
Abstract

Introduction
The use of telemedicine increased during the COVID-19 pandemic, facilitated by changes to billing structures that allowed reimbursement for telephone- and video-based care. 1 Systematic reviews have found that telemedicine for mental health and substance use disorders is effective and associated with high patient satisfaction.2,3 Despite favourable outcomes with both telephone- and video-based care, proposals have emerged to reduce or eliminate physician compensation for telephone-based care, which may decrease the number of physicians providing this service.4,5
To our knowledge, no studies have examined how de-listing telephone services would impact disparities in access to telemedicine in Canada. We sought to determine the impact of eliminating telephone-based care on Canadians’ ability to access telemedicine, and we hypothesized that removing the option of telephone-based care would increase disparities in telemedicine access. 4
Methods
The Centre for Addiction and Mental Health Research Ethics Board (REB) determined that the study was exempt from REB review. The manuscript follows the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.
Data Sources
We obtained data from the 2019 Survey of Household Spending (SHS) public use microdata files. 6 The 2019 SHS was a cross-sectional survey administered by Statistics Canada between January and December 2019. 7 The survey was completed via in-person interviews and a mail-in spending diary that was not dependent on telephone or internet access. The target population was all Canadian households in the provinces excluding households on First Nations reserves, members of the Canadian Forces living on bases, and individuals living in institutions. The survey had a stratified two-stage design, in which geographic areas were first selected within strata defined by provinces and groups of geographic areas within provinces. Households were subsequently sampled within each selected area. A single respondent from each household completed the survey. Respondent households were weighted by Statistics Canada to represent the target population.
The public use files included data from responding households that completed both the in-person interview and the subsequent mail-in spending diary. 6 These included households were weighted to represent the original target population. Data within the public use files contain additional modifications to preserve confidentiality (e.g., data perturbation) to preserve anonymity for responding households, which may result in additional small changes to estimates. 6
Outcomes and Covariates
The main outcome in our secondary analysis was the proportion of households in Canada that would lose the potential to access telemedicine at home if telephone-based care were eliminated. We extracted information about household income, age of household members, province of household, access to a motor vehicle defined as having owned, leased, or used a motor vehicle in the past year, and access to the internet or telephone service at home (landline or ≥1 cell phone in a household) from the SHS public use microdata. We included the use of a motor vehicle in the last year as households without access to a car may have increased difficulty attending in-person visits. 8
Statistical Analysis
Variances were calculated using bootstrapped weights accounting for the stratified survey design. Rao-Scott chi-square tests were used to test for associations between sociodemographic characteristics and lost potential access to telemedicine. The significance level was set at p = 0.05.
In an exploratory analysis, we assessed predictors of loss of access with the elimination of telephone-based care in a multivariable logistic regression model. We calculated adjusted odds ratios (aOR) for each household income, age distribution, access to a motor vehicle and province/region, while accounting for the survey weights. Data were analyzed using the survey package in R 4.2.1 (R Foundation for Statistical Computing) from November 16, 2022, to January 23, 2023.
Results
The SHS selected 17,491 households in the 10 provinces, with 10,890 responding households (response rate: 62.3%). The public use microdata contained 7,566 responses weighted to represent 14,706,626 Canadian households. The vast majority (99.7%, 95% CI, 99.3% to 99.8%) of households had access to either internet or telephone; 99.2% (95% CI, 98.8% to 99.5%) of households had access to telephones and 91.9% (95% CI, 90.9% to 92.8%) had access to the internet (Table 1). With the elimination of telephone-based care, 7.8% (95% CI, 6.9% to 8.7%) of households would lose the ability to access telemedicine from within the household. Removal of telephone-based care would increase disparities across age, income, and households without access to a car (p < 0.001 for all). Access to telemedicine services would be lost by 23.1% (95% CI, 20% to 26.6%) of households with residents all over age 65, 22.7% (95% CI, 19.7% to 26.0%) of households with a household income under 40,000, and 16.5% (95% CI, 13.1% to 20.6%) of households without access to a motor vehicle.
In the multivariable model, household income under $40,000 was the strongest predictor of loss of access to telemedicine (aOR 20.2; 95% CI, 7.1 to 57.2, p < 0.001) (Table 2). A household income between $40,000–79,999 (aOR 5.6; 95% CI, 2.0 to 16.0, p < 0.001), a household in which all individuals were over age 65 (aOR 4.7; 95% CI, 3.4 to 6.4, p < 0.001) and household without the use of a motor vehicle in the last year (aOR 1.6; 95% CI, 1.1 to 2.4, p = 0.012) were significantly associated increased odds of loss of access in adjusted analyses. Living in British Columbia was associated with reduced odds of losing access to telemedicine if telephone-based care were eliminated (aOR 0.6; 95% CI, 0.4 to 0.9, p = 0.008).
Discussion
This study suggests that eliminating telephone-based care would both decrease access to telemedicine among Canadian households and exacerbate disparities in access to telemedicine. Eliminating telephone-based care would result in the loss of ability to access in-home telemedicine by over 1 in 5 households in which all residents were aged 65 or over, over 1 in 5 households with a household income under $40,000, and approximately 1 in 6 households without the use of a car in the past year. Households in British Columbia were most likely to have internet access and least likely to lose access to telemedicine with the elimination of telephone-based care.
In adjusted analyses, this study found that living in a household with an income under $40,000 was the strongest predictor of potential loss of access to telemedicine, followed by living in a household with an income of $40,000 to 79,999 or living in a household with all residents over age 65. Individuals with low incomes face several barriers to in-person care, and loss of access to telemedicine may exacerbate these income-based health disparities. 9 Similar potential increases in disparities from the elimination of audio-based care have been found in the United States, with older individuals and individuals living in households with lower incomes more likely to lose potential access. 4
This study has several limitations. The SHS does not include individuals residing on First Nations reserves, in collective living environments or who are unstably housed. The public use microdata files from the SHS contained information only from households that completed both the in-person interview and the subsequent mail-in spending diary; reweighting of the responding households by Statistics Canada in the public use files adjusted for this effect. No information is available about the ability to use each telecommunication technology, which may exacerbate differences in accessibility. Information about the speed of internet connectivity was not available. The 2019 SHS was conducted before the onset of the COVID-19 pandemic, and telecommunication access may have changed since the survey administration. The definition of access to motor vehicles is broadly defined and does not reflect ease of access. Information about urban–rural status and other individual-level sociodemographic characteristics was not available.
Conclusion
This study suggests that eliminating telephone-based care would both decrease potential access to telemedicine among Canadian households and exacerbate disparities in access to telemedicine. Governments in Canada that are considering policies that would reduce access to telephone-based care should consider the differential effects on access due to such policies and attempt to mitigate the resulting disparities. Future studies should investigate the impact of eliminating telephone-based care by race, ethnicity, housing status, and rurality.
Sociodemographic characteristics of responding households and proportions of households with each type of in-home telecommunications access.
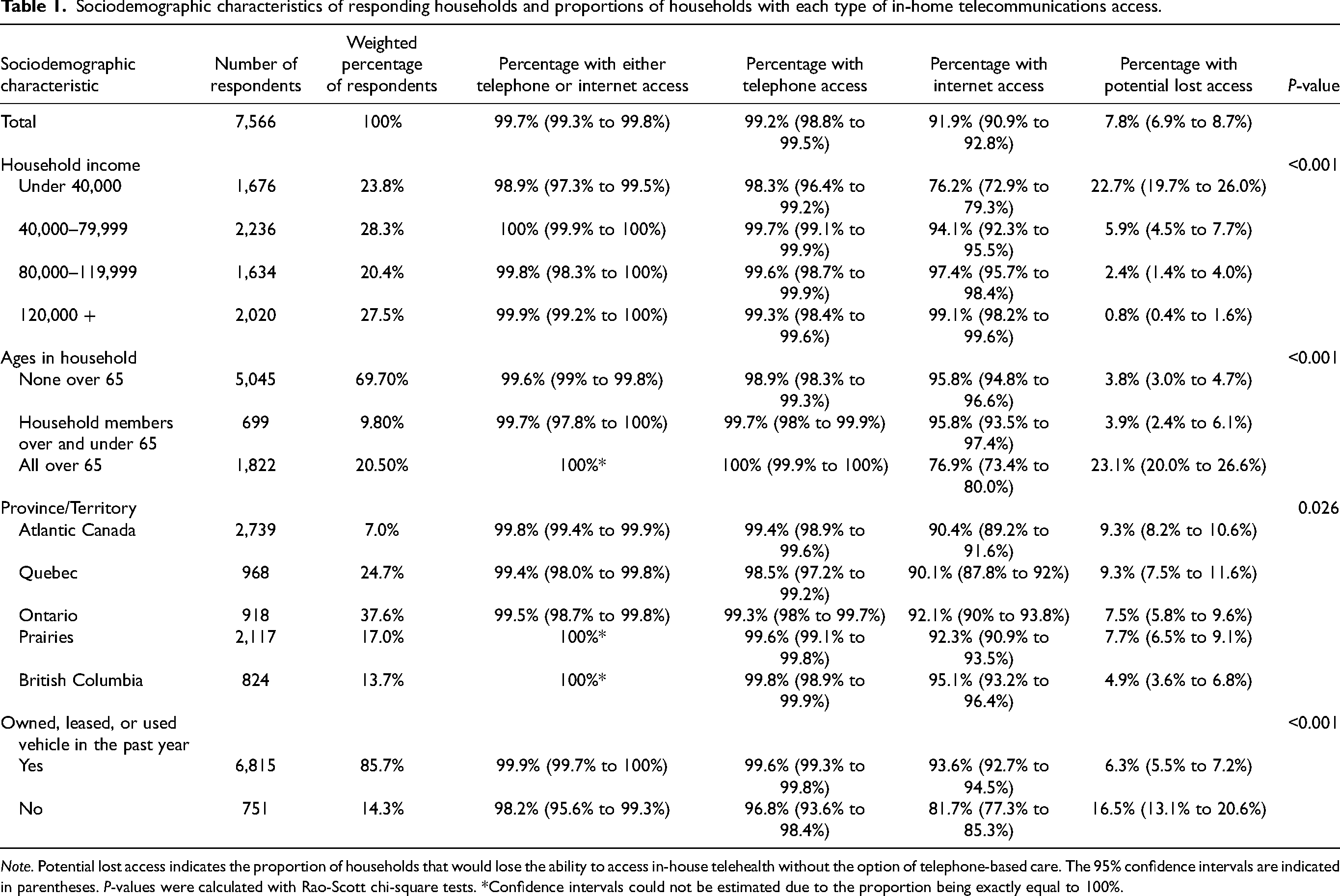
Note. Potential lost access indicates the proportion of households that would lose the ability to access in-house telehealth without the option of telephone-based care. The 95% confidence intervals are indicated in parentheses. P-values were calculated with Rao-Scott chi-square tests. *Confidence intervals could not be estimated due to the proportion being exactly equal to 100%.
Adjusted odds ratios for loss of access to in-home telemedicine from the elimination of telephone-based care.
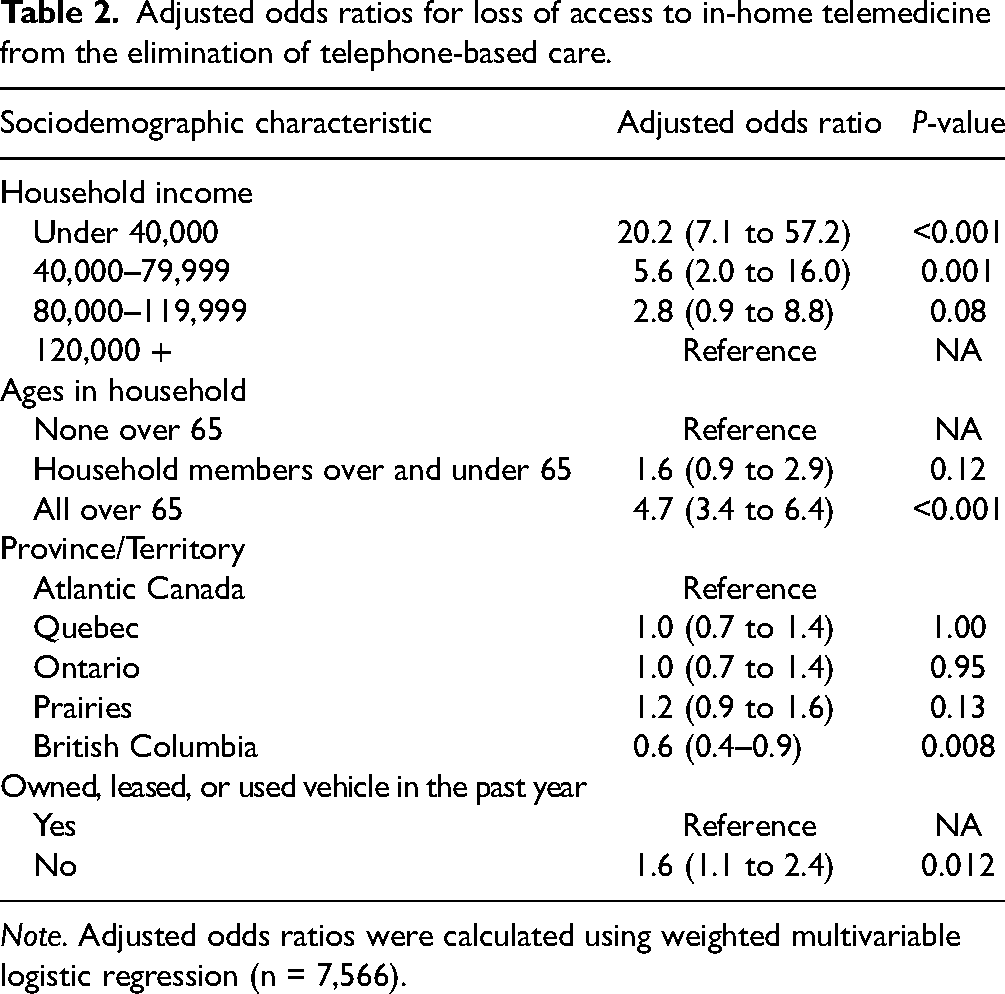
Note. Adjusted odds ratios were calculated using weighted multivariable logistic regression (n = 7,566).
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Kleinman has received research funding and training support through the Research in Addiction Medicine Scholars Program, R25DAO33211 (NIDA) for work outside of this study and travel awards from the American Psychiatric Association and American Academy of Addiction Psychiatry. Dr. Bozinoff has also received research funding and training support from the International Collaborative Addiction Medicine Research Fellowship NIDA grant R25-DA037756. Dr. Bozinoff has received research funding from the Canadian Institutes of Health Research, the Academic Health Sciences Alternate Payment Plan, and Womenmind for work outside of this study. Dr. Bozinoff has also received research funding and training support from the International Collaborative Addiction Medicine Research Fellowship NIDA grant R25-DA037756. Drs. Kleinman and Bozinoff receive remuneration for clinical services, including virtual care/telehealth services, through the Ontario Health Insurance Plan.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project received funding through the Centre for Addiction and Mental Health Discovery Fund.