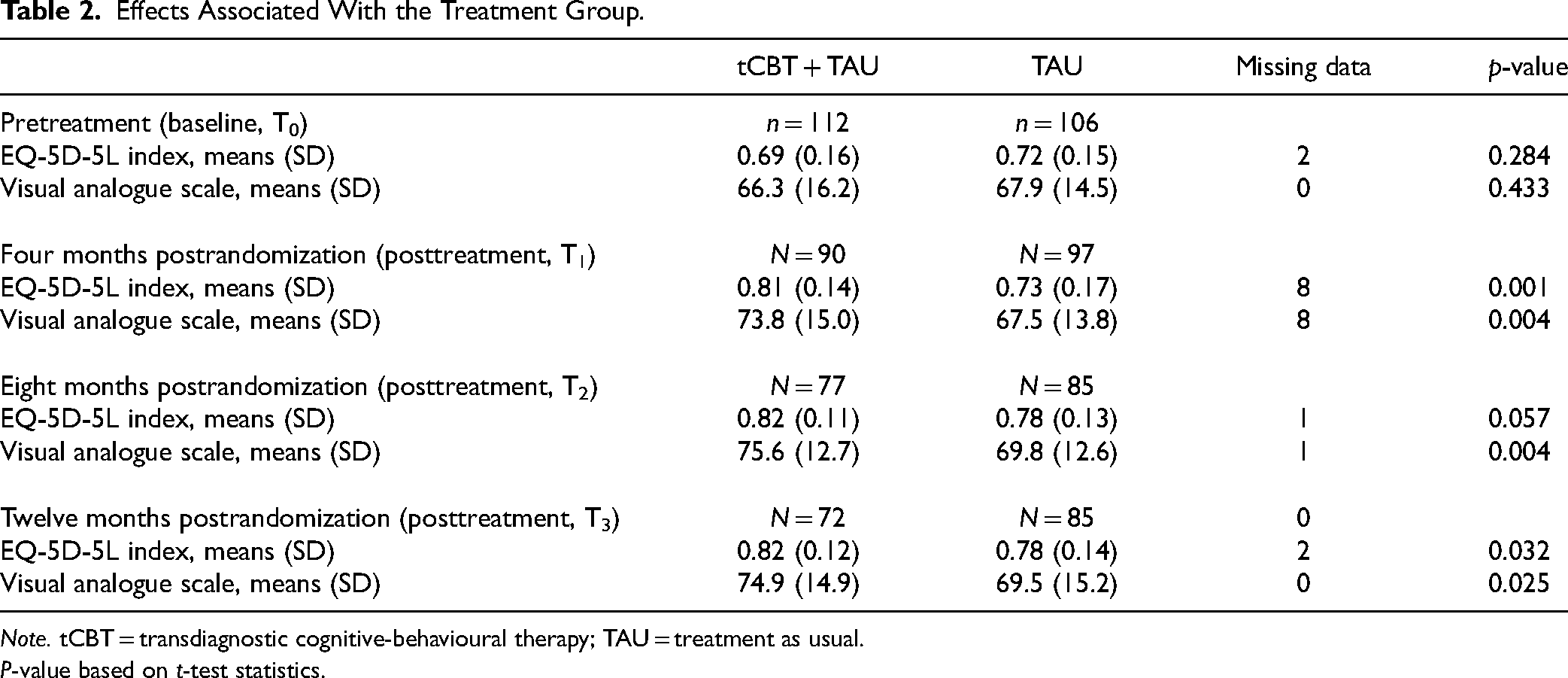
Note. tCBT = transdiagnostic cognitive-behavioural therapy; TAU = treatment as usual.
P-value based on t-test statistics.
Health care utilization according to the intervention group is presented in Supplemental Table S2. In general, no significant differences were observed in the type of health care utilization between intervention groups. The related health care costs are presented in Table 3. No significant difference was observed in total costs. In the year preceding baseline, individuals randomized in the TAU incurred higher day surgery-related costs than those in the tCBT + TAU arm and in the year following baseline, individuals randomized in the tCBT + TAU arm incurred higher emergency department costs than those in the TAU arm.
Unadjusted Costs (CAD) (mean per person) According to Treatment Groups.
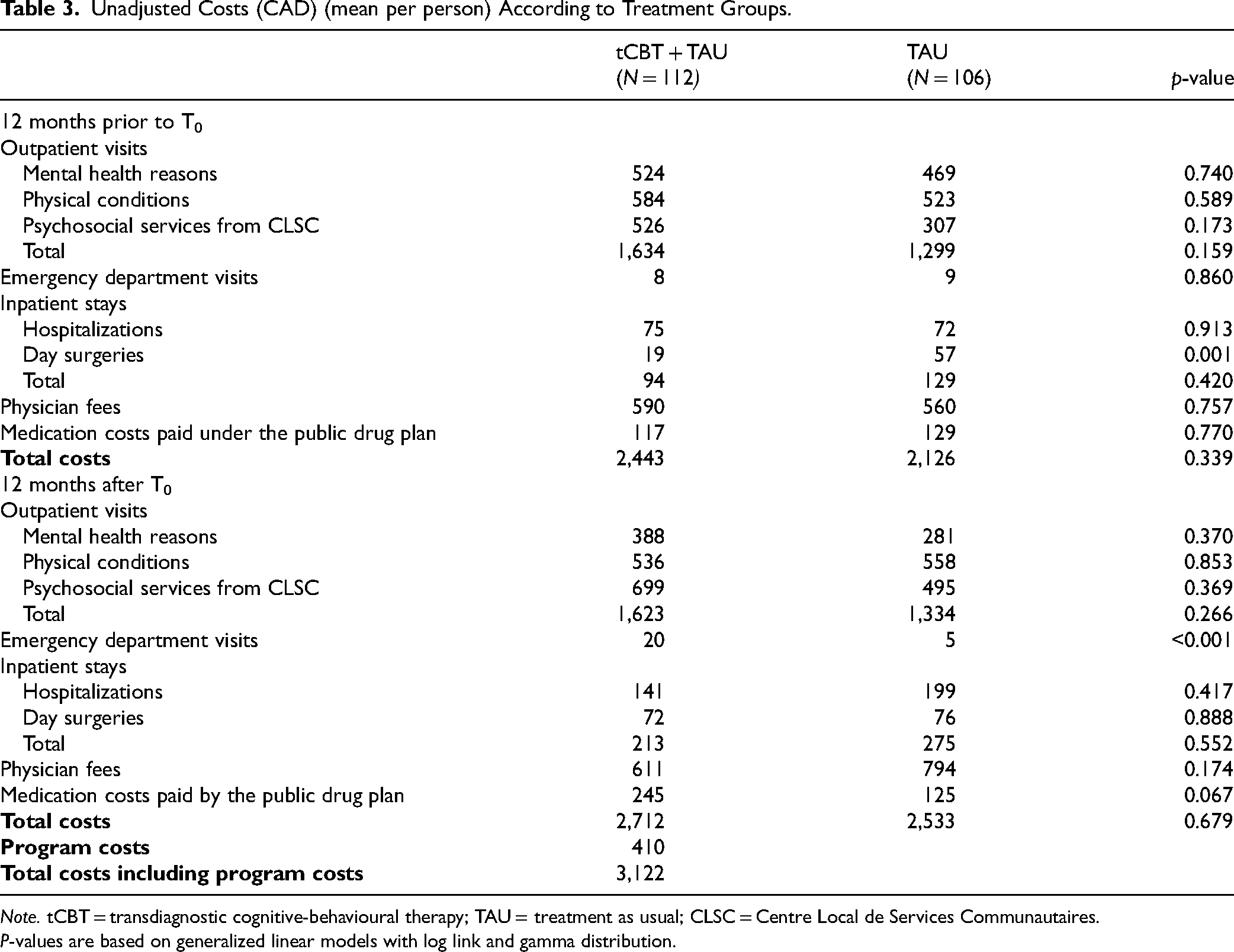
Note. tCBT = transdiagnostic cognitive-behavioural therapy; TAU = treatment as usual; CLSC = Centre Local de Services Communautaires.
P-values are based on generalized linear models with log link and gamma distribution.
The ICER point estimates from the imputed intention-to-treat and complete case analyses are presented in Table 4. The results showed that the ICER associated with tCBT + TAU as compared to TAU in the intention-to-treat analysis was $20,000/QALY and $6,581/QALY, based on unadjusted and adjusted point estimates, respectively. Complete case analysis showed similar results with an ICER of $15,556/QALY and $6,642/QALY, based on unadjusted and adjusted point estimates, respectively. The CEAC according to analyses is presented in Figure 1. Results from the adjusted NMB regression, based on intention-to-treat analyses, showed that at a WTP threshold of $20,000 and $40,000, the probability that tCBT + TAU as compared to TAU is cost-effective is 93.0% and 99.9%, respectively. Results from the complete case analyses showed that at a WTP threshold of $20,000 and $40,000, the probability that tCBT + TAU as compared to TAU is cost-effective is 82% and 97%, respectively. Results from the unadjusted NMB regressions showed that in the intention-to-treat and complete case analyses and at a WTP threshold of $60,000, the probability that tCBT + TAU as compared to TAU is >85%.
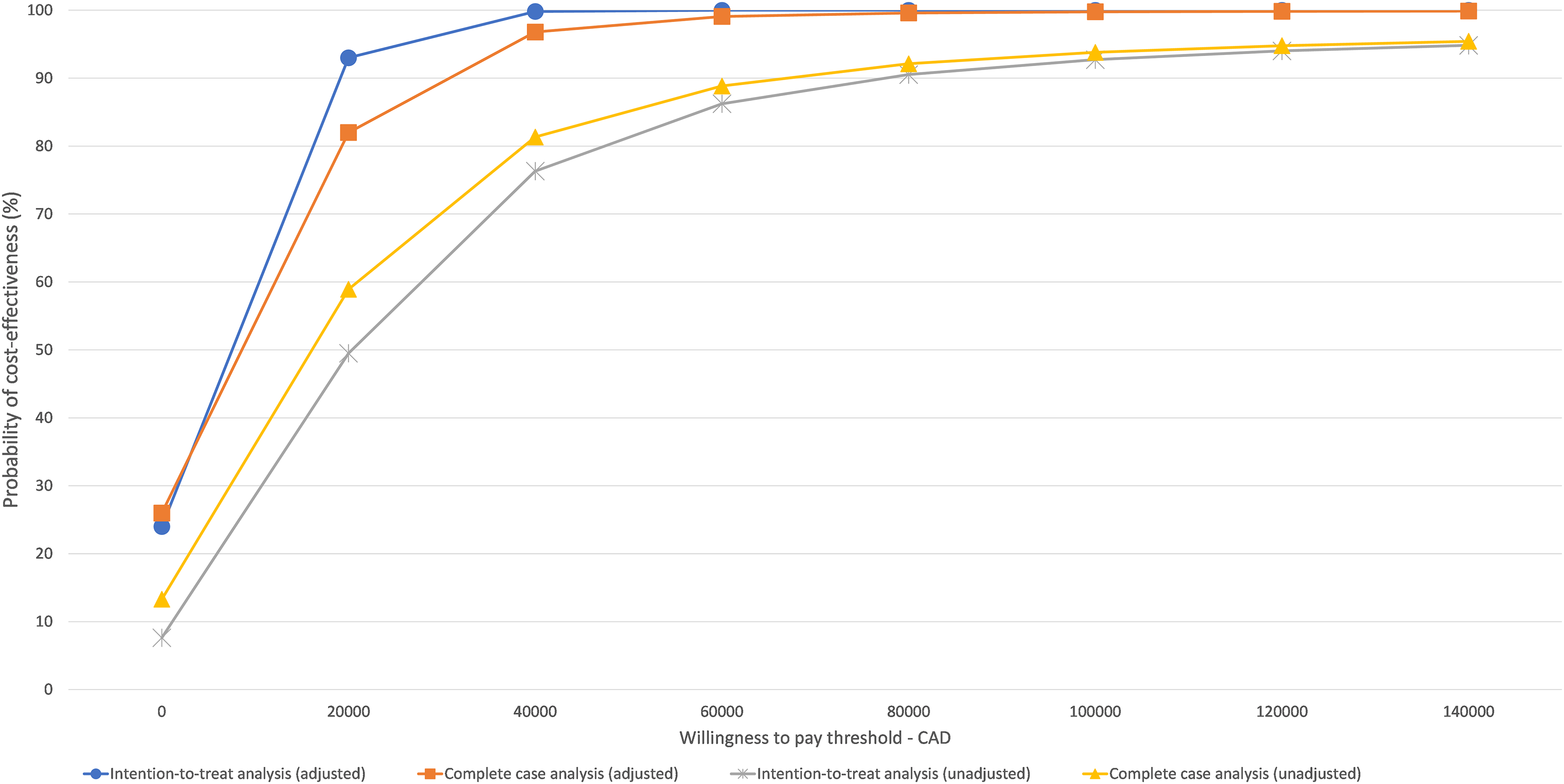
Cost acceptability curves from the healthcare system perspective.
Unadjusted and adjusted incremental QALYs, costs, and cost-effectiveness ratio from the health care system perspective over the 12-month period.
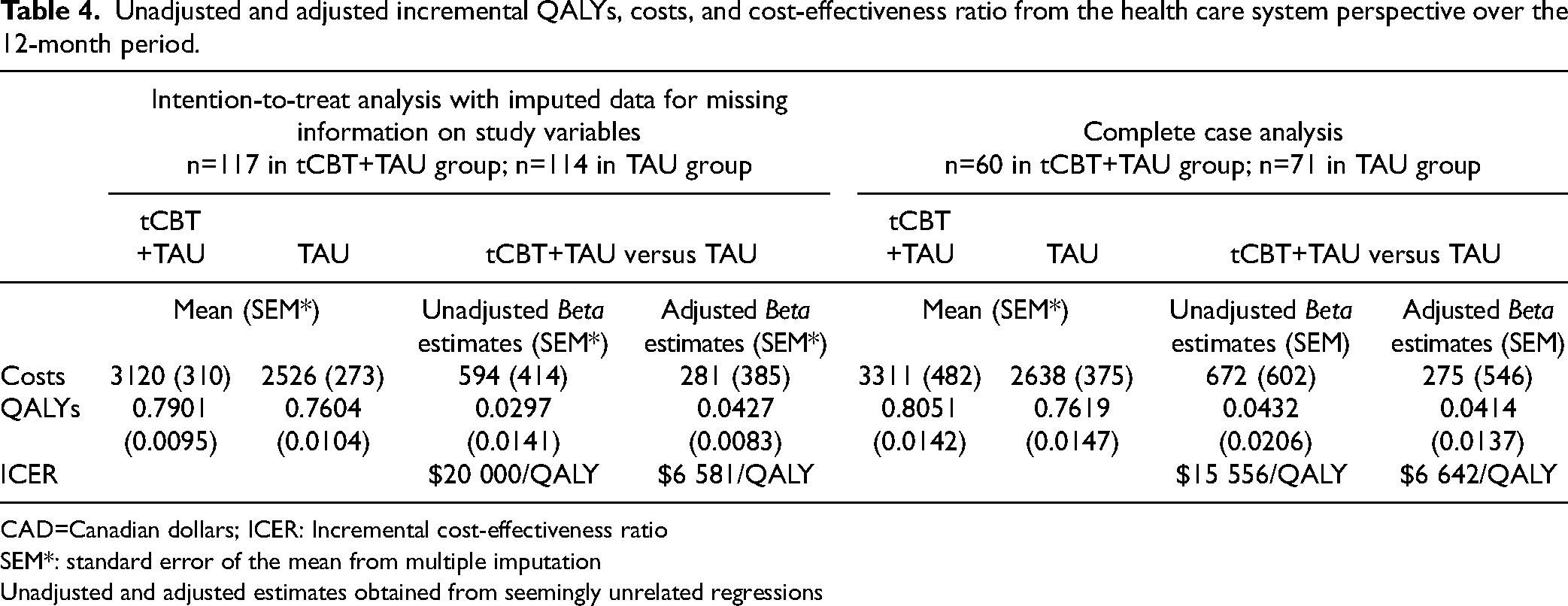
CAD=Canadian dollars; ICER: Incremental cost-effectiveness ratio
SEM*: standard error of the mean from multiple imputation
Unadjusted and adjusted estimates obtained from seemingly unrelated regressions
Discussion
This economic evaluation contributes to the rare studies on the cost-effectiveness of group tCBT for patients with anxiety disorders using information from provincial medico-administrative data to assess health care utilization and related costs, reducing recall and social desirability bias. This study also included a methodology and analytic approach that addressed missing information, skewness of data, confounders and the correlation between costs and QALYs, 42 which increased the validity of conclusions. Furthermore, this study was carried out within primary care settings where the majority of anxiety disorders are treated, and the healthcare system perspective taken provides important information for decision makers given the public healthcare system context where residents are covered for the majority of their medical consultations.
The findings showed that on average the total 1-year health care costs incurred by individuals randomized to receive group tCBT + TAU and TAU were similar. The average QALYs were, however, on average higher in those randomized to receive group tCBT + TAU as compared to TAU. The results also showed that group tCBT + TAU was more cost-effective than TAU from the healthcare system perspective for treating adult patients with anxiety disorders over a 1-year time horizon. The CEAC from the current study showed that tCBT + TAU was cost-effective as compared to TAU with high probability and this is from findings observed in the intention-to-treat and complete case analyses.
To our knowledge, very few studies have assessed the cost-effectiveness of group tCBT.29,31,56 In the current study, the ICER adjusting for potential baseline confounders was $6,581/QALY in the intention-to-treat analysis, which was similar to the ICER of $6,642/QALY observed in the complete case analysis. These estimates are similar to those reported on the effectiveness and cost-effectiveness of CBT for anxiety disorders. In Australia, the cost-effectiveness ratio for CBT compared to TAU was $6900/QALY AUD (CAD $6500/QALY) for the treatment of generalized anxiety disorder and panic disorder from the public healthcare system perspective. 57 CBT has also been shown to be cost-effective in specialized mental health settings as part of routine care for patients with anxiety disorders. 58
Although specific WTP thresholds have not been systematically used in studies, earlier benchmarks suggested a threshold of CAD $50,000/QALY to CAD $100,000/QALY.59-61 A recent meta-regression analysis of a systematic review predicted a WTP threshold in the province of Quebec of CAD 127,985/QALY. 52 Based on these WTP thresholds, the results of the current study, suggest that group tCBT + TAU as compared to TAU has a high probability of being cost-effective. In fact, the probability was 93% and 99% that tCBT + TAU as compared to TAU was cost-effective at a WTP of $20,000 and $40,000, respectively. Using self-declared health service utilization data from the same trial over an 8-month period, the probability that tCBT + TAU as compared to TAU was 97% at a WTP of $50,000 from the healthcare system perspective.
The results of this study should be interpreted with the following considerations. First, among the 231 participants randomized and who completed the baseline interview, 13 did not consent to access their medico-administrative data. Loss to follow-up was 14% at T1, 26% at T2, and 28% at T3. Of the individuals randomized, 131 had complete information on all study variables. There were no differences in losses to follow-up with regard to sociodemographic factors and anxiety symptoms. Losses were, however, more likely to have a principal diagnosis of agoraphobia and panic disorder. Second, costs were measured from the healthcare system perspective and health service utilization was assessed through information found in the provincial medico-administrative data, which may be subject to data entry errors. Studies however have shown that these provincial medical and pharmaceutical registries are valid sources for health service utilization 62 and therefore the potential information bias leading to an underestimation of health system costs is reduced. Furthermore, we do not expect that this information bias was differential between groups and therefore results presented are more likely to be conservative. Third, although the use of the EQ-5D has been recommended in economic evaluation guidelines, 63 other instruments such as the Assessment of Quality of Life-8 dimensions scale (AQoL-8D) may be more sensitive in assessing changes related to the treatment of mental disorders such as anxiety 64 and should be considered in future studies assessing the cost-effectiveness of tCBT. Finally, the findings can be generalized to adults with anxiety disorders consulting in community settings. Individuals having consulted in the past year with a psychiatrist were excluded from the study. Studies have shown that individuals with anxiety having been prescribed medications from a psychiatrist, as compared to a primary care physician, were twice more likely to receive psychotherapy. 65 Although patients consulting psychiatrists may represent different referral and health service trajectories, research should also assess the cost-effectiveness of group tCBT in patients that have received specialized mental health services such as those from psychiatrists.
Conclusion
The study findings suggest that, for anxiety disorders, group tCBT + TAU as compared to TAU has a high probability of being cost-effective. This group intervention has the potential to increase access to psychotherapy treatment for anxiety disorders in Canada, where barriers such as long waiting lists in mental health services persist. The implementation of group tCBT within a primary care context is also aligned with increasing delivery of community-based mental health interventions, a sustainable solution to improve access to mental health services in Canada. 16 Future studies including younger and older adults and different clinical patient populations with different anxiety disorders are needed to further investigate the cost-effectiveness of tCBT.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437231187459 - Supplemental material for Cost-Effectiveness of Group Transdiagnostic Cognitive Behavioural Therapy for Anxiety Disorders in Primary Care Settings: Economic Evaluation From the Healthcare System Perspective Over a 1-Year Time Horizon
Supplemental material, sj-docx-1-cpa-10.1177_07067437231187459 for Cost-Effectiveness of Group Transdiagnostic Cognitive Behavioural Therapy for Anxiety Disorders in Primary Care Settings: Economic Evaluation From the Healthcare System Perspective Over a 1-Year Time Horizon by Helen-Maria Vasiliadis, Catherine Lamoureux-Lamarche, Alexandra Chapdelaine, Martin D. Provencher, Peter J. Norton, Djamal Berbiche and Pasquale Roberge in The Canadian Journal of Psychiatry
Supplemental Material
sj-doc-2-cpa-10.1177_07067437231187459 - Supplemental material for Cost-Effectiveness of Group Transdiagnostic Cognitive Behavioural Therapy for Anxiety Disorders in Primary Care Settings: Economic Evaluation From the Healthcare System Perspective Over a 1-Year Time Horizon
Supplemental material, sj-doc-2-cpa-10.1177_07067437231187459 for Cost-Effectiveness of Group Transdiagnostic Cognitive Behavioural Therapy for Anxiety Disorders in Primary Care Settings: Economic Evaluation From the Healthcare System Perspective Over a 1-Year Time Horizon by Helen-Maria Vasiliadis, Catherine Lamoureux-Lamarche, Alexandra Chapdelaine, Martin D. Provencher, Peter J. Norton, Djamal Berbiche and Pasquale Roberge in The Canadian Journal of Psychiatry
Footnotes
Data Access
The authors are not legally authorized to share or publicly publish data. Participants were not requested to give informed consent for data sharing. Requests for access to the data should be addressed to the ethics boards who approved the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Considerations
The research protocol was approved by the principal ethics review boards of the Integrated Health and Social Services Centers in Estrie (No. MP-22-2016-570), Québec City (No. 2017-166), and Laval (No. 2016-2017-C54). All participants provided written informed consent.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The current study was funded by the Canadian Institutes of Health Research funded this study (CIHR grant nos. 334091 and 340410). The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.